
ABSTRACT
BACKGROUND
To reduce suicides among Veterans, the Department of Veterans Affairs (VA) has designated suicide risk assessments for Veterans who screen positive for depression or post-traumatic stress disorder as a national performance goal. Many VA Medical Centers (VAMCs) are using brief suicidal ideation screens, administered in non-mental health ambulatory care settings, as the first step in the assessment process.
OBJECTIVE
To explore Veterans’ perceptions of the suicide screening and risk assessment process, the barriers and facilitators to disclosing suicidal thoughts, and perceptions of possible consequences of revealing suicidal thoughts.
DESIGN
Investigators recorded one semi-structured interview with each Veteran. Transcripts were analyzed using a modified grounded theory approach.
PARTICIPANTS
Thirty-four Operation Enduring Freedom/Operation Iraqi Freedom (OEF/OIF) Veterans who screened positive for suicidal ideation in non-mental health ambulatory care settings in 2009 and 2010.
KEY RESULTS
Veterans accepted the need to assess suicide risk. They increasingly experienced attempts to suppress and avoid thoughts of suicide as burdensome and exhausting. Despite this, Veterans often failed to disclose severe and pervasive suicidal thoughts when screened because: (1) they considered suicidal thoughts as shameful and a sign of weakness; (2) they believed suicidal thoughts were private and not to be divulged to strangers; (3) they worried that disclosure would lead to unwanted hospitalization or medication recommendations; and (4) the templated computer reminder process was perceived as perfunctory and disrespectful. In contrast, admitting and discussing thoughts of suicide with a health provider who focused on building a relationship, demonstrated genuineness and empathy, offered information on the rationale for suicide risk assessment, and used straightforward and understandable language, all promoted trust that resulted in more honest disclosure of suicidal thoughts.
CONCLUSION
In ambulatory care settings, both provider behaviors and system modifications may lead to more honest disclosure of suicidal thoughts.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
INTRODUCTION
Suicide death among Veterans is a major public health concern.1,2 Up to 6,500 Veterans take their lives each year.3,4 The Department of Veterans Affairs (VA) has taken multiple steps to develop and promote suicide prevention initiatives.5–8 Since 2007, the VA requires all employees to complete suicide prevention training, underscoring the responsibility that all who interact with Veterans have in recognizing signs of suicide. In addition, the VA has designated suicide risk assessment among Veterans who screen positive for depression or post-traumatic stress disorder (PTSD) as a national performance goal.
Brief screening instruments for a variety of conditions are administered routinely across the VA, and are facilitated by a reminder/alert system at the point of care that is embedded in the electronic medical record (EMR).9 Many Veterans Affairs Medical Centers (VAMCs) have chosen to meet the requirement for suicide risk assessment by developing and using brief suicidal ideation screening instruments that are administered by clinicians or clinic staff in mental health and non-mental health settings following positive depression and PTSD. Screening questions, along with patient responses, are stored as text in electronic progress notes. For veterans identified as at risk for suicide on these screens, a more extensive suicide risk assessment is completed, and Veterans are then referred for mental health treatment when appropriate. For screening to be effective, Veterans must find the approach acceptable, useful, and be supported to provide honest answers.
Indeed, evidence suggests that Veterans may be reluctant to endorse questions regarding mental distress or suicide. In a study by Hoge and coauthors,10 only a minority of Veterans returning from Afghanistan and Iraq who screened positive for depression, PTSD or generalized anxiety received professional help―many citing stigma concerns. In a sample of Oregon Veterans who died by suicide, nearly three-quarters who were asked about suicide at their last health care visit denied suicidal thoughts.11 In a study examining psychosocial assessment processes among individuals who had self-harmed, Taylor and coauthors found three factors contributed to a positive experience during the mental health assessment: 1) having ample time to respond; 2) perceived genuineness of the clinician conducting the assessment; and 3) receiving an explanation of the rationale and goals of the assessment.12 Otherwise, little is known regarding the barriers to and facilitators of suicidal ideation disclosure among Veterans in the context of routine screening. In this study, we sought to understand, using qualitative methods, Operation Enduring Freedom/Operation Iraqi Freedom (OEF/OIF) Veteran perceptions of suicide screening and risk assessment process, the barriers and facilitators to disclosing suicidal ideation, and Veteran reactions and perceptions of possible consequences to endorsing suicidal ideation.
METHODS
This study was approved by the Institutional Review Boards of the participating medical centers and all participants gave written informed consent.
Sample and Eligibility Criteria
Eligible participants were OEF/OIF Veterans, who screened positive for depression or PTSD and concomitant suicidal ideation in non-mental health ambulatory care settings in 2009 and 2010 at three geographically dispersed VAMCs (Portland, Oregon; Indianapolis, Indiana; and Houston, Texas). Medical record review was used to identify screening status. Specific questions and algorithms for interpreting positive responses to suicidal ideation screens varied across centers, and will be published in a separate manuscript.13 In general, screens were between one and four sentences, and determined if Veterans had thoughts of being better off dead or of taking their own lives. In some sites, triage nurses or medical assistants completed screening. The research team consulted with the primary treating provider and contacted eligible Veterans who screened positive for suicidal ideation by mail within 2 to 6 months after screening. Primary treating providers excluded patients if concerned about psychiatric instability or cognitive impairment. Participants were reimbursed $50 for their time and travel to the VA for the interview. Recruitment was purposive, and the sample was enriched with women and ethnically diverse Veterans. Interviews were concluded when saturation on the main themes was achieved.
Interview Guide
The interviewers included a psychiatrist (LG), who completed over half of the interviews, an internist, who was also director of a VA post deployment clinic (DH), and a research assistant with background in social work (MH). They questioned participants on what they remembered about the suicide screening process; their comfort or discomfort with screening; how the care setting of the screening influenced their responses to questions about suicide; any hesitancy to discuss suicidal ideation; reactions from providers after disclosing suicidal ideation, positive and negative views and consequences of disclosing suicidal ideation; and experiences in the military with mental health and suicide screening. The interviews were semi-structured, using a guide with open-ended questions meant to encourage participants to tell their own stories in their own words at whatever length they chose to respond.
Data Analysis
Audiotapes were transcribed and de-identified. Following a modified grounded theory approach,14,15 two investigators (LG, a psychiatrist, and NP, an anthropologist) reviewed all transcripts separately and developed codes, which were organized using NVivo qualitative software. New codes were added to the codebook as topics emerged from initial review of interviews, and a second round of coding of all interviews was done using the revised codebook of 53 codes. Conceptual memos were used to develop a theory of the relationship among the codes and elucidate the deeper meanings of the participants’ responses. Text that further supports each theme is available in the online Appendix. For brevity and readability, words and sounds that are linguistically considered “filler” (e.g., “like”) were removed from the quotations and ellipses are used to shorten long quotes.
RESULTS
Thirty-four Veterans participated, including 17 from Portland, nine from Indianapolis and eight from Houston. The mean age of the participants was 34.6 years; 91 % were men and 73 % were white, non-Hispanic. Forty-two percent had served in the Army. Screen administrators included physicians (44 %), nurses (30 %), nurse practitioners (9 %), psychologists (6 %), social workers (6 %), or physician assistants (6 %). In 12 % of cases, Veterans were administered multiple screens. Each Veteran is identified by a randomly assigned letter from the alphabet that is not related to his or her name.
Acceptance and Appreciation of Suicide Ideation Screening
Veterans appreciated several aspects of the suicidal ideation screening process. They welcomed that the screening questions were straightforward and clear. Positive terms used to describe the screening process were, ‘straight forward,’ ‘direct,’ ‘forthright,’ or ‘cut and dry,’ meaning that the questions were direct and understandable. Veterans juxtaposed the clarity of suicidal ideation screening with their dislike of ambiguous and confusing health care interactions they had experienced and derided as, ‘sugarcoated,’ ‘pussyfooting,’ or, ‘beating around the bush.’
‘They actually did all the standardized questions...for depression as well as suicide—they seemed to be pretty straight and cut and dry questions.’ (Participant N)
‘She didn’t sugar coat it. I mean there’s not a delicate way to say, “Hey you’re thinking about killing yourself.” You just have to ask it. …she didn’t pussyfoot around it either. She was as delicate as you can be asking the questions, but direct about it.’ (Participant J)
While discussion of suicide was viewed as uncomfortable and difficult for many Veterans, most understood that the overall goal of screening was to help them. They were not surprised that they were asked similar questions about suicide as they had been asked in the military―in fact, they expected it. Participants were accepting of the need to screen large numbers of Veterans in a systematic way to determine who should receive care more urgently.
‘You got the initial standardized questions then, if the solider answered a yes to certain questions, ...it’s going to pop up with a different standardized question. Then eventually they figure out what's going on with Veterans. (Interviewer: You feel like it’s a good way to do it?) I do.’ (Participant N)
‘They are standard. They were what I was here for. I kind of expected them.’ (Participant J)
Criticism of Suicidal Ideation Screening
At times, the suicidal ideation screens were experienced as painful and shameful reminders of previous suicide attempts.
‘I’ve gotten used to it and know you guys are going to ask me every time…it is like sticking a needle through your eye sometimes.’ (Participant R)
Veterans reported being screened for suicidal ideation numerous times, by several different providers, and in various VA settings. At times, Veterans were seen by a variety of clinicians during daylong post-deployment health assessments, all of who repeated the same suicide-related questions or worked from templates embedded in the EMR that led to repetitive questions in the same session. The repetitiveness of the questions, and sense of communication gaps among providers (i.e., providers did not talk to one another about the screening results), fed Veterans’ frustrations and a sense of futility about getting their mental health needs addressed (Online appendix, Table 2).
‘It’s repetitive. Annoying. It feels like I have already answered the questions for you. And you’re in the same damn office, why should I go to somebody else and answer them all over again. It is a massive waste of time...to have to spend seven hours at that place answering the same questions over and over again. But apparently these three people cannot talk to each other.’ (Participant O)
‘But I mean that was about the gist of it. So I just, I felt like I gained nothing. I felt like it wasn’t, there was no attempt to figure out what’s going on. It was just, “Uh…yep checking the box, it’s still there, see you later.”’ (Participant AE)
Because of the simplicity of the suicidal ideation screening questions and the need to record the responses as ‘yes’ or ‘no,’ some Veterans felt that the questions did not give them the opportunity to clarify their thoughts or respond in a way that reflected the complexity of their experience. Some Veterans misperceived that the clinic visit associated with suicidal ideation screening would be therapeutic, when in fact the goal of the clinical assessment was diagnostic or for triage purposes.
‘I mean if I were in her shoes I think I would have asked a little bit more questions. I would have made sure the individual understood the questions… I mean it almost seemed like waste of time… it was too short, too simple. I had thoughts that I wanted to share and I did not get the opportunity to share them.’ (Participant AF)
Barriers to Disclosure of Suicidal Ideation
Some Veterans had pervasive difficulties admitting thoughts of killing themselves, or acknowledging the severity of their suicidal thoughts, that they needed help from others, or could not manage on their own. They were accustomed to minimizing and suppressing thoughts of suicide, and believed they should cope with their psychological problems on their own. The effort to suppress their suicidal ideation, however, required unsustainable energy that progressively increased their sense of isolation.
‘That’s the heartache…I just try to cover it up and faking it to make it. I know I am hurting, ...physically and mentally, but the thought of trying to get help is a sign of weakness.’ (Participant F)
Many of Veterans’ concerns about admitting their suicidal thoughts originated from experiences of stigmatization and harmful repercussions in the military, where admitting suicidal thought or having mental health problems was perceived as shameful and embarrassing, inconsistent with being a good soldier. At times, admitting suicidal thoughts would delay return home after deployment. (Online appendix, Table 3)
‘I finally started accepting that [having suicidal thoughts] was an issue for me, but prior to that there had been several times I filled out those questionnaire, post deployment and stuff, and it was just something you had to go through to get home. You knew pretty much to say no to everything.’ (Participant U)
‘They ask you, “Do you need to talk to mental health?” you say, “no.” It does not matter if you do or not. You say no because if your commander finds out you said yes they give you shit. What, you’re a soldier. You don’t need any fluffy bunny mental health crap.’ (Participant J)
Many Veterans admitted that on previous screens, they indicated they did not have suicidal thoughts even when these thoughts were chronic or severe. There was a striking difference in their willingness to divulge suicidal thoughts based on the context of the assessment. A lack of a comfortable, trusted, continuous relationship with a provider was a barrier to suicidal ideation disclosure. In absence of such a relationship, however, providers could facilitate disclosure with attention to rapport and personalization of the suicide risk assessment. Administration of the template of questions in the EMR decreased eye contact and led to the feeling that staff or clinicians were interviewing them by rote.
‘If that is the first thing someone were to say to me, I would just say no, because I wouldn’t want to tell them because I don’t know them. I don’t trust them. I don’t know who they are.’ (Participant AG)
‘I mean, I’m sitting in a doctor’s office with a—and no offense to, you know, levels of skill or training—but even if I am sitting there with a nurse assistant and I am asked off of a—you know, as he or she is sitting there with a form and checking the block as they go, I am not going “yeah, sure” you know. It’s not going to happen. It doesn’t seem appropriate. It’s not the right time.’ (Participant C)
Veterans were hypervigilant and sensitive toward any sign that they were not respected or their trust of the individual conducting the assessment was not warranted, particularly on initial interactions with the VA providers.
‘Those that are nice to me and treat me with respect right away, then they will get the respect—they will get all the information that they need from me.’ (Participant W)
A few Veterans were so mistrustful that they completely misunderstood the underlying rationale for the questions. For example, one Veteran confessed that he wondered if the VA was asking him about suicide so much because they were looking for consistency of answers to make sure he was not faking it (Participant F). Another Veteran actually questioned if the VA was trying to have him commit suicide (Participant R).
Veterans opined that suicidal thoughts were not medical issues, but personal concerns, among the most intimate they experienced. They accepted the value of screening for disease in general, but wondered if suicide was too sensitive and serious for standardized screening. Sometimes the evaluation was completed by a clerk, medical assistant or provider the Veteran did not know and was not part of their ongoing VA care. The screening in this context was often perceived as an invasion or a violation of privacy by strangers, experienced as perfunctory and abrupt, done for the purposes of completing paperwork, and poorly integrated into their care. (Online appendix, Table 4.)
(Regarding being seen by a physician assistant instead of a physician): ‘I mean, because she is just basically being a puppet for the doctors and she is getting the notes and then she is relaying to the person, but the person never met me so they can’t know how I am, my mannerisms from stuff off the notes…If she can take that much time in her day to read these notes to you, why couldn’t she come down here and talk to me herself personally. It’s like, cut out the middle man.’ (Participant S)
‘I think that I would be less likely to talk about it with a stranger…I mean you don’t want to talk to a different person every time you come to a doctor. Could you imagine your gynecologist was a different doctor every time you put your legs on the stirrups? There’s a different person entering your body. It’s kind of like that—you feel vulnerable when you talk about things, especially mental things.’ (Participant AC)
Veterans worried that acknowledging thoughts of hopelessness or desire for death would be misinterpreted by the screener as active suicidal thoughts. For example, they often felt their future was bleak or wished they were dead but insisted they would not attempt suicide. They felt this was important to explain and clarify and to expand on in the screening process.
‘I told her that I didn’t have thoughts of suicide like per se but I’d wished I was dead. I wouldn’t take my life, but if I got hit by a bus, you know, I couldn’t say I’d be mad, I’d be dead you know.’ (Participant S)
‘I was…feeling just worthless, like I can’t do nothing. I’ve had thoughts of…taking my life. I mean not just taking it…but I wish I wasn’t here.’ (Participant H)
They were also concerned that endorsing any suicidal ideation questions might lead to untoward and deleterious consequences. They worried that the provider might misjudge their safety and overreact by hospitalizing them, perhaps involuntarily—psychiatric hospitalization seemed countertherapeutic to many Veterans. Additionally, they worried about being medicated for their suicidal thoughts, which they viewed as useless (Online appendix, Table 5).
‘It’s difficult for me, one of the reasons I was worried about talking about it...is she going to try and lock me up in a straight jacket, I have no idea what the response is going to be if I talk to someone honestly.’ (Participant O)
As with worries about stigma, this perception had its basis in experiences in the military. Several had vivid memories of suicidal soldiers emergently restrained and guarded in the field, or emergently evacuated for mental health reasons.
Facilitators of Disclosure of Suicidal Ideation
Veterans were more comfortable and willing to admit suicidal thoughts to providers described as expressing ‘genuine concern,’ personal interest, and a caring attitude. The disclosure of suicidal ideation was enhanced in the context of consistent providers who knew the patient well and were trusted. These clinicians queried about suicidal thoughts in the context of important, Veteran-centered goals—such as being available for one’s children and family—that both the clinician and Veteran had discussed and agreed upon. The ability to ‘click’ with a new provider both represented finding someone who was the right fit for them, but also Veteran readiness and possibly less hypervigilance about the perceived slights and disrespect. (Online appendix, Table 6)
‘Cause I’ve seen people do that on their screen, “Have you ever attempted suicide?” Click on the screen. He didn’t do that. He actually sat down. He talked to me. He looked at me. He didn’t take his eyes off me. He talked to me and that’s what made me feel a lot better about it…’ (Participant AG)
‘Because it’s her, yes…I felt very comfortable. That is how she got it out of me ‘cause in order to make someone talk you have to make them feel comfortable and then you have to form a relationship with them.’ (Participant L)
Consequences of Disclosing Suicidal Thoughts
Attempting to suppress and avoid thoughts of suicide was experienced as burdensome and exhausting to Veterans. While admitting suicidal ideation was often experienced as initially frightening and shocking, eventually it was followed by a sense of relief. Suicidal thoughts, once admitted, resulted in greater tolerance of the assessment process and discussion of suicidal thoughts in the future. (Online appendix, Table 7)
‘It was actually a big weight off my shoulders ‘cause it was something that I don’t really share very often, not even to my family, just because I didn’t want to be a burden on them, so it was actually extremely helpful for me.’ (Participant X)
‘Before I think I tried to sugar coat them a little bit. That day I just really got tired of it…I just wanna put it out there because my personal life was taking huge hits, I knew it was from PTSD and it was time to just access it rather than ignore it. ...Last time when I filled the paperwork out I honestly felt—I didn’t feel uncomfortable ‘cause it’s out there now…That day just kind of hit me, it’s like, I really have no control over what’s going on right now. As hard as I try it just—I cannot hold it together so I just decided, you know, it’s time to—to come clean.’ (Participant Y)
Key Domains in Effective Suicide Screening and Risk Assessment
Table 1 identifies key domains of effective suicide risk assessment and potential provider and system level interventions to improve this process. Providers should focus on relationship building with suicide risk assessment defaulting to the provider who knows the patient best. Information should be shared on the goals and rationale of suicide risk assessment―this information could be communicated by the provider or developed into written material to be shared with Veterans. The provider should demonstrate empathy and communicate genuine interest. Finally, written and spoken communications should focus on understandable and direct language, which can form the basis for Veteran trust that honest disclosure about suicidal ideation will ultimately lead to improvement in their situation. Examples of potential interventions by providers or by the health system are given, though the need for more research on the effectiveness of these interventions is underscored.
DISCUSSION
This qualitative study explores the experiences of being assessed and screened for suicidal ideation during routine, non-mental health visits in VA facilities among Veterans who served in recent conflicts and were returned from deployments in Afghanistan and Iraq. We identified key domains around the importance of the provider being genuine and empathic, using understandable language, patient need for information on the rationale and goals of screening, and the facilitating aspect of a personal relationship; all factors that bring about the patient’s trust and willingness to risk disclosing suicidal ideation (Table 1).
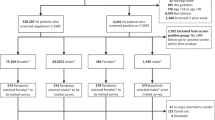
In a companion study13 we found that during the study period at these three sites, between 50 % and 59 % of all Veterans who returned from Afghanistan and Iraq were screened for depression. Among those with positive screens, 81 % were subsequently assessed one or more times for suicidal ideation. Assessment rates were higher at sites that incorporated triage nurses and medical assistants into the screening process.
There are several limitations to our study. This qualitative study reflected Veteran experiences at only three VAMCs―though there were multiple examples of each theme, indicating that thematic saturation was achieved. Although some of our sample failed to report suicidal ideation during some instances of screening, we only interviewed Veterans who eventually screened positive for possible suicidal ideation; the experiences of those with suicidal ideation who continuously screened negative—false negative screenings―are not known. In addition, Veterans with concerns about screening, or those more open to discussing thoughts of suicide, may have been more motivated to participate in this research.
Our study challenges the use of routine screening for suicidal ideation as currently implemented at some VAMCs, particularly if administered in the context of routine medical screening or by triage personnel. Similarly, Hoge and Castro16 summarize the current literature by pointing out the low predictive value of current tools for suicidal ideation screening in primary care, lack of information on deployment related screening, and unwillingness of many service members to truthfully report concerns, with the risk of adverse treatment effects, reduced patient satisfaction and treatment withdrawal. The domains identified may not only lead to provider and system level improvements, they may form the basis for further research in this area. In addition, approaches found useful in eliciting socially sensitive information in other topics such as drug use should be explored.17
REFERENCES
McCarthy JF, Valenstein M, Kim HM, Ilgen M, Zivin K, Blow FC. Suicide mortality among patients receiving care in the veterans health administration health system. Am J Epidemiol. 2009;169(8):1033–1038.
Kaplan MS, Huguet N, McFarland BH, Newsom JT. Suicide among male veterans: a prospective population-based study. J Epidemiol Community Health. 2007;61(7):619–624.
Sundararaman R, Panangala SV, Lister SA. Suicide prevention among veterans: congressional research service. May 5, 2008.
Basu S. DoD/VA suicide prevention conference. US Medicine. 2010;2010:46(2).
Department of Veterans Affairs Office of Inspector General. Healthcare Inspection: Implementing VHA’s Mental Health Strategic Plan Initiatives for Suicide Prevention. Available at: http://www.va.gov/oig/54/reports/VAOIG-06-03706-126.pdf. November 6, 2007;06-03706-126.
JCAHO. 2007 National Patient Safety Goals. Available at: http://www.jointcommission.org/NR/rdonlyres/98572685-815E-4AF3-B1C4-C31B6ED22E8E/0/07_hap_npsgs.pdf. Accessed November 6, 2007.
United States Department of Health and Human Services. The Surgeon General's Call to Action to Prevent Suicide 1999. Available at: http://www.surgeongeneral.gov/library/calltoaction/calltoaction.htm. Accessed November 6, 2007.
Institute of Medicine. Reducing Suicide: A National Imperative National Academies Press; 2002.
Department of Veterans Affairs. Clinical reminders. Available at: http://www.va.gov/vdl/documents/Clinical/CPRS-Clinical_Reminders/pxrm_2_6_um.pdf. 2007. Accessed October 25, 2011
Hoge CW, Castro CA, Messer SC, McGurk D, Cotting DI, Koffman RL. Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care. N Engl J Med. 2004;351(1):13–22.
Denneson LM, Basham C, Dickinson KC, et al. Suicide risk assessment and content of VA health care contacts before suicide completion by veterans in Oregon. Psychiatr Serv. 2011;61(12):1192–1197.
Taylor TL, Hawton K, Fortune S, Kapur N. Attitudes towards clinical services among people who self-harm: systematic review. Br J Psychiatry. 2009;194(2):104–110.
Dobscha S, Corson K, Helmer DA, Bair MJ, Denneson LM, Brandt C, Beane A, Ganzini L. Brief assessment for suicidal ideation in OEF/OIF veterans with positive depression screens. Gen Hosp Psychiatry. 2013. doi:10.1016/j.genhosppsych.2012.12.001.
Glaser BG, Strauss AL. The Discovery of Grounded Theory: Strategies for Qualitative Research. Chicago: Aldine de Gruyter; 1967.
Strauss AL, Corbin J. Basics of Qualitative Research: Grounded Theory Procedures and Techniques. Thousand Oaks: Sage; 1998.
Hoge CW, Castro CA. Preventing suicides in US service members and veterans: concerns after a decade of war. JAMA. 2012;308:671–672.
Schackman BR, Dastur Z, Rubin DS, et al. Feasibility of using audio computer-assisted self-interview (ACASI) screening in routine HIV care. AIDS Care. 2009;21:992–999.
Acknowledgements
We gratefully acknowledge the assistance of Michael Martin; Megan Crutchfield, MPH; and Monica Huffman, BS. This material is based upon work supported by the Department of Veterans Affairs, Veterans Health Administration, and Health Services Research and Development Service Project DHI-08-096. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government.
Conflict of Interest
The authors declare that they do not have a conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(DOC 78.5 kb)
Rights and permissions
About this article
Cite this article
Ganzini, L., Denneson, L.M., Press, N. et al. Trust is the Basis for Effective Suicide Risk Screening and Assessment in Veterans. J GEN INTERN MED 28, 1215–1221 (2013). https://doi.org/10.1007/s11606-013-2412-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-013-2412-6