
Abstract
Background
Family members of patients in intensive care units (ICUs) are at risk for mental health morbidity both during and after a patient’s ICU stay.
Objectives
To determine prevalences of and factors associated with anxiety, depression, posttraumatic stress and complicated grief in family members of ICU patients.
Design
Prospective, longitudinal cohort study.
Participants
Fifty family members of patients in ICUs at a large university hospital participated.
Measurements
We used the Control Preferences Scale to determine participants’ role preferences for surrogate decision-making. We used the Hospital Anxiety and Depression Scale, Impact of Event Scale, and Inventory of Complicated Grief to measure anxiety and depression (at enrollment, 1 month, 6 months), posttraumatic stress (6 months), and complicated grief (6 months).
Results
We interviewed all 50 participants at enrollment, 39 (78%) at 1 month, and 34 (68%) at 6 months. At the three time points, anxiety was present in 42% (95% CI, 29–56%), 21% (95% CI, 10–35%), and 15% (95% CI, 6–29%) of participants. Depression was present in 16% (95% CI, 8–28%), 8% (95% CI, 2–19%), and 6% (95% CI, 1–18%). At 6 months, 35% (95% CI, 21–52%) of participants had posttraumatic stress. Of the 38% who were bereaved, 46% (95% CI, 22–71%) had complicated grief. Posttraumatic stress was not more common in bereaved than nonbereaved participants, and neither posttraumatic stress nor complicated grief was associated with decision-making role preference or with anxiety or depression during the patient’s ICU stay.
Conclusions
Symptoms of anxiety and depression diminished over time, but both bereaved and nonbereaved participants had high rates of posttraumatic stress and complicated grief. Family members should be assessed for posttraumatic stress and complicated grief.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
INTRODUCTION
Family members of patients in intensive care units (ICUs) are at risk for mental health morbidity both during and after the ICU stay. In large observational studies conducted in France, for example, Pochard et al. found that 69% of these family members had anxiety and 35% had depression early in their relative’s ICU stay,1 while 73% had anxiety and 35% had depression in the days preceding their relative’s ICU discharge or death.2 After patient discharge or death, family members develop posttraumatic stress related to the ICU experience, and bereaved family members are at risk for complicated grief.3–6 When Siegel et al. surveyed U.S. family members within 1 year of their relative’s death, 34% met criteria for at least one psychiatric illness and 5% had complicated grief disorder.6
Research to date has measured family members’ psychiatric symptoms either during or after the patients’ ICU stay, but it is unclear whether family members with anxiety and depression in the ICU are the same family members who later develop posttraumatic stress and complicated grief. Also, we are only beginning to understand how family members’ involvement in ICU decision-making might affect later development of these syndromes. Azoulay et al. found that family members who were more involved in decisions were more likely to have posttraumatic stress symptoms 3 months later.3 In the USA, Tilden et al. found that both oral and written advance directives decreased family members’ risk of posttraumatic stress.5 In our recent study of family members of ICU patients, we found that those who preferred to play a passive role in decision-making about their relative’s care were at greater risk for both anxiety and depression.7 The relationship between relatives’ self-stated role preferences in the ICU and posttraumatic stress and complicated grief has not been investigated.
In this paper, we report the results of our longitudinal cohort study of ICU family members. We had three goals: (1) to describe the frequency of symptoms of anxiety and depression in the cohort over time; (2) to describe the frequency of posttraumatic stress symptoms and complicated grief 6 months after enrollment; (3) to examine whether anxiety, depression, and decision-making role preference during a patient’s ICU stay are associated with posttraumatic stress symptoms and complicated grief.
MATERIALS AND METHODS
Study Setting and Participants
Our study took place at a large University hospital in Pittsburgh, Pennsylvania, where we recruited from several types of ICUs: four medical (32 beds), three surgical and trauma (40 beds), one cardiothoracic (20 beds), one neurologic (20 beds), one cardiac (10 beds), and one transplant (28 beds).
We recruited adult family members of 50 patients whose attending physicians anticipated an ICU stay of more than 2 days. For each patient, we enrolled the family member identified by the patient’s family and medical team as the primary decision-maker (the patient’s next-of-kin or designated power of attorney for health care). To maximize recruitment, we included family members of patients at any point in the ICU stay. The Institutional Review Board at the University of Pittsburgh approved the study, and all participants provided written informed consent.
Study Procedures and Measures
Participant enrollment was coordinated through the Clinical Trials Program of the Department of Critical Care Medicine at the University of Pittsburgh. During the enrollment period, research nurses visited the designated ICUs twice per week and asked each unit’s nursing coordinator for a census of patients who a) they expected to be in the ICU for more than 2 days and b) were unable to make medical decisions and so required a surrogate. If the patient’s next-of-kin was present in the ICU or waiting room, the patient’s care nurse asked the next-of-kin whether we could approach them about the study. Family members who agreed met with a research nurse, were informed about the study procedures, and completed a consent form. Enrollment continued until we reached our goal of 50 relatives.
At enrollment, we asked participating family members to provide at least two telephone numbers, so we could contact them for follow-up interviews. We collected sociodemographic data about each participant, including his or her age, gender, ethnicity, race, education, religion, and relationship to the patient. We assessed the participant’s preference for involvement in decisions about the patient’s medical care using the Control Preferences Scale8,9 modified for surrogate decision-making.10,11 This scale distinguishes among levels of responsibility in decision-making (active, shared, and passive) and has been successfully used in ICU family members.10,11 To measure symptoms of anxiety and depression, we used the Hospital Anxiety and Depression Scale (HADS).12 The HADS is valid and reliable,13 is easy to administer, and has been successfully used to measure symptoms of anxiety and depression in the general population and in family members of ICU patients.1–3,14 Because this was a feasibility study, we did not collect patient data in the ICU.
One month after enrollment, we contacted each participant by telephone to determine whether his or her relative was still alive and to assess the participant again for symptoms of anxiety and depression. We tried to reach the participant by calling at various times (during daytime and evening hours on weekdays and weekends) and via all phone numbers provided at enrollment. For patients with message-recording devices, we left two messages explaining the purpose of the call and requesting a callback. Participants were considered lost to follow-up if they could not be contacted or were unable to schedule an interview after seven calls.
At 6 months after enrollment, we repeated the process of contacting each participant and determining whether his or her relative was still alive. At this point, we assessed for anxiety, depression, and posttraumatic stress in all participants and for complicated grief in those whose relative had died. To measure posttraumatic stress symptoms, we used the Impact of Event Scale (IES), a valid and reliable scale that has been used successfully in family members of ICU patients.3–5,14–16 To assess for complicated grief, we used the Inventory of Complicated Grief (ICG) to distinguish between complicated bereavement and normal bereavement.17–19
Analyses
First, we converted scores on the HADS subscales, IES, and ICG into dichotomous variables. Based on cutoffs used in previous studies, we considered HADS subscale scores >10 to indicate the presence of symptoms of anxiety or depression,1–3,13,14 IES scores >30 to indicate the presence of symptoms of posttraumatic stress,3,14 and ICG scores >25 to indicate the presence of complicated grief.19,20 Because some studies have used higher cutoffs for the ICG,21,22 we also analyzed our data using a more conservative cutoff of >32. We summarized discrete variables in terms of frequencies and continuous variables in terms of central tendency and variability. We calculated 95% confidence intervals around the estimates for prevalence of anxiety, depression, PTSD, and complicated grief.
Second, to compare the proportions of participants who had anxiety or depression at enrollment, 1 month, and 6 months, we used the McNemar test for paired proportions.
Third, we tested for associations between the presence of posttraumatic stress symptoms and complicated grief at 6 months and the following variables: the status of the patient (living or deceased), the participant’s sociodemographic factors, the presence of symptoms of anxiety and depression in the participant at enrollment, and the participant’s stated decision-making role preference at enrollment. For this, we used two-tailed t-tests for continuous variables (age, which was normally distributed), the Pearson chi-square test for discrete variables, and Fischer’s exact test if appropriate. We used the Kruskal-Wallis test to examine associations between the variables and the Control Preferences Scale, which is a five-category ordinal scale. We also used these tests to compare sociodemographic factors, decision-making role preferences, and anxiety and depression scores of participants who completed the 6-month interview with those of participants who were lost to follow-up. We did not perform multivariate analyses for posttraumatic stress and complicated grief, because our sample size was small and because we did not find any associations with these variables in univariate analyses.
We used SPSS 11 for Macintosh (SPSS Inc, Chicago, IL) to perform all statistical analyses.
RESULTS
Characteristics of Study Participants
Between July 2006 and February 2007, we enrolled 50 participants. Our initial consent rate was 63%. The participants’ sociodemographic characteristics are shown in Table 1. Their mean age was 54 years. Most were white, Christian, and female and about one-third had attended college. The participants were the patient’s spouse (36%), parent (26%), child (12%), sibling, niece, or nephew (6%), or of unknown relationship (20%).
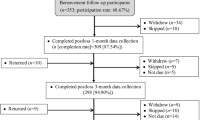
Follow-up data were available for 39 participants (78%) at 1 month and 34 (68%) at 6 months. At the 6-month follow-up, 13 participants (38%) were bereaved. At the 1-month time point, we were unable to complete interviews in 11 cases for several reasons: participant could not find a time to schedule an interview (n = 5), did not answer the phone (n = 2), did not want to participate (n = 2), had a telephone that was not in service (n = 1), or was in emotional distress (n = 1). At the 6-month time point, we were unable to complete interviews in five additional cases because a participant could not find a time to schedule an interview (n = 3) or did not answer the phone (n = 2). We found no significant association between failure to complete the 6-month interview and the participant’s sociodemographic characteristics, relationship to the patient, decision-making role preference, or presence of anxiety or depression at enrollment.
Anxiety
Symptoms of anxiety among participants decreased over the 6-month follow-up period. The mean HADS anxiety score was 10 (SD, 4; range, 2–21; median, 10) at enrollment. It dropped to 7 (SD, 5; range, 0–19; median, 6) at 1 month and decreased to 6 (SD, 4; range, 0–16; median, 5) at 6 months. Using a cutoff score of >10, we found that the proportions of participants with symptoms of anxiety at enrollment, 1 month, and 6 months were 42% (95% CI, 29–56%), 21% (95% CI, 10–35%), and 15% (95% CI, 6–29%), respectively (Table 2). The proportion at enrollment was significantly higher than the proportion at 1 month (p = .04) or 6 months (p = .008).
Associations of variables with symptoms of anxiety at enrollment have been reported elsewhere.7 The only variable that remained associated with anxiety at 1 month was young age. The mean age of participants with anxiety was 46 years (SD, 10), while the mean age of participants without anxiety was 57 years (SD, 12) (p = .02). At the 6-month follow-up, anxiety was not associated with age. At 1 month and 6 months, anxiety was not associated with other sociodemographic variables, relationship to patient, decision-making role preference, or patient status (living or deceased).
Depression
Symptoms of depression were less common than symptoms of anxiety at enrollment and follow-up (Table 2). The mean HADS depression score was 7 (SD, 4; range, 0–18; median, 6) at enrollment, and 4 at both 1 month (SD, 4; range, 0–15; median, 3) and 6 months (SD, 3; range, 0–12; median, 3). Using a cutoff score of >10, we found that the proportions of participants who had symptoms of depression at enrollment, 1 month, and 6 months were 16% (95% CI, 8–28%), 8% (95% CI, 2–19%), and 6% (95% CI, 1–18%), respectively (Table 2). The proportion at enrollment was not significantly different than the proportion at 1 month or 6 months.
Associations of variables with symptoms of depression at enrollment have been reported elsewhere.7 Again the only variable associated with depression at the 1-month follow-up was younger age. The mean age of participants with depression was 38 years (SD, 6), while the mean age of those without depression was 56 years (SD, 12) (p = .02). the At 6-month follow-up, depression was not associated with age. At 1 month and 6 months, depression was not associated with any other variables that were examined.
Posttraumatic Stress
Symptoms of posttraumatic stress were assessed only at 6 months. The mean IES score was 25 (SD, 19; range, 0–69; median, 21). Using a cutoff score of >30, we found that 12 participants (35%; 95% CI, 21–52%) had posttraumatic stress symptoms (Table 2).
Posttraumatic stress was not associated with anxiety at enrollment. There was a trend toward association between anxiety at 1 month and posttraumatic stress (p = .099), and an association between anxiety at 6 months and posttraumatic stress (p = .04). Posttraumatic stress was not associated with any other variables that were examined.
Complicated Grief
Symptoms of complicated grief were assessed only at the 6-month follow-up and only in bereaved participants. For the 13 bereaved participants, the mean ICG score was 22 (SD 12; range 5–41; median 18). Using a cutoff score of >25, we found that 6 (46%; 95% CI, 22–71%)) of the 13 bereaved participants had complicated grief (Table 2). When a cutoff score of >32 was used for the ICG, 3 (23%) had complicated grief.
The ICG was administered a mean of 185 days after the patient’s death (SD, 77; range, 10–280; median, 195). There was no association between the ICG score and the time that had lapsed between the patient’s death and the ICG administration.
Complicated grief was not associated with anxiety or depression at any time point (enrollment, 1 month, or 6 months). All bereaved participants with posttraumatic stress also had complicated grief (p = .001). There was a trend toward an association between complicated grief and education, with complicated grief present in 67% of participants who had attended college but in only 33% of those who had not (p = .1). All bereaved participants were Christian. Complicated grief was not associated with anxiety or depression at any study point (enrollment, 1 month, or 6 months) or with sociodemographic variables, relationship to patient, or decision-making role preference.
DISCUSSION
In our prospective longitudinal cohort study of 50 family members of ICU patients at a large university hospital in the United States, anxiety and depression decreased over the follow-up period, approximating rates in the general population at 6 months.13 Despite this, 35% of participants had symptoms of posttraumatic stress related to the ICU experience at 6 months, and 46% of bereaved participants had complicated grief at 6 months.
To our knowledge, our study is the first to measure both posttraumatic stress and complicated grief in family members of ICU patients, and only the second to describe the prevalence of complicated grief in ICU family members. The prevalences of posttraumatic stress and mean IES score in our sample are comparable to those of U.S., French, and British studies of bereaved and nonbereaved family members.3–5 Yet, the prevalence of complicated grief in our study (23%) was much greater than prevalence in the study of Siegel et al. (5%),6 even when we used a more conservative ICG cutoff. Though we used different instruments to measure complicated grief (the original ICG,19,20 versus the ICG-Revised23), it seems unlikely that this fully explains the discrepant estimates, suggesting true differences in prevalence between our studies. Larger, multicenter studies will be important to better estimate the prevalence rates.
The high prevalences of posttraumatic stress and complicated grief are concerning, because these disorders have a profound impact on physical, mental, and social functioning.3,19,21,24 Assessment and treatment of psychiatric disorders are important roles for primary care physicians,25–27 who are likely to be the first to encounter patients with mental disorders. Our results indicate that patients with a family member in the ICU should be screened for acute anxiety and depression during the ICU experience and for posttraumatic stress and complicated grief after the patients’ discharge or death. Screening for these specific disorders is important because, as this and other studies indicate, patients with these disorders may not have symptoms of anxiety and depression.28 Further, they often do not resolve without specific and intensive psychotherapeutic treatment.3,19,21,24 Although Azoulay et al. found that bereaved family members were more likely than nonbereaved family members to have posttraumatic stress,3 we did not find a difference between the two groups. Our results indicate that the negative effects of an ICU stay on family members’ psychological health is not limited to those who are bereaved. Thus, family members of patients who are still living should be screened as well.
It is unclear whether the lack of association between anxiety, depression, and decision-making role preference in the ICU and posttraumatic stress or complicated grief is authentic or is a result of our small sample size. The finding raises the question of whether the risk factors for anxiety and depression while the patient is in the ICU are the same as the risk factors for posttraumatic stress and complicated grief. Individuals who are distressed during a patient’s ICU stay may not be the same individuals who later develop mental illness; alternatively the effect of the ICU experience may attenuate after a few months. For example, in Tilden et al.’s study, bereaved family members who decided to withdraw life-sustaining treatments in the absence of an advance directive were more likely to have symptoms of posttraumatic stress 1–2 months later, but not at 6 months.5 Also, many risk factors for complicated grief, such as separation anxiety in childhood and dependency,29,30 are independent of the ICU experience. For now, our results suggest that family members of ICU patients should be assessed for posttraumatic stress and complicated grief even if they did not exhibit anxiety and depression during the patients’ ICU stay.
Our study had several limitations. First, our sample was small and demographically homogeneous, being predominantly female and white. Most studies of ICU caregivers have found a predominance of women,3,5,6,10,14,31 and the racial distribution of our study participants is typical of Pittsburgh, PA.31,32 However, our findings will need to be replicated in a larger multicenter study. Second, we collected data from family members of patients in different types of ICUs at different points in the patients’ ICU stay, and we included bereaved and nonbereaved family members. In future studies, it will be important to standardize data collection points (e.g., ICU admission and ICU discharge) and to measure patient-related and ICU-related factors. Third, we only used symptom scales to measure anxiety and depression, which may not adequately detect depression in ICU family members. In part, this may explain the lower prevalence of depression among our participants (6%) compared to bereaved participants in the Siegel et al. study (27%),6 which administered the Structured Clinical Interview for DSM-IV Disorders (SCID).33 Finally, our results could reflect bias introduced by enrollment practices or retention rates. For example, family members who were present in the ICU at the same time as the research nurse may have been systematically different from family members who could only visit on nights or weekends. It will be important in future studies to have study personnel available during evening and weekend hours to enroll family members. Also, family members who chose not to participate in the study may have been systematically different from those who did participate. Unfortunately, data collected at enrollment regarding sociodemographics, relationship to the patient, decision-making role preference, and symptoms of anxiety and depression are not available for family members who were approached but declined to participate in our study. However, when we compared these data from the group of individuals who completed follow-up and the group of individuals who were lost to follow-up, we found no differences.
Given the significant proportion of family members with posttraumatic stress and complicated grief after their ICU experience, it is critical that we better understand the risk factors for developing these syndromes. Some factors, such as communication and decision-making, are modifiable, but the ICU experience is an inherently stressful one for family members. Thus screening and appropriate referral becomes a critical step in curtailing the effects of this experience on family members’ physical, mental, and social functioning.
References
Pochard F, Azoulay E, Chevret S, et al. Symptoms of anxiety and depression in family members of intensive care unit patients: Ethical hypothesis regarding decision-making capacity. Crit Care Med. 2001;29:1893–1897.
Pochard F, Darmon M, Fassier T, et al. Symptoms of anxiety and depression in family members of intensive care unit patients before discharge or death. A prospective multicenter study. J Crit Care. 2005;20:90–96.
Azoulay E, Pochard F, Kentish-Barnes N, et al. Risk of post-traumatic stress symptoms in family members of intensive care unit patients. Am J Respir Crit Care Med. 2005;171:987–994.
Jones C, Skirrow P, Griffiths RD, et al. Post-traumatic stress disorder-related symptoms in relatives of patients following intensive care. Intensive Care Med. 2004;30:456–460.
Tilden VP, Tolle SW, Nelson CA, Fields J. Family decision-making to withdraw life-sustaining treatments from hospitalized patients. Nurs Res. 2001;50:105–115.
Siegel MD, Hayes E, Vanderwerker LC, Loseth DB, Prigerson HG. Psychiatric illness in the next-of-kin of patients who die in the intensive care unit. Crit Care Med. 2008;36:1722–1728.
Anderson WG, Arnold RM, Angus DC, Bryce CL. Passive decision-making preference is associated with anxiety and depression in relatives of patients in the intensive care unit. Journal of Critical Care. in press
Degner LF, Sloan JA. decision-making during serious illness: what role do patients really want to play? J Clin Epidemiol. 1992;45:941–950.
Degner LF, Sloan JA, Venkatesh P. The control preferences scale. Can J Nurs Res. 1997;29:21–43.
Heyland DK, Rocker GM, O’Callaghan CJ, Dodek PM, Cook DJ. Dying in the ICU: Perspectives of family members. Chest. 2003;124:392–397.
Heyland DK, Cook DJ, Rocker GM, et al. Decision-making in the ICU: perspectives of the substitute decision-maker. Intensive Care Med. 2003;29:75–82.
Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67:361–370.
Herrmann C. International experiences with the Hospital Anxiety and Depression Scale-A review of validation data and clinical results. J Psychosom Res. 1997;42:17–41.
Lautrette A, Darmon M, Megarbane B, et al. A communication strategy and brochure for relatives of patients dying in the ICU. N Engl J Med. 2007;356:469–478.
Sundin EC, Horowitz MJ. Impact of Event Scale: psychometric properties. Br J Psychiatry. 2002;180:205–209.
Horowitz M, Wilner N, Alvarez W. Impact of event scale: a measure of subjective stress. Psychosom Med. 1979;41:209–218.
Prigerson HG, Bierhals AJ, Kasl SV, et al. Complicated grief as a disorder distinct from bereavement-related depression and anxiety: a replication study. Am J Psychiatry. 1996;153:1484–1486.
Prigerson HG, Frank E, Kasl SV, et al. Complicated grief and bereavement-related depression as distinct disorders: Preliminary empirical validation in elderly bereaved spouses. Am J Psychiatry. 1995;152:22–30.
Prigerson HG, Maciejewski PK, Reynolds CFr, et al. Inventory of complicated grief: a scale to measure maladaptive symptoms of loss. Psychiatry Res. 1995;59:65–79.
Shear MK, Frank E, Foa E, et al. Traumatic grief treatment: a pilot study. Am J Psychiatry. 2001;158:1506–1508.
Shear K, Frank E, Houck PR, Reynolds CF 3rd. Treatment of complicated grief: a randomized controlled trial. JAMA. 2005;293:2601–2608.
Prigerson HG, Bridge J, Maciejewski PK, et al. Influence of traumatic grief on suicidal ideation among young adults. Am J Psychiatry. 1999;156:1994–1995.
Prigerson HG, Jacobs SC. Perspectives on care at the close of life. Caring for bereaved patients: “All the doctors just suddenly go”. JAMA. 2001;286:1369–1376.
Keane TM, Marshall AD, Taft CT. Posttraumatic stress disorder: etiology, epidemiology, and treatment outcome. Annu Rev Clin Psychol. 2006;2:161–197.
Tylee A, Walters P. Underrecognition of anxiety and mood disorders in primary care: why does the problem exist and what can be done? J Clin Psychiatry. 2007;68Suppl 227–30.
Gelenberg AJ, Hopkins HS. Assessing and treating depression in primary care medicine. Am J Med. 2007;120:105–108.
Bobo WV, Warner CH, Warner CM. The management of post traumatic stress disorder (PTSD) in the primary care setting. South Med J. 2007;100:797–802.
Lichtenthal WG, Cruess DG, Prigerson HG. A case for establishing complicated grief as a distinct mental disorder in DSM-V. Clin Psychol Rev. 2004;24:637–662.
Vanderwerker LC, Jacobs SC, Parkes CM, Prigerson HG. An exploration of associations between separation anxiety in childhood and complicated grief in later life. J Nerv Ment Dis. 2006;194:121–123.
Johnson JG, Vanderwerker LC, Bornstein RF, Zhang B, Prigerson HG. Development and validation of an instrument for the assessment of dependency among bereaved persons. J Psychopath Beh Ass. 2006;28:263–272.
Van Pelt DC, Milbrandt EB, Qin L, et al. Informal caregiver burden among survivors of prolonged mechanical ventilation. Am J Respir Crit Care Med. 2007;175:167–173.
Census Pittsburgh Census data, http://www.hellopittsburgh.com/Census.Cfm. Accessed June, 2008.
First M, Spitzer R, Gibbon M. Structured Clinical Interview for DSM-IV Axis I Disorders-Patient Edition (SCID-1/P, Version 2.0). New York: Biometrics Research Department, New York State Psychiatric Institute; 1995
Acknowledgements
The University of Pittsburgh’s Institute for Doctor–Patient Communication and The Greenwall Foundation supported this project. The Open Society Institute and the Senator H. John Heinz III Fellowship in Palliative Medicine at the University of Pittsburgh’s Institute to Enhance Palliative Care funded Dr. Anderson’s salary. The authors would like to thank Sharon Maddox for her critical review of the manuscript.
Conflict of interest statement
None disclosed.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Anderson, W.G., Arnold, R.M., Angus, D.C. et al. Posttraumatic Stress and Complicated Grief in Family Members of Patients in the Intensive Care Unit. J GEN INTERN MED 23, 1871–1876 (2008). https://doi.org/10.1007/s11606-008-0770-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-008-0770-2