
Abstract
Background
The COVID-19 pandemic disrupted delivery of health care services worldwide. We examined the impact of the pandemic on clinics participating in the Veterans Affairs (VA) Clinical Resource Hub (CRH) program, rolled out nationally in October 2019, to improve access to care at under-resourced VA clinics or “spoke” sites through telehealth services delivered by regional “hub” sites.
Objective
To assess whether the CRH program was associated with increased access to primary care, we compared use of primary, emergency, and inpatient care at sites that adopted CRH for primary care (CRH-PC) with sites that did not adopt CRH-PC, pre-post pandemic onset.
Design
Difference-in-difference and event study analyses, adjusting for site characteristics.
Study Cohort
A total of 1050 sites (254 CRH-PC sites; 796 comparison sites), fiscal years (FY) 2019–2021.
Intervention
CRH Program for Primary Care.
Main Measures
Quarterly number of VA visits per site for primary care (across all and by modality, in-person, video, and phone), emergency care, and inpatient care.
Results
In adjusted analyses, CRH-PC sites, compared with non-CRH-PC sites, had on average 221 additional primary care visits (a volume increase of 3.4% compared to pre-pandemic). By modality, CRH-PC sites had 643 fewer in-person visits post-pandemic (− 14.4%) but 723 and 128 more phone and video visits (+ 39.9% and + 159.5%), respectively. CRH-PC sites, compared with non-CRH-PC sites, had fewer VA ED visits (− 4.2%) and hospital stays (− 5.1%) in VA medical centers. Examining visits per patient, we found that CRH-PC sites had 48 additional telephone primary care visits per 1000 primary care patients (an increase of 9.8%), compared to non-program sites.
Conclusions
VA’s pre-pandemic rollout of a new primary care telehealth program intended to improve access facilitated primary care visits during the pandemic, a period fraught with care disruptions, and limited in-person health care delivery, indicating the potential for the program to offer health system resilience.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
INTRODUCTION
The onset of the COVID-19 pandemic disrupted health care services globally.1, 2 Health systems began shutting down non-essential patient services in March 2020 to prevent the spread of COVID-19 infection. The disruption to care delivery posed threats of severely worsening health care access in already fragile rural and underserved areas that face perennial shortages of health care professionals. In response to the pandemic, health systems began making unprecedented shifts to delivering care remotely via telehealth modalities.3 Telehealth is broadly defined as “the use of electronic information and telecommunication technologies to support long-distance clinical healthcare.”3, 4 The pandemic emphasized the importance of telehealth, specifically synchronous audio-only and audio–video episodes of care between patients and clinicians,5 as a key strategy for maintaining and facilitating access to care during crisis times, with the potential to enable health system resilience.1, 6,7,8,9,10,11,12
However, very few large-scale or national studies have evaluated whether existing telehealth infrastructure facilitates delivery of health care during crisis times.8, 13 The lack of studies on this topic may, in part, be attributed to the historically low uptake of telehealth by health systems prior to the COVID-19 pandemic. The U.S. Veterans’ Health Administration (VA) is an important exception as it was a leading provider of telehealth services in the USA even prior to the COVID-19 pandemic.14 As such, VA programs and data allow opportunities to examine how existing telehealth infrastructure can help maintain access to care and minimize care disruptions if crises, such as the COVID-19 pandemic, arise.
In this study, we leverage VA’s existing telehealth infrastructure and a relatively more established culture of telehealth encounters between patients and providers to examine the provision of primary care facilitated by the pre-pandemic rollout of VA’s Clinical Resource Hub (CRH) telehealth program. Building on pilot programs, VA began implementing a national contingency staffing program in October 2019, 11, 15,16,17 just before the onset of the COVID-19 pandemic. CRH aimed to provide staffing on a contingency basis in cases of non-catastrophic staff deficits or gaps in health care supply at primary and mental health clinics primarily through telehealth services administered from VA regional hub sites to local VA clinics within the VA regional networks.15 While CRH was originally intended to be a site-to-site telehealth model, the majority of CRH services shifted to a site-to-home telehealth model at the onset of the pandemic.
We hypothesized that adoption of the CRH program would provide telehealth infrastructure advantages that would facilitate primary care utilization during the pandemic and also potentially reduce downstream emergency and inpatient care use as some care may be preventable through timely and improved access to primary care.18,18,20 In this study, we evaluated the impact of the pandemic on CRH’s delivery of primary care (total and by modality) and use of emergency and inpatient care within VA by comparing CRH sites and non-program sites pre- and post-pandemic.
INTERVENTION
CRH uses a “hub-and-spoke” model to connect patients at outpatient “spoke” sites with clinical staff at “hub” sites in regional VA networks primarily via telehealth. VA’s interdisciplinary primary care teams, called Patient Aligned Care Teams (PACT), in hub sites assume responsibility for a panel of patients at spoke sites. Spoke sites with PACT team shortages and difficulties with provider recruitment may be eligible for CRH. CRH-PC sites were defined by the CRH program as sites with at least 10 CRH-PC visits per month for 2 consecutive months.
DATA AND METHODS
Study Cohort
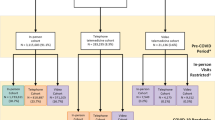
To identify our study cohort, we began with all VA clinics or sites (n = 1110) and excluded atypical such as community living centers or sites with fewer than 450 patients over the study period, similar to prior work.21 The final study cohort included 1050 VA sites (CRH-PC: 254; non-CRH-PC: 796). All patients assigned to a PACT team in each site were included; patient assignments were identified from the Reengineered Patient Care Management Module in the Corporate Data Warehouse (CDW).22
Outcomes
As adoption of CRH can impact both the number of care visits and patients seen at sites, we examined the quarterly number of visits and patients served per site for two types of care:
-
VA outpatient primary care—primary care visits (total across all modalities—phone, video, and in-person and by each modality) and primary care patients served.
-
VA emergency department (ED) visits and hospitalizations—visits to and patients seen in EDs and inpatient stays within the VA system.
We considered reporting change in visits per patient assigned to each site; however, many patients assigned to a PACT team are not expected to and do not use primary care in each quarter. We therefore reported results as the percentage change in volume of visits and patients served compared to baseline patterns of utilization, adjusting for site size. We also reported the number of visits per 1000 primary care patients served to indicate the extent of changes for patients who do utilize primary care in each quarter.
Note that if a hub provider had a telehealth visit for a patient assigned to a spoke site, the visit was attributed to the spoke site. Data on PC and ED encounters were obtained from Managerial Cost Accounting (MCA) OUT (Outpatient) National Data Extract (NDE),23 where we categorized primary and secondary clinic stop code pairs into categories and modalities of care. Hospitalizations were obtained from MCA TRT (Treating Specialty) NDE.23
Covariates
We adjusted for differences in outcomes due to potentially differing site characteristics. We adjusted for site rurality (e.g., urban, rural, highly rural), site type (e.g., VHA Medical Center (VAMC), PC Community-Based Outpatient Clinic (PC-CBOC), multi-specialty CBOC (MS-CBOC), other), site size (number of patients with PACT team assignments by quarter), geographic region of each VA service network (East Coast, Southeast, Rocky Mountain/Gulf, Midwest, West Coast), and the quarterly average Elixhauser Comorbidity Score of patients assigned to each site. Importantly, we also included a binary indicator of whether a site ever adopted CRH-PC to adjust for any remaining unobservable differences across program and non-program sites that were time-invariant. In sensitivity analyses, we also adjusted for site-level summaries of other patient covariates such as mean age, as well as percents male, White, Black, Hispanic, and VA enrollment priorities 1 and 2.
In all models, we included the quarterly count of COVID-19 cases in each county24 and included quarter indicators to adjust for any shocks to health care systems or care use in each quarter, including lingering effects of the pandemic outside of the case count.
Covariate data were obtained from the CDW,22 VHA’s Geospatial Service Support Center,25 and New York Times’ COVID-19 county-year level data downloaded from GitHub.24
Statistical Analyses
We first examined baseline site characteristics for CRH-PC and non-CRH-PC sites from FY2020Q1 (October-December 2019) before pandemic-related shutdown of in-person care began. We then examined unadjusted trends of CRH-PC and non-CRH-PC sites before and after the onset of COVID-19 to determine whether a difference-in-difference (DiD) framework was appropriate. Event studies improve on the traditional DiD estimator26,26,28 because they estimate differences between treatment and control group for each period prior to and after treatment (i.e., each quarter pre- and post-pandemic onset in our case).26, 28 This allows to visually and more transparently assess whether pre-pandemic model-adjusted differences between CRH-PC sites and non-CRH-PC sites were significant or trending upward or downward in a manner that could obscure or mask true differences in the post-pandemic onset period.26, 28, 29 An absence of pre-pandemic differences across CRH-PC and non-CRH-PC sites after covariate adjustment followed by abrupt differences post-pandemic signals attributability of findings to the pandemic.26, 28, 29 We also generated traditional DiD estimates to obtain the average effect of CRH-PC across all post-pandemic onset quarters (methods details in Appendix Section A).
As effects may vary across types of VA sites or site size, we conducted identical analyses, stratified by site type as site size is vastly different across site types and among these stratified analyses, further adjusted for site size. We also examined the number of visits per 1000 primary care patients served.
To strengthen attributability of findings to the CRH program, we conducted sensitivity analyses restricting the sample of CRH-PC sites to sites with pre-pandemic program implementation and to sites with program implementation during the majority of the post-pandemic onset period. We also examined reliance on CRH-PC services at CRH-PC sites (Appendix Section D).
All statistical analyses were conducted in Stata 17.0 (StataCorp, LLC).
This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. It was funded by VA’s Office of Primary Care for quality improvement purposes and was therefore exempted from review by the Stanford institutional review board.
RESULTS
Unadjusted Baseline Characteristics and Trends
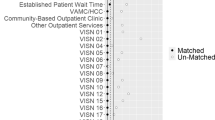
We found no differences in site rurality and average Elixhauser comorbidity score of patients across CRH-PC and non-CRH-PC sites, but noted some differences in site type, site size, and geographic region (Table 1). We found that VAMCs, MS-CBOCs, and larger sites were more likely to adopt CRH-PC. West Coast VA sites, followed by Rocky Mountain/Gulf region sites, were more likely to adopt CRH-PC. Similar comparisons stratified by site type are also provided in Appendix Tables 5, 6, and 7.
Unadjusted trends in primary care visits, ED visits, and hospitalizations show that prior to pandemic onset, CRH-PC sites and non-CRH-PC sites had roughly parallel trends, providing support for the use of DiD methods (Fig. 1). Unadjusted trends were very similar when we examined total number of patients served (Appendix Fig. 3).

Unadjusted visit trends for VA primary care (total and by modality), emergency and inpatient care in Clinical Resource Hub program sites and non-program comparison sites FY2019–2021.
Adjusted Event Study Results
Event study graphs show that after covariate adjustment, there were virtually no differences between CRH-PC and non-CRH-PC sites prior to the pandemic onset, whereas there were abrupt differences across CRH-PC and non-CRH-PC sites just after the onset of the pandemic (Fig. 2). This pattern of no differences pre-pandemic onset followed by abrupt differences post-onset signals attributability of post-onset changes to the pandemic onset. Event study results were very similar when we examined number of patients served (Appendix Fig. 4).

Adjusted visits for VA primary care (total and by modality), emergency and inpatient care, FY2019–FY2021, in Clinical Resource Hub program sites compared to non-program sites relative to the baseline quarter FY2020Q1—event study estimates (and 95% C.I.s).
We also found similar results in sensitivity analyses restricting the sample of CRH-PC sites to sites pre-pandemic program implementation (Appendix Fig. 5) and to sites with program implementation for a majority of the post-pandemic onset period (Appendix Fig. 6). In analyses focusing on CRH-PC sites only, we demonstrated that reliance on CRH-PC increases during the post-pandemic onset period but that sites were using CRH infrastructure also for non-CRH services (Appendix Fig. 7).
Adjusted difference-in-difference results
In traditional DiD analyses (Table 2), we found that CRH-PC sites, compared with non-CRH-PC sites, had 221 (95% CIs 11:431) additional primary care visits across all modalities per quarter, a 3.4% increase compared to prior to the pandemic. By modality, we found that CRH sites had 643 (95% CIs − 910: − 377) fewer in-person visits (− 14.4% compared to pre-pandemic utilization at CRH-PC sites) but had 723 (95% CIs 433:1,014) and 128 (95% CIs 56:199) more visits via phone and video telehealth per quarter (+ 39.9% and + 159.5% compared to pre-pandemic utilization) than comparison sites, respectively. We also found that CRH-PC sites had 29 (95% CIs − 57: − 1) fewer VA ED visits and 10 (95% CIs − 18: − 2) fewer VA hospital stays post-pandemic onset per quarter (− 4.2% and − 5.1% compared to pre-pandemic), respectively, compared with non-CRH-PC sites. DiD estimates were broadly similar when we examined the impact of CRH-PC on the number of patients served (Table 3).
Examining the number of visits per 1000 primary care patients served (Table 4), we did not find significant differences in in-person visits or video visits per patient served, but found that CRH-PC sites had 48 (95% CIs 10: 85) additional phone primary care visits per 1000 primary care patients served, compared to comparison sites.
In analyses stratified by site type (Table 2), we found that PC-CBOCs with CRH-PC, compared to PC-CBOCs without CRH-PC, had 240 fewer in-person visits (− 10.4% compared to pre-pandemic) but 300 additional phone visits (+ 31.6%). MS-CBOCs with CRH-PC, compared to MS-CBOCs without CRH-PC, had additional 521 primary care visits across all modalities (+ 7.1%) and 915 more phone visits for primary care (+ 46.4%). Examining the number of patients, we found that PC-CBOCs and MS-CBOCs with CRH served more patients through telephone visits than comparison PC-CBOCs and MS-CBOCs (+ 29.6% and + 38.7%, respectively, compared to pre-pandemic) (Appendix, Table C1).
DISCUSSION
This study is the first to compare use of primary care in sites with and without CRH-PC before and after the COVID-19 pandemic. We found that VA’s CRH-PC program was associated with a modest 3.4% increase in primary care visit volume across all modalities (in-person, telephone, video, and other) during the pandemic, driven by increases in telephone and video visits, which offset declines in in-person visits that occurred immediately after the onset of the pandemic. We also found that CRH-PC was associated with modest decreases in VA ED visits and in VA inpatient stay volumes (− 4.6% and − 5.7%, respectively) relative to non-CRH-PC sites. Findings were similar when we examined the volume of patients served in primary care.
We stratified all our analyses by site type as medical center-based clinics are typically much larger than community-based outpatient clinics. In these analyses, we found that the pattern of volume declines in in-person visits and offsetting increases in telehealth for primary care was more prominent at VA’s PC-CBOCs and MS-CBOCs. This is consistent with prior studies on CRH (and its pilot versions16, 17) which have shown that over 53% of CRH care was delivered at MS-CBOCs with CRH’s overall intention and focus being to serve such under-resourced CBOCs, many of which are in geographic areas where substantial numbers of Veterans reside but these areas face healthcare professional shortages.15
When we examined the extent of visits among patients who utilized primary care in each quarter, we found that CRH-PC sites, compared to non-program sites, had 48 additional telephone visits per 1000 primary care patients served (+ 9.8%).
This study contributes to several strands of literature. Firstly, it builds upon recent work evaluating VA’s CRH, providing critical quantitative evidence to complement qualitative work suggesting that VA’s CRH facilitated health system resiliency.11 Our comparison of CRH-PC vs. non-CRH-PC sites expands on prior analyses focusing on CRH-only visits30 to strengthen the link between VA’s CRH program and facilitation of primary care visits during the COVID-19 pandemic.
Next, we contribute to the literature on improving access to primary care via telehealth. Similar to prior studies examining primary care visits across all modalities which typically find either no impact or modest impact on overall primary care use,5, 16, 31 we found VA’s CRH-PC to be associated with a modest 3.4% increase in primary care visits across all modalities, a magnitude closely aligned with a recent large-scale study from Israel showing pandemic-driven access to telehealth increased primary care visits by 3.5%.31
Finally, we found that CRH-PC adoption was associated with very modest decreases in the volume of VA ED visits and hospital stays during the pandemic. However, we did not have data on care provided in the community for this study despite the large growth in community care since the MISSION Act. It is possible that patients in CRH sites sought more care at EDs and hospitals outside the VA health care system during the pandemic. Therefore, the impact of CRH adoption on total acute and inpatient utilization is still unclear. Additional studies examining CRH’s impact on non-VA care are needed.
Limitations
There are some limitations of this study. As our study focused on the impact of the CRH-PC program during the COVID-19 pandemic, we did not examine utilization pre-post CRH-PC adoption at sites as we did not have site-specific start dates for CRH. As such, it is possible that some CRH sites continued to adopt CRH-PC post-pandemic onset. Analyses focusing on the association with the specific timing of uptake or penetration of CRH at VA sites would be helpful for further isolating the impact of CRH. Nonetheless, in sensitivity analyses restricting the sample of CRH-PC sites to sites that adopted CRH-PC pre-pandemic (Fig. 5 in the Appendix) or sites that had CRH-PC during the majority of the post-pandemic period (Fig. 6 in the Appendix), we observed very similar results.
Next, an unavoidable methodological limitation in evaluating a population-level intervention is there may have been unobservable factors that influenced outcomes and the adoption of CRH-PC. As such, we leveraged a DiD design which allows for level differences in baseline characteristics across CRH-PC and comparison sites. DiD allows for unobservable reasons for program adoption as long as CRH-PC and comparison sites exhibit parallel trends in outcomes. We first provided evidence that unadjusted trends exhibit parallel outcome trends for CRH-PC and non-CRH-PC sites (Fig. 1), and then in adjusted event study graphs (Fig. 2), we demonstrated that pre-pandemic differences observed between CRH-PC and non-CRH-PC sites were eliminated after covariate adjustment. The stark contrast in differences across CRH-PC and non-CRH-PC sites immediately post-pandemic then strengthened attributability of post-pandemic differences to CRH-PC. Nonetheless, our methods are not able to distinguish between differences in CRH-PC and non-CRH-PC sites unrelated to the CRH program which may have occurred simultaneously with pandemic onset. For example, if CRH-PC sites improved their infrastructure or management in response to the pandemic for reasons unrelated to the CRH program, our analysis cannot disentangle these associations from the associations with the CRH program. Additional studies of CRH will be important to validate our findings.
We also did not study health care utilization that may have occurred outside VA so utilization by patients in CRH and non-CRH sites may have been under-measured. Additional studies are needed to examine the impact of CRH on total outpatient, acute, and inpatient care for each patient. Furthermore, as CRH also provided mental health care and specialty care, our analyses focusing on primary care remain limited in scope. Future work should also examine CRH’s impact on these other types of care. Finally, our results may not readily generalize to all types of telehealth programs or to non-VA settings.
CONCLUSION
VA’s pre-pandemic rollout of the Clinical Resource Hub telehealth program for primary care intended to improve health care access at under-resourced clinics facilitated primary care during the pandemic, a period fraught with care disruptions and limited in-person health care delivery. Telehealth may be an important strategy to maintain access to care and offer health system resilience during times of crises.
Data Availability
Data cannot be shared publicly because of VA policies regarding data privacy and security. Data contain potentially identifying and sensitive patient information. All relevant de-identified data are included in the manuscript. For investigators with appropriate authorizations within the Department of Veterans Affairs, contact HERC@va.gov or VINCI@va.gov for more information about accessing data.
References
Haldane V, Morgan GT. From resilient to transilient health systems: the deep transformation of health systems in response to the COVID-19 pandemic. Health Policy Plan. 2021;36(1):134-135. https://doi.org/10.1093/heapol/czaa169.
Mustafa S, Zhang Y, Zibwowa Z, et al. COVID-19 Preparedness and Response Plans from 106 countries: a review from a health systems resilience perspective. Health Policy Plan. 2022;37(2):255-268. https://doi.org/10.1093/heapol/czab089.
Rural Telehealth Evaluation Center. Telehealth: current definitions and future trends. 2022. https://idhi.uams.edu/rtec/wp-content/uploads/sites/4/2022/05/Telehealth-Definitions-Paper-06MAY2022-1.pdf. Accessed April 6, 2023.
Yang TY. Telehealth Parity Laws. Health Affairs (Project Hope). 2016.
Chen K, Zhang C, Gurley A, Akkem S, Jackson H. Primary care utilization among telehealth users and non-users at a large urban public healthcare system. Cubo Delgado E, ed. PLoS ONE. 2022;17(8):e0272605. https://doi.org/10.1371/journal.pone.0272605.
Bhaskar S, Bradley S, Chattu VK, et al. Telemedicine across the globe-position paper from the COVID-19 pandemic health system Resilience PROGRAM (REPROGRAM) International Consortium (Part 1). Front Public Health. 2020;8:556720. https://doi.org/10.3389/fpubh.2020.556720 .
Hassankhani M, Alidadi M, Sharifi A, Azhdari A. Smart city and crisis management: lessons for the COVID-19 pandemic. IJERPH. 2021;18(15):7736. https://doi.org/10.3390/ijerph18157736.
Lamberti-Castronuovo A, Valente M, Barone-Adesi F, Hubloue I, Ragazzoni L. Primary health care disaster preparedness: a review of the literature and the proposal of a new framework. Int J Disast Risk Reduct. 2022;81:103278. https://doi.org/10.1016/j.ijdrr.2022.103278.
Bhaskar S, Bradley S, Chattu VK, et al. Telemedicine as the new outpatient clinic gone digital: position paper from the pandemic health system REsilience PROGRAM (REPROGRAM) International Consortium (Part 2). Front Public Health. 2020;8:410. https://doi.org/10.3389/fpubh.2020.00410.
Lurie N, Carr BG. The role of telehealth in the medical response to disasters. JAMA Intern Med. 2018;178(6):745. https://doi.org/10.1001/jamainternmed.2018.1314.
Cannedy S, Bergman A, Medich M, Rose DE, Stockdale SE. Health system resiliency and the COVID-19 pandemic: a case study of a new nationwide contingency staffing program. Healthcare. 2022;10(2):244. https://doi.org/10.3390/healthcare10020244.
Arsenault C, Gage A, Kim MK, et al. COVID-19 and resilience of healthcare systems in ten countries. Nat Med. 2022;28(6):1314-1324. https://doi.org/10.1038/s41591-022-01750-1.
Fleming P, O’Donoghue C, Almirall-Sanchez A, et al. Metrics and indicators used to assess health system resilience in response to shocks to health systems in high income countries—a systematic review. Health Policy. 2022;126(12):1195-1205. https://doi.org/10.1016/j.healthpol.2022.10.001.
VA Health Services Research & Development. Spotlight on Telehealth. Published 2020. https://www.hsrd.research.va.gov/news/feature/telehealth-0720.cfm. Accessed September 21, 2022.
Burnett K, Stockdale S, Yoon J, et al. The Clinical Resource Hub initiative: first year implementation of the Veterans Health Administration regional telehealth contingency staffing program. J Ambul Care Manag. 2023.
Gujral K, Scott JY, Ambady L, et al. A primary care telehealth pilot program to improve access: associations with patients’ health care utilization and costs. Telemedicine and e-Health. 2022;28(5):643-653. https://doi.org/10.1089/tmj.2021.0284.
Oh A, Scott JY, Chow A, et al. Rural and urban differences in the implementation of Virtual Integrated Patient‐Aligned Care Teams. J Rural Health. 2023;39(1):272-278. https://doi.org/10.1111/jrh.12676.
Bokolo A Jr. Exploring the adoption of telemedicine and virtual software for care of outpatients during and after COVID-19 pandemic. Ir J Med Sci. 2021;190(1):1-10. https://doi.org/10.1007/s11845-020-02299-z.
Chami N, Shah HA, Nastos S, et al. Association between virtual primary care and emergency department use during the first year of the COVID-19 pandemic in Ontario, Canada. CMAJ. 2023;195(3):E108-E114. https://doi.org/10.1503/cmaj.212051.
Xu S, Glenn S, Sy L, et al. Impact of the COVID-19 pandemic on health care utilization in a large integrated health care system: Retrospective Cohort Study. J Med Internet Res. 2021;23(4):e26558. https://doi.org/10.2196/26558.
O’Shea AMJ, Haraldsson B, Shahnazi AF, et al. A novel gap staffing metric for primary care in the Veterans Health Administration and Implications for Rural and Urban Clinics. J Ambul Care Manag. 2023;46(1):25-33. https://doi.org/10.1097/JAC.0000000000000429.
VIREC. VA Information Resource Center. https://vaww.virec.research.va.gov/CDW/Overview.htm#FAQs. Accessed March 19, 2021.
Managerial Cost Accounting Office (MCAO). National Data Extracts & Reporting Information. National Data Extracts & Reporting Information. http://vaww.dss.med.va.gov/nationalrptg/nr_extracts.asp. Accessed April 18, 2023.
The New York Times. Coronavirus (Covid-19) Data in the United States. https://github.com/nytimes/covid-19-data. Published June 2021.
Geospatial Service Support Center Home. Geospatial Service Support Center Home. https://vaww.va.gov/GSSC/index.asp. Accessed April 18, 2023.
Wing C, Simon K, Bello-Gomez RA. Designing difference in difference studies: best practices for public health policy research. Ann Rev Public Health. 2018;39:453-469.
Goodman-Bacon A. Difference-in-differences with variation in treatment timing. J Econ. 2021;225(2):254-277.
Sun L, Abraham S. Estimating dynamic treatment effects in event studies with heterogeneous treatment effects. J Economet. 2020.
Freyaldenhoven S, Hansen C, Shapiro JM. Pre-event Trends in the panel event-study design. Am Econ Rev. 2019.
Leung LB, Rubenstein LV, Jaske E, Wheat CL, Nelson KM, Felker BL. Contrasting care delivery modalities used by primary care and mental health specialties in VA’s telehealth contingency staffing program during the COVID-19 pandemic. J Gen Intern Med. 2022;37(10):2607-2610. https://doi.org/10.1007/s11606-022-07527-z.
Zeltzer D, Einav L, Rashba J, Balicer R. The impact of increased access to telemedicine. National Bureau of Economic Research; 2021:w28978. https://doi.org/10.3386/w28978.
Funding
This work was funded by the Primary Care Analytics Team though the Veterans Healthcare Administration (VHA) Office of Primary Care for the purposes of quality improvement; therefore, no IRB approval was obtained. Funding for the Clinical Resource Hub (CRH) program was provided by the VHA Office of Rural Health.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclaimer
The funders were not involved in the design and conduct of the study, interpretation of the data, preparation, and review of this manuscript, nor had a role in the decision to submit the manuscript for publication. We are also grateful for our discussions with Adam Chow, BA, Chelle L. Wheat, PhD, and Steve Fihn, MD, MPH about this manuscript.
Conflict of Interest
The authors have no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gujral, K., Scott, J.Y., Dismuke-Greer, C.E. et al. The Clinical Resource Hub Telehealth Program and Use of Primary Care, Emergency, and Inpatient Care During the COVID-19 Pandemic. J GEN INTERN MED 39 (Suppl 1), 118–126 (2024). https://doi.org/10.1007/s11606-023-08476-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-023-08476-x