
Abstract
This study aimed to assess the temporal trends in opioid-involved overdose deaths in New York City (NYC) from 1999 to 2020 overall, and by age, sex, race/ethnicity, county, opioid type, and intent. Using data from the Centers for Disease Control and Prevention’s WONDER database, opioid overdose fatalities were identified by referencing the multiple cause of death files, utilizing codes from the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision. Joinpoint regression assessed temporal trends, with annual percentage changes and average annual percentage changes calculated using the permutation method. 95% confidence intervals were estimated using both the empirical quantile method and the parametric method. From 1999 to 2020, New York City recorded a total of 14,371 opioid-involved overdose deaths. In recent years, overall deaths have increased by 14.5% per year (95% CI, 10.7–20.8) from 2011 to 2020. Contemporary trends have worsened across the subcategories of age, sex, race/ethnicity, and opioid type. The findings of this study offer specific metrics for areas within NYC, facilitating targeted interventions and establishing baselines to underpin the sustainability of these efforts.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Opioid-involved overdose deaths represent a pressing public health concern in New York City. In 2020 alone, the city witnessed a total of 2062 drug overdose deaths, marking a 38% increase in fatalities since 2019 and a 42% increase since 2018 (NYC Health 2020). Fentanyl, a synthetic opioid known for its extreme potency—50 to 100 times more deadly than morphine—remains the most common opioid involved in overdose fatalities for the fifth consecutive year (NYC Health 2023).
Between 2000 and 2012, fentanyl was implicated in only 2% of drug overdose deaths in New York City (Colon-Berezin, 2019). However, by 2017, at least 57% of all drug overdose deaths in the city were attributed to fentanyl (Colon-Berezin, 2019). By 2021, this proportion has risen to 80% (NYC Health 2023). The emergence of fentanyl in New York City’s illicit drug scene highlights a significant escalation in the ongoing battle against opioid misuse. Initially utilized as a potent adulterant in heroin, fentanyl’s prevalence surged notably around the mid-2010s (Colon-Berezin, 2019). Alarming reports began to surface, documenting the direct sale of fentanyl in various forms, including counterfeit pills and clandestine mixtures with other substances, unknown to users (Klobucista and Ferragamo, 2023). This illicit infiltration led to a surge in overdose fatalities, as fentanyl’s heightened potency and unpredictability surpassed that of heroin, inflicting a devastating toll on individuals throughout the city (Colon-Berezin, 2019).
Analyses of opioid mortality trends in New York City over the years have revealed distinct patterns. Between 1990 and 2006, there was a substantial seven-fold surge in analgesic-associated deaths, with rates escalating from 0.39 to 2.7 per 100,000 individuals (Cerdá et al., 2013). In a more recent examination from 2000 to 2015, predating the introduction of fentanyl into the illicit drug market, overdose deaths involving heroin exhibited increases across multiple demographic subgroups, including men, Black and White individuals, and those aged 15 to 54 years (Tuazon et al., 2019). Additionally, the broader spectrum of opioid overdose mortality, including both heroin and non-heroin-related incidents, displayed an upward trajectory from 2000 to 2015 across all demographic subgroups (Tuazon et al., 2019).
Despite the elevated rates of opioid overdose deaths in New York City, surpassing national estimates (Dinapoli, 2022), empirical studies on the contemporary trends of opioid-involved overdose deaths in the city remain scarce. Previous investigations heavily relied on Epi Data reports (NYC Health, 2017; NYC Health 2019; NYC Health 2020). These reports are based on annual data, omitting the essential multi-year data required for valid temporal assessments. Some studies were outdated, such as those based on data spanning 1990 to 1998 or 1990 to 1996 (Cerdá et al., 2013; Galea et al., 2003), while one study that used more recent data was limited to 2000 to 2015, a period preceding the introduction of fentanyl into the illicit opioid market (Tuazon et al., 2019). Allen et al. (2019) conducted a study on opioid overdose deaths; however, their analysis solely relied on 2017 data and was limited to assessing racial and ethnic differences rather than examining temporal trends. Given the public health significance of opioid overdose deaths, along with changes in the opioid landscape from the introduction of synthetic opioids like fentanyl and the official declaration of the opioid epidemic, it is imperative to update the literature on overdose death trends in New York City. This will provide essential insights for evidence-based public health interventions. The aim of this study is to assess the temporal trends in opioid overdose deaths in New York City by age, sex, race/ethnicity, opioid type, intent, and county, from 1999 to 2020. We hypothesize a worsening in opioid overdose death trends in recent years, especially post-2015, following the introduction of synthetic opioids like fentanyl. Additionally, we anticipate observing variations in trends across regional and demographic groups.
Methods
Data Sources
Death records were obtained from the Centers for Disease Control and Prevention’s Wide-ranging Online Data for Epidemiologic Research (CDC WONDER) for the years 1999 through 2020 (Centers for Disease Control and Prevention, 2023a). We identified decedents of opioid-involved overdoses in New York City using the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10), for the underlying cause of death: X40-X44; X60-X64; X85; and Y10-Y14, and T40.0-T40.4 and T40.6 as the multiple causes of death. A compilation of the ICD-10 codes, including their descriptions, can be found in eTable 1 within the online supplement. Crude and age-adjusted mortality rates were extracted, stratified by age (< 25, 25 to 44, 45 to 64), sex (male, female), race/ethnicity (non-Hispanic White, non-Hispanic Black, Hispanic, Asian/Pacific Islander, American Indian/Alaska Native), type of opioid (methadone, heroin, non-heroin), county (Bronx, Kings, New York, Queens, Richmond), and intent (unintentional, suicide).
As the CDC WONDER data are de-identified and publicly available, the current study was exempt from Institutional Review Board review.
Statistical Analysis
We assessed the temporal trends in opioid-involved overdose deaths using a Joinpoint regression model. This technique accounts for interannual variation in rates and estimates both the annual percentage change (APC) and the average annual percentage change (AAPC) in Age-Adjusted Mortality Rates (AAMR) over the study period (Kim et al., 2000). The APC measures the trend over short-term, piecewise periods, while the AAPC estimates the average trend across the entire study period (Kim et al., 2000).
The Joinpoint regression model begins by assuming that AAMR follows a linear trend across the entire study period. Subsequently, a Joinpoint is introduced, signifying an inflection point or a change in the trend. A permutation test is then conducted to assess the statistical significance of this model relative to the null model. If the model with a Joinpoint is deemed significant, the Joinpoint is retained; otherwise, it is excluded. Additional Joinpoints are incorporated, and the process is repeated, with adjustments for multiple testing using Bonferroni correction, until a final model is derived with an optimal number of Joinpoints (National Cancer Institute, 2023a, 2023b).
To estimate the 95% confidence intervals for the final selected model, we utilized the Empirical Quantile Method. For the other models, their 95% confidence intervals were derived using the parametric method.
Model Specification/Parameter Settings
The outcome variable, the log-transformed AAMR, was modeled against the independent variable, the year of death. The variance of the standard errors was determined to be constant; thus, the homoscedastic option was selected, and an uncorrelated error model was fitted. For the interval type, the default option of “annual” was chosen to permit yearly trend estimations. The method employed for analysis was “grid search,” with a range of joinpoints set from 0 to 4. Model selection was based on the permutation test, with an overall significance level set at P < 0.05. A total of 4499 default permutations were conducted.
Supplemental Analysis
To determine if the opioid-involved overdose trends observed in New York City are reflective of regional patterns, we analyzed the data across each of the US census regions- the Northeast, Midwest, South, and West. Additionally, we assessed trends within individual states located in the Northeastern region, including New York, Connecticut, New Jersey, Pennsylvania, Massachusetts, Rhode Island, Vermont, New Hampshire, and Maine.
To account for the potential impact of the COVID-19 pandemic on opioid-involved overdose fatalities, we excluded data from the year 2020 and replicated the analysis.
All statistical analyses were performed using Joinpoint Regression Program, version 5.0.2 (Calverton, MD) and Stata 17.0 (College Station, Texas).
Results
Between 1999 and 2020, a total of 14,371 individuals died from opioid-involved overdose in New York City, resulting in an AAMR of 7.7 per 100,000 (95% CI, 7.6, 7.9). The highest mortality burden was observed among men (AAMR = 12.; 95% CI, 11.9–12.4), non-Hispanic White individuals (AAMR = 9.8; 95% CI, 9.5–10.0), residents of Richmond County (AAMR = 12.7; 95% CI, 12.0–13.4), individuals aged 45 to 64 years (AAMR = 15.5; 95% CI, 15.2–15.9), and deaths attributed to Heroin (AAMR = 2.5; 95% CI, 2.4–2.6) and unintentional causes (AAMR = 7.3; 95% CI, 7.2–7.4). (Table 1).
Temporal Trends
Overall, opioid-involved overdose death trends remained stable from 1999 to 2011 but increased at an annual rate of 14.5% per year (95% CI, 10.7–20.8) from 2011 to 2020.
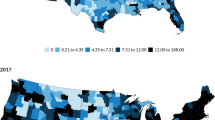
When examining rates by race/ethnicity, the most recent trend showed an increase of 9.5% per year (95% CI, 6.1–20.8) from 2011 to 2020 among non-Hispanic White individuals, 28.8% per year (95% CI, 16.0–71.3) from 2013 to 2020 among non-Hispanic Black individuals, and 20.2% per year (95% CI, 14.4–30.1) from 2012 to 2020 among Hispanic individuals. Trends for Asian/Pacific Islander individuals and American Indians/Alaska Natives were not estimated due to low and unreliable counts (Fig. 1).

Temporal trends in opioid-involved deaths by race/ethnicity, USA
Analysis by sex revealed that contemporary mortality trends increased in both sexes, with higher rates among men (15.8% per year from 2011 to 2020) than women (13.4% per year from 2013 to 2020).
When stratified by county, an increase in recent mortality trends was observed across all five counties in New York City. The Bronx County had the highest rate, increasing at an annual rate of 24.9% (95% CI, 18.6–34.9) from 2013 to 2020, followed by New York County with an annual increase of 17.7% (95% CI, 0.6–32.2) from 2010 to 2020. Queens County experienced an increase of 15.4% annually (95% CI, 8.5–40.5) from 2012 to 2020, Kings County recorded an annual increase of 12.7% (95% CI, 8.8–19.5) from 2012 to 2020, while Richmond County saw an increase of 8.2% per year (95% CI, 7.0–9.5) from 1999 to 2020.
Recent mortality trends increased across all age groups during the study period, with the highest rate observed among individuals aged 45 to 64 years, where the trend increased at an annual rate of 19.8% (95% CI, 12.4–41.6) from 2014 to 2020. The 25 to 44-year age group saw an increase of 14.5% per year (95% CI, 10.0–22.6) from 2011 to 2020, and individuals aged less than 25 years experienced an increase of 5.7% per year (95% CI, 3.5–8.1) from 1999 to 2020.
When categorized by opioid type, the most recent trend indicated the highest increase from non-heroin causes, at 28.8% per year (95% CI, 20.9–40.9) from 2014 to 2020. Heroin-related deaths increased at an annual rate of 22% (95% CI, 19.6–24.5) from 1999 to 2020, while methadone-related deaths initially increased from 1999 to 2006 (APC = 7.9; 95% CI, 1.9–31.3) but declined by 5% per year (95% CI, − 23.4 to − 1.0) from 2006 to 2015, and subsequently increased at an annual rate of 14.2% (95% CI, 2.5–48.7) from 2015 to 2020.
When stratified by intent, unintentional opioid overdose deaths increased at an annual rate of 15.7% (95% CI, 11.2–24.2) from 201 1 to 2020, while opioid suicide rates initially increased from 1999 to 2010 (APC = 5.8; 95% CI, 2.3–25.3) but remained stable from 2010 to 2020 (APC = − 3.8; 95% CI, − 18.5 to 0.0) (Table 2).
Regional and State-Level Trends
Our analysis revealed an increase in contemporary opioid-involved overdose trends across all four US census regions. Specifically, within the Northeastern region, these trends exhibited an increasing pattern from 1999 to 2020, with the most recent increase occurring at an annual rate of 10.1% (95% CI, 1.3–15.5) from 2016 to 2020. In the Midwestern region, we observed a sustained annual increase of 12.4% (95% CI, 11.6–13.1) from 1999 to 2020. The Southeastern region also experienced a significant rise, with contemporary trends surging at a rate of 13.5% per year (95% CI, 9.9–24.8) from 2013 to 2020. Meanwhile, the Western region saw the most recent trend increase at an annual rate of 37.7% (95% CI, 0.9–88.0) from 2018 to 2020. (Table 3).
Upon further disaggregation of trends within the Northeastern region, we discovered that contemporary rates increased across all nine states in the region, except for Massachusetts (APC = 0.9; 95% CI, − 11.9 to 15.7) and New Hampshire (APC = − 9.4; 95% CI, − 28.2 to 14.4), where the trends stabilized from 2016 to 2020 (Table 3).
COVID-19 Sensitivity Analysis
Upon excluding the data from the year 2020, the results remained robust, consistently indicating an increase in contemporary trends across the subcategories of age, sex, race/ethnicity, county, opioid type, and intent. However, when compared to 2019, the rate of trend increase in 2020 was higher across all the specified subcategories.
For instance, the overall opioid-involved overdose death trend showed an annual increase of 14.5% from 2011 to 2020, whereas the increase from 2011 to 2019 was slightly lower at 13.4% (95% CI, 9.8–18.7). The most substantial rate of increase in recent trends was observed among non-Hispanic Blacks, with a significant annual increase of 28.8% from 2013 to 2020. Similar findings were obtained for the period 1999–2019, with the highest rate of increase also occurring among non-Hispanic Blacks, but at an annual rate of 27.1% (95% CI, 13.4–67.5) from 2013 to 2019 (eTable 2).
Discussion
This study presents insights into opioid-related mortality trends in New York City, utilizing national death certificate records for the past two decades. The analysis reveals a deterioration in contemporary trends of opioid-involved overdose fatalities across diverse demographic and geographic subgroups, including age, sex, race/ethnicity, county, and opioid type. The hypothesis driving this investigation is rooted in understanding the evolving landscape of opioid-related fatalities, particularly in light of shifting demographic profiles and emerging synthetic opioids like fentanyl.
Non-Hispanic White individuals exhibit the highest mortality burden, but temporal trends have increased the largest among non-Hispanic Black individuals, followed by Hispanics, and then non-Hispanic White persons. The elevated mortality burden among the non-Hispanic White population could be attributed to their higher cumulative (historical) rate of opioid-related mortality, particularly originating from prescription opioids during the initial wave of the opioid epidemic (Alexander et al., 2018; Pletcher et al., 2008; Singhal et al., 2016). Regarding contemporary trends, non-Hispanic Black and Hispanic communities in the USA have faced systemic inequities, including limited access to quality healthcare, educational opportunities, and economic stability, which can lead to an increased risk of opioid addiction as a means of coping with environmental stressors (Cano, 2021; Khan et al., 2023). Additionally, illicitly manufactured opioids, including the potent synthetic opioid, fentanyl, may be more widely available in these communities, which has contributed to the worsening trend among Non-Hispanic Black persons (Cano, 2021). In the earlier stages of the opioid crisis, opioid overdose deaths were predominantly reported among Non-Hispanic White persons, largely driven by the misuse of prescription opioids (Alexander et al., 2018; Pletcher et al., 2008; Singhal et al., 2016). However, the trend has now shifted, with other racial/ethnic subgroups being more likely to record a higher mortality, especially from synthetic opioids (Alexander et al., 2018).
The Bronx stands out with the highest trend in opioid-involved deaths among New York City’s counties. Historically, the Bronx has grappled with elevated levels of poverty, unemployment, and housing instability, conditions closely linked to opioid misuse (Kaplan et al., 2006). Limited access to quality healthcare and addiction treatment services in the county further complicates the situation, discouraging timely intervention for opioid addiction (Kaplan et al., 2006; Nolan et al., 2019). Additionally, the Bronx may experience higher availability of opioids, both prescription and illicit, potentially due to factors such as drug trafficking routes or a greater prevalence of prescription opioids (Nolan et al., 2019). The demographic composition of the Bronx, with a significant minority population, can influence substance use patterns and disparities in opioid-related outcomes (Kaplan et al., 2006; Nolan et al., 2019).
The most recent trend exhibited the highest rate of worsening among individuals aged 45 to 64 years, with an annual increase of 19.8% documented from 2014 to 2020. This finding aligns with previously documented reports. For example, in both 2019 and 2020, the highest mortality rates were reported among individuals aged 55 to 64 years (NYC Health 2019; NYC Health 2020). Several potential explanations may account for this observation. First, many individuals in this age group could have been exposed to prescription opioids in the late 1990s and early 2000s for pain management, which could have increased their risk of opioid use disorder and death. Further, relative to the younger generation, individuals in this age group are more likely to experience chronic pain conditions, including arthritis and back pain (Chang, 2018; Cochran et al., 2017; Oh et al., 2019). These conditions result in prolonged opioid use and increased risk of addiction and death. It is also possible that these individuals compared to the younger generation, may be less likely to seek help for opioid addiction due to the stigma associated with substance abuse (Kuerbis et al., 2014; Sahker et al., 2015; Zullo et al., 2020). Undiagnosed or untreated mental health conditions in this age group can also contribute to self-medication with opioids (Lin et al., 2011; Post et al., 2006). Further studies are needed to identify the determinants of opioid-involved overdose mortality among individuals aged 45 to 64 years to facilitate the planning and provision of targeted public health interventions.
The higher prevalence of opioid-involved deaths among men compared to women is also consistent with the literature and can be attributed to a complex interplay of biological, social, and behavioral factors. Men and women may exhibit differences in pain perception and tolerance, with men often less inclined to seek medical help for pain, potentially leading to self-medication with opioids (Hoopsick et al., 2021; Lynch et al., 2002). Historically, healthcare providers have also been more likely to prescribe opioids to men, increasing their exposure to these drugs and contributing to higher rates of addiction and overdose (Coleman et al., 2022). Socially, men may engage in riskier behaviors, including illicit substance use, and societal norms may foster a greater acceptance of substance use among men (Bagley et al., 2020; Hoopsick et al., 2021).
The analysis of opioid-involved deaths, categorized by opioid subtype, reveals the highest rate from non-heroin opioids, followed by heroin, and methadone. This trend signifies a shift in the opioid crisis, predominantly influenced by the surge in potent synthetic opioids such as fentanyl (Centers for Disease Control and Prevention 2023b; Manchikanti et al., 2018). Fentanyl’s potency, significantly surpassing that of traditional opioids, presents a challenge in combating the crisis. Its heightened strength not only escalates the risk of unintentional overdoses but also magnifies the potential for addiction due to its powerful effect on µ-opioid receptors, particularly µ2 receptors (Bird et al., 2023). Furthermore, fentanyl’s pervasive presence extends beyond its legitimate medical use, with instances of clandestine mixing with other illicit opioids and drugs becoming increasingly common (Jannetto et al., 2019; Manchikanti et al., 2018; Volkow, 2021). This adulteration practice poses dangers for users, as even minuscule, undetected amounts of fentanyl in a drug mixture can lead to fatal overdoses (Jannetto et al., 2019; Volkow, 2021). Overall, the potency of synthetic opioids like fentanyl contributes to the worsening trends in opioid-involved mortality by increasing the risk of overdose and addiction (Jannetto et al., 2019; Volkow, 2021). Addressing this aspect of the crisis requires comprehensive strategies aimed at curtailing the proliferation of synthetic opioids, improving surveillance efforts and detection mechanisms, new and specific strategies to fentanyl reversal, and expanding access to evidence-based treatment and harm reduction services (Thevathasan et al., 2020).
The observed trends in opioid-involved mortality, marked by rising rates of unintentional deaths and stabilizing rates from suicide or intentional causes, can be explained by several factors, including the rise of counterfeit prescription medicines, which contain fentanyl (Daniulaityte et al., 2022; Jewell et al., 2023). Further, the availability of mental health services and suicide prevention programs may be instrumental in stabilizing opioid-involved suicide rates, ensuring that individuals facing mental health issues receive the necessary support and treatment to prevent self-harm (Olfson et al., 2019). Finally, variations in access to lethal means, such as firearms, may differentiate the patterns of unintentional and intentional opioid-involved deaths, contributing to the observed trends (Karaye, 2022; Olfson et al., 2019).
Our supplementary analysis of regional and state-level trends in opioid-involved overdose deaths underscores the pervasive nature of worsening rates (Rudd et al., 2016). Recognizing that New York City is not isolated from the broader context, it becomes imperative to emphasize that while city and state-level initiatives are vital, they must be complemented by comprehensive national interventions to effectively address this epidemic.
In our sensitivity analysis, we found that our results were robust to the exclusion of data from the year 2020. However, the trends exhibited a pronounced increase in 2020 when compared to the preceding years, which is most likely related to the COVID-19 pandemic, including disruptions in healthcare access, heightened social isolation, increased stress and anxiety, economic and housing instability, and changes in drug supply and use patterns (Stephenson 2021; Friedman & Akre, 2021; Allen et al., 2021; Garcia et al., 2022).
Our findings have significant implications for policy and practice in addressing the opioid crisis. Firstly, understanding the demographic and geographic disparities in opioid-related mortality can inform targeted interventions tailored to specific communities. Efforts to mitigate systemic inequities in access to healthcare, education, and economic stability, particularly in underserved minority populations, are pivotal for preventing opioid addiction and reducing overdose fatalities. Additionally, the identification of synthetic opioids, especially fentanyl, as a major contributor to worsening trends highlights the urgency of strategies aimed at interrupting the proliferation of these potent substances. Policymakers and healthcare providers must collaborate to implement policies and practices that address the multifaceted nature of opioid misuse and overdose, with a focus on promoting equity, expanding access to treatment and support services, and enhancing surveillance and detection efforts to prevent further escalation of opioid-related fatalities in New York City.
Limitations
This study has several limitations. The primary endpoint, which is opioid-involved overdose death, represents a terminal outcome. Further studies should complement this analysis by assessing trends in the incidence of opioid use disorder and sociodemographic patterns of opioid use disorder and opioid-related hospitalizations. Second, due to its ecological design, the findings presented in this study cannot be directly applied to individuals, avoiding the ecologic fallacy (Piantadosi et al., 1988). Finally, the data utilized in this study relied on death certificate records, which may occasionally result in misclassifications of race and ethnicity, particularly among Hispanic individuals (Arias et al., 2010).
Conclusions
Opioid-involved overdose trends have worsened across all demographic and geographic subgroups in New York City, mirroring the nationwide epidemic. Particularly concerning are the worsening trends among individuals aged 45 to 64 years, men, non-Hispanic Black residents, Bronx inhabitants, and accidental overdose deaths. This underscores the imperative for tailored interventions targeting different age groups, the implementation of gender-sensitive strategies, and a comprehensive approach aimed at addressing healthcare disparities and structural inequities, particularly within racial and ethnic minority populations.
References
Alexander, M. J., Kiang, M. V., & Barbieri, M. (2018). Trends in black and white opioid mortality in the United States, 1979–2015. Epidemiology, 29(5), 707–715.
Allen, B., El Shahawy, O., Rogers, E. S., Hochman, S., Khan, M. R., & Krawczyk, N. (2021). Association of substance use disorders and drug overdose with adverse COVID-19 outcomes in New York City: January–October 2020. Journal of Public Health, 43(3), 462–465.
Allen, B., Nolan, M. L., Kunins, H. V., & Paone, D. (2019). Racial differences in opioid overdose deaths in New York City, 2017. JAMA Internal Medicine, 179(4), 576–578.
Arias, E., Eschbach, K., Schauman, W. S., Backlund, E. L., & Sorlie, P. D. (2010). The Hispanic mortality advantage and ethnic misclassification on US death certificates. American Journal of Public Health, 100(S1), S171–S177.
Bagley, S. M., Gai, M. J., Earlywine, J. J., Schoenberger, S. F., Hadland, S. E., & Barocas, J. A. (2020). Incidence and characteristics of nonfatal opioid overdose among youths aged 11 to 24 years by sex. JAMA Network Open, 3(12), e2030201–e2030201.
Bird, H. E., Huhn, A. S., & Dunn, K. E. (2023). Fentanyl absorption, distribution, metabolism, and excretion: Narrative review and clinical significance related to illicitly manufactured fentanyl. Journal of Addiction Medicine, 17(5), 503–508.
Cano, M. (2021). Racial/ethnic differences in US drug overdose mortality, 2017–2018. Addictive Behaviors, 112, 106625.
Centers for Disease Control and Prevention. (2023a). About Multiple Cause of Death, 1999–2020. 2023. Retrieved from https://wonder.cdc.gov/mcd-icd10.html
Centers for Disease Control and Prevention. (2023b). Understanding the opioid overdose epidemic. 2023. Retrieved from https://www.cdc.gov/opioids/basics/epidemic.html
Cerdá, M., Ransome, Y., Keyes, K. M., Koenen, K. C., Tracy, M., Tardiff, K. J., Vlahov, D., & Galea, S. (2013). Prescription opioid mortality trends in New York City, 1990–2006: examining the emergence of an epidemic. Drug and alcohol dependence, 132(1–2), 53–62.
Chang, Y. P. (2018). Factors associated with prescription opioid misuse in adults aged 50 or older. Nursing Outlook, 66(2), 112–120.
Cochran, G., Rosen, D., McCarthy, R. M., & Engel, R. J. (2017). Risk factors for symptoms of prescription opioid misuse: Do older adults differ from younger adult patients? Journal of Gerontological Social Work, 60(6–7), 443–457.
Coleman, C., Lennon, R. P., Robinson, J. M., Wen-Jan Tuan, D. H. A., Sehgal, N., & Zgierska, A. E. (2022). Provider and patient sex disparities in opioid prescribing and patient outcomes. Journal of Opioid Management, 18(5), 435–445.
Colon-Berezin, C. (2019). Overdose deaths involving fentanyl and fentanyl analogs—New York City, 2000–2017. MMWR Morbidity and Mortality Weekly Report 68
Daniulaityte, R., Sweeney, K., Ki, S., Doebbeling, B. N., & Mendoza, N. (2022). “They say it’s fentanyl, but they honestly look like Perc 30s”: Initiation and use of counterfeit fentanyl pills. Harm Reduction Journal, 19(1), 52.
DiNapoli, TP. (2022). Continuing crisis: Drug overdose deaths in New York. Retrieved from https://www.osc.state.ny.us/reports/continuing-crisis-drug-overdose-deaths-new-york
Friedman, J., & Akre, S. (2021). COVID-19 and the drug overdose crisis: Uncovering the deadliest months in the United States, January-July 2020. American Journal of Public Health, 111(7), 1284–1291.
Galea, S., Ahern, J., Tardiff, K., Leon, A., Coffin, P. O., Derr, K., & Vlahov, D. (2003). Racial/ethnic disparities in overdose mortality trends in New York City, 1990–1998. Journal of Urban Health, 80, 201–211.
Garcia, G. G. P., Stringfellow, E. J., DiGennaro, C., Poellinger, N., Wood, J., Wakeman, S., & Jalali, M. S. (2022). Opioid overdose decedent characteristics during COVID-19. Annals of Medicine, 54(1), 1081–1088.
Hoopsick, R. A., Homish, G. G., & Leonard, K. E. (2021). Differences in opioid overdose mortality rates among middle-aged adults by race/ethnicity and sex, 1999–2018. Public Health Reports, 136(2), 192–200.
Jannetto, P. J., Helander, A., Garg, U., Janis, G. C., Goldberger, B., & Ketha, H. (2019). The fentanyl epidemic and evolution of fentanyl analogs in the United States and the European Union. Clinical Chemistry, 65(2), 242–253.
Jewell, M. L., Jewell, H. L., Singer, R., Fontbona, M., Triana, L., & Walden, J. L. (2023). Patient safety advisory: fentanyl counterfeit prescription medications that contain fentanyl and patient safety
Kaplan, S. A., Calman, N. S., Golub, M., Davis, J. H., Ruddock, C., & Billings, J. (2006). Racial and ethnic disparities in health: A view from the South Bronx. Journal of Health Care for the Poor and Underserved, 17(1), 116–127.
Karaye, I. M. (2022). Differential trends in US suicide rates, 1999–2020: Emerging racial and ethnic disparities. Preventive Medicine, 159, 107064.
Khan, M. R., Hoff, L., Elliott, L., Scheidell, J. D., Pamplin, J. R., Townsend, T. N., & Bennett, A. S. (2023). Racial/ethnic disparities in opioid overdose prevention: Comparison of the naloxone care cascade in White, Latinx, and Black people who use opioids in New York City. Harm Reduction Journal, 20(1), 24.
Kim, H. J., Fay, M. P., Feuer, E. J., & Midthune, D. N. (2000). Permutation tests for joinpoint regression with applications to cancer rates. Statistics in Medicine, 19(3), 335–351.
Klobucista, C & Ferragamo, M. (2023). Fentanyl and the U.S. opioid epidemic. Retrieved from https://www.cfr.org/backgrounder/fentanyl-and-us-opioid-epidemic
Kuerbis, A., Sacco, P., Blazer, D. G., & Moore, A. A. (2014). Substance abuse among older adults. Clinics in Geriatric Medicine, 30(3), 629–654.
Lin, W. C., Zhang, J., Leung, G. Y., & Clark, R. E. (2011). Chronic physical conditions in older adults with mental illness and/or substance use disorders. Journal of the American Geriatrics Society, 59(10), 1913–1921.
Lynch, W. J., Roth, M. E., & Carroll, M. E. (2002). Biological basis of sex differences in drug abuse: Preclinical and clinical studies. Psychopharmacology (berl), 164, 121–137.
Manchikanti, L., Sanapati, J., Benyamin, R. M., Atluri, S., Kaye, A. D., & Hirsch, J. A. (2018). Reframing the prevention strategies of the opioid crisis: Focusing on prescription opioids, fentanyl, and heroin epidemic. Pain Physician, 21(4), 309.
National Cancer Institute. (2023a). How joinpoint conducts permutation testing. Retrieved March 24, 2024, from https://surveillance.cancer.gov/help/joinpoint/setting-parameters/method-and-parameters-tab/model-selection-method/permutation-tests/model-selection-method-how-joinpoint-conducts-permutation-testing
National Cancer Institute. (2023b). Permutation test. Retrieved March 24, 2020, from https://surveillance.cancer.gov/help/joinpoint/setting-parameters/method-and-parameters-tab/model-selection-method/permutation-tests
Nolan, M. L., Mantha, S., Tuazon, E., & Paone, D. (2019). Unintentional drug poisoning (Overdose) deaths in New York City in 2018. New York City Department of Health and Mental Hygiene: Epi Data Brief 116
NYC Health. (2017). Epi data brief. Retrieved March 24 2024, from https://www.nyc.gov/assets/doh/downloads/pdf/epi/databrief120.pdf
NYC Health. (2019). Epi data brief. Retrieved March 24, 2024, from https://www.nyc.gov/assets/doh/downloads/pdf/epi/databrief122.pdf
NYC Health. (2020). Epi data brief. Retrieved March 24, 2024, from https://www.nyc.gov/assets/doh/downloads/pdf/epi/databrief129.pdf
NYC Health. (2023). New York city releases 2021 overdose data showing unprecedented overdose levels. Retrieved March 24, 2024, from https://www.nyc.gov/site/doh/about/press
Oh, G., Abner, E. L., Fardo, D. W., Freeman, P. R., & Moga, D. C. (2019). Patterns and predictors of chronic opioid use in older adults: A retrospective cohort study. PLoS ONE, 14(1), e0210341.
Olfson, M., Rossen, L. M., Wall, M. M., Houry, D., & Blanco, C. (2019). Trends in intentional and unintentional opioid overdose deaths in the United States, 2000–2017. JAMA, 322(23), 2340–2342.
Piantadosi, S., Byar, D. P., & Green, S. B. (1988). The ecological fallacy. American Journal of Epidemiology, 127(5), 893–904.
Pletcher, M. J., Kertesz, S. G., Kohn, M. A., & Gonzales, R. (2008). Trends in opioid prescribing by race/ethnicity for patients seeking care in US emergency departments. JAMA, 299(1), 70–78.
Post, L. A., Swierenga, S. J., Oehmke, J., Salmon, C., Prokhorov, A., Meyer, E., & Joshi, V. (2006). The implications of an aging population structure. International Journal of Interdisciplinary Social Sciences, 1(2), 47–58.
Rudd, R. A., Aleshire, N., Zibbell, J. E., & Gladden, R. M. (2016). Increases in drug and opioid overdose deaths—United States, 2000–2014. American Journal of Transplantation, 16(4), 1323–1327.
Sahker, E., Schultz, S. K., & Arndt, S. (2015). Treatment of substance use disorders in older adults: Implications for care delivery. Journal of the American Geriatrics Society, 63(11), 2317–2323.
Singhal, A., Tien, Y. Y., & Hsia, R. Y. (2016). Racial-ethnic disparities in opioid prescriptions at emergency department visits for conditions commonly associated with prescription drug abuse. PLoS ONE, 11(8), e0159224.
Stephenson, J. 2021 CDC warns of surge in drug overdose deaths during COVID-19. In JAMA Health Forum (Vol. 2, No. 1, pp. e210001-e210001). American Medical Association
Thevathasan, T., Grabitz, S. D., Santer, P., Rostin, P., Akeju, O., Boghosian, J. D., & Eikermann, M. (2020). Calabadion 1 selectively reverses respiratory and central nervous system effects of fentanyl in a rat model. British Journal of Anaesthesia, 125(1), e140–e147.
Tuazon, E., Kunins, H. V., Allen, B., & Paone, D. (2019). Examining opioid-involved overdose mortality trends prior to fentanyl: New York City, 2000–2015. Drug and Alcohol Dependence, 205, 107614.
Volkow, N. D. (2021). The epidemic of fentanyl misuse and overdoses: Challenges and strategies. World Psychiatry, 20(2), 195.
Zullo, A. R., Danko, K. J., Moyo, P., Adam, G. P., Riester, M., Kimmel, H. J., ... & Balk, E. M. (2020). Prevention, diagnosis, and management of opioids, opioid misuse, and opioid use disorder in older adults.
Acknowledgements
We thank Dr. Luther Elliott for his feedback on this manuscript.
Author information
Authors and Affiliations
Contributions
Dr. IK, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: IMK, ME, CL, GE, and AE; acquisition, analysis, and interpretation of data: IK, CL, AE, and GE; drafting of the manuscript: IK, CL, AE, and GE; critical revision of the manuscript for important intellectual content: ME, NA, OA, MR, AB, and VB; statistical analysis: IK; study supervision: ME.
Corresponding author
Ethics declarations
Conflicts of Interest
Matthias Eikermann has received unrestricted funds from philanthropic donors Jeffrey and Judy Buzen, as well as grants from Merck & Co. not related to this study. He also holds a patent describing the value of acyclic CB[n]-type compounds for reversing the effects of drugs of abuse (Patent number: 9956229).
All other investigators declare no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Karaye, I.M., Ludeke, C.M., Eikermann, G.M. et al. Recent Trends in Opioid-Involved Overdose Deaths in New York City, 1999 to 2020. Int J Ment Health Addiction (2024). https://doi.org/10.1007/s11469-024-01306-z
Accepted:
Published:
DOI: https://doi.org/10.1007/s11469-024-01306-z