
Abstract
Unlike developed countries, we find a bell-shaped curve for the average frequency of depressive symptoms from the Indonesian Family Life Survey where the same people are followed over 14 years (2000–2014). This incidence is at a high level around the age of 60 and lower for younger and older people. If we may assume that a high incidence of depressive symptoms goes together with a low average of mental health then we may conclude that the average mental health is at at a low level around 60 and higher for younger and older people (U-shape). In addition, we provide evidence for the first time that positive future expectations of one’s physical health significantly reduces incidence of depressive symptoms after accounting for reverse causality. This is however contingent on gender as optimistic health expectation is effective for male but not for female. This effect is also more pronounced for those 60 years and below as well as urban residents. However, the association of health optimism with incidence of depressive symptoms weakens with age. Results from this paper show that a focus on rural/urban residency, younger and older age cohorts and gender can provide targeted social policies to effectively promote better mental health.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Never has mental health become a more important issue since the onset of COVID-19. The 2020 pandemic has brought mental health to the fore as it raises anxiety levels and particularly, people’s insecurity about their health in the future to an extent not seen before. The global concern on mental health is however not limited to developed countries. The World Health Organization (2015) reported that 75% of people with mental disorders live in low- or middle-income countries and the majority of them do not have access to any kind of care.
Most studies on mental health (Ang, 2018; Fluharty et al., 2021; McIntosh et al., 2016) are on developed countries except for a few such as that on China (Chen et al., 2017), India (Amudhan et al., 2020), and Indonesia (Sujarwoto et al., 2019; Tampubolon & Hanandita, 2014). But these studies on developing economies are predominantly cross-sectional and hence are not robust or conclusive. To address this, this paper uses panel data on Indonesia to address the dearth of studies on developing countries. Indonesia is an appropriate case study as the prevalence of depression symptoms among Indonesians is consistent with the global average (Ferrari et al., 2013).
Mental health arises as a complex interaction between social, psychological, and biological factors (Fahmi et al., 2019). Amongst the psychological factors, findings show that positive expectation regarding the future may significantly influence mental well-being by the promotion of a healthy lifestyle as well as by adaptive behaviours and cognitive responses, such as greater flexibility, problem-solving capacity, and a more efficient elaboration of negative information (Conversano et al., 2010).
While our paper utilizes specific data regarding individuals' expectations concerning their future health, its primary focus lies in exploring the significance of these expectations on health outcome, rather than if expectations in themselves are rational. We aim to investigate how these expectations impact the incidence of depressive symptoms. The frequencies of depressive symptoms can be interpreted as a measure of mental health (Payne et al., 2014; Zhang & Harper, 2022). Therefore, this paper provides evidence on how these expectations influence public health through their impact on mental health.
The significance of expectations in shaping the overall quality of life has garnered heightened attention. This focus is particularly noteworthy in the realm of economics, with longstanding theories positing the pivotal role of income expectations in influencing happiness. Noteworthy examples include Senik's tunnel effect hypothesis (Senik, 2004) and Easterlin's theory of erroneous income expectations (Easterlin, 2001). The growing interest in the role of expectations stems from their potential implications for individual well-being and societal welfare, underscoring their relevance in economic analyses and policy considerations. For instance, studies have shown that positive income expectation for the future has value for the present times in terms of current happiness (Frijters et al., 2012; Knight & Gunatilaka, 2010), life satisfaction (Senik, 2008) and mental health (de Grip et al., 2012). Positive expectation of future consumption could also increase present consumption value (Brunnermeier & Parker, 2005) and hence provide happiness (Wang et al., 2019).
With health expectations, some studies have focused on patients’ expectation on health care or treatment outcomes to show that unmet health care expectation relates to recurrent medical visits for unresolved symptoms (McPhillips-Tangum et al., 2018), poorer adherence with treatment and lower satisfaction with health care (Bell et al., 2002). Another type of expectations research in health covers economic and social determinants of life expectancy and expectations regarding ageing (see Olshansky et al., 2005; Sarkisian et al., 2002). Although health expectations are integral to the quality of life in health (Skevington & McCrate, 2012), to date, the expectation of an individual’s health status (be it optimism or pessimism) and its effect on one’s mental health has not been examined and this is the focus of our paper.
In this paper, we intend to quantify the role of optimistic health expectations in keeping the good mental health with an example from a developing country. The main research questions we pursue are: what is the relationship between health expectations and incidence of depressive symptoms from the life course perspective? To what extent do these optimistic health expectations contribute to reducing incidence of depressive symptoms? And, how does this effect vary across different demographic groups? We try to answer these questions using a large-scale household survey conducted from 2000 to 2014. The survey contains information on both future health expectations and incidence of depressive symptoms, in addition to extensive information about socioeconomic characteristics and personality traits.
In doing so, this study contributes to the existing literature in several aspects. First, we are among the first to examine the impact of expectation regarding personal health on incidence of depressive symptoms. Second, we investigate whether and how the effect of health expectations on incidence of depressive symptoms changes with age. Ang (2018) notes that previous studies on mental health that include a wide age range do not consider trajectories of health over extended periods, and may be capturing health differences between cohorts instead of by age. This paper addresses both these limitations using growth curves. Third, we deal with endogeneity (due to potential reverse causation from incidence of depressive symptoms to health expectations) using instrumentation and explicitly analyse gender differences, rural/urban residency effects and different age cohorts. Our findings also point to the significance of social capital in the form of personal community engagement and strong community building in shaping Indonesians’ mental health.
Data and Variables
Data Source
This study makes use of data from the third (2000), fourth (2007) and fifth (2014) waves of the Indonesian Family Life Survey (IFLS). The IFLS was conducted by the RAND Corporation in 13 of the 27 provinces in Indonesia, representing 83% of the population. The high follow-up rate in IFLS enabled us to trace the same individual in their life course. In our baseline year of 2000, the total number of respondents is 28,340, while in 2007 there are 29,059 respondents and 34,464 in 2014. For this research, we consider adult respondents aged 20 years and above in 2000 and only include respondents who have no missing data for the chosen variables in all three waves. This provided a sample size of 12,183 respondents.
Variables
Measure of Incidence of Depressive Symptoms
Depressive symptoms are measured by the Center for Epidemiologic Studies Depression Scale (CESD-10), which has 10 items designed to evaluate self-reported current depressive symptoms severity in the general population (Andresen et al., 1994). The CESD-10 includes response categories that range from 0 to 3 with the ascending order indicating increasing frequency of depressive symptoms. The responses to the 10 items are then summed with a total score ranging from 0 to 30, where the larger (smaller) score refers to a higher (lower) frequency of depressive symptoms. A low (high) frequency of depressive symptoms is interpreted as a high (low) level of mental health.
Measure of Health Expectations
Information on health expectations is obtained from the following question, ‘How do you expect your health to be next year?’ Answers from the respondents are 1) much better than now 2) somewhat better than now 3) about the same 4) somewhat worse 5) much worse. These response categories are treated as continuous scores, which are then reverse-coded, with 1 referring to the lowest expectation and 5 referring to the highest expectation.
Control Variables
Age and age square are both included in the growth curve model to examine the non-linear effect of age. We also have the cohort indicator in the model, as illustrated in Ang (2018) and Yang and Lee (2010), to improve model fit. Moreover, growth curve models have the capability to generate precise age trajectories by accounting for cohort variations and considering the clustering of data within individuals (Raudenbush & Chan, 1992). Following Yang and Lee (2010), we group respondents into 5 birth cohorts (1970–1980 as cohort 1, 1960–1970 as cohort 2, 1950–1960 as cohort 3, 1940–1950 as cohort 4, and before 1940 as cohort 5), and the cohort indicator is a categorical variable in the model. Socioeconomic variables used in the analysis includes gender, education (elementary as 1, junior school as 2, senior school as 3, college and above as 4), rural/urban residency, marital status, self-valued living standards (1–3 is from less than adequate to more than adequate for my needs). We also control for the physical health of the respondents, with the general health measured from self-evaluation. We use a Likert scale response ranging from 1 (very unhealthy) to 4 (very healthy) which is recorded for the question of, ‘In general, how is your health?’.
The importance of social capital in maintaining good mental status has been shown in many studies (Ang, 2018; Miller et al., 2006; Nizeyumukiza et al., 2021). Therefore, we include social capital as one of the control variables. Following Cao and Rammohan (2016), we measure social capital from the individual’s perspective of his/her participation in the community (as a measure of social connections) Specifically, we add up the number of ‘yes’ responses to the following questions: Did you: (a) participate in community meetings? (b) participate in voluntary labour? (c) participate in programs to improve village/neighbourhood? and (d) participate in religious activities? The combined scores for community participation range from 0 to 4.
In addition, we control for one’s personality associated with health expectations as studies (Ahadi & Basharpoor, 2010; Lincoln, 2008) suggest that one’s personality has direct and indirect effects on psychological distress and this has implications for expectations on health. Personality is measured by the Big Five personality, which is a suggested taxonomy for personality traits, identifying Extraversion, Agreeableness, Openness to Experience, Conscientiousness and Neuroticism (Saucier & Goldberg, 1998).Footnote 1 The Big Five Inventory (BFI) is a self-reported inventory with 44 items, designed to measure an individual on the Big Five traits. Each item belongs to one of the five traits and is rated on a Likert scale from 1 (disagree a lot) to 5 (agree a lot). The score for one particular trait is calculated as the sum of its respective items, with some items reverse scored. The final highest score for each of the five personality types will be used to characterise that personality trait to be the primary personality.
Statistical Analysis
To investigate the effect of health expectations on incidence of depressive symptoms and whether this effect changes with the individual’s age, we apply the hierarchical linear models approach — specifically, growth curve models—for analysis of three waves of panel data. The growth curve model allows for the estimation of inter-individual variability in intra-individual patterns of change over time (Curran et al., 2010). All models are estimated using weights provided in the IFLS dataset to account for sample design and non-response, making the sample representative at each wave of the population.
Model specifications are represented by two equations. In the level-1 repeated observations model given by Eq. (1), each person’s growth trajectory in CES-D score is a function of age and other time-varying covariates. The level-2 model given by Eqs. (2) and (3) specifies a distinct average trajectory for each cohort and incorporates other time-invariant covariates associated with each individual. The first level describing the growth trajectory of incidence of depressive symptoms for each person is as follows:
where \({CESD}_{it}\) represents the CESD score of individual \(i\) at time \(t;\) \({\beta }_{0i}\) is the intercept of the trajectory of the CESD; \({Age}_{it}\) is the age for \(i\) at time \(t\), and \({X}_{j}{\prime}s\) are the time-varying covariates with the associated \(\beta {\prime}s\).
The level-2 model measures the effect of health expectations and other individual characteristics on the intercept and slopes in level-1 as seen in Eq. (1). Equations (2) and (3) represent the estimation for the intercept and slope respectively.
where \({Z}_{j}\) stands for the time-invariant variables, and \({Cohort}_{i}\) is coded 0–4 for cohorts 1–5. \({\gamma }_{00}\) is the expected CESD score for males in cohort one with mean level of education and health expectations at time one, namely the year of 2000. \({\gamma }_{01}\) is the mean difference in CESD between cohorts in the year 2000. In Eq. 3, the growth rate per year further varies by cohort and health expectations. \({\gamma }_{10}\) is the expected rate of change in CESD for cohort one with mean level of health expectations at time one. \({\gamma }_{11}\) represents the age-by-cohort interaction effect and \({\gamma }_{12}\) measures the magnitude regarding the effect of health expectations in CESD changing with ages. Finally, \({u}_{0i}\) and \({u}_{1i}\) are the residual random effects assumed to have a bivariate normal distribution. Maximum likelihood estimation is adopted and the Akaike information criterion (AIC) and Bayesian information criterion (BIC) statistics are used to assess goodness of fit.
Results
Descriptive Statistics
Table 1 presents the descriptive statistics for all variables considered in the analysis. Men account for about 45% of the sample and nearly 60% live in the urban areas. With respect to personality, over 38% report themselves as being agreeable, and only 2% are categorized as neurotic. Mean CESD score for the average respondent in 2014 is 5.56 which is higher than the mean CESD score of 3.9 in 2007. This shows a higher level of incidence of depressive symptoms (worsening mental health status) in Indonesia during this period of time. In terms of health expectation, on average, respondents expect their health status to be better than now, indicating that the population has an optimistic attitude towards their health. Additionally, we find negative and significant correlation coefficients between health expectation and age (-0.0715) as well as health expectation and cohort (-0.1731). These negative coefficients indicate that individuals tend to be less optimistic about their health as they age.
Health Expectations and Incidence of Depressive Symptoms
Table 2 shows results from the growth curve models that predict depressive symptoms. Models 1 and 2 which assess age effects with the presence of cohort effect only, show a quadratic age effect. Models 3 to 5 in Table 2 show that this age effect stays in the presence of health expectations and when progressively adjusted for the control variables. Respondents with higher health expectation are significantly more likely to report lower level in incidence of depressive symptoms (better mental health status) and this result is robust with the inclusion of control variables and personality traits. The interaction term between health expectations and age is positive and significant, showing that the positive influence of health expectations on mental health diminishes as one gets older.Footnote 2
It can also be seen that better education, better physical health status, and higher living standards, all negatively affect incidence of depressive symptoms (positively affect mental health) as expected. Compared with males, female show a higher CESD score similar to previous findings (Salk et al., 2017; Zhao et al., 2020). In addition, we find that married people and rural residents are less depressed compared to their counterparts. Evidence on the urban/rural residency effect on mental health in the literature is mixed (Kovess-Masféty, 2005; Li & Ma, 2017; Probst et al., 2006). Lastly, being involved in community activities helps decrease incidence of depressive symptoms, confirming the importance of social capital in mental health.
Variations by Age, Residency and Gender
As shown in Fig. 1, the turning point in the growth curve of CESD score for the general population is at the age of 60. Therefore, we separately estimate the effect for the group younger and older than 60 years as seen in Table 3. For the younger cohort presented in Model 1, we confirm the growth in incidence of depressive symptoms with age, but this is not significant in the older group presented in Model 2. With the covariates controlled, the effect of positive health expectations on incidence of depressive symptoms is significant in both age groups with the effect in the younger cohort being twice that of the older cohort. Education contributes to a decrease in the incidence of depressive symptoms among the older group, thereby enhancing their mental health. On the other hand, community participation is particularly advantageous for the younger group in terms of their mental health status.

Source: Computed from IFLS3, IFLS4 and IFLS5
Age Trajectories for Incidence of Depressive Symptoms from Unconditional Growth Curve Models.
Models 1 and 2 in Table 4 present results for the urban and rural areas respectively. For urban and rural residents, there is no significant difference in terms of the quadratic age growth trajectories of the CESD score. However, for urban residents, the effect from health expectations is higher than that for rural residents.
In both urban and rural areas, we examine female and male cohorts as seen from model 3 to model 6 in Table 4. Unlike males, there is no impact of health expectations for females regardless of where they reside. Education has a significant impact on incidence of depressive symptoms not only in urban Indonesia. Social capital significantly reduces incidence of depressive symptoms of women regardless of whether they live in urban or rural areas.
Endogeneity Issue and Sensitivity Analyses
This paper examines the impact of health expectations on incidence of depressive symptoms and how it varies with age, as discussed in the previous section. First, some studies have shown that current status of life satisfaction (Bertoni & Corazzini, 2018; Schwandt, 2016) and income (Knight and Gunatilaka (2010) has an effect on future expectations of the outcome variable of interest. Thus we check on the correlation coefficient of self-reported physical health status and future physical health expectations. This was no higher than 0.01 for the general population and the subgroups of males, females, urban and rural cohorts, thus ruling out any multicollinearity concerns in the estimations.
Second, there may be endogeneity due to reverse causality as it is possible that those who are less depressed are inherently positive about their health expectation. To check on this, we need to identify appropriate instrumental variables that influence health expectations without directly affecting incidence of depressive symptoms. Our main instrument is the financial budget position of the community/village where the respondents live. A healthy financial budget would provide residents with the confidence of better and more health facilities and increased transport facilities providing greater access to clinics and hospitals. This is likely to affect residents’ health expectations (and we have controlled for individual’s living standards) without directly affecting incidence of depressive symptoms. We select the module of community-facility in the IFLS answered by the community/village head or committee and use the question of, ‘What was the total budget for the village in the fiscal year?’ This response is a continuous variable as it was reported in Indonesian Rupees. Another instrument used is lagged health expectations. The health expectation in the previous wave (seven years ago) is unlikely to have a direct effect on the mental status today (in the current wave) but could affect respondent’s general level of health optimism.
Both instruments are valid given by the over-identification and strength of the instruments tests reported in Appendix Table 5. First-stage estimations in Appendix Table 5 show that individual health expectation is are significantly influenced by community/village financial budget and lagged health expectations. According to the IV estimate in Appendix Table 6, health expectations still negatively impact individual incidence of depressive symptoms, indicating a positive impact on mental health.
Third, to further check on the robustness of the results, we conduct sensitivity analyses using incidence of depressive symptoms measured as predicted scores of CESD. We use Ordinary Least Square regressions to first obtain predicted CESD scores with the same set of explanatory variables described above. Results in Appendix Table 6 confirm the bell-shaped curve in the age trajectory of depressed symptoms and support previous finding that health expectations have a beneficial role in depressive symptoms and that this effect diminishes with age.
Discussion
Three major findings emerge from this study. First, the age trajectory of depressive symptoms during the Indonesian adult life course is non-linear with a bell-shaped curve. This contrasts with the U-shaped age trajectory for depressive symptoms in developed countries such as the USA (Ang, 2018; Sutin et al., 2013) and England (Tampubolon & Maharani, 2017) while studies on developing country such as China (Hu et al., 2019; Wang et al., 2023) show a linear relationship. We find that adult mental health gets worse with the increase of age until 60 years and then improves in life after 60. This could be supported by Brockmann’s argument (Brockmann, 2010) that middle-aged people are generally in worst mental status, caused by the pressures from work and life. At every age, females’ CESD is higher than males but the turning point comes earlier for females at 58.6 years while it is 62 years for males.
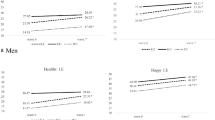
The second major finding is the significant negative effect of health expectation on incidence of depressive symptoms. That is, individuals who have better expectation for health, namely being optimistic about their future health, have better mental health than their pessimistic counterparts. This can be seen in Fig. 2 which shows that optimists have a lower CESD score than pessimists irrespective of whether they live in urban or rural area. The declining positive effect of health expectation with age noted earlier is also illustrated in Fig. 2. This can be seen by the narrowing of the trajectories representing the pessimists and optimists in both urban and rural areas. It shows that as people get older, the positive health expectation plays a smaller role compared with in their younger life in maintaining a better mental health condition.

Source: Computed from IFLS3, IFLS4 and IFLS5
Health Expectation and Incidence of Depressive Symptoms. Notes: Expect health to be somewhat better or much better than now is defined as being optimistic. Being pessimistic refers to expecting health to be somewhat worse or much worse.
Third, some differences emerge with respect to the various subgroups. For example, education benefits those above 60 (and not below that age) and this is due to the educated elderly having better access to information and awareness about mental health. Thus it is important to reach out to the less educated elderly in a more direct manner to make them aware of mental health issues and educate them to seek help and overcome any social stigma associated with depression, especially in less developed Asian countries such as Indonesia. On the other hand, the positive effect of community participation is only seen for those under the age of 60, and not those 60 and above. This could be explained by the possibility that the older cohort may be constrained in their community participation due to their lack of energy or weaker physical health than the younger cohort.
Lastly, better health expectations do not diminish the symptoms of depression in women in both urban and rural regions. But for men, positive expectations are a good way to improve their mental health. On the other hand, having more social capital (community participation) improves mental health more so for women than men irrespective of their residency location. This is in line with Riumallo-Herl et al., (2014) and Umberson et al., (1996) who show that social interactions have a greater impact on female than male depression.
Conclusion
This paper is the first to highlight the role of optimism about future health expectation and the effect of the association of health expectation with age on incidence of depressive symptoms. Using longitudinal data on Indonesia, we find that optimistic expectation helps reduce an individual’s depressive symptoms but this effect diminishes with the increase of age. This effect is particularly strong and important for those 60 years and younger and living in the urban area. These findings add to the body of knowledge on expectation, which has not previously been studied from a health perspective.
One limitation of the study is that we are unable to explain the mechanisms underlying these observed relationships as it is beyond the scope of this study. Thus a natural extension is to find why and in what ways optimistic health expectations reduce incidence of depressive symptoms, and the reasons for the declining effect of optimism with age on incidence of depressive symptoms. Another extension is to conduct similar research in other developing and developed countries to understand if there are any differences in the patterns of the age trajectory and CESD.
Another limitation of this study is that the quality of and accessibility to health facilities in the areas where the respondents live could not be considered due to lack of data. Do these affect health expectations or incidence of depressive symptoms directly? It is also unclear whether and how risky behaviours like smoking and drinking are related to health expectations and incidence of depressive symptoms.
Instead of using social capital as a control variable, it would be interesting to see for instance if social capital could negate the diminishing effect of health expectation with age on incidence of depressive symptoms. In this regard, specific dimensions of social capital such as social trust and social norms which were not examined in this paper could be used.
Despite the above limitations, the finding that health expectation constitutes a non-trivial determinant of incidence of depressive symptoms lends importance to the current situation of the Covid-19 pandemic whereby positive future prospects are critical. Thus governments of today need to be mindful of how well they manage the pandemic as this is likely to affect health expectations. Future studies could look at data collected before and after the epidemic to see if the influence of health anticipation has changed or how it affects incidence of depressive symptoms over time.
Notes
According to Saucier and Goldberg (1998), Extraversion reflects the individual's determination, leadership, enterprising and activeness; Agreeableness reflects the individual's cooperation with others, tolerance and trust to others; Openness reflects the individual's creativity, innovation and curiosity; Conscientiousness reflects the individual's sense of accomplishment and hard work; and Neuroticism reflects the individual's self-doubt, pessimism and inability to withstand stress.
Although the coefficient of the interaction term of health expectations and age is positive, it is very small. For instance, taking the first derivative to find the effect of health expectations at age 80 equals to -0.562 + (0.002 X 80) which is -0.366. That is, the effect of health expectations has declined for CESD from 0.562 to 0.366 for an individual aged 80.
References
Ahadi, B., & Basharpoor, S. (2010). Relationship between sensory processing sensitivity, personality dimensions and mental health. Journal of Applied Sciences, 10(7), 570–574.
Amudhan, S., Gururaj, G., Varghese, M., Benegal, V., Rao, G. N., Sheehan, D. V. et al. (2020). A population-based analysis of suicidality and its correlates: findings from the National Mental Health Survey of India, 2015–16. The Lancet Psychiatry, 7(1), 41–51.
Andresen, E. M., Malmgren, J. A., Carter, W. B., & Patrick, D. L. (1994). Screening for depression in well older adults: Evaluation of a short form of the CES-D. American Journal of Preventive Medicine, 10(2), 77–84.
Ang, S. (2018). Social participation and health over the adult life course: Does the association strengthen with age? Social Science & Medicine, 206, 51–59.
Bell, R. A., Kravitz, R. L., Thom, D., Krupat, E., & Azari, R. (2002). Unmet expectations for care and the patient-physician relationship. Journal of General Internal Medicine, 17(11), 817–824.
Bertoni, M., & Corazzini, L. (2018). Asymmetric affective forecasting errors and their correlation with subjective well-being. PLoS ONE, 13(3), e0192941.
Brockmann, H. (2010). Why are middle-aged people so depressed? Evidence from West Germany. Social Indicators Research, 97(1), 23–42.
Brunnermeier, M. K., & Parker, J. A. (2005). Optimal expectations. American Economic Review, 95(4), 1092–1118.
Cao, J., & Rammohan, A. (2016). Social capital and healthy ageing in Indonesia. BMC Public Health, 16(1), 1–14.
Chen, Y., Bennett, D., Clarke, R., Guo, Y., Yu, C., Bian, Z. et al. (2017). Patterns and correlates of major depression in Chinese adults: a cross-sectional study of 0.5 million men and women. Psychological Medicine. 47, 958–970.
Conversano, C., Rotondo, A., Lensi, E., Della Vista, O., Arpone, F., & Reda, M. A. (2010). Optimism and its impact on mental and physical well-being. Clinical Practice and Epidemiology in Mental Health, 6, 25–29.
Curran, P. J., Obeidat, K., & Losardo, D. (2010). Twelve frequently asked questions about growth curve modeling. Journal of Cognition and Development, 11(2), 121–136.
de Grip, A., Lindeboom, M., & Montizaan, R. (2012). Shattered dreams: The effects of changing the pension system late in the game. The Economic Journal, 122(559), 1–25.
Easterlin, R. A. (2001). Income and happiness: Towards a unified theory. The Economic Journal, 111(473), 465–484.
Fahmi, M., Panjaitan, N. A., Habibie, I., Siregar, A. Y., Amarullah, G., & Sunjaya, D. K. (2019). Does your neighborhood protect you from being depressed? A study on social trust and depression in Indonesia. BMC Public Health, 19(1), 1–8.
Ferrari, A. J., Somerville, A. J., Baxter, A. J., Norman, R., Patten, S. B., Vos, T., & Whiteford, H. A. (2013). Global variation in the prevalence and incidence of major depressive disorder: A systematic review of the epidemiological literature. Psychological Medicine, 43(3), 471.
Fluharty, M., Bu, F., Steptoe, A., & Fancourt, D. (2021). Coping strategies and mental health trajectories during the first 21 weeks of COVID-19 lockdown in the United Kingdom. Social Science & Medicine, 279, 113958.
Frijters, P., Liu, A. Y., & Meng, X. (2012). Are optimistic expectations keeping the Chinese happy? Journal of Economic Behavior & Organization, 81(1), 159–171.
Hu, Y., Li, P., & Martikainen, P. (2019). Rural-urban disparities in age trajectories of depression caseness in later life: The China Health and Retirement Longitudinal Study. PLoS ONE, 14(4), e0215907.
Knight, J., & Gunatilaka, R. (2010). Great expectations? The subjective well-being of rural–urban migrants in China. World Development, 38(1), 113–124.
Kovess-Masféty, V., Alonso, J., de Graaf, R., & Demyttenaere, K. (2005). A European approach to Rural—Urban differences in mental health: The ESEMeD 2000 comparative study. The Canadian Journal of Psychiatry, 50(14), 926–936.
Li, J. S., & Ma, W. J. (2017). Prevalence and influencing factors of depression symptom among middle-aged and elderly people in China. Chinese Journal of Public Health, 33, 177–181.
Lincoln, K. D. (2008). Personality, negative interactions, and mental health. Social Service Review, 82(2), 223–252.
McIntosh, A. M., Stewart, R., John, A., Smith, D. J., Davis, K., Sudlow, C. et al. (2016). Data science for mental health: a UK perspective on a global challenge. The Lancet Psychiatry, 3(10), 993-998
McPhillips-Tangum, C. A., Cherkin, D. C., Rhodes, L. A., & Markham, C. (2018). Reasons for Repeated Medical Visits Among Patients with Chronic Back Pain. Journal of General Internal Medicine, 13(5), 289–295.
Miller, D. L., Scheffler, R., Lam, S., Rosenberg, R., & Rupp, A. (2006). Social capital and health in Indonesia. World Development, 34(6), 1084–1098.
Nizeyumukiza, E., Pierewan, A. C., Ndayambaje, E., & Ayriza, Y. (2021). Social Capital and Mental Health among Older Adults in Indonesia: A Multilevel Approach. Journal of Population and Social Studies, 29, 1–14.
Olshansky, S. J., Passaro, D. J., Hershow, R. C., Layden, J., Carnes, B. A., Brody, J. et al. (2005). A potential decline in life expectancy in the United States in the 21st century. New England Journal of Medicine, 352(11), 1138–1145.
Payne, C., Hedberg, E. C., Kozloski, M., Dale, W., & McClintock, M. K. (2014). Using and interpreting mental health measures in the National Social Life, Health, and Aging Project. Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 69((Suppl_2)), S99–S116.
Probst, J. C., Laditka, S. B., Moore, C. G., Harun, N., Powell, M. P., & Baxley, E. G. (2006). Rural-urban differences in depression prevalence: Implications for family medicine. Family Medicine, 38(9), 653.
Raudenbush, S. W., & Chan, W. S. (1992). Growth curve analysis in accelerated longitudinal designs. Journal of Research in Crime and Delinquency, 29(4), 387–411.
Riumallo-Herl, C. J., Kawachi, I., & Avendano, M. (2014). Social capital, mental health and biomarkers in Chile: Assessing the effects of social capital in a middle-income country. Social Science & Medicine, 105, 47–58.
Salk, R. H., Hyde, J. S., & Abramson, L. Y. (2017). Gender differences in depression in representative national samples: Meta-analyses of diagnoses and symptoms. Psychological Bulletin, 143(8), 783. https://doi.org/10.1037/bul0000102
Sarkisian, C. A., Hays, R. D., & Mangione, C. M. (2002). Do older adults expect to age successfully? The association between expectations regarding aging and beliefs regarding healthcare seeking among older adults. Journal of the American Geriatrics Society, 50(11), 1837–1843.
Saucier, G., & Goldberg, L. R. (1998). What is beyond the Big Five? Journal of Personality, 66, 495–524.
Schwandt, H. (2016). Unmet aspirations as an explanation for the age U-shape in wellbeing. Journal of Economic Behavior & Organization, 122, 75–87.
Senik, C. (2004). When information dominates comparison: Learning from Russian subjective panel data. Journal of Public Economics, 88(9–10), 2099–2123.
Senik, C. (2008). Is man doomed to progress? Journal of Economic Behavior & Organization, 68(1), 140–152.
Skevington, S. M., & McCrate, F. M. (2012). Expecting a good quality of life in health: assessing people with diverse diseases and conditions using the WHOQOL‐BREF. Health Expectations, 15(1), 49–62.
Sujarwoto, S., Tampubolon, G., & Pierewan, A. C. (2019). A tool to help or harm? Online social media use and adult mental health in Indonesia. International Journal of Mental Health and Addiction, 17(4), 1076–1093.
Sutin, A. R., Terracciano, A., Milaneschi, Y., An, Y., Ferrucci, L., & Zonderman, A. B. (2013). The trajectory of depressive symptoms across the adult life span. JAMA Psychiatry, 70(8), 803–811.
Tampubolon, G., & Hanandita, W. (2014). Poverty and mental health in Indonesia. Social Science & Medicine, 106, 20–27.
Tampubolon, G., & Maharani, A. (2017). When did old age stop being depressing? Depression trajectories of older Americans and Britons 2002–2012. The American Journal of Geriatric Psychiatry, 25(11), 1187–1195.
Umberson, D., Chen, M. D., House, J. S., Hopkins, K., & Slaten, E. (1996). The effect of social relationships on psychological well-being: Are men and women really so different? American Sociological Review, 837–857. https://doi.org/10.2307/2096456
Wang, H., Cheng, Z., & Smyth, R. (2019). Consumption and Happiness. Journal of Development Studies, 55(1), 120–136.
Wang, S., Lu, T., Sun, J., Huang, L., Li, R., Wang, T., & Yu, C. (2023). Long-term trends in the incidence of depressive disorders in China, the United States, India and globally: A comparative study from 1990 to 2019. Frontiers in Psychology, 13, 1066706.
World Health Organization (2015). Update of the Mental Health Gap Action Programme Guidelines for Mental, Neurological and Substance Use Disorders, 2015. Geneva: World Health Organization. Available in https://pubmed.ncbi.nlm.nih.gov/26937539/
Yang, Y., & Lee, L. C. (2010). Dynamics and heterogeneity in the process of human frailty and aging: Evidence from the US older adult population. Journals of Gerontology Series b: Psychological Sciences and Social Sciences, 65(2), 246–255.
Zhang, Y., & Harper, S. (2022). The impact of son or daughter care on Chinese older adults’ mental health. Social Science & Medicine, 306, 115104.
Zhao, L., Han, G., Zhao, Y., Jin, Y., Ge, T., Yang, W. et al. (2020). Gender differences in depression: evidence from genetics. Frontiers in Genetics, 11, 1145. https://doi.org/10.3389/fgene.2020.562316
Funding
We are supported by Guangdong Planning Office of Philosophy and Social Science, with the Grant Number: GD23XGL002.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Fan, S., Mahadevan, R. How Important is Optimism for Mental Health? A Spatial Temporal Life Course Analysis on Indonesia. Applied Research Quality Life 19, 135–154 (2024). https://doi.org/10.1007/s11482-023-10234-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11482-023-10234-4