
Abstract
In 2014, China experienced the worst outbreak of dengue fever in the last decade with over 40,000 dengue cases including six deaths by the end of October. As one of the “neglected” tropical diseases, dengue is affecting substantially increasing number of people and proportion of global population due to factors including globalization, human settlement, and possibly climate change. Here, the authors summarized the most recent data about dengue outbreaks in China and reviewed the global trend of dengue epidemiology. Future directions for dengue surveillance, control and prevention are also introduced.
概要
中国在2014年经历了近十年来最严重的登革热疫情,截至10月底,登革热病例超过4万例,其中6例死亡。随着全球化、人类聚居和气候等因素的变化,登革热这一“被忽视”的热带疾病在全球范围所影响的人群日益扩大。近期的研究估计全球每年有3.9亿人被登革热病毒感染,其中约0.96亿出现不同程度的症状。尽管75%的登革热感染者不会出现临床症状,但严重的登革热疾病可能致命。登革热在我国是法定传染病之一,自2005年开始的登革热监测显示该疾病在我国的传播趋势发生着变化,特别是暴发疫情出现的时间间隔逐渐缩短。迄今尚无预防登革热感染的疫苗,也缺乏治疗该疾病的特效药物。但值得关注的是,近期国外的一项临床试验已证实一种4价登革热疫苗的有效性。除了疫苗药物的研发,依托准确的实验室诊断技术开展高灵敏度的登革热监测是防控登革热的又一关键。同时,研发新型高效的病媒防治技术也势在必行。
Similar content being viewed by others

Avoid common mistakes on your manuscript.
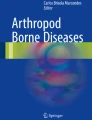
In 2014, China experienced the worst outbreak of dengue fever (DF) in the last decade (Fig. 1a, b). A total of 44,591 dengue cases were reported to the national notifiable infectious diseases reporting system by the end of October including six deaths, and 99 % of cases were reported in south China provinces, such as Guangdong, Fujian, Yunnan and Zhuang Autonomous Region [1]. On November 3, the U.S. Centers for Disease Control and Prevention (CDC) issued a travel notice for Guangdong province, China because of the dengue outbreak [2].

Number of reported dengue fever (DF) cases in China's mainland from 2004 to 2013 (a) and from January to October 2014 (b). Data source: Notifiable infectious disease reporting summary, China CDC [1]
1 The global threat of dengue
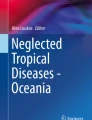
Dengue fever (DF), caused by any one of the four closely related dengue viruses (DENV 1–4), is a viral illness transmitted by Aedes mosquitoes. Originating in monkeys, dengue viruses were transmitted to humans between 100–800 years ago, and dengue remained a relatively minor and geographically restricted disease until the 1950s when epidemics occurred in the Philippines and Thailand [3, 4]. Dengue has emerged as a worldwide problem, with a 30-fold increase in incidence globally in the past 50 years (Fig. 2) [4]. Today, dengue is regarded as the most prevalent and rapidly spreading mosquito-borne viral disease of humans [4]. It is found in at least 100 tropical and sub-tropical countries, including countries in Africa, Southeast Asia, the western Pacific, the Americas, the Caribbean, and the eastern Mediterranean regions [3, 5]. More than one-third of the world’s population lives in areas at risk of infection with dengue virus [3], and a recent estimate using cartographic approaches in 2013 showed that 390 million people have dengue virus infections per year, of which 96 million cases manifest symptoms worldwide [6].

Average number of dengue and severe dengue (DHF) cases reported to WHO from 1955 to 2007 [4]
Dengue is a complex disease with a wide spectrum of clinical presentation. Classic DF is characterized by acute onset of high fever 3–14 days after the bite of an infected mosquito, and the high fever can persist for 2–7 days accompanied by frontal headache, retro-orbital pain, myalgias, arthralgias, rash, and low white blood cell count [7, 8]. Due to the severe muscle, joint and bone pains, dengue is also known as “break bone fever”. Most dengue patients recover after a few days, but some DF patients develop dengue hemorrhagic fever (DHF) or dengue shock syndrome (DSS), which are severe and sometimes fatal forms of the disease [7]. About three quarters of dengue infections can be asymptomatic, especially in children and those with previous dengue infection, but they can still infect mosquitoes [3, 7]. However, secondary dengue infection is one of the two factors thought to be associated with increased risk of disease severity; the other factor is infection by particularly virulent strains of dengue viruses [8].
At present, no vaccine exists to prevent dengue infection, nor are there specific medications to treat the disease. The most effective protective measures are those that prevent mosquito bites, namely vector control [3]. The main arthropod vector for dengue virus transmission is Aedes aegypti, and a second, less effective vector is Aedes albopictus [8]. Control of dengue vectors has mainly been addressed by community-based source reduction: The elimination of containers that are favorable sites for oviposition and development of the aquatic stages [4]. For individuals, preventive measures include sleeping under a mosquito bed net, eliminating mosquito indoors and wearing repellent [3].
The World Health Organization (WHO) described dengue as a “neglected” tropical disease (NTD) in its Dengue Prevention and Control Strategy 2012–2020, due to the lack of global coordination efforts, research, and political will [4]. The contemporary worldwide distribution of the risk of dengue virus infection and its public health burden is poorly known, and the greatest uncertainties in national burden estimates are in India, Indonesia, Brazil, and China [6]. The economic burden of dengue on both governments and individuals is high. Based on a systematic review analysis, the estimated cost of dengue disease in the Americas including North America, Central America and Mexico, the Andean region, Brazil, the Southern cone, and the Caribbean region is 2.1 billion USD per year on average, excluding cost on vector control [9]. Another 12-country economic analysis also showed high dengue burden in Southeast Asia, with an annual average of 950 million USD resulted from 2.9 million dengue episodes and 5,906 deaths [10]. Information on economic burden of dengue in China, however, is not available.
2 Dengue in China
NTDs including dengue are still widespread and create a substantial burden in China [11]. Infectious diseases in China are divided into three categories (A, B, and C) according to their transmission modes, speed, and hazard to humans; DF, together with Severe Acute Respiratory Syndrome (SARS), H1N1 influenza, rabies, tuberculosis etc., belong to infectious diseases category B. In 2005, China established a national monitoring program for DF in humans and vector monitoring in Aedes mosquitoes, focusing on five provinces (Guangdong, Fujian, Yunnan, Guangxi Autonomous Region, and Hainan) with 16 national monitoring sites. Other efforts that China has made to prevent and control dengue include control of mosquito vector density, enhanced surveillance for imported cases, improvement of diagnosis and treatment, enhancing the cooperation among the related different public health departments and neighboring countries, and engaging communities to combat the epidemic [11, 12]. In response to the dengue outbreak in 2014, four technical guidelines [13], including surveillance of DF cases, laboratory tests and diagnosis, surveillance of dengue vectors, and control of dengue vectors, were developed and issued by China CDC, together with the previous two dengue guidelines (Diagnosis and Treatment of Dengue Fever in 2014 and Dengue Outbreak Investigation and Management in 2006) issued by the National Commission for Health and Family Planning, formed a complete national technical framework for dengue control and prevention [13].
DF in China's mainland was characterized as an imported epidemic disease and was not confirmed as an endemic in the past [4], but after the 2014 large dengue outbreak, it is possible that DENV will be endemic in southern China, especially in Guangdong [14]. All four dengue viruses are detected in China [11]. Upon review of the surveillance data collected by the monitoring program started in 2005 with a focus on southern provinces as-described above for the past years, a changing circulation pattern of DF has been observed in Guangdong, from non-endemicity (no virus sustained), to hypo-endemicity (one serotype present), and even hyper-endemicity (multiple serotypes present) of dengue infections [15]. In the last two decades, the biological behavior and vectorial capacity of Aedes mosquitoes have changed significantly in China, possibly due to urbanization and global climate changes [12]. Therefore, dengue illnesses have spread from southern coastal regions to the relatively northern and western areas of the country, and the interval between epidemics has become shorter since the 1990s compared to those that occurred before the 1990s, beginning with the first reported outbreak of DF in Guangdong in 1978 [11, 12]. In 2013, a severe dengue outbreak of 1,245 cases happened in Yunnan Province, with a significant proportion of severe dengue cases; DENV-3 was identified to be the cause of the outbreak using real-time RT-PCR assays [16]. In the same year, the first dengue outbreak in central China was reported in Henan Province, a northern temperate province of China; 73 of 106 suspected DF cases of this outbreak were confirmed DENV-3 infections [17].
The recent data from Guangdong, the most affected province of the 2014 dengue outbreak, showed that as of December 15, 20 prefectures reported a total of 45,171 clinical or laboratory confirmed dengue cases according to the case definition in China’s dengue surveillance guideline 2005, with the highest number (37,354) reported in the capital city of Guangzhou, followed by Foshan City with 3,542 cases [18]. According to the Guangdong Provincial CDC, the peak of the dengue outbreak was reached on October 1, and case numbers started to decline after October 11 [19]. Guangdong is located in a subtropical zone in China, and it has a high relative humidity, which may have created climatic and environmental conditions conducive to the proliferation of Aedes species. The DF epidemic area in Guangdong was mainly located in the old town which is under construction, and the poor sanitary infrastructure may contribute to this DF epidemic. A previous study from Guangdong showed that urbanization substantially increased the density, larval development rate, and adult survival time of Aedes species, which in turn potentially increases the vector capacity, and therefore, disease transmissibility [20].
3 Future directions for dengue control
Experts predict geographic expansion and increased incidence of dengue in the future [8]. The expansion of dengue is multifactorial, and the main “drivers” of increase in dengue incidence include globalization, travel, trade, socioeconomic factors, human settlement, viral evolution, and possibly also climate change [8].
With the substantial increase in the number of people and the proportion of the global population at risk of DF, a safe and effective dengue vaccine is greatly needed. Very recently, a tetravalent dengue vaccine has been reported showing efficacy against DF and severe DF, leading to fewer hospitalizations in a randomized, blinded, placebo-controlled trial in Latin America [21]. The observed reduction in the severity of clinical disease and the prevention of hospitalization are encouraging, and the progress is considered a milestone in dengue prevention and control [22].
Accurate disease burden estimates and sensitive outbreak monitoring for dengue through improved epidemiological and entomological surveillance are another key for dengue control. Dengue is an acute febrile illness, and only diagnostic testing can accurately determine the etiology of the syndrome and differentiate dengue from acute febrile illness caused by other pathogens. However, the current dengue surveillance programs in China and internationally are all syndrome based (that is, entail clinical case-definitions without laboratory confirmation) and almost all are passive [23]. With the development of sensitive and specific diagnostic algorithms and increased awareness of dengue expansion, robust, laboratory-based dengue surveillance is needed to document and monitor the regional and global dengue incidence, and to evaluate the effectiveness of dengue control interventions. More accurate epidemiological and surveillance data will support greater political prioritization for this currently “neglected” disease. It would also allow improved decision making and rational allocation of financial, research, and other resources to the areas of greatest need [24].
Although the current control approach has shown some effectiveness, innovative vector control tools are still needed to control mosquito more effectively [25]. Recent systematic review and meta-analysis showed low relative effectiveness (25 %) with high heterogeneity of community-based interventions with educational message for dengue control [26]. Vector-borne diseases such as dengue have raised public health concern worldwide due to climate change, global trade, worldwide travel, and urban crowding. “One Health” is a relatively new term, but the concept that the health of humans is connected to the health of animals and the environment has long been recognized [27]. It has become more important in recent years because many factors have changed the interactions among humans, animals, and the environment, which have caused the emergence and reemergence of many diseases, including dengue. Successful public health interventions for disease control require the cooperation of the human health, veterinary health, and environmental health communities [27].
References
China Centers for Disease Control and Prevention (2014) Notifiable infectious disease report. http://www.chinacdc.cn/tjsj/fdcrbbg/. Accessed 15 Dec 2014
Centers for Diseases Control and Prevention (2014) Dengue in China-travelers’ health. http://wwwnc.cdc.gov/travel/notices/watch/dengue-china. Accessed 5 Nov 5 2014
Centers of Disease Control and Prevention (2014) Dengue. http://www.cdc.gov/dengue/. Accessed 4 Nov 2014
World Health Organization (2012) Global strategy for dengue prevention and control 2012–2020. World Health Organization, Geneva
Guzman MG, Harris E (2014) Dengue. Lancet 385:453–465
Bhatt S, Gething PW, Brady OJ et al (2013) The global distribution and burden of dengue. Nature 496:504–507
Centers for Disease Control and Prevention (2009) Dengue and dengue hemorrhagic fever. http://www.cdc.gov/Dengue/resources/Dengue&DHF%20Information%20for%20Health%20Care%20Practitioners_2009.pdf. Accessed 4 Nov 2014
Murray NE, Quam MB, Wilder-Smith A (2013) Epidemiology of dengue: past, present and future prospects. Clin Epidemiol 5:299–309
Shepard DS, Coudeville L, Halasa YA et al (2011) Economic impact of dengue illness in the Americas. Am J Trop Med Hyg 84:200–207
Shepard DS, Undurraga EA, Halasa YA (2013) Economic and disease burden of dengue in Southeast Asia. PLoS Negl Trop Dis 7:e2055
Yang GJ, Liu L, Zhu HR et al (2014) China’s sustained drive to eliminate neglected tropical diseases. Lancet Infect Dis 14:881–892
Wu JY, Lun ZR, James AA et al (2010) Dengue fever in mainland China. Am J Trop Med Hyg 83:664–671
National Institute for Communicable Disease Control and Prevention, China Centers for Disease Control and Prevention (2014) Infectious diseases report
Qin C, Shi P (2014) Dengue in China: not a passing problem. Sci China Life Sci 57:1230–1231
Guo RN, Lin JY, Li LH et al (2014) The prevalence and endemic nature of dengue infections in Guangdong, South China: an epidemiological, serological, and etiological study from 2005–2011. PLoS One 9:e85596
Zhang FC, Zhao H, Li LH et al (2014) Severe dengue outbreak in Yunnan, China, 2013. Int J Infect Dis 27:4–6
Huang XY, Ma HX, Wang HF et al (2014) Outbreak of dengue fever in central China, 2013. Biomed Environ Sci 27:894–897
Emergency Management Office, The Peoples’ Government of Guangdong Province (2014) Guangdong dengue outbreak report (December 9–December 15). http://www.gdwst.gov.cn/a/yiqingxx/2014121512665.html. Accessed 29 Dec 2014
Guangdong Centers for Disease Control and Prevention (2014) Guangdong dengue outbreak is under control. http://cdcp.org.cn/gdsjbyfkzzx/xwfb/201410/67ccaff220994ff8b9ce6b4e82dce449.shtml. Accessed 5 Nov 2014
Li Y, Kamara F, Zhou G et al (2014) Urbanization increases Aedes albopictus larval habitats and accelerates mosquito development and survivorship. PLoS Negl Trop Dis 8:e3301
Villar L, Dayan GH, Arredondo-Garcia JL et al (2015) Efficacy of a tetravalent dengue vaccine in children in Latin America. N Engl J Med 372:113–123
Thomas SJ (2015) Preventing dengue—is the possibility now a reality? N Engl J Med 372:172–173
Beatty ME, Stone A, Fitzsimons DW et al (2010) Best practices in dengue surveillance: a report from the Asia-Pacific and Americas Dengue Prevention Boards. PLoS Negl Trop Dis 4:e890
Horstick O, Morrison AC (2014) Dengue disease surveillance: improving data for dengue control. PLoS Negl Trop Dis 8:e3311
Morrison AC, Zielinski-Gutierrez E, Scott TW et al (2008) Defining challenges and proposing solutions for control of the virus vector Aedes aegypti. PLoS Med 5:e68
Al-Muhandis N, Hunter PR (2011) The value of educational messages embedded in a community-based approach to combat dengue fever: a systematic review and meta regression analysis. PLoS Negl Trop Dis 5:e1278
Centers for Diease Control and Prevention (2013) One health. http://www.cdc.gov/onehealth/. Accessed 15 Dec 2014
Acknowledgments
The authors thank Drs. Harold Margolis and Changwen Ke for their valuable advice on this topic, and Drs. Carol Rao and Ronald Moolenaar for their continuous supervisory support and polishing the language.
Conflict of interest
The authors declare that they have no conflict of interest. The findings and conclusions of this report are those of the authors and do not necessarily represent the official position of the U.S. Centers for Disease Control and Prevention.
Author information
Authors and Affiliations
Corresponding author
About this article

Cite this article
Li, Y., Wu, S. Dengue: what it is and why there is more. Sci. Bull. 60, 661–664 (2015). https://doi.org/10.1007/s11434-015-0756-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11434-015-0756-5