
ABSTRACT
BACKGROUND
Federal initiatives are underway that provide physicians with financial incentives for meaningful use (MU) of electronic health records (EHRs) and assistance to purchase and implement EHRs.
OBJECTIVE
We sought to examine readiness and interest in MU among primary care physicians and specialists, and identify factors that may affect their readiness to obtain MU incentives.
DESIGN/PARTICIPANTS
We analyzed 4 years of data (2008–2011) from the National Ambulatory Medical Care Survey (NAMCS) Electronic Medical Record (EMR) Supplement, an annual cross-sectional nationally representative survey of non-federally employed office-based physicians.
MAIN MEASURES
Survey-weighted EHR adoption rates, potential to meet selected MU criteria, and self-reported intention to apply for MU incentives. We also examined the association between physician and practice characteristics and readiness for MU.
KEY RESULTS
The overall sample consisted of 10,889 respondents, with weighted response rates of 62 % (2008); 74 % (2009); 66 % (2010); and 61 % (2011). Primary care physicians’ adoption of EHRs with the potential to meet MU nearly doubled from 2009 to 2011 (18 % to 38 %, p < 0.01), and was significantly higher than specialists (19 %) in 2011 (p < 0.01). In 2011, half of physicians (52 %) expressed their intention to apply for MU incentives; this did not vary by specialty. Multivariate analyses report that EHR adoption was significantly higher in both 2010 and 2011 compared to 2009, and primary care physicians and physicians working in larger or multi-specialty practices or for HMOs were more likely to adopt EHRs with the potential to meet MU.
CONCLUSIONS
Physician EHR adoption rates increased in advance of MU incentive payments. Although interest in MU incentives did not vary by specialty, primary care physicians had significantly higher rates of adopting EHRs with the potential to meet MU. Addressing barriers to EHR adoption, which may vary by specialty, will be important to enhancing coordination of care.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
BACKGROUND
Recent evidence suggests that health information technology (HIT) has the potential to improve the effectiveness and efficiency of health care delivery not only among large institutions, but also within smaller practices and organizations.1 HIT could also serve as a foundation to enable improvements in clinical care and support initiatives such as the patient-centered medical home.2
Yet, adoption of electronic health records (EHRs) in ambulatory care has been relatively limited. In 2009, about a fifth (22 %) of office-based physicians reported having a basic EHR.3 Numerous barriers to physician adoption have been identified.4 They include problems with practices’ capacity to implement technology and misaligned incentives that result in practices bearing the full costs of implementing systems, while many benefits accrue to patients and insurers. Certain types of physicians or practices may be more likely to experience these barriers and have lower adoption rates.4–8
Recent federal HIT policy initiatives seek to address these barriers, especially among physicians who may not have the means and capabilities to readily adopt HIT. Beginning in 2011, the Health Information Technology for Economic and Clinical Health Act (HITECH) of 2009 made incentive payments available for eligible physicians who demonstrated ‘meaningful use’ (MU) of EHRs that possess functionalities capable of meeting specific criteria.9 Eligible physicians will receive up to $44,000 from Medicare or $63,750 from Medicaid, translating to an estimated $14 to $27 billion in financial incentives.10 A federally funded regional extension center program (REC) also began providing physicians with assistance to purchase and implement EHR systems, to train staff, and to address changes to clinical workflow.11 Primary care physicians are among the key groups of physicians that are the focus of these efforts.
In order to assess progress and interest in MU among office-based physicians, we used an annual, nationally representative sample of office-based physicians to examine EHR adoption from 2008 to 2011 among primary care physicians and specialists. We specifically examined physicians’ intent to apply for MU, and their potential readiness to demonstrate MU of EHRs, which requires the adoption of EHRs with specific functionality. We also examined physician and practice characteristics associated with EHR adoption, in order to identify factors that may affect readiness to apply for MU.
METHODS
Data Source & Collection
We analyzed 4 years of data (2008–2011) from the National Ambulatory Medical Care Survey (NAMCS) Electronic Medical Record (EMR) Supplement, an annual cross-sectional nationally representative mail survey of non-federally employed office-based physicians who provide direct patient care.3,12,13 The survey included items related to: physician and practice characteristics; EHR adoption; EHR functionalities; and intent to apply for MU. Non-respondents received telephone follow-up. The sample size was increased in 2010 to generate state-level estimates.
Measures of EHR Adoption
We examined EHR adoption using several approaches. We considered a physician to have “any” EHR if he or she responded positively to the following question: “Does this practice use electronic medical records or electronic health records (not including billing records)?” EHRs were also defined based upon specific functionalities. A “basic” EHR enables providers to record patient demographics, problem and medication lists, and clinical notes; to perform computerized physician order entry (CPOE) for medications; and to view labs and imaging results. This definition has been applied in several national studies and reports, and has evolved over time to include newer functionalities.3,4
However, neither of these measures captures the full set of functionalities needed to assess how ready physicians are to meet the MU criteria. We constructed a measure that assessed whether physicians had adopted EHRs with the 15 required “core” functionalities for the first stage of meaningful use, by mapping the “core” functionalities to items in the survey that assess EHR functionality by year, from 2008 to 2011.14 The survey was developed prior to the final MU criteria and therefore did not include items to assess all the MU criteria. We identified proxies for eight of the “core” elements in 2010–2011 and six in 2008–2009 (Online Appendix Table 1). The functionalities associated with “basic” and our measure of “core” MU EHRs partially overlap.
In addition to the “core” criteria, eligible physicians must select five out of ten “menu set” functionalities in order to obtain the first stage of MU incentives. We only identified proxies from the survey for four out of the ten “menu” set functionalities for 2010–2011, and only two for 2008–2009. We encountered high rates of missing and unknown values for menu options related to public health reporting (ranging from 14 % to 21 %). Thus, we do not report on physicians’ capability to meet the menu set criteria.
Respondents who either indicated they did not know if they had particular EHR functionality or left the item blank were assumed not to have these functionalities.
Definition of Primary Care
We designated the following specialties as primary care, following the National Center for Health Statistics convention: family practice, family medicine, general practice, internal medicine, pediatrics, obstetrics and gynecology.15
Definition of Urban Versus Rural
We designated physicians as practicing in an urban area if their practice was located in a metropolitan statistical area (MSA); we designated rural providers as those practicing in a non-MSA region.
Analysis
We calculated the proportion of primary care physicians and specialists that had adopted “any,” “basic,” and selected “core” MU EHR measures from 2008 to 2011, and plotted these trends. We calculated the proportion of primary care physicians and specialists that had adopted specific functionalities associated with these EHR measures. We used t-tests to assess changes in EHR adoption and specific functionalities over time, and to assess differences in adoption of EHRs and specific functionalities between primary care physicians and specialists. Since HITECH started in 2009, data from year 2009 rather than 2008 were used as a reference to compare adoption rates at the start of HITECH to the current environment.
We used multivariate logistic regression to examine the association between physician characteristics (age, gender, specialty—primary care vs. other specialist) and practice characteristics (urban/rural, region, practice size, practice type, and practice setting by ownership) with adoption of EHRs (across the various definitions) over time (2008 through 2011). We assessed whether trends over time were significant, controlling for these characteristics.
We assessed physicians’ interest in applying for MU incentives, comparing primary care physicians and specialists. We conducted analyses using SAS 9.2 (SAS Institute, Carey, NC) and SUDAAN 10.0 (RTI, Cary, NC). All analyses used weights to account for non-response and standard errors that accounted for the complex sample design. We report the weighted response rate that reflects the proportion of the survey population (in this case, a nationally representative population of physicians) that responded to the survey.
RESULTS
Survey Respondents
The overall sample consisted of 10,889 respondents, with weighted response rates of 62 % (n = 843) in 2008; 74 % (n = 1,054) in 2009; 66 % (n = 4,666) in 2010; and 61 % (n = 4,326) in 2011. Almost three-quarters (73 %) of the respondents were 45 years or older and about a quarter (26 %) were female (see Online Appendix Table 2). The majority of respondents worked in smaller or single specialty practices, with about 77 % working in single specialty groups, and 68 % working in practices with five physicians or fewer. In addition, a majority of physicians (69 %) worked in a physician-owned private practice or free-standing clinic. Less than half (48 %) were primary care physicians.
In comparison to primary care physicians, specialists were significantly less likely to be female, and more likely to be working in a single specialty setting or physician-owned practice, or in an urban area (p < 0.05).
EHR Adoption Trends: Primary Care and Specialists
As shown in Fig. 1, both primary care and specialist physicians’ adoption of EHRs increased dramatically between 2009 and 2011. The increase in EHR adoption among primary care physicians was not significant between 2008 and 2009. Since 2009, primary care physicians’ adoption of EHRs significantly increased each year (p < 0.01); this was consistent regardless of whether the EHR was categorized as “any” EHR (61 % vs. 41 %); “basic” EHR (39 % vs. 20 %); or whether the EHR had the capability to meet selected “core” MU criteria (38 % vs. 18 %). Primary care adoption of EHRs (regardless of definition) was significantly higher in 2011 compared to 2009 (p < 0.01). Specialist physicians’ adoption was significantly higher in 2011 compared to 2009 (p < 0.01), but with annual increases only significant from 2010 to 2011 (Fig. 2).

EHR adoption rates among primary care physicians: 2008–2011 (n = 5,262).

EHR adoption rates among specialists: 2008–2011 (n = 5,627).
Comparisons between primary care and specialist adoption of EHRs during this period indicate that in both 2010 and 2011, primary care physicians’ adoption of EHRs was significantly higher in comparison to specialists (p < 0.01 for “basic” and “core”). Primary care physicians’ adoption of EHRs that had the capability to meet selected MU criteria was also significantly higher than specialists in both 2010 (28 % vs. 13 %, p < 0.01) and 2011 (38 % vs. 19 %, p < 0.01), but did not significantly differ in 2009.
Trends in Adoption of Specific EHR Functionalities by Primary Care and Specialists: 2008–2011
Both primary care and specialist physicians increased their adoption of most EHR functionalities. In comparison to 2009, primary care physicians significantly (p < 0.01) increased their adoption of five out of 11 selected functionalities associated with MU or basic EHRs in 2010 and nine out of 11 in 2011 (Table 1). Specialists significantly increased their adoption of two out of 11 of these functionalities in 2010 and seven out of 11 in 2011 in comparison to 2009. Primary care and specialist physicians’ adoption of CPOE for medications; medication alerts; e-prescribing; diagnosis and problem lists; and clinical notes significantly increased in 2011 in comparison to 2009 (p < 0.01). In comparison to 2009, primary care and specialist physicians’ adoption of reminders for guideline-based interventions significantly increased in 2011 (p < 0.01 and p < 0.05, respectively). Although still relatively high, adoption of functionalities associated with recording patient demographics significantly decreased in 2011 in comparison to 2009 for both specialists and primary care physicians (p < 0.01).
Readiness and Intent to Apply for Meaningful Use: Primary Care Versus Specialists
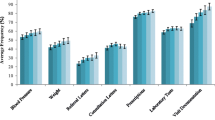
Compared to specialists, primary care physicians have adopted a greater number of functionalities required to receive MU incentive payments; however, the proportion that intended to apply for those payments did not differ significantly. In 2010, primary care physicians had significantly higher rates of adopting eight out of 11 functionalities compared to specialists (p < 0.05), including six out of eight functionalities associated with MU (p < 0.05) (data not shown). In 2011, primary care physicians had significantly higher rates of adopting ten out of 11 functionalities compared to specialists (p < 0.05), including eight out of eight functionalities associated with MU (p < 0.01) (Fig. 3). This included functionalities, such as recording patient demographics (76 % vs. 70 %, p < 0.01), as well as reminders for guideline-based interventions (50 % vs. 31 %, p < 0.01) and e-prescribing (61 % vs. 49 %, p < 0.01). For basic functionalities, primary care physicians had significantly higher rates of adopting functionality that enabled viewing labs results (p < 0.01) and recording clinical notes electronically (p < 0.05) in comparison to specialists.

Physician adoption of selected functionality associated with “core” meaningful use criteria and “basic” EHRs by specialty type: 2011.
In 2011, half of all physicians indicated that they intend to apply for MU incentives, which represented a significant increase in intent to apply over 2010 (52 % vs. 41 %, p < 0.01) (data not shown). Physicians’ intent to apply for MU did not significantly differ between primary care physicians and specialists in 2011 (54 % vs. 50 %) or in 2010 (42 % vs. 40 %) (data not shown). In 2011, one-third of physicians indicated they were uncertain whether they would apply, significantly less than the proportion in 2010 (33 % vs. 45 %, p < 0.01) (data not shown).
Physician and Practice Characteristics Associated with EHR Adoption and Readiness to Meet Meaningful Use
Multivariate analyses confirmed that even after adjusting for physician and practice characteristics, the odds of physicians adopting EHRs with the capability to meet selected “core” MU criteria was significantly higher in both 2010 and 2011 in comparison to 2009 (p < 0.01) (Table 2). We also found that primary care physicians had significantly higher odds of adopting EHRs with selected MU “core” functionalities compared to specialists (OR 2.22, 95 % CI 1.89–2.70). Physicians who worked in practices that were larger (OR 2.30, 95 % CI 1.78–2.98); multispecialty (OR 2.19, 95 % CI 1.77–2.70); or owned by an HMO (OR 7.96, 95 % CI 4.27–14.83) had significantly higher odds of adopting EHRs with the capability to meet selected “core” criteria. Older physicians (OR 0.78, 95 % CI 0.65–0.95) and physicians practicing in the southern region of the U.S. (OR 0.68, 95 % CI 0.53–0.86) had significantly lower odds of adopting EHRs with the capability to meet selected “core” criteria.
Multivariate findings regarding adoption of “any” or “basic” EHRs showed similar patterns with regards to significant time trends, physician age, practice size and type, and practice setting and ownership (Online Appendix Table 3). Neither urban/rural status nor gender was significantly associated with adoption of “any” or “basic” EHRs, or with the adoption of EHRs with the capability to meet selected “core” MU criteria.
DISCUSSION
Using a nationally representative survey of office-based physicians, we found that primary care and specialist physicians’ adoption of EHRs increased significantly since the HITECH Act of 2009. Physician adoption of EHRs was significantly higher in both 2010 and 2011 compared to 2009, even after adjusting for physician and practice characteristics. Specialists and primary care physicians indicated comparable levels of intent to apply (50 % vs. 54 %) for MU incentives in 2011; however, primary care physicians’ adoption of EHRs with the potential to meet MU incentives was nearly twice that of specialists (38 % vs. 19 %).
Although our analyses show a significant rise in overall EHR adoption rates since 2009, the number of physicians adopting EHRs has been increasing since 2003.3 Thus, it is possible that the HITECH Act may have accelerated the existing trend in physician adoption, in addition to being influenced by market forces, state health information technology (IT) initiatives, and health care delivery and payment reform mechanisms which involve the use of EHRs.2,16,17
Some of these forces driving EHR adoption may affect primary care physicians in particular. An examination of trends prior to 2007 indicates that primary care adoption rates were lower than specialists.18 An early study of physician adoption of computerized functionalities also found that medical specialists had higher rates of adopting certain functionalities compared to primary care physicians.19 Although some indications of a reversal of this trend began in 2007, only recently have EHR adoption rates among primary care physicians become substantially higher than those of specialists. We found large, significant differences between specialists’ and primary care physicians’ readiness for MU that began in 2010 and further widened in 2011. These differences may reflect in part the early efforts of the Regional Extension Centers (RECs) in promoting EHR adoption among primary care physicians; the particular Medicare and Medicaid eligibility requirements for MU; and the proliferation of health care delivery redesign efforts, such as the Patient Centered Medical Home, which focus on primary care physicians and require the use of health IT.11,16,20–22
The increased number and types of functionalities adopted by primary care physicians in comparison to specialists in 2011 may place them in a better position to qualify for financial incentives and reap other benefits. Physicians using EHRs with advanced functionalities have reported greater benefits from using EHRs.4 Furthermore, certain MU functionalities such as CPOE, electronic prescribing and clinical decision support have been associated with improvements in care.2,23–30 However, the full clinical benefits of MU have yet to be empirically evaluated and warrant future research.
Although adoption of many functionalities varied by specialty, adoption of several functionalities associated with e-prescribing significantly increased between 2009 and 2011 across both primary care physicians and specialists. This pattern may reflect the influence of prior policies, such as the Medicare Modernization Act (MMA) of 2003, which included incentives for e-prescribing, as well as the growth of private sector networks which enable e-prescribing. Assessing the effects of HITECH and other recent initiatives on the adoption of EHR functionalities associated with MU will be important in future studies.
In addition to specialty, physicians’ adoption of EHRs and readiness for MU may be dependent on a practice’s organization. Our findings show that between 2009 and 2011, physicians working in practices that were larger, multi-specialty or owned by entities other than physicians, especially HMOs, were more likely to have adopted EHRs than physicians working in smaller practices. Physicians in smaller practices continued to lag behind larger practices4,7 and those working in closed health systems,31 as found in earlier studies. Monitoring these trends to assess whether this gap diminishes through the provision of the MU financial incentives and assistance through the regional extension center program will be important.
Our study had several limitations. These findings are based upon self-reported survey data that could not be independently verified. EHR adopters may be more likely to respond, potentially leading to overestimates of EHR adoption and readiness for MU. Additionally, because the surveys were developed prior to MU incentive criteria, we could not identify proxies for all measures. One anomalous finding that the percentage of all physicians recording patient demographics decreased between 2009 and 2011 may be due to sampling variation or other unobserved selection effects.32
In addition, although the current survey focuses on adoption, future versions of the survey will ask physicians to report usage, offering opportunities to empirically examine use of ‘meaningful use’ functionalities. Another new national survey addresses barriers and facilitators of EHR adoption.33
In summary, we found that a majority of physicians intend to apply for MU incentives and that physician EHR adoption rates have nearly doubled since 2009. However, readiness to meet MU varied by physician and practice characteristics. Primary care physicians were significantly more likely to have adopted EHRs with the potential to meet MU, as were physicians working in larger practices. EHRs serve as a critical component of interventions designed to improve coordination of care across a fragmented healthcare system.2,34 To achieve the HITECH Act’s goals of promoting nationwide electronic exchange and use of health information to improve quality and coordination of care, these variations in readiness to meaningfully use EHRs will need to be addressed.
REFERENCES
Buntin MB, Burke MF, Hoaglin MC, Blumenthal D. The benefits of health information technology: a review of the recent literature shows predominantly positive results. Health Aff (Millwood). 2011;30(3):464–71.
Buntin MB, Jain SH, Blumenthal D. Health information technology: laying the infrastructure for national health reform. Health Aff (Millwood). 2010;29(6):1214–9.
Hsiao CJ, Hing E, Socey TC, Cai B. Electronic Health Record Systems and Intent to Apply for Meaningful Use Incentives Among Office-Based Physician Practices: United States, 2001–2011. NCHS Data Brief, No79. Hyattsville: National Center for Health Statistics; 2011.
DesRoches CM, Campbell EG, Rao SR, et al. Electronic health records in ambulatory care—a national survey of physicians. N Engl J Med. 2008;359(1):50–60.
Simon SR, Kaushal R, Cleary PD, et al. Physicians and electronic health records: a statewide survey. Arch Intern Med. 2007;167(5):507–12.
Bramble JD, Galt KA, Siracuse MV, Abbott AA, Drincic A, Paschal KA, et al. The relationship between physician practice characteristics and physician adoption of electronic health records. Health Care Manag Rev. 2010;35(1):55–64.
Rao SR, Desroches CM, Donelan K, Campbell EG, Miralles PD, Jha AK. Electronic health records in small physician practices: availability, use, and perceived benefits. J Am Med Inform Assoc. 2011;18(3):271–5.
Menachemi N, Powers TL, Brooks RG. Physician and practice characteristics associated with longitudinal increases in electronic health records adoption. J Healthc Manag. 2011;56(3):183–97.
Blumenthal D. Launching HITECH. N Engl J Med. 2010;362(5):382–5.
Blumenthal D, Tavenner M. The “meaningful use” regulation for electronic health records. N Engl J Med. 2010;363(6):501–4.
Maxson E, Jain S, Kendall M, Mostashari F, Blumenthal D. The regional extension center program: helping physicians meaningfully use health information technology. Ann Intern Med. 2010;153(10):666–70.
Hsiao CJ, Beatty PC, Hing E, Woodwell DA, Rechtsteiner EA, Sisk JE. Electronic medical record/electronic health record use by office-based physicians: United States, 2008 and preliminary 2009. National Center for Health Statistics Health E-stat.
Hsiao CJ, Burt CW, Rechsteiner E, Hing E, Woodwell DA, Sisk JE. Electronic medical record use by office-based physicians: United States, 2008; 2008. National Center for Health Statistics Health E-stat.
Marcotte L, Seidman J, Trudel K, et al. Achieving meaningful use of health information technology: a guide for physicians to the EHR incentive programs. Arch Intern Med. 2012;172(9):731–6.
National Center for Health Statistics. National Ambulatory Medical Care Survey Microdatafile; 2008.
Bitton A, Martin C, Landon BE. A nationwide survey of patient centered medical home demonstration projects. J Gen Intern Med. 2010;25(6):584–92.
Kern LM, Barron Y, Abramson EL, Patel V, Kaushal R. HEAL NY: promoting interoperable health information technology in New York State. Health Aff (Millwood). 2009;28(2):493–504.
Decker SL, Jamoom EW, Sisk JE. Physicians in nonprimary care and small practices and those age 55 and older lag in adopting electronic health record systems. Health Aff (Millwood). 2012;31(5):1108–14.
Corey C Grossman JM. Clinical Information Technology Adoption Varies Across Physician Specialties. Center for Health System Change; 2007; 34.
Rittenhouse DR, Shortell SM. The patient-centered medical home: will it stand the test of health reform? JAMA. 2009;301(19):2038–40.
Bruen BK, Ku L, Burke MF, Buntin MB. More than four in five office-based physicians could qualify for federal electronic health record incentives. Health Aff (Millwood). 2011;30(3):472–80.
US. Department of Health and Human Services. Office of the National Coordinator for Health Information Technology. Regional Extension Centers. ONC’s Regional Extension Centers Sign Up 100,000 Primary Care Providers. Available at:.(http://www.healthit.gov/buzz-blog/regional-extension-centers/rec-primary-care-providers/). Accessed November 15, 2012.
Abramson EL, Kaushal R. Computerized provider order entry and patient safety. Pediatr Clin N Am. 2012;59(6):1247–55.
Wolfstadt JI, Gurwitz JH, Field TS, Lee M, Kalkar S, Wu W, Rochon PA. The effect of computerized physician order entry with clinical decision support on the rates of adverse drug events: a systematic review. J Gen Intern Med. 2008;23(4):451–8. Review.
Kaushal R, Shojania KG, Bates DW. Effects of computerized physician order entry and clinical decision support systems on medication safety: a systematic review. Arch Intern Med. 2003;163(12):1409–16. Review.
Kern LM, Barrón Y, Dhopeshwarkar RV, Edwards A, Kaushal R; with the HITEC Investigators. Electronic health records and ambulatory quality of care. J Gen Intern Med. 2012; doi:10.1007/s11606-012-2237-8.
Cebul RD, Love TE, Jain AK, Hebert CJ. Electronic health records and quality of diabetes care. N Engl J Med. 2011;365(9):825–33.
Abramson EL, Barron Y, Quaresimo J, Kaushal R. Electronic prescribing within an electronic health record reduces ambulatory prescribing errors. Jt Comm J Qual Patient Saf. 2011;37(10):470–8.
Jain A, McCarthy K, Xu M, Stoller JK. Impact of a clinical decision support system in an electronic health record to enhance detection of alpha-antitrypsin deficiency. Chest. 2011;140(1):198–204.
Bell LM, Grundmeier R, Localio R, et al. Electronic health record-based decision support to improve asthma care: a cluster-randomized trial. Pediatrics. 2010;125(4):e770–7.
Chen C, Garrido T, Chock D, Okawa G, Liang L. The Kaiser Permanente Electronic Health Record: transforming and streamlining modalities of care. Health Aff (Millwood). 2009;28(2):323–33.
Cai B, Shimizu I. Electronic Medical Record Systems Nonresponse Bias Analysis for 2011 NAMCS Mail Survey. Joint Statistical Meeting; 2012.
Jamoom E, Beatty P, Bercovitz A, Woodwell D, Palso K, Rechtsteiner E. Physician Adoption of Electronic Health Record Systems: United States, 2011. NCHS Data Brief, No 98. Hyattsville: National Center for Health Statistics; 2012.
Ventres WB, Frankel RM. Patient-centered care and electronic health records: it’s still about the relationship. Fam Med. 2010;42(5):364–6.
Acknowledgements
Funders
The Office of the National Coordinator (ONC) for Health Information Technology at the U.S. Department of Health and Human Services funded the survey and supported the salaries of ONC and National Center for Health Statistics staff to conduct this study.
Conflict of Interest
The authors declare that they do not have conflict of interest.
Prior Presentations
This paper was presented as an oral presentation at the AcademyHealth Annual Research Meeting, in Seattle in June, 2011.
Author information
Authors and Affiliations
Corresponding author
Additional information
The views expressed should not be interpreted as those of the Centers for Disease Control and Prevention, the Congressional Budget Office or the Office of the National Coordinator for Health Information Technology.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Appendix Table 1
MU Criteria to National Ambulatory Medical Care Survey EMR Supplement MU Final Rule (PDF 24 kb)
Appendix Table 2
Physician Characteristics: Primary Care Specialty Versus Other Specialties, 2008–2011 (PDF 26 kb)
Appendix Table 3
Multivariate Analyses: Factors Significantly Associated with Physician Adoption of “Any” and “Basic” EHRs (p < 0.05) (PDF 31 kb)
Rights and permissions
About this article
Cite this article
Patel, V., Jamoom, E., Hsiao, CJ. et al. Variation in Electronic Health Record Adoption and Readiness for Meaningful Use: 2008–2011. J GEN INTERN MED 28, 957–964 (2013). https://doi.org/10.1007/s11606-012-2324-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-012-2324-x