
Abstract
Background
Healthcare systems are increasingly implementing programs for high-need patients, who often have multiple chronic conditions and complex social situations. Little, however, is known about quality indicators that might guide healthcare organizations and providers in improving care for high-need patients. We sought to conduct a systematic review to identify potential quality indicators for high-need patients.
Methods
This systematic review (CRD42020215917) searched PubMed, CINAHL, and EMBASE; guideline clearing houses ECRI and GIN; and Google scholar. We included publications suggesting, evaluating, and utilizing indicators to assess quality of care for high-need patients. Critical appraisal of the indicators addressed the development process, endorsement and adoption, and characteristics, such as feasibility. We standardized indicators by patient population subgroups to facilitate comparisons across different indicator groups.
Results
The search identified 6964 citations. Of these, 1382 publications were obtained as full text, and 53 studies met inclusion criteria. We identified over 1700 quality indicators across studies. Quality indicator characteristics varied widely. The scope of the selected indicators ranged from detailed criterion (e.g., “annual eye exam”) to very broad categories (e.g., “care coordination”). Some publications suggested disease condition–specific indicators (e.g., diabetes), some used condition-independent criteria (e.g., “documentation of the medication list in the medical record available to all care agencies”), and some publications used a mixture of indicator types.
Discussion
We identified and evaluated existing quality indicators for a complex, heterogeneous patient group. Although some quality indicators were not disease-specific, we found very few that accounted for social determinants of health and behavioral factors. More research is needed to develop quality indicators that address patient risk factors.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
BACKGROUND
High-need patients are defined as those who represent a considerable challenge for healthcare delivery organizations. This population is considerably heterogeneous due to the different ways this population can be defined. “High-need” may refer to the complexity created by medical conditions interacting with comorbid psychiatric and/or substance use disorder.1 It may also refer to frailty and multimorbidity, for example elderly, patients with multiple medical conditions or those who require higher levels of nursing assistance.2 Furthermore, social determinants of health concurrently exacerbate the health of these patients and contribute to the difficulties in their care management.3 Often, these complexities lead to frequent, high utilization of the healthcare system, often in ways that are considered low value from the standpoint of the healthcare system or insurance payer.4 Furthermore, this heterogeneity contributes to unclear goals and outcomes related to the high-needs patient as well as lack of knowledge regarding effective processes or models of care.
Much of the difficulty in developing models of care for high-needs patients is that the typical biomedical model of disease and treatment is by itself inadequate to address their comorbidities, as it fails to capture not only the synergistic interplay of medical comorbidities but also the contextual factors of a patient.5 High-needs patients by definition do not fit into the traditional model due to their comorbidity across multiple types of determinants, which can include medical, psychiatric, social, behavioral and functional limitations. Health problems across these domains do not function in a vacuum but instead can be compounding and serve to complicate the care of other illnesses, an obvious example of this being the patient with depression and diabetes who experiences difficulty with diabetic medication compliance due to their psychiatric symptoms.
The ongoing failure to develop effective models of care for high-needs patients is in part due to a lack of evidence-based guidelines regarding the optimal approach to this heterogeneous population. While quality indicators are well established and readily available for individual medical conditions, those for complex (and high-need patients) are notably scarce and, moreover, have a poor evidence-base. In order to reduce healthcare expenditures of high-cost, high-need patients and to simultaneously increase quality of care for this population, first we need to establish proven indicators that signal quality care of complex, high-needs patients.6 Thus, the purpose of our systematic review was to examine the literature to describe quality indicators for the care of complex, high-needs patients, which could in turn be used as a reference for physicians seeking to improve assessment and delivery of care for this heterogeneous population.
METHODS
The systematic review followed a detailed protocol, reporting follows PRISMA guidance, and the review is registered in PROSPERO (CRD42020215917). The results of the evidence review informed a RAND Appropriateness Panel to establish quality indicators for high-need patients.
Searches
The systematic review required a carefully designed search strategy given the diverse terminology and definitions used to describe complex, high-need patients in the literature. The search was conducted by a systematic review reference librarian with input from content experts to identify appropriate search terms to identify complex, high-needs patients. The search strategy is documented in the Appendix.
We searched PubMed, CINAHL, EMBASE, Cochrane Database of Systematic Reviews, and PROSPERO from database inception through July 2020. In addition, we searched Google, Google Scholar, and the guideline clearing houses ECRI and GIN for published practice guidelines for high-need patients using the search terms high-needs, complex, high-cost, high utilizers (services or cost), super users, high-risk, and multi-morbid patients.
Eligibility Criteria
Two independent reviewers (MB, KS, SH, TS) screened the search output. All citations deemed relevant by at least one reviewer were obtained as full text. Full-text publications were screened by two reviewers against the eligibility criteria and discrepancies were resolved through discussion (MB, KS, SH, TS). Studies meeting these criteria were eligible for inclusion in the review:
-
Population:
-
We accepted the authors’ definition of high-needs patients. Given that there is no consensus for the nomenclature, we included studies that described frequent user, high attenders, high utilizers, complex patients, high cost patients, and multi-morbid patients/patients with comorbidities or multiple chronic conditions. We included high-need patients of all ages. Older age was not used as an indicator of high-need but qualifiers such as frail elderly were included.
-
-
Quality indicators
-
We included potential quality indicators as suggested by the authors. Quality indicators could encompass care processes-related measures (e.g., follow-up post discharge, continuity of care, medication errors), heath services utilization measures (e.g., hospital readmission, emergency department visit), care satisfaction (e.g., patient satisfaction, care needs met, trust in care provider), and health outcomes (e.g., mortality, physical functional status, mental functioning, quality of life).
-
Indicators specific to only one clinical condition were excluded (e.g., a set of quality indicators for depression treatment was not eligible). We also excluded quality indicators specific to antenatal care and those exclusively addressing end-of-life care.
-
-
Study design
-
We included publications that explicitly suggested quality of care indicators. These encompassed publications suggesting quality indicators based on expert consensus identified in a consensus finding process; suggestions from individual authors were excluded. We also included publications reporting empirical data on quality indicators (e.g., studies assessing whether a set of quality of care indicators has been met). We also included publications that set out to evaluate quality of care for patients and that used indicators designed for the study or previously developed indicators. In addition, publications that evaluated the validity of potential quality indicators, e.g., by documenting the presence or absence of evidence that the indicator was useable, or by providing other measurement characteristics (e.g., reliability or rater agreement for the indicator) were eligible.
-
Studies reporting on the effect of an intervention on patients without clear mention of evaluating the quality of care were excluded. Publications only reporting examples of quality indicators were also excluded. Care guidelines without explicit quality of care indicators and systematic reviews were retained as background and used for reference mining.
-
-
Other limiters
Publications were limited to English language publications and full-text publications. Quality indicators were collected to support an Appropriateness Panel and the language restriction was implemented to ensure timely delivery of the review and transparency for panelists evaluating the indicators. Publications in abbreviated format were excluded (e.g., conference abstracts).
All inclusion screening decisions were documented in citation management software.
Data Abstraction
The data abstraction used detailed, pilot-tested forms in an online software for systematic reviews. Data abstraction focused on study characteristics necessary to understand and evaluate the publications’ results. The data extraction included author and year, multiple publications with additional information on the specific set of quality indicators (where available), type of study (consensus guideline or empirical study to suggest indicators, empirical study to evaluate a proposed indicator), the number and type of stakeholders involved in development of indicators, consensus method, all suggested indicators (label and brief description), number and type of high-need patients in empirical studies testing quality indicators, and evidence for suggested indicators (presence and absence of supporting evidence). Data were abstracted by one reviewer (KS, JS, MB) and checked by an experienced systematic reviewer and a content expert (SH, TS).
We standardized the indicators to the extent possible by translating the indicators into labels followed by a description. Each label started with the care process of action (e.g., “Complex health care needs documentation”). More details about the process were added in parentheses, and timing information was moved to the end of the indicator (e.g., “annual foot exam” changed to “foot exam annually”) to facilitate comparisons across indicator sets and author groups.
Analysis
We summarized quality indicators in a narrative synthesis. All included studies were documented in a detailed evidence table to allow a concise overview. We analyzed the frequency of indicators across the different indicator sets. Studies were categorized by setting, age group, and patient characteristics to illustrate differential populations among those included in the literature review.
Critical Appraisal
We used a published tool relevant to quality of care indicators.7,8 Critical appraisal domains included stakeholder involvement and use of empirical evidence in establishing the quality indicators. Stakeholder involvement was operationalized as three items (Item 1.1: The group developing the indicator includes individuals from relevant professional groups; Item 1.2: Considering the purpose of the indicator, all relevant stakeholders have been involved at some stage of the development process; Item 1.3: The indicator has been formally endorsed). The domain Scientific evidence was also operationalized as three items (Item 2.1: Systematic methods were used to search for scientific evidence; Item 2.2: The indicator is based on recommendations from an evidence-based guideline; Item 2.3: The supporting evidence has been critically appraised). The third domain; Additional evidence, formulation, and usage; included nine items addressing the feasibility, reliability, and validity of the indicators (Item 3.1: The numerator and denominator are described in detail; Item 3.2: The target patient population of the indicator is defined clearly; Item 3.3: A strategy for risk adjustment has been considered and described; Item 3.4: The indicator measures what it is intended to measure (validity); Item 3.5: The indicator measures accurately and consistently (reliability); Item 3.6: The indicator has sufficient discriminative power; Item 3.7: The indicator has been piloted in practice; Item 3.8: The efforts needed for data collection have been considered; Item 3.9: Specific instructions for presenting and interpreting the indicator results are provided).
Synthesis and Quality of Evidence
The quality of evidence assessment for each condition-unspecific indicator is documented in a summary of findings table. To be included in the summary table, indicators had to have been described in at least five identified studies given the large number of suggested indictors. The assessment took into account the following: the number of studies that used the indicator, the critical appraisal results regarding developing the indicator, applying the indicator in practice, and the evidence supporting the indicator. We used the GRADE categories High, Moderate, Low, and Very low to describe the quality of evidence for the indicators across studies.9High quality of evidence would indicate the indicator has been shown to reliably identify outcomes for the care of high-need patients (e.g., differentiate from other patients). Moderate quality of evidence was reserved for indicators have been tested in practice and that have shown some discriminant validity in so far that there was variation in the study sample (not everyone met the criterion, the indicator can distinguish between high and low need). Low quality of evidence was given when one of the criteria was not met (e.g., criteria to establish the indicator, to apply the indicator, or evidence for the content of the indicator). Very low quality of evidence was reserved for indicators where multiple criteria were not met.
RESULTS
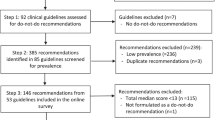
The search identified 6964 citations. Of these, 1382 publications were obtained as full text, and 53 studies reported in 70 publications met inclusion criteria.10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79 Although we searched without date restriction, the earliest included study was published in 2004.28 Of these, 39 (74%) were based in the USA, 14 (26%) were international. The list of excluded studies and the reasons for exclusion are documented in Appendix 2. In addition, Appendix 3 shows the list of background publications that were used to identify additional studies and publications. The diagram (Fig. 1) documents the literature flow.

Literature flow diagram.
The evidence table in the appendix provides an overview of all included studies (Supplementary Appendix 4). The branch diagram in Figure 2 displays the distribution of the 53 included studies across population subgroups as defined by types and combinations of comorbidities. Figure 2 illustrates the differential amount of evidence between different quality indicators based on how specifically the population was defined. The studies were categorized by (1) care setting: community dwelling (48 Citations), hospitalized (3 Citations), and home-bound (2 Citations) as well as by (2) age: children (5 Citations), adults (29 Citations), and elderly (19 Citations). In addition, we categorized the studies by the theme of the complexity defined. These themes included medical comorbidity (45 Citations); psychological/mental comorbidity (15 Citations); behavioral comorbidity (6 Citations), (including addiction); social needs (8 Citations), (including poverty, housing insecurity, food insecurity), functional limitation/decline (21 Citations), (including dementia, loss of mobility) and those only definable by utilization as high utilization (14 Citations). These latter patient characteristics were only applied to the community-dwelling populations, as specific characteristic descriptions were not available for the home-bound and hospitalized population manuscripts.

Distribution of literature among subpopulations.
In total, 1703 individual quality indicators have been suggested across identified studies. The indicators are displayed in alphabetical order in Appendix 6. The scope of the selected indicators ranged from detailed criteria (e.g., HgA1c < 6.5%) to very broad categories (e.g., “care coordination”). Identified indicators also ranged from treatment recommendations to explicit scoring criteria to determine whether quality standards were met (Fig. 3). Some studies described condition-specific indicators relevant to patient subgroups (“in patients with diabetes, assess…”), some used exclusively condition-independent criteria (e.g., “documentation of the medication list in the medical record available to all care agencies”), and some sets of indicators used a mixture of indicator types. Some studies documented broad domains under which they categorized individual quality indicators. Figure 4 provides an overview of the eight domains this review found in the included studies, organized by broad groupings. Distinct domains included disease and symptoms, delivery of care, outcomes, prevention, collaboration/coordination, patient engagement, access to care, and patient safety.

Critical appraisal.

Quality indicator domains.
The summary of findings table (Table 1) provides an overview of the quality of evidence supporting the most frequently suggested quality indicators. The table displays the indicators, supporting evidence, and the GRADE score. All identified indicators ranged between Moderate and Low quality of evidence. Hospital continuity of care (including discharge planning and follow-up) and hospitalization-related indicators such as readmission rates were included in most studies (16 and 15, respectively). Furthermore, other indicators involved starting or monitoring medications, patient assessments and screenings, new symptom or disease follow-up and treatment, safety and preventive medicine, and documentation.
Figure 3 provides an overview of the critical appraisal assessment across studies.
Studies varied in their methodological rigor. Half (49%) of the studies provided clear definitions of the target populations of high-need patients. Very few studies included any indicators that had been formally endorsed (16%) or were based on recommendations from evidence-based guidelines (11%), although some used systematic methods to search for scientific evidence (29%). Some studies included indicators that had already been piloted (31%). Few studies documented risk adjustments for indicators. Ratings of the individual studies are shown in the table in the appendix (Supplementary Appendix 5: Critical Appraisal).
The evidence table (Supplementary Appendix 4) describes the difference in approaches to quality indicator development. Approaches included quality indicator proposals (e.g., following a consensus process), evaluation of existing quality indicators (e.g., evaluating which quality indicators could be assessed in chart review), or use of quality indicators to document quality of care (e.g., to test the effect of an intervention on care quality). Some studies provided detailed information about the development process of the quality of care indicators, while other studies included indicators that had never been used in practice. Studies varied widely in their reporting of validity and reliability of proposed indicators and not all provided evidence that the indicators are measuring what they are supposed to measure, i.e., care quality.
DISCUSSION
We identified and evaluated existing quality indicators in an effort to support healthcare organizations, clinicians, and patients to ensure that quality of care is assessed and quantified in this heterogeneous patient group. Many quality indicators were specific, identifiable, and externally valid as demonstrated in multiple pilot and validity studies. However, overall, the large quantity of widely varied quality indicators in this review clearly demonstrates a lack of consensus to guide studies that attempt to measure care delivered to high-needs patients.
Our review of the studies that suggested, used, or evaluated quality indicators in high-needs populations produced an astounding 1703 indicators. Even more astonishing is that while there was conceptual overlap across studies and quality indicators, there were notably very few true duplicate quality indicators.
Overall, our findings in this systematic review reflect the challenging heterogeneity of this population and the extraordinary amount of unique indicators found through our review appears to represent a failure of consensus of key quality of care measures that can be applied specifically to all high-needs patients. This failure is important in its own right in that it demonstrates not only the state of the literature, but also likely demonstrates the need for a novel approach to forming expert consensus of quality indicators to be used in measuring care delivered to this population. Several observations can be made that point out uniquely neglected subset populations that represent potential areas to advance quality indicators. While we found no sets of criteria from organizations such as CMS and the National Quality Forum for this patient group, there are select examples of successful quality indicator frameworks (e.g., ACOVE) applied to well-defined subset populations within the larger, more varied cohort of high-needs patients.
Among age- and setting-based populations displayed in Figure 2, community-dwelling adults and elderly constituted the majority of the literature, representing 28 and 15 studies, respectively. There were few home-bound (2 total, 1 adult, 1 elderly) and hospitalized (3 elderly) patient population articles. The literature pertaining to complex children was small (5 Citations) and represented a myriad of quality indicators among diverse populations within children, yielding little congruence among indicators. This was partially due to the way the high-needs child was defined, with several of the studies focused on complexity as defined by experts, others with complexity based on tertiary and quaternary care (e.g., congenital diseases), another focused on high utilization among asthma with depression/anxiety, and the last manuscript looking broadly at high utilization as compared to the general pediatric populations.
Across the various age and setting subpopulations, further subcategorizations were found to define high-needs patients. Among the community-dwelling population, some were specified by high utilization (14 total, 4 adult, 4 children, 6 elderly) and others used comorbidity-based definitions. These overlapping comorbidity subgroups included categories of medical (26 adult, 5 children, 14 elderly), psychological/mental (12 adult, 3 children, 0 elderly), behavioral (5 adult, 1 children, 0 elderly), social (7 adult, 0 children, 1 elderly), and functional limitation/decline (9 adult, 4 children, 8 elderly). These various categories not only delineate different quality indicators, but also differ in the level of evidence supporting the measures of quality. The frequency of manuscripts pertaining to these subgroupings illustrates some of the disparity in the quantity of evidence among the different populations—especially the lack of focus on patient characteristics that are not medical comorbidities.
The most frequently represented and rigorously supported quality indicators exist in the medically comorbid adult and elderly populations, centered on several iterations of the Assessing Care of Vulnerable Elderly Study (ACOVE) and their subsequent application in other populations. This original study developed quality measures specifically devoted to the vulnerable elderly defined as those most likely to die or become severely disabled in the next two years. This study created an impetus for development of substantial further examination into quality of care among the vulnerable elderly. This development is evidenced by the predominance of quality indicators from ACOVE studies in the quality of evidence table with basic care coordination indicators, such as “hospital continuity of care, discharge planning and follow-up after inpatient stay” and “hospitalization (appropriate vs inappropriate including readmissions)” (Table 1). Nonetheless, despite some concordance among the most common indicators in the quality of evidence table, most indicators reached only moderate quality of evidence based on GRADE criteria, with several of low quality. This embodies the opportunity to improve measurement of quality within the broader high-needs population other than the frail elderly quality indicators developed by ACOVE.
Quality indicators that had enough concordance to meet the criteria for the quality of evidence table (Table 1) included condition-specific screening measures (vision screening, blood pressure screening), prevention measures (fall prevention, stroke prevention), treatment measures (aspirin use, beta-blocker offered in heart failure,), behavioral interventions (smoking cessation counseling), and documentation measures (weight documented, alcohol/substance use intake documentation, constipation documentation). These represented consistent primary care–related quality indicators that substantially overlap with United States Prevention and Screening Task Force items, particularly regarding prevention and screening.80,81
While there was substantial evidence for quality indicators specific to the frail elderly (ACOVE) and for disease-specific measures, there was an absence of evidence surrounding quality indicators for patients with serious mental illness (e.g., schizophrenia), social, and behavioral comorbidities and those defined solely by high utilization. These patients remain extremely challenging for the healthcare system, and yet there are few attempts to evaluate care delivery in the quality indicators literature.
There is a lack of consensus across the literature as to how the high-needs population should be defined, and this creates a lack of comparability, lowering the external validity of each of the quality indicators due to unclear population concordance.6 The fundamental challenge of defining the high-needs population exists in the great diversity of comorbidities and contextual contributors that lead them to be high utilizers of the healthcare system. The comorbidity subpopulations in Figure 2 illustrate this diversity and the lack of robust evidence, apart from the adult and elderly population with medical comorbidities. The majority of the literature furthermore tends to focus on a single or few disease conditions (e.g., diabetes and hypertension) rather than patients with comorbidities across many subgroups (e.g., diabetes with bipolar disorder, homelessness, and substance use). This bias leads to quality indicators addressing patients with several medical conditions, which does not adapt well to patients with complex biopsychosocial needs.
Care models to address social and behavioral determinants of health have developed over the last decade in other literature, utilizing programs that involve interprofessional teams, intensive care coordination, and necessary restructuring of care delivery.82,83,84,85,86 These programs share the recognition that the high-need patients, though belonging to a wide range of etiologies of their utilization, are similar in that they do not fit into the current medical infrastructure. Despite forays into treatment regimens and new models of care to approach this population, lack of development of quality indicators continues to hamstring providers and health systems in improvement of outcomes among the most difficult to treat high utilizers.
Our review had several limitations. First, our search strategy was purposefully broad in order to capture all quality indicators being suggested, used, or evaluated in patients who could be considered high-needs to avoid reliance on authors’ use of identical terminology. This approach led to a highly sensitive catchment of both quality indicators and high-needs populations and provides a comprehensive analysis of the quality indicators currently utilized internationally in the delivery of medical care to high-needs patients. However, this methodology results in many of the quality indicators being disease-specific (e.g., glucose monitoring for diabetes) and not necessarily exclusive to the high-needs patient. In addition, we restricted to English language studies, which may have missed important indicators, in particular those in other cultures. Furthermore, we also note that our quality of evidence assessment was not based on standard GRADE criteria. We designed criteria relevant to assess the quality of evidence for the proposed quality indicators, which future research should replicate or develop further.
To improve quality indicators and their application, we need to better define and more specifically apply quality indicators according to the varying profiles of high-need patients. Development of quality indicators among high-needs patients may benefit from following the success of the ACOVE literature, which succeeded in large part due to its focus on a specific sub population. Other subpopulations of high-needs patients need a similarly focused quality indicator infrastructure to be rigorously developed in order to maximize efficacy and clinician relevance. Finally, patients with social and behavioral comorbidities require prompt study, as they lag behind the other subpopulations of high-needs patients in the quality indicator literature.
References
Valderas JM, Starfield B, Sibbald B, Salisbury C, Roland M. Defining comorbidity: implications for understanding health and health services. Ann Fam Med. 2009;7(4):357-63. https://doi.org/10.1370/afm.983
Buja A, Claus M, Perin L, Rivera M, Corti MC, Avossa F, et al. Multimorbidity patterns in high-need, high-cost elderly patients. PLoS One. 2018;13(12):e0208875. https://doi.org/10.1371/journal.pone.0208875
Schickedanz A, Sharp A, Hu YR, Shah NR, Adams JL, Francis D, et al. Impact of Social Needs Navigation on Utilization Among High Utilizers in a Large Integrated Health System: a Quasi-experimental Study. J Gen Intern Med. 2019;34(11):2382-9. https://doi.org/10.1007/s11606-019-05123-2
Wammes JJG, van der Wees PJ, Tanke MAC, Westert GP, Jeurissen PPT. Systematic review of high-cost patients’ characteristics and healthcare utilisation. BMJ Open. 2018;8(9):e023113. https://doi.org/10.1136/bmjopen-2018-023113
Hochman M, Asch SM. Disruptive Models in Primary Care: Caring for High-Needs, High-Cost Populations. J Gen Intern Med. 2017;32(4):392-7. https://doi.org/10.1007/s11606-016-3945-2
Long P, Abrams M, Milstein A, Anderson G, Apton KL, Dahlberg ML, et al. Effective Care for High-Need Patients: Opportunities for Improving Outcomes, Value, and Health. Washington, DC: National Academy of Medicine 2017.
De Roo ML, Leemans K, Claessen SJ, Cohen J, Pasman HR, Deliens L, et al. Quality indicators for palliative care: update of a systematic review. J Pain Symptom Manage. 2013;46(4):556-72. https://doi.org/10.1016/j.jpainsymman.2012.09.013
De Koning J, Burgers JS, Klazing N. Appraisal of Indicators through Research and Evaluation (English version based on original Dutch version 2.0). Amsterdam: University of Amsterdam 2007.
Balshem H, Helfand M, Schunemann HJ, Oxman AD, Kunz R, Brozek J, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-6. https://doi.org/10.1016/j.jclinepi.2010.07.015
ACOVE. Assessing care of vulnerable elders-3 quality indicators. J Am Geriatr Soc. 2007;55 Suppl 2:S464-87. https://doi.org/10.1111/j.1532-5415.2007.01329.x
Universal health outcome measures for older persons with multiple chronic conditions. J Am Geriatr Soc. 2012;60(12):2333-41. https://doi.org/10.1111/j.1532-5415.2012.04240.x
Complex Care Management Guidelines. Michigan Center for Clinical Systems Improvement; 2015. p. 1-28.
Ajmera M, Wilkins TL, Findley PA, Sambamoorthi U. Multimorbidity, Mental Illness, and Quality of Care: Preventable Hospitalizations among Medicare Beneficiaries. Int J Family Med. 2012;2012:823294. https://doi.org/10.1155/2012/823294
Arora VM, Fish M, Basu A, Olson J, Plein C, Suresh K, et al. Relationship between quality of care of hospitalized vulnerable elders and postdischarge mortality. J Am Geriatr Soc. 2010;58(9):1642-8. https://doi.org/10.1111/j.1532-5415.2010.03024.x
Bayliss EA, McQuillan DB, Ellis JL, Maciejewski ML, Zeng C, Barton MB, et al. Using Electronic Health Record Data to Measure Care Quality for Individuals with Multiple Chronic Medical Conditions. J Am Geriatr Soc. 2016;64(9):1839-44. https://doi.org/10.1111/jgs.14248
Cheak-Zamora NC, Thullen M. Disparities in Quality and Access to Care for Children with Developmental Disabilities and Multiple Health Conditions. Matern Child Health J. 2017;21(1):36-44. https://doi.org/10.1007/s10995-016-2091-0
Chen AY, Schrager SM, Mangione-Smith R. Quality measures for primary care of complex pediatric patients. Pediatrics. 2012;129(3):433-45. https://doi.org/10.1542/peds.2011-0026
Domino ME, Beadles CA, Lichstein JC, Farley JF, Morrissey JP, Ellis AR, et al. Heterogeneity in the quality of care for patients with multiple chronic conditions by psychiatric comorbidity. Med Care. 2014;52 Suppl 3:S101-9. https://doi.org/10.1097/mlr.0000000000000024
DuBard CA, Jacobson Vann JC, Jackson CT. Conflicting Readmission Rate Trends in a High-Risk Population: Implications for Performance Measurement. Popul Health Manag. 2015;18(5):351-7. https://doi.org/10.1089/pop.2014.0138
DuGoff EH, Boyd C, Anderson G. Complex Patients and Quality of Care in Medicare Advantage. J Am Geriatr Soc. 2020;68(2):395-402. https://doi.org/10.1111/jgs.16236
DuGoff EH, Dy S, Giovannetti ER, Leff B, Boyd CM. Setting standards at the forefront of delivery system reform: aligning care coordination quality measures for multiple chronic conditions. J Healthc Qual. 2013;35(5):58-69. https://doi.org/10.1111/jhq.12029
Dy SM, Pfoh ER, Salive ME, Boyd CM. Health-related quality of life and functional status quality indicators for older persons with multiple chronic conditions. J Am Geriatr Soc. 2013;61(12):2120-7. https://doi.org/10.1111/jgs.12555
Edelen MO, Rose AJ, Bayliss E, Baseman L, Butcher E, Garcia RE, et al. Patient-Reported Outcome-Based Performance Measures for Older Adults with Multiple Chronic Conditions. Rand Health Q. 2018;8(2):3.
Esposito D, Taylor EF, Gold M. Using qualitative and quantitative methods to evaluate small-scale disease management pilot programs. Popul Health Manag. 2009;12(1):3-15. https://doi.org/10.1089/pop.2008.0037
Eton DT, Linzer M, Boehm DH, Vanderboom CE, Rogers EA, Frost MH, et al. Deriving and validating a brief measure of treatment burden to assess person-centered healthcare quality in primary care: a multi-method study. BMC Fam Pract. 2020;21(1):221. https://doi.org/10.1186/s12875-020-01291-x
Giovannetti ER, Dy S, Leff B, Weston C, Adams K, Valuck TB, et al. Performance measurement for people with multiple chronic conditions: conceptual model. Am J Manag Care. 2013;19(10):e359-66.
Hartmann J, Hehner S, Hemmrich K, Kors B, Mohlmann T. Providing better care at lower cost for multimorbid patients. Health International. 2011;11.
Higashi T, Shekelle PG, Solomon DH, Knight EL, Roth C, Chang JT, et al. The quality of pharmacologic care for vulnerable older patients. Ann Intern Med. 2004;140(9):714-20. https://doi.org/10.7326/0003-4819-140-9-200405040-00011
Hong SI, Morrow-Howell N, Proctor E, Wentz JD, Rubin E. The quality of medical care for comorbid conditions of depressed elders. Aging Ment Health. 2008;12(3):323-32. https://doi.org/10.1080/13607860802121118
Jeffs L, Law MP, Straus S, Cardoso R, Lyons RF, Bell C. Defining quality outcomes for complex-care patients transitioning across the continuum using a structured panel process. BMJ Qual Saf. 2013;22(12):1014-24. https://doi.org/10.1136/bmjqs-2012-001473
Johnston KJ, Hockenberry JM. Are Two Heads Better Than One or Do Too Many Cooks Spoil the Broth? The Trade-Off between Physician Division of Labor and Patient Continuity of Care for Older Adults with Complex Chronic Conditions. Health Serv Res. 2016;51(6):2176-205. https://doi.org/10.1111/1475-6773.12600
Kahn LS, Fox CH, Olawaiye A, Servoss TJ, McLean-Plunkett E. Facilitating quality improvement in physician management of comorbid chronic disease in an urban minority practice. J Natl Med Assoc. 2007;99(4):377-83.
Katon WJ, Richardson L, Russo J, Lozano P, McCauley E. Quality of mental health care for youth with asthma and comorbid anxiety and depression. Med Care. 2006;44(12):1064-72. https://doi.org/10.1097/01.mlr.0000237421.17555.8f
Kistler CE, Van Dongen MJ, Ernecoff NC, Daaleman TP, Hanson LC. Evaluating the care provision of a community-based serious-illness care program via chart measures. BMC Geriatr. 2020;20(1):351. https://doi.org/10.1186/s12877-020-01736-z
Kranz AM, DeYoreo M, Eshete-Roesler B, Damberg CL, Totten M, Escarce JJ, et al. Health system affiliation of physician organizations and quality of care for Medicare beneficiaries who have high needs. Health Serv Res. 2020;55(S3):1118-28. https://doi.org/10.1111/1475-6773.13570
Kroger E, Tourigny A, Morin D, Cote L, Kergoat MJ, Lebel P, et al. Selecting process quality indicators for the integrated care of vulnerable older adults affected by cognitive impairment or dementia. BMC Health Serv Res. 2007;7:195. https://doi.org/10.1186/1472-6963-7-195
Lail J, Fields E, Paolella A, Schoettker PJ. Primary Care Quality Improvement Metrics and National Committee on Quality Assurance Medical Home Recognition for Children With Medical Complexity. Pediatr Qual Saf. 2019;4(6):e231. https://doi.org/10.1097/pq9.0000000000000231
Lauriks S, de Wit MA, Buster MC, Arah OA, Klazinga NS. Composing a core set of performance indicators for public mental health care: a modified Delphi procedure. Adm Policy Ment Health. 2014;41(5):625-35. https://doi.org/10.1007/s10488-013-0506-4
Maxwell CA, Mion LC, Dietrich MS, Fallon WF, Minnick A. Hospitals’ adoption of targeted cognitive and functional status quality indicators for vulnerable elders. J Nurs Care Qual. 2014;29(4):354-62. https://doi.org/10.1097/ncq.0000000000000061
Min L, Kerr EA, Blaum CS, Reuben D, Cigolle C, Wenger N. Contrasting effects of geriatric versus general medical multimorbidity on quality of ambulatory care. J Am Geriatr Soc. 2014;62(9):1714-21. https://doi.org/10.1111/jgs.12989
Long P, Abrams M, Milstein A, Anderson G, Lewis Apton K, Lund Dahlberg M, Whicher D, Editors. Effective Care for High-Need Patients: Opportunities for Improving Outcomes, Value, and Health. Washington, DC: National Academy of Medicine. 2017. Available at: https://nam.edu/wp-content/uploads/2017/06/Effective-Care-for-High-Need-Patients.pdf. Accessed 21 Feb 2022.
National Institute for Health and Care Excellence (NICE). Multimorbidity (QS153)June 29, 2017.
Nouwens E, van Lieshout J, Wensing M. Comorbidity complicates cardiovascular treatment: is diabetes the exception? Neth J Med. 2012;70(7):298-305.
Palmer K, Marengoni A, Forjaz MJ, Jureviciene E, Laatikainen T, Mammarella F, et al. Multimorbidity care model: Recommendations from the consensus meeting of the Joint Action on Chronic Diseases and Promoting Healthy Ageing across the Life Cycle (JA-CHRODIS). Health Policy. 2018;122(1):4-11. https://doi.org/10.1016/j.healthpol.2017.09.006
Parikh PB, Yang J, Leigh S, Dorjee K, Parikh R, Sakellarios N, et al. The impact of financial barriers on access to care, quality of care and vascular morbidity among patients with diabetes and coronary heart disease. J Gen Intern Med. 2014;29(1):76-81. https://doi.org/10.1007/s11606-013-2635-6
Petrosyan Y, Barnsley JM, Kuluski K, Liu B, Wodchis WP. Quality indicators for ambulatory care for older adults with diabetes and comorbid conditions: A Delphi study. PLoS One. 2018;13(12):e0208888. https://doi.org/10.1371/journal.pone.0208888
Pillay M, Dennis S, Harris MF. Quality of care measures in multimorbidity. Aust Fam Physician. 2014;43(3):132-6.
Poitras ME, Maltais ME, Bestard-Denomme L, Stewart M, Fortin M. What are the effective elements in patient-centered and multimorbidity care? A scoping review. BMC Health Serv Res. 2018;18(1):446. https://doi.org/10.1186/s12913-018-3213-8
Rijken M, Hujala A, van Ginneken E, Melchiorre MG, Groenewegen P, Schellevis F. Managing multimorbidity: Profiles of integrated care approaches targeting people with multiple chronic conditions in Europe. Health Policy. 2018;122(1):44-52. https://doi.org/10.1016/j.healthpol.2017.10.002
Ritchie CS, Leff B, Garrigues SK, Perissinotto C, Sheehan OC, Harrison KL. A Quality of Care Framework for Home-Based Medical Care. J Am Med Dir Assoc. 2018;19(10):818-23. https://doi.org/10.1016/j.jamda.2018.05.020
Schiotz ML, Host D, Christensen MB, Dominguez H, Hamid Y, Almind M, et al. Quality of care for people with multimorbidity - a case series. BMC Health Serv Res. 2017;17(1):745. https://doi.org/10.1186/s12913-017-2724-z
Schuttner L, Wong ES, Rosland AM, Nelson K, Reddy A. Association of the Patient-Centered Medical Home Implementation with Chronic Disease Quality in Patients with Multimorbidity. J Gen Intern Med. 2020;35(10):2932-8. https://doi.org/10.1007/s11606-020-06076-7
Sinvani L, Kozikowski A, Smilios C, Patel V, Qiu G, Akerman M, et al. Implementing ACOVE Quality Indicators as an Intervention Checklist to Improve Care for Hospitalized Older Adults. J Hosp Med. 2017;12(7):517-22. https://doi.org/10.12788/jhm.2765
Smith KL, Soriano TA, Boal J. Brief communication: National quality-of-care standards in home-based primary care. Ann Intern Med. 2007;146(3):188-92. https://doi.org/10.7326/0003-4819-146-3-200702060-00008
Strickland BB, Jones JR, Newacheck PW, Bethell CD, Blumberg SJ, Kogan MD. Assessing systems quality in a changing health care environment: the 2009-10 national survey of children with special health care needs. Matern Child Health J. 2015;19(2):353-61. https://doi.org/10.1007/s10995-014-1517-9
The National Committee for Quality Assurance. Policy Approaches to Advancing Person-Centered Outcome Measurement. 2015. Available at: https://www.ncqa.org/wp-content/uploads/2018/07/20150930_Policy_AdvancingPersonCenteredOutcomeMeasurement.pdf. Accessed 21 Feb 2022.
Valderas JM, Gangannagaripalli J, Nolte E, Boyd CM, Roland M, Sarria-Santamera A, et al. Quality of care assessment for people with multimorbidity. J Int Med. 2019;285(3):289-300. https://doi.org/10.1111/joim.12881
van der Ploeg E, Depla MF, Shekelle P, Rigter H, Mackenbach JP. Developing quality indicators for general practice care for vulnerable elders; transfer from US to The Netherlands. Qual Saf Health Care. 2008;17(4):291-5. https://doi.org/10.1136/qshc.2007.023226
Venables D, Reilly S, Challis D, Hughes J, Abendstern M. Standards of care in home care services: a comparison of generic and specialist services for older people with dementia. Aging Ment Health. 2006;10(2):187-94. https://doi.org/10.1080/13607860500310518
Wenger NS, Roth CP, Martin D, Nickels L, Beckman R, Kamberg C, et al. Quality of care provided in a special needs plan using a nurse care manager model. J Am Geriatr Soc. 2011;59(10):1810-22. https://doi.org/10.1111/j.1532-5415.2011.03599.x
Wierenga PC, Klopotowska JE, Smorenburg SM, van Kan HJ, Bijleveld YA, Dijkgraaf MG, et al. Quality indicators for in-hospital pharmaceutical care of Dutch elderly patients: development and validation of an ACOVE-based quality indicator set. Drugs Aging. 2011;28(4):295-304. https://doi.org/10.2165/11587700-000000000-00000
Zingmond DS, Wilber KH, Maclean CH, Wenger NS. Measuring the quality of care provided to community dwelling vulnerable elders dually enrolled in Medicare and Medicaid. Med Care. 2007;45(10):931-8. https://doi.org/10.1097/MLR.0b013e318127143e
Arora VM, Johnson M, Olson J, Podrazik PM, Levine S, Dubeau CE, et al. Using assessing care of vulnerable elders quality indicators to measure quality of hospital care for vulnerable elders. J Am Geriatr Soc. 2007;55(11):1705-11. https://doi.org/10.1111/j.1532-5415.2007.01444.x
Chang JT, Hays RD, Shekelle PG, MacLean CH, Solomon DH, Reuben DB, et al. Patients’ global ratings of their health care are not associated with the technical quality of their care. Ann Intern Med. 2006;144(9):665-72. https://doi.org/10.7326/0003-4819-144-9-200605020-00010
Health Resources & Services Administration (HRSA). Children and Youth with Special Health Care Needs: NSCH Data Brief. 2020. Available at: https://mchb.hrsa.gov/sites/default/files/mchb/Data/NSCH/nsch-cshcn-data-brief.pdf. Accessed 21 Feb 2022.
Higashi T, Wenger NS, Adams JL, Fung C, Roland M, McGlynn EA, et al. Relationship between number of medical conditions and quality of care. N Engl J Med. 2007;356(24):2496-504. https://doi.org/10.1056/NEJMsa066253
Lichtenstein BJ, Reuben DB, Karlamangla AS, Han W, Roth CP, Wenger NS. Effect of Physician Delegation to Other Healthcare Providers on the Quality of Care for Geriatric Conditions. J Am Geriatr Soc. 2015;63(10):2164-70. https://doi.org/10.1111/jgs.13654
MacLean CH, Louie R, Shekelle PG, Roth CP, Saliba D, Higashi T, et al. Comparison of administrative data and medical records to measure the quality of medical care provided to vulnerable older patients. Med Care. 2006;44(2):141-8. https://doi.org/10.1097/01.mlr.0000196960.12860.de
National Guideline Centre (UK). Multimorbidity: Assessment, Prioritisation and Management of Care for People with Commonly Occurring Multimorbidity. London: National Institute for Health and Care Excellence (UK),; 2016.
National Quality Forum. Multiple Chronic Conditions Measurement Framework. 2012. Washington, DC. Available at: https://www.qualityforum.org/Publications/2012/05/MCC_Measurement_Framework_Final_Report.aspx. Accessed 21 Feb 2022.
Opondo D, Visscher S, Eslami S, Medlock S, Verheij R, Korevaar JC, et al. Feasibility of automatic evaluation of clinical rules in general practice. Int J Med Inform. 2017;100:90-4. https://doi.org/10.1016/j.ijmedinf.2017.01.010
Rijken M, Struckmann V, van der Heide I, Richardson E, Van Ginneken E, et al., eds. How to improve care for people with multimorbidity in Europe?. Copenhagen (Denmark): European Observatory on Health Systems and Policies; 2017. https://pubmed.ncbi.nlm.nih.gov/29144712/
Roth CP, Ganz DA, Nickles L, Martin D, Beckman R, Wenger NS. Nurse care manager contribution to quality of care in a dual-eligible special needs plan. J Gerontol Nurs. 2012;38(7):44-54. https://doi.org/10.3928/00989134-20120606-10
Solomon DH, Wenger NS, Saliba D, Young RT, Adelman AM, Besdine RK, et al. Appropriateness of quality indicators for older patients with advanced dementia and poor prognosis. J Am Geriatr Soc. 2003;51(7):902-7. https://doi.org/10.1046/j.1365-2389.2003.513331.x
Strickland BB, van Dyck PC, Kogan MD, Lauver C, Blumberg SJ, Bethell CD, et al. Assessing and ensuring a comprehensive system of services for children with special health care needs: a public health approach. Am J Public Health. 2011;101(2):224-31. https://doi.org/10.2105/AJPH.2009.177915
Wenger NS, Roth CP, Shekelle P. Introduction to the assessing care of vulnerable elders-3 quality indicator measurement set. J Am Geriatr Soc. 2007;55 Suppl 2:S247-52. https://doi.org/10.1111/j.1532-5415.2007.01328.x
Wenger NS, Roth CP, Shekelle P, Investigators A. Introduction to the assessing care of vulnerable elders-3 quality indicator measurement set. J Am Geriatr Soc. 2007;55 Suppl 2:S247-52. https://doi.org/10.1111/j.1532-5415.2007.01328.x
Wenger NS, Solomon DH, Amin A, Besdine RK, Blazer DG, Cohen H, et al. Application of assessing care of vulnerable elders-3 quality indicators to patients with advanced dementia and poor prognosis. J Am Geriatr Soc. 2007;55 Suppl 2:S457-63. https://doi.org/10.1111/j.1532-5415.2007.01375.x
Zingmond DS, Ettner SL, Wilber KH, Wenger NS. Association of claims-based quality of care measures with outcomes among community-dwelling vulnerable elders. Med Care. 2011;49(6):553-9. https://doi.org/10.1097/MLR.0b013e31820e5aab
Siu AL, Force USPST. Screening for high blood pressure in adults: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2015;163(10):778-86. https://doi.org/10.7326/M15-2223
Siu AL, Force USPST, Bibbins-Domingo K, Grossman DC, Baumann LC, Davidson KW, et al. Screening for Depression in Adults: US Preventive Services Task Force Recommendation Statement. JAMA. 2016;315(4):380-7. https://doi.org/10.1001/jama.2015.18392
Madden EF, Kalishman S, Zurawski A, O’Sullivan P, Arora S, Komaromy M. Strategies Used by Interprofessional Teams to Counter Healthcare Marginalization and Engage Complex Patients. Qual Health Res. 2020;30(7):1058-71. https://doi.org/10.1177/1049732320909100
O’Brien CW, Breland JY, Slightam C, Nevedal A, Zulman DM. Engaging high-risk patients in intensive care coordination programs: the engagement through CARInG framework. Transl Behav Med. 2018;8(3):351-6. https://doi.org/10.1093/tbm/ibx004
Carey G, Crammond B. Systems change for the social determinants of health. BMC Public Health. 2015;15:662. https://doi.org/10.1186/s12889-015-1979-8
Zulman DM, O’Brien CW, Slightam C, Breland JY, Krauth D, Nevedal AL. Engaging High-Need Patients in Intensive Outpatient Programs: A Qualitative Synthesis of Engagement Strategies. J Gen Intern Med. 2018;33(11):1937-44. https://doi.org/10.1007/s11606-018-4608-2
Fleming MD, Shim JK, Yen IH, Thompson-Lastad A, Rubin S, Van Natta M, et al. Patient engagement at the margins: Health care providers’ assessments of engagement and the structural determinants of health in the safety-net. Soc Sci Med. 2017;183:11-8. https://doi.org/10.1016/j.socscimed.2017.04.028
Acknowledgements
We thank Lisa Rubenstein and Paul Shekelle for input on the literature searches.
Funding
Funding was provided by the Veterans Health Administration Office of Primary Care XVA 65-54. The views expressed are those of the authors and do not represent the views of the US Department of Veterans Affairs or the US Government.
Author information
Authors and Affiliations
Contributions
TS, MB, JS, EC, KS, JD, EJ, AM, and SH were responsible for study concept and design. TS, EC, MB, KS, JD, and SH were responsible for analysis and interpretation of the data. TS, EC, MB, KS, and SH were responsible for drafting the article. All authors were responsible for critical revision of the article for important intellectual content. TS takes responsibility for the paper as a whole. All authors attest to meeting the four ICMJE.org authorship criteria: (1) Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND (2) Drafting the work or revising it critically for important intellectual content; AND (3) Final approval of the version to be published; AND (4) Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they do not have a conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
PROSPERO Registration
CRD42020215917
This has been presented as a conference abstract at the virtual Academy Health Annual Research Meeting in 2021.
Supplementary Information
ESM 1
(DOCX 1394 kb)
Rights and permissions
About this article

Cite this article
Schneberk, T., Bolshakova, M., Sloan, K. et al. Quality Indicators for High-Need Patients: a Systematic Review. J GEN INTERN MED 37, 3147–3161 (2022). https://doi.org/10.1007/s11606-022-07454-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-022-07454-z