
ABSTRACT
BACKGROUND
Prognosis is critical in individualizing care for older adults with late life disability. Evidence suggests that preferences for prognostic information may be culturally determined. Yet little is known about the preferences of diverse elders for discussing prognosis.
OBJECTIVE
To determine the preferences for discussing prognosis of a diverse sample of older adults with late-life disability
DESIGN & PARTICIPANTS
We interviewed 60 older adults with mean age 78 and mean 2.5 Activities of Daily Living dependencies. Participants were recruited from San Francisco’s On Lok program, the first Program of All-inclusive Care for the Elderly (PACE). Participants were interviewed in English, Spanish, and Cantonese, and responded to scenarios in which their doctors estimated they had 5 years and 1 year left to live. Open-ended questions explored the reasons for their responses. Results were analyzed qualitatively using grounded theory.
KEY RESULTS
Sixty-five percent of participants wanted to discuss the prognosis if their doctor estimated they had <5 years to live and 75% if the estimate was <1 year. Three themes were prominent among patients who wanted to discuss prognosis: to prepare, to make the most of the life they had left, and to make medical or health-related decisions. Those who preferred not to discuss prognosis described emotional difficulty, the uncertainty of prognosis, or that it would not be useful. Nearly all participants said that doctors should not make assumptions based on race or ethnicity, though differences between ethnic groups emerged.
CONCLUSIONS
Most patients in this diverse sample of disabled elders were interested in discussing prognosis, while a substantial minority was not. Among those participants who preferred to discuss prognosis, many said that prognostic information would be important as they made difficult medical and personal decisions in late-life. Clinicians should inquire about preferences for discussing prognosis before sharing prognostic estimates.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
BACKGROUND
Prognosis is an important factor in individualizing care for older adults living with late life disability,1 and physical disability is a major predictor of limited prognosis.2-7 As a result, medical treatment guidelines are increasingly based on prognostic information rather than on arbitrary age-based cutoffs.8-11 In addition, prognosis impacts the likelihood of benefits and harms arising from tests or treatments with up-front harms and delayed benefits, such as cancer screenings12,13 or medications targeted at risk factor reduction.14 When shared with patients, prognostic information may also facilitate greater patient involvement in medical decision-making.15-19
Despite evidence suggesting that prognosis is an important tool in the care of older adults with late-life disability, we know very little about the preferences for discussing prognostic information in this population. Moreover, although Latinos, Chinese-Americans, and African-Americans are among the fastest growing groups of American elderly,20 the extent to which preferences for prognosis may vary across racial and ethnic groups is not well understood.21 One study of 214 older adults with limited life expectancy (91% white) found that 50% of participants with a prognosis of 5 years left to live and 83% of those with a prognosis of less than 1 year wanted to discuss prognosis with their doctor.22 Literature from outside the US shows that elders in traditional Chinese families may prefer non-disclosure of poor prognosis,23,24 though more recent findings from China and Korea suggest that patient attitudes in Asian cultures may be changing in favor of direct, patient-centered disclosure.25,26 A limited number of studies from the advance planning literature also point to Latinos’ unique perspectives on patient-doctor discussions around the end of life.27,28 Additional studies have addressed how best to discuss prognosis given patients’ preferences and perceived needs,17,29,30 but we could find no deep, qualitative investigations of the reasons behind patient preferences for prognosis in a diverse elderly population. An in-depth understanding of the factors that motivate patients to desire or decline prognostic information, however, could enable clinicians to provide individualized and patient-centered care for diverse older adults in late life.
To address the lack of in-depth information about preferences for prognosis from diverse communities, we conducted a qualitative study of diverse elders’ attitudes towards discussing prognosis. We explored the reasons behind stated preferences for prognostic information, included probes about the roles of uncertainty, hope, and family, and asked participants to discuss how clinicians could communicate prognosis most effectively.
METHODS
Design and Setting
We conducted a qualitative study using in-person interviews with 60 older adults from San Francisco’s On Lok Lifeways program, the first Program of All-inclusive Care for the Elderly (PACE). On Lok patients are nursing home eligible and live an average of 4.5 years from the time of their enrollment.31 With its interdisciplinary model of community-based long-term care, On Lok aims to help seniors live at home and in their familiar communities for as long as possible. Though each On Lok center serves a diverse patient base, some centers focus on providing services to specific groups such as Latino or Chinese elders. Thus, recruitment sites for this study were selected to ensure an ethnically diverse sample.
Participants and Procedures
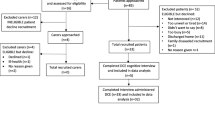
Eligible participants included all On Lok enrollees at six of eight San Francisco sites whose primary language was English, Spanish, or Cantonese, and who scored greater than 17 on the Mini-Mental State examination. Querying the On Lok database using these parameters, we identified a sample of 177 potential participants. On Lok social workers then helped us to identify the subjects among this group that could participate in a 45-min interview and did not have severe mental illness. We then began interviewing, seeking a balance of participants among ethnic groups. We conducted semi-structured qualitative interviews in private settings at each patient’s On Lok site. Interviews were conducted in English, Spanish, and Cantonese by native-speaking researchers who were not affiliated with On Lok. After translation from English into Spanish and Cantonese, the interview guide was reverse-translated to ensure accuracy. Where words or concepts did not translate well from English to Spanish or Cantonese, we located a word or concept that worked well in Spanish and Cantonese and translated back to English.
Following a short series of questions to establish rapport, participants were asked if they had ever talked with their doctor about how long they might have left to live. Participants were asked to respond to scenarios in which their doctors estimated that they had less than 5 years and 1 year left to live. Using the example of a prognosis of less than 5 years to live, interviewers then asked a series of open-ended questions to further explore patient preferences for discussing prognosis (see Online Appendix for interview guide). The interview guide was modified as interviews were conducted to further explore emerging themes. All interviews took place over a 6-month period in 2010. Demographic and health data were collected from On Lok medical records, including Activities of Daily Living (ADL) and Instrumental ADL dependencies.
Analysis
Interviews were recorded, translated, and transcribed, and results were analyzed following standard grounded theory principles. 32,33 Data were analyzed using a system of constant comparative analysis, reviewing interviews iteratively to identify new themes. A multidisciplinary research team including scholars from medicine, geriatrics, ethics, and health policy reviewed transcripts from early interviews to develop a common codebook. A single researcher then coded all subsequent interviews. Coding of 25% of all data, using randomly selected transcript pages, was repeated by a second researcher with >80% concordance, and disagreements were resolved by consensus. As new themes emerged, new codes were developed with input from the multidisciplinary research team, and previously coded interviews were re-coded. Because our objective was to determine the preferences for discussing prognosis of a diverse sample of older adults with late-life disability, the emergence of new themes within ethnic groups guided our study end-point. When no new themes emerged from multiple interviews with participants from each ethnic group, thematic saturation was reached, and no further interviews were conducted.34
RESULTS
The characteristics of 60 older adults interviewed for this study are detailed in Table 1. The mean age of participants was 78; 63% were female. Our sample was diverse, comprised of 12 (20%) African-Americans, 19 (32%) Chinese-Americans, 14 (23%) Whites, 11 (18%) Latinos, and 4 (7%) participants who reported their race/ethnicity as “other” (Hawaiian, Filipina, African, and Native American). On average, participants in the study were dependent in 2.5 of 6 Activities of Daily Living (ADLs) and in 6.6 of 7 Instrumental ADLs.
Discuss Prognosis with a Physician or Clinician
Only one participant in our study reported ever having discussed prognosis with a doctor. This participant described a brief, patient-initiated discussion that took place in response to a new course of treatment: “When they did my dialysis, they said it may be that I have 10 years left. I have about 6 now. He told me just like that—my husband was there—he told me 10 years or more, depending on my treatment” (Latino woman, age 69).
While over 95% of participants had never discussed prognosis with a doctor, a dominant theme to emerge from participant interviews was a preference for discussing prognosis. When given a hypothetical scenario in which their doctor believed they may have less than 5 years to live, 65% of participants said they would want their doctor to discuss their prognosis with them. As prognostic estimates shortened, more participants reported wanting to discuss prognosis with their doctor; at 1 year or less to live, 75% of participants said they would want this information (8 of 12 African-Americans, 15 of 19 Chinese-Americans, 12 of 14 Whites, and 7 of 11 Latinos). Among participants who reported wanting to discuss prognosis at both 5 years and 1 year, many described their preference for discussion at 1 year in more urgent terms: “In 1 year, it passes, time flies” (Chinese-American woman, age 87).
Reasons to Discuss Prognosis
Three broad themes emerged to describe participants’ reasons for wanting to discuss prognosis: (1) to prepare for the end of life, (2) to make the most of the life they had left, and (3) to make medical or health-related decisions (see Table 2). Many, in particular, emphasized how they expected prognostic information to enable “preparation” or “readiness” ahead of death: “I can prepare mentally” (Chinese-American man, age 78); “to prepare myself emotionally and religiously” (Latino woman, age 70); “to make preparations for my family, financial and emotional” (White woman, age 60); “to help me get ready” (African-American woman). Three domains describing prognosis-aided preparation were dominant: (1) financial and logistical, (2) psychological or spiritual, and (3) preparing friends and family. Two domains were also described by participants who said prognostic information would enable them to make the most of the time they had remaining. Some believed they would feel free to pursue pleasurable activities; others felt that knowing their prognosis would push them to pursue good deeds before death (Table 2). Among participants who desired prognostic information for medical decision-making, some felt that knowing their prognosis would help them make decisions that could improve their prognosis. An 80-year-old Chinese-American man, for example, said: “When I know, I’ll take special precautions like eat less sugar and rice.” Others believed that knowing prognosis would provide a helpful context in which to make decisions about their care: “I would want them to tell me so that I could decide what I am going to do. I don’t want to die here. I want to die at home” (Latina woman, age 69).
Participants often weighed competing concerns before arriving at their preference for prognostic information. “There would be days I get depressed, being human. But I think not knowing is worse” (White woman, age 78); “Your heart will be uncomfortable but you will die anyway. It’s better if you know” (Chinese-American man, age 80). These participants often described a psychological resiliency that would allow them to successfully adapt to knowing their prognosis: “The first thing comes shock and then comes a tremendous amount of anger and then comes sort of like—you get used to it kind of a thing—and then you start thinking logically what to do” (White man, age 76). Others expected to counter emotional challenges using a religious or spiritual coping strategy: “The hope issue is not even in there because with my religion, I don’t have any fear of dying” (White woman, age 59).
Reasons Not to Discuss Prognosis
A significant proportion of participants (25%) said they would prefer not to discuss prognosis at any timeframe. Three themes emerged to describe this preference: (1) knowing prognosis imposes too great an emotional burden, (2) prognosis is not medically determined or is too uncertain, and (3) prognostic information is not useful (see Table 2). Among these themes, concerns over the emotional burdens associated with knowing prognosis were most prominent. Participants felt that discussing prognosis could lead to “anguish” (Latino woman, age 88), “depression” (Latino man, age 66), or difficulty avoiding negative thoughts. Others doubted doctors’ ability to know or estimate prognosis: “They don’t know, so they should just not even start to discuss it with the patient” (White man, age 81). A smaller number of participants preferred not to discuss prognosis because they felt the information would not be useful. More often, however, participants who declined to discuss prognosis also acknowledged ways in which prognostic information could be useful. The man (White, age 81) quoted above, for example, still felt that if it was possible to know his prognosis, discussing it “would be helpful to me because I wouldn’t take everything for granted.”
Racial/Ethnic Themes
While a majority of participants of each race/ethnicity expressed a preference for discussing prognosis with their doctors, themes within racial/ethnic groups and pairings also emerged. Unlike others, some White and African-American participants, for example, spoke of an obligation on the part of doctors to share prognostic estimates: “I think I’m entitled to that information; if that’s actually what they think or believe, I’m supposed to know that” (White woman, age 89). Latinos, more than others, expressed concern over the emotional burdens associated with discussing prognosis. Latinos were also the only participants to express a preference for a clinician from their same ethnic background. For example, when asked if she would prefer that discussions of prognosis be conducted in her native language, one participant replied: “yes…there is a better understanding there—you understand better when [doctors] are Latino and they speak Spanish” (Latino woman, age 69). Similarly, though the majority of participants arrived at a clearly stated preference, a theme of indifference emerged almost exclusively among Chinese-American participants: “however long one has to live, that’s how long one has to live. Whether or not I know, it doesn’t matter” (Chinese-American man, age 87).
Despite these differences between racial/ethnic groups, nearly all participants felt that a doctor should not make assumptions based on the patient’s ethnicity. Rather, participants stressed that preferences for prognostic information are deeply personal and that doctors should ask each patient if he or she would like to discuss prognosis before sharing prognostic estimates. Participants agreed that the communication skills and strategies doctors use during the discussion of prognosis would impact how they receive the information. Participants said they would be more receptive to discussing prognosis if doctors were direct, empathic, and not rushed. Many also felt that doctors should acknowledge that any prognostic estimate is uncertain (Table 3).
CONCLUSION
The strongest theme from our study of diverse older adults with late-life disability was the acceptability and even desire to discuss prognosis by most participants. Moreover, as prognostic estimates decreased from 5 years to 1 year, more participants were interested in discussing prognosis. In describing why they preferred to discuss prognosis, participants talked about preparing themselves and their families, providing for their own emotional and spiritual needs, and making medical and health-related decisions. Conversely, a substantial minority of older adults said they would not want to discuss prognosis. These participants feared the emotional burdens associated with knowing prognosis, felt that prognostic estimates were too uncertain, or doubted that prognostic information could be useful to them. Important differences between racial/ethnic groups emerged, though nearly all participants preferred that doctors not make assumptions based on ethnicity. Participants also stressed specific communication strategies clinicians could use to ensure that discussions of prognosis are productive. These results point to a discord between clinical practice and patient preferences in prognostic disclosure and underline the need for clinicians who are capable of both determining patient preferences and disclosing prognostic information with care and sensitivity when patients desire it. Indeed, our findings suggest that clinicians should consider sharing prognosis with disabled older patients as an important element of patient-centered care. As one participant said: “The discussion should be initiated. It is the reality” (Chinese-American man, age 89).
Our study is the first we know of to examine preferences for prognostic information in a sample of diverse older adults living with late-life disability. In previous quantitative studies, Fried and Kaplowitz found that a majority of (mostly white) patients would want to discuss the amount of time they might have left to live, and similar to our study, Fried demonstrated that patients’ desire to discuss prognosis increased as prognosis shortened.22,35 Our study extends those findings to a group of diverse older adults and adds a clinically relevant, in-depth understanding of how and why patients desire or do not desire to receive prognostic information. We found just one participant in our study who had previously discussed prognosis with their doctor, consistent with the contention that clinicians share prognosis less often than their patients would prefer.29,36-38 Participant perspectives in our study also supported those who have argued for clinician-initiated discussions of prognosis that are highly personalized,17 empathic,30 and begin with the explicit determination of each patient’s preferences for discussion.29 As evidence of the deeply personal nature of patient preferences for prognostic information, we noted that many patients viewed prognosis as uncertain, yet some saw this as a reason to avoid prognostic information, while others preferred that clinicians simply acknowledge uncertainty in their prognostic discussions (final quotes, Tables 2 and 3). Our results also added evidence that a thoughtful consideration of patients’ cultural backgrounds is warranted as preferences for communication may vary across racial and ethnic groups.
Specifically, our findings extend those of previous studies showing that preferences for prognostic information may be culturally influenced among Latino, African-American, and Asian-American elders. Morrison and Meier undertook a study of advance care planning across three groups (White, African-American, and Hispanic) in New York City, finding that while preferences for information across groups were similar, how and why patients preferred to discuss end of life issues differed in important respects.21 They, and others, have shown that Latinos’ attitudes in particular may differ notably from those in other ethnic groups.27,28,39,40 Latinos in our study described feeling more comfortable with the idea of discussing prognosis with a clinician from their same ethnic background, and were also more likely to express considerable concern over the emotional burdens associated with knowing prognosis. Published studies similarly show that older Asian-Americans may not want to discuss a poor prognosis and that many would prefer that family members take the lead in communicating with doctors.41,42 Yet we found that elderly Chinese-Americans were interested in prognostic information and that many of those who showed some initial reluctance ultimately expressed willingness to discuss prognosis at the doctor’s discretion. Further, Chinese-Americans in our study did not prefer that their family be told first of their prognosis, suggesting that such attitudes may be shifting over time, perhaps due to the spread of Western values through traditional Chinese-American communities. Taken together, these findings suggest that clinicians should be aware of the diversity of perspectives both between and within cultural groups when determining patients’ preferences for prognostic information.
Our primary finding, that a majority of participants across racial/ethnic groups preferred to discuss prognosis if their doctors believed they had less than 5 years to live, has broad clinical relevance as well, suggesting that clinicians should consider including prognostic estimation as a critical component of their care for older adults with late-life disability. Many participants in our study viewed a discussion of their prognosis as an opportunity and of knowing their estimated prognosis as a potential motivation to pursue concrete goals. Thus, prognostic estimates may serve as a meaningful framework within which older adults can prioritize among competing late-life demands: family and relationships, emotional well-being, spiritual or religious fulfillment, financial stability and legacy, medical care, long-term care enrollment, and others. Evidence from our study suggests that prognosis may help patients make medical decisions in the context of late life goal-setting and decision-making, potentially leading to more patient-centered outcomes.
It is important to consider the limitations of our study. Our sample of community-dwelling elders with late-life disability was drawn from a PACE program, which provided significant support for health care and related needs. In addition, our sample was selected based on subject availability and to ensure ethnic balance among participants. It is possible that the most readily available subjects were also healthier or had a more positive outlook than other potential interviewees. As a result, our study is not representative of larger populations of elders with late-life disability such as the large proportion of elders living in nursing homes. Moreover, because our sample was created to ensure ethnic representation above other considerations, future studies may wish to more closely examine the roles of other factors, such as gender, age, disability level, or quality of life, in determining preferences for prognosis. Indeed, this work is theory generating rather than hypothesis testing. As such, studies based on larger samples using quantitative measures comprise the next step in testing and refining our conclusions. In addition, there is evidence that information preferences for patients nearing the end of life may change as their condition deteriorates.15,35 However, our findings confirm that clinicians should take the time to determine patient preferences before disclosing prognostic estimates, a practice that would account for changing patient preferences. Finally, it is also possible that our participants underestimated the emotional burdens of knowing one’s prognosis. Yet, many of our participants proactively described strategies they would use to cope with this information.
As prognostic disclosure in clinical practice is rare, particularly for patients without a dominant terminal condition, our findings underscore the important potential that discussing prognosis may have in improving patient-centered care in the diverse population of older adults with late-life disability. Our findings further suggest that a carefully shared prognostic estimate can empower older adults in important areas of late-life beyond immediate medical decision-making. Clinicians interested in incorporating prognosis in their care for this population should engage in direct, empathic, clinician-initiated communication. Finally, while awareness of cultural attitudes is important, clinicians cannot generalize patients’ desires to discuss prognosis based on ethnicity, suggesting the importance of asking individuals about their preference.
References
Carey EC, Covinsky KE, Lui LY, Eng C, Sands LP, Walter LC. Prediction of mortality in community-living frail elderly people with long-term care needs. J. Am. Geriatr. Soc. 2008;56(1):68–75.
Carey EC, Walter LC, Lindquist K, Covinsky KE. Development and validation of a functional morbidity index to predict mortality in community-dwelling elders. J. Gen. Intern. Med. 2004;19(10):1027–1033.
Covinsky KE, Justice AC, Rosenthal GE, Palmer RM, Landefeld CS. Measuring prognosis and case mix in hospitalized elders. The importance of functional status. J Gen Intern Med. Apr. 1997;12(4):203–208.
Fried LP, Kronmal RA, Newman AB, et al. Risk factors for 5-year mortality in older adults: the Cardiovascular Health Study. JAMA. 1998;279(8):585–592.
Inouye SK, Peduzzi PN, Robison JT, Hughes JS, Horwitz RI, Concato J. Importance of functional measures in predicting mortality among older hospitalized patients. JAMA. 1998;279(15):1187–1193.
Saliba D, Elliott M, Rubenstein LZ, et al. The Vulnerable Elders Survey: a tool for identifying vulnerable older people in the community. J. Am. Geriatr. Soc. 2001;49(12):1691–1699.
Walter LC, Brand RJ, Counsell SR, et al. Development and validation of a prognostic index for 1-year mortality in older adults after hospitalization. JAMA. 2001;285(23):2987–2994.
American Geriatrics Society Clinical Practice Committee. Breast cancer screening in older women. J. Am. Geriatr. Soc. 2000;48(7):842–844.
Screening for breast cancer: recommendations and rationale. Ann Intern Med. Sep 3 2002;137(5 Part 1):344–346.
Berg AO. Screening for colorectal cancer: recommendations and rationale. Am. J. Nurs. 2002;102(9):107–117.
Holmes HM, Hayley DC, Alexander GC, Sachs GA. Reconsidering medication appropriateness for patients late in life. Arch. Intern. Med. 2006;166(6):605–609.
Lee SJ, Lindquist K, Segal MR, Covinsky KE. Development and validation of a prognostic index for 4-year mortality in older adults. JAMA. 2006;295(7):801–808.
Walter LC, Covinsky KE. Cancer screening in elderly patients: a framework for individualized decision making. JAMA. 2001;285(21):2750–2756.
Fried TR, Tinetti ME, Towle V, O'Leary JR, Iannone L. Effects of benefits and harms on older persons' willingness to take medication for primary cardiovascular prevention. Arch. Intern. Med. 2011;171(10):923–928.
Butow PN, Maclean M, Dunn SM, Tattersall MH, Boyer MJ. The dynamics of change: cancer patients' preferences for information, involvement and support. Ann. Oncol. 1997;8(9):857–863.
Bradley EH, Hallemeier AG, Fried TR, et al. Documentation of discussions about prognosis with terminally ill patients. Am. J. Med. 2001;111(3):218–223.
Clayton JM, Butow PN, Tattersall MH. When and how to initiate discussion about prognosis and end-of-life issues with terminally ill patients. J. Pain Symptom Manage. 2005;30(2):132–144.
Fallowfield LJ, Jenkins VA, Beveridge HA. Truth may hurt but deceit hurts more: communication in palliative care. Palliat. Med. 2002;16(4):297–303.
Jenkins V, Fallowfield L, Saul J. Information needs of patients with cancer: results from a large study in UK cancer centres. Br. J. Cancer. 2001;84(1):48–51.
Yeo G. How will the U. healthcare system meet the challenge of the ethnogeriatric imperative. J. Am. Geriatr. Soc. 2009;57(7):1278–1285.
Morrison RS, Meier DE. High rates of advance care planning in New York City's elderly population. Arch Intern Med. 2004;164(22):2421–2426.
Fried TR, Bradley EH, O'Leary J. Prognosis communication in serious illness: perceptions of older patients, caregivers, and clinicians. J. Am. Geriatr. Soc. 2003;51(10):1398–1403.
Huang X, Butow P, Meiser B, Goldstein D. Attitudes and information needs of Chinese migrant cancer patients and their relatives. Aust. N. Z. J. Med. 1999;29(2):207–213.
Orona CJ, Koenig BA, Davis AJ. Cultural aspects of nondisclosure. Camb. Q. Healthc. Ethics. 1994;3(3):338–346.
Jiang Y, Liu C, Li JY, et al. Different attitudes of Chinese patients and their families toward truth telling of different stages of cancer. Psychooncology. 2007;16(10):928–936.
Yun YH, Kwon YC, Lee MK, et al. Experiences and attitudes of patients with terminal cancer and their family caregivers toward the disclosure of terminal illness. J. Clin. Oncol. 2010;28(11):1950–1957.
Cohen MJ, McCannon JB, Edgman-Levitan S, Kormos WA. Exploring attitudes toward advance care directives in two diverse settings. J. Palliat. Med. 2010;13(12):1427–1432.
Perkins HS, Geppert CM, Gonzales A, Cortez JD, Hazuda HP. Cross-cultural similarities and differences in attitudes about advance care planning. J. Gen. Intern. Med. 2002;17(1):48–57.
Elkin EB, Kim SH, Casper ES, Kissane DW, Schrag D. Desire for information and involvement in treatment decisions: elderly cancer patients' preferences and their physicians' perceptions. J. Clin. Oncol. 2007;25(33):5275–5280.
Wenrich MD, Curtis JR, Ambrozy DA, Carline JD, Shannon SE, Ramsey PG. Dying patients' need for emotional support and personalized care from physicians: perspectives of patients with terminal illness, families, and health care providers. J. Pain Symptom Manage. 2003;25(3):236–246.
Eng C, Pedulla J, Eleazer GP, McCann R, Fox N. Program of All-inclusive Care for the Elderly (PACE): an innovative model of integrated geriatric care and financing. J. Am. Geriatr. Soc. 1997;45(2):223–232.
Glaser B, Strauss A. Discovery of Grounded Theory. Strategies for Qualitative Research: Sociology Press, 1967.
Strauss A, Corbin J. Basics of Qualitative Research. Thousand Oaks. CA: Sage; 1998.
Sandelowski M. Sample size in qualitative research. Res. Nurs. Health. 1995;18(2):179–183.
Kaplowitz SA, Campo S, Chiu WT. Cancer patients' desires for communication of prognosis information. Health Commun. 2002;14(2):221–241.
Christakis NA, Iwashyna TJ. Attitude and self-reported practice regarding prognostication in a national sample of internists. Arch. Intern. Med. 1998;158(21):2389–2395.
Curtis JR, Patrick DL, Caldwell ES, Collier AC. Why don't patients and physicians talk about end-of-life care? Barriers to communication for patients with acquired immunodeficiency syndrome and their primary care clinicians. Arch. Intern. Med. 2000;160(11):1690–1696.
Lamont EB, Christakis NA. Prognostic disclosure to patients with cancer near the end of life. Ann. Intern. Med. 2001;134(12):1096–1105.
Blackhall LJ, Murphy ST, Frank G, Michel V, Azen S. Ethnicity and attitudes toward patient autonomy. JAMA. 1995;274(10):820–825.
Kelley AS, Wenger NS, Sarkisian CA. Opiniones: end-of-life care preferences and planning of older Latinos. J. Am. Geriatr. Soc. 2010;58(6):1109–1116.
Blackhall LJ, Frank G, Murphy S, Michel V. Bioethics in a different tongue: the case of truth-telling. J. Urban Health. 2001;78(1):59–71.
Mitchell JL. Cross-cultural issues in the disclosure of cancer. Cancer Pract. 1998;6(3):153–160.
Acknowledgements
All authors included in this manuscript have contributed sufficiently to the project to be included as authors. Every person who contributed to the writing of this manuscript is listed as an author.
Funders
Dr. Smith was supported by a pilot grant from the Center for Aging in Diverse Communities, grant no. P30-AG15272 of the Resource Centers for Minority Aging Research program funded by the National Institute on Aging, National Institutes of Health. Additional support was provided by the National Center for Research Resources UCSF-CTSI (UL1 RR024131), Atlantic Philanthropies, the Society of General Internal Medicine, the John A. Hartford Foundation, and the Association of Specialty Professors.
Prior Presentations
This paper has not been previously presented.
Conflicts of Interest
None disclosed.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(DOC 26 kb)
Rights and permissions
About this article
Cite this article
Ahalt, C., Walter, L.C., Yourman, L. et al. “Knowing is Better”: Preferences of Diverse Older Adults for Discussing Prognosis. J GEN INTERN MED 27, 568–575 (2012). https://doi.org/10.1007/s11606-011-1933-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-011-1933-0