
Abstract
Concerns about the increasing consumption of medicines have been raised due to their contribution to waste pollution and environmental impacts. However, limited research addresses the profile and disposal practices of household medicines, particularly in Latin America. Therefore, this study analyzes the consumption, waste, and disposal of medicines within households in the commune of La Serena, Chile. Primary data were gathered through a semi-structured survey administered directly to a random sample of 430 households. The results indicate that women play a central role in managing medicines within households, with four therapeutic groups being most frequently used in medicines and generating waste: anti-inflammatory/analgesics, antihypertensives, lowering cholesterol, and antidiabetics. Ninety-six% of respondents were unaware of the collection points for this waste, and they disposed of it mainly in household garbage (78%) and sewage (13%). However, over 70% of them considered storing or disposing of medicines in household garbage or sewage to be “dangerous or very dangerous.” Furthermore, 97% expressed support for collection campaigns. These results indicate the need for public policies to establish collection points for this waste and to inform consumers about the responsible use and proper disposal of medicines, particularly for women and patients with chronic illnesses.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The spread of the pharmaceutical market and clinical guidelines has facilitated access to medicines in many territories. In households, these products become waste when they are no longer wanted, either because they are expired or unused. This is due to the exacerbated or inappropriate acquisition of medicines; abandonment or change of treatment in the face of symptom relief or perception of adverse effects; over-prescription by physicians; or over-selling medicines, generally due to packaging with fixed quantities that make fractioned purchases unfeasible (Lima et al. 2022). Furthermore, the literature reveals that in several countries, household pharmaceutical waste (HPW) is commonly disposed of in household garbage or sewage (Al-jalehawi et al. 2023; Althagafi et al. 2022; Chung and Brooks 2019; Pereira et al. 2019; Pérez et al. 2019; Rogowska et al. 2019; Shah et al. 2023). However, current water and municipal solid waste treatment systems do not remove many of these persistent pharmaceutical compounds (Sandoval et al. 2024), thus favoring their continuous and diffuse arrival to aquatic and terrestrial ecosystems. This has led to mandatory collection and treatment programs for these wastes in several countries (Felipe Fernandes et al. 2023; Rogowska et al. 2019; Veiga et al. 2023). Despite this, there is still a need for more knowledge about medicine consumption and disposal in households, which is crucial information for developing suitable strategies for HPW management and reducing their impacts.
There is extensive global evidence of the presence of human and veterinary medicines—analgesics, hormones, anti-inflammatories, antibiotics, stimulants, antihypertensives, among others—in surface and groundwater, drinking water, seabed sediments, soils, and wastewater and sewage sludge, as well as in animal organisms, which can affect the stability of ecosystems (Adeleye et al. 2022; Gworek et al. 2020; Pivetta and Gastaldini 2019). In Latin America, Sandoval et al. (2024) emphasize that the main products detected in water bodies are atrazine, acenaphthene, caffeine, carbamazepine, ciprofloxacin, diclofenac, diuron, estrone, losartan, sulfamethoxazole, and trimethoprim. In Chile, hormones and anti-inflammatory medicines have already been detected in surface water, groundwater, affluent, and effluent from water treatment plants (WTP) in the country’s central region (Arismendi et al. 2019).
The negative impacts of these pollutants on ecosystems are multiple. Some of them are sexual anomalies in fish (Bain 2010) and frogs (Kvarnryd et al. 2011), resistance of pathogenic microorganisms to antibiotics, development of cancer (Bain 2010), metabolic disorders (Pivetta and Gastaldini 2019), and eco-toxicological risks (Adeleye et al. 2022; Gworek et al. 2020). These impacts can be increased in territories where there is no systematic process for collecting HPW at the national level, such as Chile. To our knowledge, there are no studies on the consumption of medicines in households and the profile of HPW in Chile. Information regarding the country’s knowledge, management, and final disposal of these wastes was not found. Therefore, knowing the situation of these wastes in Chile is relevant to reducing the local and regional information gap and contributing to the global perception of the problem of HFW in different socio-cultural and economic contexts.
This study aims to analyze the consumption, waste, and disposal of medicines in households in the commune of La Serena, Chile. This is essential for developing strategic actions to adequately manage expired or unused household medicines and thus reduce their environmental impacts. For this purpose, 430 semi-structured surveys were carried out and applied directly in the urban and rural areas of the study area, addressing four aspects: the socioeconomic profile of the household representative, the consumption of medicines, the method of disposal, and the perception of consumers concerning the HPW problem.
Our study is the first approximation of the consumption of medicines and their waste in Chilean households. This information supports formulating public policies or specific strategies aimed at the responsible consumption of medicines in households and the minimization, collection, and environmentally proper disposal of HPW.
Methods
Study area
In Chile, the regions with the highest prevalence of use of at least one medicine (over 63%) are Coquimbo, O’Higgins, and Metropolitana (Passi et al. 2019). In Coquimbo region, the cities of Coquimbo and La Serena likewise concentrate 45% of the 196,821 private households (PH) in the province of Elqui (Instituto de Salud Pública de Chile (ISP), 2019). However, in contrast to the city of Coquimbo, in La Serena, the distribution of inhabitants in urban and rural (90.8% and 9.2%) areas is close to that of the province of Elqui and the country (87.8% and 12.2%) (INE 2019). For this reason, the commune of La Serena is chosen as the area of study to represent the characterization of medicine consumption, management, and disposal of HPW in one of the regions with the highest medicine consumption. La Serena has an area of 129 km2 and a population of 221,054 inhabitants, which corresponds to 29.2% of the 757,586 inhabitants of the Coquimbo region and 1.2% of the national total: 17,574,003 people (INE 2017).
Population and sample determination
In 2017, La Serena presented 87,267 PH, corresponding to 99.8% of the type of households in the commune, being the other collective households (INE 2017). Thus, the unit of analysis under study is the PHs. According to INE (2017), the PH is a property destined, totally or partially, to the permanent or temporary habitation of one or more persons. To be considered such, it must have independent access for its dwellers. The concept of property does not refer to legal ownership but rather to a geographic space with recognizable boundaries.
In this context, considering the large size of the population of interest and the importance of saving time and resources in gathering information, we opted for a probabilistic sample applied to large (over 100,000 individuals) and finite populations, calculated by using Eq. 1 (Hernández Sampieri et al. 2014):
where n corresponds to the sample size; z is the value of the standard normal table associated with the desired 95% confidence level (1.96); p is the maximum variability of the population (0.5); q is equivalent to the proportion of individuals who do not possess that characteristic, i.e., 1-p (0.5); N is the size of the universe of individuals (87,267 PH); and e corresponds to the maximum accepted error (5%) (Paut Kusturica et al. 2016). From the above, a sample of 382 PH was obtained, to which 10% was added to overcome incomplete or invalid data, totaling 421 PH.
The sampling frame used to identify the sample elements (the PHs) is a list and map elaborated from the microdata of the 2017 Census (INE 2017), where there are two types of primary sampling units (PSU): 1—the blocks in the urban area and 2—the entities in the rural area. According to Hernández Sampieri et al. (2014), in studies with a map sampling frame, the use of clusters/conglomerates is applied, and stratification increases the precision of the sample by considering strata or categories that are relevant in the population. Thus, the sampling of the units of analysis was stratified (between urban and rural areas) and by clusters/conglomerates (proportionally to the two types of PSUs) (Table 1).
The PSUs were selected randomly using the “randbetween” function of the Excel software, which uses an internal algorithm to generate a random number between two specified values. In the selected PSUs, all the PH were visited for interviews until a number equal to or greater than the calculated sample was completed: 421 PH.
Data collection and analysis
To reach the objective proposed, the study has a non-experimental methodological design and a mixed approach, with collection and analysis of quantitative and qualitative data, as well as their integration and combined discussion (Hernández Sampieri et al. 2014). Nine stages were carried out for data collection, executed for 16 months: June/2021 to September/2022 (Fig. 1). This included from the survey’ design to the review of the data tabulation by personnel external to the research.

Process for obtaining primary data from May 2021 to September 2022. T, period of the activity; D, duration of the activity; P, number of people involved
The instrument used to collect data was the semi-structured interview form, developed from the literature review on medicine consumption and HPW generation (Dias-Ferreira et al. 2016; Ministerio de Salud de Chile [MINSAL] 2011). Government reports and studies available in the ScienceDirect and Web of Science databases were used. The terms “household medicine waste” and “pharmaceutical waste” were used as search engines, in addition to their respective equivalents in Portuguese and Spanish, to broaden the literature base on the subject in Latin America.
The interview was designed for an application time of approximately 15 min and consists of 2 open questions and 16 closed questions, including dichotomous and multiple-choice questions, regarding three aspects: (1) socioeconomic and demographic profile of the leading household provider; (2) use, acquisition, and storage of medicines; and (3) generation and management of HPW. The application of this instrument was carried out directly in households in the commune of La Serena through face-to-face interviews with adults (aged 18 years or older), representatives of the households, with knowledge about the medicines used in the household. The exclusion criterion was people with cognitive limitations.
The interview form was validated by five expert judges from medicine, pharmacy, and environment, with experience from 12 to 52 years. The purpose was to ensure that the form measures the variables of interest and has clear, precise, and understandable questions and answer options. Content validity was determined using the judges’ logical-critical analysis of each question by applying the Content Validity Coefficient (CVC) of Hernández-Nieto (2011). The evaluation of each judge was independent and voluntary and carried out through a content validity form (FVC).
The FVC had three sections: (1) judge’s profile, for recording first and last name, academic degree, affiliation, and years of experience; (2) instructions on the judge’s degree of agreement, on a 5-point Likert scale (1 = strongly disagree; 2 = disagree; 3 = neither agree nor disagree; 4 = agree; 5 = strongly agree); (3) judge’s evaluation regarding the adequacy (clarity, response options, logical order) and relevance of each question and response items, plus the need for modifications, recommendations, and reasons for such. The validation process was carried out for two months, with a response time of approximately one month from the judges.
Subsequently, a pilot test was conducted on 10 participants not included in the sample of interest to evaluate reliability and application conditions, detect possible flaws, and correct the form. After obtaining the final form, the research was submitted for approval to the Ethical-Scientific Committee of the Universidad de La Serena (CEC-ULS) as the study is applied in homes and involves the participation of people. The CEC-ULS analysis lasted slightly over a month.
Parallel to the analysis of the CEC-ULS, a call for volunteer interviewers was made through social networks and advertisements on the ULS installations. At this stage, 27 interviewers were selected, including undergraduate students and researchers of the project, who participated in a 2-h training on ethical, technical, and safety aspects for the proper conduction of the interviews.
The interviews were conducted in June and July 2022. They were conducted in pairs, preferentially a man and a woman, outside the homes (at the door) to reduce possible security problems. Initially, the interviewers were presented wearing uniforms, credentials, and a project card with a QR code that gave access to the university’s website with information about the project to generate confidence in the participants. After that, the interview began with the prior written consent of the participants.
During the interviews, it was also asked if there was HPW in the household and, if so, if the participant wanted to deliver it to the project for subsequent characterization and send it to the appropriate final treatment: incineration. The waste received was stored in plastic bags and labeled with a code corresponding to the respective household. This same code was used to identify the interview forms and anonymize confidential household information during the data tabulation stage. Thus, the tabulation does not contain participants’ names, household numbers, or other data that would allow their individualization. The HPW collected were characterized in terms of the type of packaging, expiration date, pharmaceutical presentation (solid, liquid, semisolid, ampoule, and aerosol), condition of sale, number of doses, active ingredients, and pharmacological groups, according to the medicine’s technical data sheet. The mass of these residues was also determined using a PTQ-A30 electronic balance, with a capacity of 30 kg and a resolution of 0.1 g.
Two researchers recorded the information obtained in a database for 1 month. After this, a person external to the research verified the data to determine if there were discrepancies between the electronic information and that recorded on the physical forms, correcting them before the descriptive statistical analysis.
Results
This section is divided into four parts, beginning with a profile of the members of the households studied and their demographic and socioeconomic characteristics (the “Interviews of household representatives” section). Next, it describes the medicines frequently used in the household, detailing their consumption, frequent diseases, way of acquisition, active ingredients, and aspects related to their storage and monitoring (the “Medications frequently used in households” section). The HPW collected during the interviews are also described, specifying their mass and validity, among others (the “Household pharmaceutical waste profile” section). Finally, knowledge of collection points, ways of discarding HPW, and the consumer’s perception of possible actions to reduce the problem of this waste is addressed (the “Household pharmaceutical waste disposal” section).
Interviews of household representatives
A total of 640 visits were made to homes located in the urban and rural areas of La Serena (Fig. 2) during four Saturdays between June and July 2022, from 9:00 A.M. until 6:00 P.M. This considering the greater presence of people in their homes on non-working days in Chile. Each day of visits had a group of 7 to 10 pairs of interviewers who collectively executed about 100 interviews per day.

Location of the study area. Left—urban zone, where selected blocks include the sectors of Centro, El Olivar, Las Compañías, La Florida, La Pampa, San Joaquín, and Barrio Universitario; right—rural zone, being selected El Romero, El Rosario, and Pelícana
During the 640 visits, 430 interviews were conducted (67%). Thus, the participation refusal rate was 33% (Fig. 3). As for the profile of the household representatives interviewed, a large number were women (274; 63.7%) and adults (194; 45%) aged between 46 and 65 years (Fig. 3). In general, about four persons lived in each household (\(\overline{x }\), SD, median: 4; 2; 4).

Interviews conducted in households in the commune of La Serena, Chile, during June and July 2022. Left—number of interviews conducted and rejected in urban and rural areas; right—age group and sex of household representatives interviewed
In terms of educational level, more than 2/3 of household breadwinners have completed secondary school (208; 48%) or graduate education (102; 24%). Among the current occupations, slightly more than half are professionals, scientists, and intellectuals (90; 21%), unskilled workers in sales and services, agricultural, forestry, or construction laborers (65; 15%), other unidentified groups, such as pensioners, retirees, and others (53; 12%), and workers in services and trade or market sales (43; 10%).
Medications frequently used in households
The frequent use of medications was confirmed by 92% of the representatives of the households interviewed. Of these, the main pharmacological groups mentioned were anti-inflammatory medicines, antihypertensives, hormones, and antidiabetics, totaling 84 active ingredients (Fig. 4). Of these active ingredients, 42.3% corresponded to paracetamol and non-steroidal anti-inflammatory drugs (NSAIDs), especially ibuprofen and diclofenac. Another relevant group was drugs for continuous use, with particular emphasis on antidiabetic drugs (49; 11.3%) such as insulin, and those for cardiovascular control (79; 18.2%), mainly antihypertensives and cholesterol-lowering drugs such as losartan, metformin, atorvastatin, and others.

Main medicines (a) and therapeutic groups (b) frequently used in households in the commune of La Serena, Chile, during June and July 2022
The above is consistent with the most frequent diseases that occur in households, such as general complaints (538; 54%), hypertension, and other cardiac problems (163; 20%) (Table 2). The acquisition of medicines occurs mainly in commercial drugstores (339; 74.2%) and the public health system (109; 23.9%), with little influence of neighborhood businesses, small market, or free fairs (6, 1.3%). The most frequent buying condition is through prescription (265; 61.6%), while about a third indicated buying over the counter (149; 34.7%). The acquisition frequency is mainly monthly (245; 57%) or when an ailment or malaise occurs (108; 25%), in the latter case, without medical advice.
Table 3 shows that medicine storage occurs in only half of the households (217; 50.5%), most of which have between 1 and 10 primary packages of medicines (158; 36.7%). The most common reasons for storage were to deal with an eventuality (88; 18%), products that are not expired (74; 15.1%), and a package that had more medicines than required (48; 9.8%), considering that, in many cases, drugstores do not sell at the retail level (Table 3). The group “others” includes frequent use, change of treatment, or death of the patient.
83.7% (373) of the participants affirm that they check the expiration date of the medicines. In general, this occurs at consumption (127; 29.5%), every month (123; 28.6%), or every 3 months (45; 10.5%).
Household pharmaceutical waste profile
Eleven percent (49) of the interviewees reported having HPWs at the time of the interview. Of these, 36 agreed to give their HPWs, while 13 refused. Thirty-nine percent of them had these HPWs due to abandonment of treatments or storage to face some eventuality.
The HPW received was quantified regarding its mass and packaging units. Regarding the mass of the medicines—including primary and secondary packaging—a total of 13,036 g of HPW was received (Fig. 5a), which had an asymmetric distribution among households: \(\overline{x }\) 395.5, SD 1188.7, median 100, min. 7.2, and max. 6831.3. Of these, 94% (12,262 g) corresponds to waste in its primary packaging, while the remaining corresponds to uncontaminated secondary packaging composed of paper or cardboard boxes.

Mass (a) and validity (b) of HPWs collected during interviews conducted in households of the La Serena commune, Chile, during June and July 2022
Regarding the number of packages—such as blister packs, bottles, ampoules, aerosols, among others—a total of 535 primary packages of medicines were received (Fig. 5b), with asymmetric amounts of primary packages per household: \(\overline{x }\) 16, SD 22, median 7, min. 1, and max. 96. It is important to note that 41.9% of them were valid, where May/2025 was the most extended validity date, i.e., unused medicines suitable for consumption. On the other hand, 57% were expired medicines, with May/2014 being the oldest expiration date, which indicates low monitoring or elimination of medicines unsuitable for consumption.
Most of the HPW received is in solid form (84%) and is sold by prescription (77%) (Fig. 6). Medications such as ampoules, creams, and sprays were in tiny quantities.

Pharmaceutical form and condition of sale of HPW collected during interviews conducted in households of the La Serena commune, Chile, during June and July 2022
However, considering that the primary packages were not always complete of medicines and that this would lead to an extrapolation in the number of medicines, the number of doses in each package was counted. This was applied only for medicines in solid form, considering their representativeness in this study, and because small volumes of liquids—such as eye drops, for example—generated a discrepant total of doses when compared with those in solid form or with liquids with larger volume doses, such as syrups.
Thus, HPW in solid form totaled 8127 doses distributed among 96 products, of which three pharmacological groups prevail: (1) anti-inflammatory/corticosteroid analgesics (3,031; 37%), such as fluticasone propionate; (2) those that act on the cardiovascular system (1434; 17. 6%), whether cholesterol-lowering or antihypertensive, such as atorvastatin, hydrochlorothiazide, and losartan; and (3) antidiabetics (495, 6.1%), such as metformin hydrochloride (Fig. 7). Antacids were not included as a predominant group of HPW in the households because they were from a single household, being originated from the change of treatment of a single patient.

Active ingredients (a) and pharmacological groups (b) of HPWs, according to solid and liquid state, collected during interviews conducted in households of the La Serena commune, Chile, during June and July 2022. (1) In pharmaceutical products, it was considered the active ingredient with the highest concentration in the medicine; (2) for pharmacological groups, only HPWs in the solid state were considered
Household pharmaceutical waste disposal
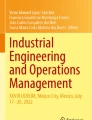
Ninety-six percent of those interviewed were unaware of HPW collection points, while only 1.9% were informed that the Red Cross receives unused medicines with current validity. HPW is mostly disposed of in household garbage (336; 78%) and sewage (56; 13%) (Fig. 8).

Disposal routes for HPWs in 430 households of La Serena commune, Chile, during June and July 2022
However, it is important to highlight that 70% of those interviewed consider it dangerous or very dangerous to store medicines at home and dispose of them in household garbage or sewage (Table 4). According to them, this is mainly due to risks of accidents with children who may consume these medicines and environmental contamination.
On the other hand, 97% of the participants stated that they would participate in campaigns to collect expired or unused medicines. For this, they highlighted three points as the main motivating factors: more collection points in the city (290/629; 46%), the nearness of these points to the home (102/629; 16%), and knowledge that HPW would be appropriately managed (95/629; 15%). Other options mentioned were access to more information on the danger of disposing of medicines in the environment, getting economic incentives, exchanging one medicine for another, making donations, and disposing of HPW at enterprise collection points.
Last, we also asked about a possible personal contribution and that of other stakeholders to minimize the MW problem. Most of the interviewees emphasized the individual need to receive more information and knowledge on the subject, as well as the responsible acquisition and consumption of medicines, avoiding excess/leftovers. Regarding the other stakeholders, they mentioned that the national government and municipalities should establish public policies to install permanent medicine waste collection points and promote information campaigns in the communities.
Discussions
Interviews of household representatives
At the end of the application of the surveys, we observed that the refusal rate obtained in this study (33%) is lower than in other studies with data collection through telephone interviews or self-administered forms, such as that of Paut Kusturica et al. (2016), which received 62% refusal of telephone interviews after contacting 1008 people in their homes, and that of Rogowska et al. (2019), which obtained 37% of non-responses from the 1000 forms left by HPW collection points in Poland. We believe that applying forms through face-to-face interviews contributed to obtaining more responses despite their higher cost and execution time. In addition, direct interviews have the advantage of ensuring the reliability of the information collected by training the interviewers to solve doubts and reduce ambiguities in the participants’ answers.
Regarding the participants’ sex, women were prevalent in all age groups, which indicates that women’s role in managing household medicines is relevant. In addition, during the interviews, men frequently mentioned, “The woman of the home is the one who knows/handles the medicines. I will call her.” Morales-Rojas et al. (2023) and Veiga et al. (2023) also highlight the above in Mexican and Portuguese households, respectively. These last authors also associate women with correct HPW disposal practices.
It is important to highlight that the HPW problem was presented as a cross-cutting factor at different socioeconomic levels since most interviewees have a high education level and a diverse range of occupations. At the same time, almost all of them (96%) lack information about HPW and dispose of it improperly. However, considering there are no HPW collection points in the area under study, it is essential to reevaluate this aspect in areas where HPW collection points exist.
Consumption of medicines in households
Medicines are regularly used in almost all (92%) households studied. Furthermore, the frequent illnesses in the household (ailments in general or chronic diseases) coincided with the pharmacological group of medicines regularly used (NSAIDs and those of continuous use: antihypertensives, cholesterol-lowering medicines, and antidiabetics). These results show a similarity between the case study area’s situation and the national one since among the active ingredients with the highest consumption in the country are, in the first place, paracetamol (12.4%), acetylsalicylic acid (10.7%), losartan (10.3%), metformin (9.5%), and atorvastatin (7.6%) (Ministerio de Salud de Chile (MINSAL), 2018). Similar findings were observed in Ethiopia, Indonesia, China, and Poland, where analgesics and cold medicines were the main medicines consumed in households (Bekele et al. 2023; Chung and Brooks 2019; Rogowska et al. 2019; Septianingrum et al. 2021). These findings may be related to the easy access to medicines, such as NSAIDs that are low cost and sold without prescription; the increasing prevalence of obesity in many countries, which may contribute to diseases such as diabetes, hypertension, and dyslipidemia; increased accessibility of pharmaceutical therapies; and the evolution of clinical guidelines.
The medicine providers were mostly commercial drugstores, medical offices, hospitals, or the public health system network. According to MINSAL (2018), 95% of the national population also obtains medicines from these providers. This puts drugstores and the health system as critical stakeholders in informing and raising consumer awareness about the responsible use and handling of medicines, from the acquisition process to disposal at collection points. This health professional-supplier–consumer relationship is fundamental to improving HPW management, considering many consumers purchase medicines monthly.
Despite using medicines in almost all households, only half of the participants claimed to stock them. Therefore, we believe that we obtained an underreporting of medicine storage, mostly of up to 10 products and motivated by preventive purchases or leftover packaging that had a higher quantity than required. The denied storage is probably because the participants considered it a negative response, or they relate the storage to a first aid box where all medicines are stored, which is often non-existent in households. Althagafi et al. (2022), Correia and Marcano (2016), and Shah et al. (2023) also reported that 49% (n = 1100), 17% (n = 1152), and 81.6% (n = 676) of their study participants claimed to store leftover medicines at home, respectively. Morales-Rojas et al. (2023) warn that leftover medicines can be misused and lead to risks for people, such as self-medication and medicine poisoning, especially in children and older people. These risks could be reduced through the retail sale of medicines, favoring the purchase of medicines according to the amount required by the consumer.
The expiration date of medicines is reviewed mainly before consumption or for up to 1 month. The prevalence of review in short periods favors the proper management of products, such as monitoring of storage conditions (access, humidity, temperature, and others) (Morales-Rojas et al. 2023), preference for the consumption of products with earlier expiration dates, and donation of unwanted medicines and medicines from completed or atypical treatments to minimize their conversion into waste. Patient education on properly handling of medicines at home is essential in reducing the wastage of these products and reducing possible environmental damage.
HPW profile
Almost half of the HPW collected in this study were current medications, a large part of which originated from storage due to the abandonment of treatments or to deal with some emergency. This indicates the importance of greater attention from (1) health professionals and patients for the control and adaptation of medicine treatments; (2) consumers to avoid self-medication and excessive purchase of medicines; and (3) suppliers to ensure retail sales, reducing sales in quantities greater than those required by the consumer.
In addition, it is also important to disseminate the possibility of sharing unexpired medicines with third parties or donating them to healthcare entities, such as the Red Cross, whenever possible. In Chile, the donation of unexpired medicines to health facilities is regulated by D.S. 3/10 MINSAL (Ministerio de Salud de Chile (MINSAL), 2010). Such donation is also lawful in Mexico, where unexpired medicines in good condition are received in penal town halls, integral family development, and establishments for older adults (Pérez et al. 2019). Furthermore, in general, the donation of medicines is welcomed by consumers, an example being the study by Ong et al. (2020), where 68% of respondents considered it a mistake to discard unused medicines in good condition and expressed their willingness to donate them before they expire; half of them would also share their excess medicines with others. Finally, it is worth emphasizing some of the benefits of donating medicines, such as supporting low-income people in need of medicines, reducing medicine waste, and minimizing environmental impacts and accidents due to improper consumption of medicines, mainly by children.
As for the pharmacological groups of HPWs, corticosteroid anti-inflammatory/analgesics and those acting on the cardiovascular system predominated. These last ones are similar to the profile of often-used medicines in the studied households. However, they are different from those reported by other studies, such as those conducted in China, South Africa, and Iraq, where analgesics and anti-influenza medicines are the most common medicine waste, with paracetamol standing out (Al-jalehawi et al. 2023; Chung and Brooks 2019; Magagula et al. 2022).
This group of medicines also figures as emerging contaminants in the study by Wilkinson et al. (2022), who measured active pharmaceutical compounds in rivers in 104 countries, where among those detected in all continents are over-the-counter (OTC) medicines, such as acetaminophen/paracetamol (analgesic) with the highest concentration among the compounds, 227 μg/L. Additionally, besides Antarctica, other contaminants also detected globally are naproxen (anti-inflammatory), atenolol (β-blocker), cetirizine and fexofenadine (antihistamines), lidocaine (anesthetic), metformin and sitagliptin (anti-hyperglycemic), and others.
HPW disposal
The lack of knowledge about HPW collection points can be explained by the fact that there are no HPW collection programs in the study area or at the national level since this waste is not included as a priority product in the Chilean Extended Producer Responsibility (EPR) Law (Ministerio del Medio Ambiente [MMA] 2016). Nowadays, Felipe Fernandes et al. (2023) reveal that HPW collection in Chile is voluntary and occurs on an isolated basis in some drugstores and communes in the central region. Other 13 studies conducted in Africa and Asia also show that only 3 to 33% of the public knew proper disposal methods or had received/read instructions on this waste (Hiew and Low 2024; Shah et al. 2023).
Inadequate disposal of HPW predominates in the households under study, where the main disposal routes are household waste and sewage. Similar results were reported in Brazil, China, Iraq, Mexico, Pakistan, Poland, Saudi Arabia, and Venezuela, where disposal in household garbage was 54 to 81% (Al-jalehawi et al. 2023; Althagafi et al. 2022; Chung and Brooks 2019; Correia and Marcano 2016; Pereira et al. 2019; Pérez et al. 2019; Rogowska et al. 2019; Shah et al. 2023). The latter reveals the inadequate disposal of HPW as a current practice in many countries and continents, which lack effective actions to enhance the collection of these wastes. Additionally, studies such as Wilkinson et al. (2022) reveal the contamination by pharmaceutical compounds in rivers across 104 countries in all continents, where Pakistan, Bolivia, and Ethiopia present higher average cumulative concentrations of these pollutants: 70.8 μg/L, 68.9 μg/L, and 51.3 μg/L. Thus, the problem of HPW is especially worrisome in territories with limited regulation of these emerging pollutants and deficient water and solid waste treatment infrastructures, increasing the risks to the ecosystem and human health.
Household waste and effluents in the Coquimbo region have different management forms and most favor the dispersion of HPW. This region does not have a selective collection of household solid waste or HPW; in addition, most of its final waste disposal sites are landfills (9; 90%) are operational and receive almost half of the area’s waste (188,315 tons; 44%) (Subsecretaría de Desarrollo Regional y Administrativo de Chile (SUBDERE) 2024). This indicates that inadequate disposal of solid household waste occurs in considerable quantity and is scattered throughout the territory, favoring the dispersion and impacts of HPW on the soil and water bodies. On the other hand, domestic effluents are sent to submarine outfalls (29,696,342 m3; 72%) used mainly in the coastal area, such as in the urban areas of La Serena city, while in inland and rural areas the effluents are usually sent to activated sludge systems (1,220,909 m3; 3%) and aerated lagoons (10,313,177 m3; 25%) (Aguas del Valle 2022). These traditional methods of domestic effluent treatment do not effectively remove pharmaceutical residues and favor their dispersion in natural ecosystems (Sandoval et al. 2024). One way to reduce the input of HPW into water and waste treatment systems is to implement collection points and promote environmental education among consumers about the problem of this waste, encouraging its environmentally sound disposal. In addition, the presence and concentration of medicine wastes in local water bodies should be analyzed, and based on this, the need for further implementation of effluent treatments capable of removing these pollutants, such as ozonation, advanced oxidation processes (AOP), adsorption with activated carbon or membranes (Gworek et al. 2020).
On the other hand, there is also a dissonance between consumer knowledge, attitude, and practice (KAP) about HPW, which has little knowledge, positive attitudes towards collection programs, and inadequate disposal practices. Similar results were observed in Hiew and Low (2024), where most respondents agreed that there is a lack of information and points for the safe disposal of medicines. These authors explain that inadequate disposal of HPW, linked to a deficit of information and accessible disposal facilities, is compounded by insufficient guidance from health professionals. In this context, it is essential to prevent the generation of HPW. Medications should be used only when necessary, and the health professional should provide guidance not only on the use/posology of the medicine but also on the importance of avoiding leftover medicines to reduce waste generation (this type of guidance could be printed by default on medical prescriptions). At the same time, the medicine leaflet or packaging should emphasize the correct storage and disposal of the medicine in the same way as it does for information on the composition, indications, dosage, interactions, and others.
Participants of this study perceive the storage of medicines as a risk of accidents with children who may consume these products accidentally, as in some cases experienced by them. Hiew and Low (2024) explain that contamination and risks of accidents, especially with children, are the main issues of the public concerning HPW. In Chile, acute medicine poisonings have continuously increased in recent years, a large part (85%) being due to suicide attempts, mainly with clonazepam (14%) and paracetamol (10%) (Instituto de Salud Pública de Chile (ISP) 2019). Paracetamol was the most widely used active ingredient in the households in this study, probably because it has a wide range of uses and can be purchased over the counter. Additionally, Grabska and Pilarska (2022) explain that medication poisonings are frequent in accidents with children but also suicide attempts among adolescents, with over-the-counter analgesics being the most common cause of acute poisoning. Thus, it is important to restrict children’s and adolescents’ access to medicines stored in the home, using locked storage boxes. Likewise, households should seek rational storage of these products in quantities that comply with medical guidelines. However, they should avoid too many surpluses, as they could be improperly used or become waste due to non-use within the validity period.
Finally, it is essential to note that medicine users identify that HPW management requires consumer and government efforts. They highlight the responsible consumption of medicines, the promotion of information through community and/or mass media campaigns, and the establishment of collection points, preferably located near homes. The latter was also an important factor in the study by Veiga et al. (2023), where the distance between homes and drugstores with collection points was a significant variable for HPW collection in Portugal.
Final comments
The results show the importance of establishing points for collecting HPW and raising consumer awareness on the acquisition and responsible use of medicines, with information from the health clinic to the medicine distribution establishment. In the case of treatments prescribed by health professionals, proper follow-up of the therapy is decisive to avoid leftover medicines becoming waste, and if they exist, they can be donated while they are still useful, following the regulations of each country. Thus, the proper management of HPW depends on the mutual responsibility of consumers and public and private institutions.
In this study, no HPW for veterinary use was received, and only a small part of the sample (7.4%) gave us their HPW for later analysis. Therefore, for comparative purposes, future studies can focus on collecting HPW from a larger sample of households and consider the inclusion of veterinary medicines, taking care to classify them and avoid receiving waste that corresponds to more than one household or comes from health entities/services. This is because some studies characterize HPW received directly at collection points, not at homes.
In addition, a limitation of the study was comparing the data obtained with the existing literature, which mostly has the primary package as the unit of analysis rather than the number of doses. This highlights the importance of using a unit of analysis (packaging, number of doses, mass, or other) to provide reliable information about the collected HPW, such as mass or pharmacological group. This is relevant to avoid comparative biases in the data reported.
Conclusions
The study analyzed the consumption, waste, and disposal of medicines in households of the La Serena commune, Chile. This is the first approach to the subject in the country, and although it is in a local context, the HPW issue is global. Thus, these findings highlight common routes for policies and health campaigns in public and private institutions as well as the practices of consumers and health professionals on properly managing medicines to prevent HPW and minimize associated environmental impacts. The above, mainly in countries where there is no legislation for the collection and disposal of HPW, and it is more critical in territories with reduced availability or quality of solid waste and domestic effluent treatment systems.
Women’s role in managing household medications is noteworthy, as well as the similarity between the pharmacological groups of stored and wasted medicines. In both groups, anti-inflammatories and analgesics, antihypertensives, cholesterol reducers, and antidiabetics were prevalent. Therefore, strategies and public policies for HPW management should consider special attention to the female public and patients with chronic diseases who make continuous use of the pharmacological groups listed above to avoid abandonment of treatment or medical recommendations, which causes their medicines to go unused and become waste when they reach their expiration date.
Furthermore, the participant’s lack of knowledge about environmental problems and the inadequate disposal of HPW accentuates the need for efforts to inform them, raise their awareness, and change their attitudes. In this context, the actions of health professionals, health centers, and medicine distribution sites are essential. Likewise, it is important to promote permanent and periodic campaigns—such as May 17, World Recycling Day—to disseminate the importance of the responsible use of medicines and the collection of HPW to generate an accentuated and sustainable intervention towards the prevention and appropriate management of this waste.
Data availability
The authors confirm that all data generated or analyzed during this study are included in this published article.
References
Adeleye AS, Xue J, Zhao Y, Taylor AA, Zenobio JE, Sun Y, Han Z, Salawu OA, Zhu Y (2022) Abundance, fate, and effects of pharmaceuticals and personal care products in aquatic environments. J Hazard Mater 424:127284. https://doi.org/10.1016/j.jhazmat.2021.127284
Aguas del Valle (2022) Sustainability report. Esval S.A. https://www.esval.cl/media/xz0orh0w/reporte-de-sostenibilidad-adv-2022.pdf (in Spanish). Accessed 26 June 2024
Al-jalehawi A, Al-zidan R N, Al-mahmood S, Azeez A, Fakhreldin L (2023) Exploring household medicine waste in Iraq. Latin American Journal of Pharmacy, 42 (4th International Scientific Conference of Alkafee University (ISCKU)), 5–11. https://doi.org/10.21203/rs.3.rs-1613875/v1
Althagafi A, Alshibani M, Alshehri S, Noor A, Baglagel A, Almeleebia T (2022) Assessment of knowledge and awareness of safe disposal of unused or expired medication in Saudi Arabia: a cross-sectional study. Saudi Pharmaceutical Journal 30(11):1672–1678. https://doi.org/10.1016/j.jsps.2022.09.012
Arismendi D, Becerra-Herrera M, Cerrato I, Richter P (2019) Simultaneous determination of multiresidue and multiclass emerging contaminants in waters by rotating-disk sorptive extraction–derivatization-gas chromatography/mass spectrometry. Talanta 201:480–489. https://doi.org/10.1016/j.talanta.2019.03.120
Bain KT (2010) Public health implications of household pharmaceutical waste in the United States. Health Serv Insights 3:HSI.S4673. https://doi.org/10.4137/HSI.S4673
Bekele DW, Dadebo E, Tilahun G (2023) Gebremariam Z (2023) Awareness and disposal practices of medicines among the community in Hawassa City Ethiopia. J Toxicol 1:4603993. https://doi.org/10.1155/2023/4603993
Chung S, Brooks BW (2019) Identifying household pharmaceutical waste characteristics and population behaviors in one of the most densely populated global cities. Resour Conserv Recycl 140:267–277. https://doi.org/10.1016/j.resconrec.2018.09.024
Correia A, Marcano L (2016) Evaluation of the income routes of domestic use pharmaceutical compounds to the environment study case: Municipaly of Vallencia, Carabobo state, Venezuela. Revista Internacional de Contaminacion Ambiental, 32(1), 77–86. http://www.scielo.org.mx/scielo.php?script=sci_arttext&pid=S0188-49992016000100077&lng=es&nrm=iso
Dias-Ferreira C, Valente S, Vaz J (2016) Practices of pharmaceutical waste generation and discarding in households across Portugal. Waste Manage Res 34(10):1006–1013. https://doi.org/10.1177/0734242X16639388
Felipe Fernandes JA, Álvarez P, Carvajal D, Mera AC, Garcia GM, Aguiar Silva LD (2023) Challenges of household medical waste collection systems: an analysis of regulatory instruments and stakeholders in three Latin American countries. J Environ Plan Manag 30:1–25. https://doi.org/10.1080/09640568.2023.2232539
Grabska K, Pilarska I (2022) Acute poisoning among children and adolescents: a narrative review. Med Sci Pulse 16(2):1–7. https://doi.org/10.5604/01.3001.0015.9656
Gworek B, Kijeńska M, Zaborowska M, Wrzosek J, Tokarz L, Chmielewski J (2020) Occurrence of pharmaceuticals in aquatic environment-a review. Desalin Water Treat 184:375–387. https://doi.org/10.5004/dwt.2020.25325
Hernández Sampieri R, Fernández C C, Baptista L M del P (2014) Research methodology, 6th edn. McGraw-Hill, Mexico D.F. (in Spanish)
Hernández-Nieto R (2011) Data collection instruments in social sciences and biomedical sciences. CreateSpace Independent Publishing Platform, Mérida (in Spanish), Validity and reliability. Design and construction. Standards and formats
Hiew SY, Low BY (2024) The knowledge, attitude, and practice of the public regarding household pharmaceutical waste disposal: a systematic review (2013–2023). Int J Pharm Pract 32(2):120–32. https://doi.org/10.1093/ijpp/riae001
Instituto de Salud Pública de Chile (ISP) (2019) Statistics on acute poisonings reported to the National Pharmacovigilance Programme, period 2012–2018. https://www.ispch.cl/newsfarmacovigilancia/15/images/parte02b.pdf (in Spanish). Accessed 26 June 2024
Instituto Nacional de Estadísticas de Chile (INE) (2017) Census: Housing Results. http://www.censo2017.cl/descargue-aqui-resultados-de-comunas/ (in Spanish). Accessed 10 May 2021
Kvarnryd M, Grabic R, Brandt I, Berg C (2011) Early life progestin exposure causes arrested oocyte development, oviductal agenesis and sterility in adult Xenopus tropicalis frogs. Aquatic Toxicol 103(1):18–24. https://doi.org/10.1016/j.aquatox.2011.02.003
Lima PAB, Delgado FCM, dos Santos TL, Florentino AP (2022) Medications reverse logistics: a systematic literature review and a method for improving the Brazilian case. Clean Logistics Supply Chain 3:100024. https://doi.org/10.1016/J.CLSCN.2021.100024
Magagula BK, Rampedi IT, Yessoufou K (2022) Household pharmaceutical waste management practices in the Johannesburg Area, South Africa. Int J Environ Res Public Health 19(12):7484. https://doi.org/10.3390/ijerph19127484
Ministerio de Salud de Chile (MINSAL) (2010) Decree 3 of 25 January 2010, approving the regulation of the national control system for pharmaceuticals for human use. Subsecretaría de Salud Pública, 2010, 2021–2023. https://bcn.cl/2f8qc (in Spanish).
Ministerio de Salud de Chile (MINSAL) (2011). Rational use of medicines survey final report. Minsal, 61. http://web.minsal.cl/sites/default/files/files/Informe Final - Estudio URM MINSAL.pdf (in Spanish). Accessed 12 May 2021
Ministerio de Salud de Chile (MINSAL) (2018). National health survey 2016–2017: use of medicines. http://epi.minsal.cl/wp-content/uploads/2018/12/2018.12.24_Presentación-uso-de-medicamentos-ENS-2016-2017_RevJIA.pdf (in Spanish). Accessed 14 February 2022
Ministerio del Medio Ambiente (MMA) (2016) Law 20.920 of 1 June 2016, which establishes the framework for waste management, extended producer responsibility and recycling promotion. Biblioteca del Congreso Nacional de Chile (BCN), 1, 1 de June de 2016. https://bcn.cl/2f7b2 (in Spanish).
Morales-Rojas M, Aké-Canul D, Balam-Gómez M, Cohuo-Cob S (2023) Risk factors associated with excessive storage of medicines in an urban area of Mexico. Ciencia y Enfermería, 29. https://doi.org/10.29393/CE29-16FRMS40016 (in Spanish). Accessed 26 June 2024
Ong SC, Ooi GS, Shafie AA, Hassali MA (2020) Knowledge, attitude and disposing practice of unused and expired medicines among the general public in Malaysia. J Pharm Health Serv Res 11(2):141–148. https://doi.org/10.1111/jphs.12333
Passi A, Valenzuela Guiñez F, Margozzini P (2019) Use of medicines in Chile: results of the National Health Survey ENS 2017. Health Statistics - V Chilean Congress of Public Health and VII Chilean Congress of Epidemiology. https://doi.org/10.5867/medwave.2019.S1 (in Spanish).
PautKusturica M, Tomas A, Tomic Z, Bukumiric D, Corac A, Horvat O, Sabo A (2016) Analysis of expired medications in Serbian households. Slovenian J Public Health 55(3):195–201. https://doi.org/10.1515/sjph-2016-0025
Pereira FGF, Sá FHD, Silva RDL, Silva R, Formiga LMF, de Souza EC (2019) Authorreferated knowledge and behavior on disposal of domiciliary medicines. R Pesq-Cuid Fundam Online 11(1):154–159. https://doi.org/10.9789/2175-5361.2019.v11i1.154-159
Pérez FJS, Méndez JLA, Pech-Canché JM, Maldonado CS (2019) Main waste medicines generated in households and their ecotoxicological potential in Tuxpan Veracruz. Acta Universitaria 29:1–12. https://doi.org/10.15174/AU.2019.2398
Pivetta GG, Gastaldini MDC (2019) Presence of emerging contaminants in urban water bodies in southern Brazil. J Water Health 17(2):329–337. https://doi.org/10.2166/wh.2019.092
Rogowska J, Zimmermann A, Muszyńska A, Ratajczyk W, Wolska L (2019) Pharmaceutical household waste practices: preliminary findings from a Case Study in Poland. Environ Manage 64(1):97–106. https://doi.org/10.1007/s00267-019-01174-7
Sandoval MA, Calzadilla W, Vidal J, Brillas E, Salazar-González R (2024) Contaminants of emerging concern: occurrence, analytical techniques, and removal with electrochemical advanced oxidation processes with special emphasis in Latin America. Environ Poll 345:123397. https://doi.org/10.1016/j.envpol.2024.123397
Septianingrum MAN, Yuliastuti F, Hapsari WS (2021) How do people manage of their unused medicines at home? Proceedings of the 2nd Borobudur International Symposium on Humanities and Social Sciences. https://doi.org/10.4108/EAI.18-11-2020.2311761
Shah S, Abbas G, Hanif M, Ali M, Rehman AU, Chand UR, Khurram H (2023) Disposal practices of expired and unused medications among households in Punjab. Pakistan Current Drug Safety 18(2):196–201. https://doi.org/10.2174/1574886317666220513102654
Subsecretaría de Desarrollo Regional y Administrativo de Chile (SUBDERE) (2024) Diagnosis and national cadastre of household solid waste: national synthesis. https://www.subdere.gov.cl/sites/default/files/Sintesis Nacional_Diagnóstico y Catastro Nacional de RSD Marzo_2024_0.pdf (in Spanish). Accessed 26 June 2024
Veiga A, Sousa AC, Sousa C, Oliveira M, Neto B (2023) End-of-life management strategies of pharmaceuticals in Portuguese households. Waste Manage Res 41(1):235–247. https://doi.org/10.1177/0734242X221105416
Wilkinson JL, Boxall ABA, Kolpin DW, Leung KMY, Lai RWS, Galbán-Malagón C, Adell AD, Mondon J, Metian M, Marchant RA, Bouzas-Monroy A, Cuni-Sanchez A, Coors A, Carriquiriborde P, Rojo M, Gordon C, Cara M, Moermond M, Luarte T, Teta C (2022) Pharmaceutical pollution of the world’s rivers. Proc Natl Acad Sci 119(8):e2113947119. https://doi.org/10.1073/pnas.2113947119
Acknowledgements
We are grateful for the support of the expert judges and interviewers who voluntarily made the execution of this study possible. We are also grateful for Ligia de Nazaré Aguiar Silva’s support in editing the maps.
Funding
This work was supported by the National Agency for Research and Development of Chile (ANID)—Subdirección de Capital Humano [Doctorado Nacional/2021–21210126].
Author information
Authors and Affiliations
Contributions
Conceptualization, formal analysis, funding acquisition, investigation, methodology, project administration, and first draft: Juana Angélica Felipe Fernandes. Methodology, resources, supervision, and review: Danilo Carvajal and Adriana C. Mera.
All authors contributed to the study conception and design. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval
The questionnaire and methodology for this study was approved by the Ethical-Scientific Committee of the Universidad de La Serena (CEC-ULS) (ethics approval number: Report 03/2022).
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Consent for publication
Participants signed informed consent regarding publishing their data.
Competing interests
The authors declare no competing interests.
Additional information
Responsible Editor: Philippe Garrigues
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Fernandes, J.A.F., Carvajal, D. & Mera, A.C. The scenario of household pharmaceutical products: consumption, wastes, and disposal practices from a case study in Chile. Environ Sci Pollut Res 31, 51719–51732 (2024). https://doi.org/10.1007/s11356-024-34650-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-024-34650-7