
Abstract
Evidence on the short-term effects of ambient air pollution on chronic obstructive pulmonary disease (COPD) mortality is still not conclusive. The aim of this study was to investigate the relationships between them in Wuhan China. Daily death numbers, concentrations of air pollutants (PM2.5, PM10, SO2, NO2, and O3), and meteorological characteristics in Wuhan from January 1, 2014, to December 31, 2019, were collected. Time-series analysis using generalized additive model was applied. The results showed that a total of 16,150 deaths (7.37 deaths per day) from COPD were observed. The daily average concentrations of PM2.5, PM10, SO2, NO2, and O3 were 59.03, 90.48, 12.91, 48.84, and 91.77 μg/m3, respectively. In single pollutant model, for every increase of 10 μg/m3 in PM10, SO2, and NO2 levels, COPD mortality increased by 0.583% (95% CI: 0.055–1.113%), 4.299% (95% CI: 0.978–7.729%), and 1.816% (95% CI: 0.515–3.313%) at lag03, respectively. No significant associations were found for PM2.5 and O3. Subgroup analysis demonstrated that females were more susceptible to PM2.5, PM10, SO2, and NO2. The concentrations of PM10, SO2, and NO2 were significantly associated with COPD mortality for older adults. The effects of PM2.5 and O3 on COPD mortality were higher in warm period. In two-pollutant models, the significantly positive associations between SO2 and NO2 and COPD mortality remained after adjusting for PM2.5 or O3. In conclusions, short-term exposure to PM10, SO2, and NO2 are significantly associated with a higher risk of COPD mortality. Female or elderly are more susceptible to air pollution. It is urgent to implement the environmental protection policy.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Background
With the rapid development of modern industry and social economy, air pollution has become a common global problem that cannot be neglected in recent years. As a developing country, the magnitude of China is quite different from developed countries. Especially in several megacities, air pollution has become a major threat to public health. In 2010, air pollution is the fourth burden of disease in China, which leads to 1.234 million deaths and 250 million disability adjusted life yeas (DALY) (Yang et al. 2013). Wuhan, as the capital city of Hubei province, has a large population of about 11.21 million. The air pollution is severe because of the drastic urbanization and industrial expansion. During 2013 to 2017, average annual limits of PM10, PM2.5, and NO2 are 1.3~1.8, 1.5~2.7, and 1.2~1.5 times higher than the annual average acceptable limit, respectively (Yassin et al. 2019). Therefore, exploring the associations between ambient air pollution and health in Wuhan is of great importance.
Since the 1990s, numerous evidences have found that short-term exposure to ambient air pollution can increase the risk of adverse health, ranging from sub-health status to death, especially respiratory disorders (Khilnani and Tiwari 2018; Schraufnagel et al. 2019; Guan et al. 2016; Brugha and Grigg 2014). It is accepted that air pollution can disturb the function of respiratory system. Particulate matter may exert oxidative stress on cells in the lung by presenting or by stimulating the cells to produce reactive oxygen species (ROS) and inflammatory factors, and these play important roles in lung tissue injury (Tao et al. 2003; Goldsmith et al. 1997; Ghio and Andrew 1999). Chronic respiratory diseases cause a substantial health-care burden in China, and chronic obstructive pulmonary disease (COPD) is the third most common causes of mortality, with 910,809 deaths in 2013(Yang et al. 2013). Cohort and case crossover studies have shown that ambient air pollution has contributed to increased incidence and prevalence of COPD (Song et al. 2014). Among individuals with COPD, exposure to air pollution is associated with decreased lung function and increased respiratory symptoms (Doiron et al. 2019). The World Health Organization (WHO) estimates that ambient air pollution is responsible for 3.7 million of premature death worldwide in 2012, and 14% of these deaths are due to COPD or acute lower respiratory infections (WHO 2014). It is urgent to further investigate the effects of ambient air pollution exposure on COPD mortality.
Many researches have explored the health effects of air pollution with time-series methods (Astudillo-García et al. 2019; Guo et al. 2017; Katsouyanni et al. 1995; Luo et al. 2020; Mokoena et al. 2019), but few studies specifically measured the association between ambient air pollution and COPD mortality. Evidence on the short-term effects of ambient air pollution on COPD mortality is still not conclusive to date. Furthermore, the characteristics of air pollution in different regions vary substantially. Hence, the aim of this study was to investigate the associations between the concentrations of ambient PM2.5, PM10, SO2, NO2, and O3 and COPD mortality in Wuhan, China.
Methods
Data collection
Death counts between January 1, 2014, and December 31, 2019, were obtained from Mortality Register System in the Wuhan Center for Disease Control and Prevention. For this analysis, we selected the deaths due to COPD, which were classified according to the International Statistical Classification of Disease, 10th Revision codes (ICD-10: J40-J44, I27.9). In view of the vast majority of pulmonary heart diseases (I27.9) caused by chronic bronchitis and emphysema, few were caused by pulmonary embolism, primary pulmonary hypertension, kyphoscoliotic heart disease, and so on; hence, all pulmonary heart diseases were included in COPD. The information of date of death, cause of death, sex, and age was collected. Because the death data were surveillance data, there was no requirement for informed consent. This study was approved by the Ethical Committee of the Wuhan Center for Disease Control and Prevention and was conducted in compliance with the tenets of the Declaration of Helsinki. The results were reported according to the STORBE statement.
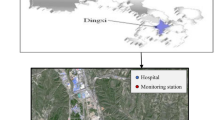
Wuhan is located in central China (29° 58′–31° 22 ′N, 113° 41′–115° 05′ E), with an area of 8569 km2. Ten national air quality monitoring stations have been established. In this study, daily average concentrations of air pollutants including PM2.5 (mass of particles with aerodynamic diameter <2.5 μm), PM10 (mass of particles with aerodynamic diameter <10 μm), SO2 (sulfur dioxide), NO2 (nitrogen dioxide), and O3 (ground-level ozone) during January 1, 2014, to December 31, 2019, were obtained from the Wuhan Ecology and Environmental Bureau.
Daily meteorological data, including daily mean temperature, atmospheric pressure, and relative humidity during the same period, were obtained from the Wuhan Meteorological Administration.
Statistical analysis
Daily COPD mortality, air pollutants, and meteorological data were described as mean, standard deviation (SD), and quartile. Spearman’s correlation was used to estimate the associations between air pollutants and meteorological factors.
For the time-series analysis, daily COPD mortality data was low, belonging to small probability event and approximately followed the Poisson distribution. Therefore, generalized additive Poisson regression with a log-link function was conducted to assess the association between daily counts of COPD mortality and air pollutant concentrations. The model is as below:
In this equation, t refers to the day of the observation; Yt is the observed daily death counts on day t; E(Yt) is the expected daily death count on day t; α is the intercept of the model; β represents the regression coefficient for each air pollutant; Xt is the concentration of air pollutant at day t; Zt represents meteorological data at day t; DOW is the dummy variable for day of the week; Holiday is the dummy variable for day of the holiday; and s is the smoothing spline function for the nonlinear variables such as temperature, humidity, atmospheric pressure, and calendar time. We used the value of Akaike information criterion (AIC) to determine the degrees of freedom (df), and the smaller AIC value indicated the preferred model. Finally, we selected 7 df per year for the time to adjust the time trend and seasonality, and 3 df were used for temperature, humidity, and atmospheric pressure. Regarding the concentrations of air pollutants, we estimated the associations with different lag structures using single lag from the current day up to the previous 5 days (lag0–lag5), as well as moving averages of the current and previous days (lag01–lag05). For meteorological data, the current day measurement was adopted in all lag structures. After the working model was built, the air pollutants were included separately. Subgroup analyses by age (<65, ≥65), sex (males, females), and season (cold period (from May to October), warm period (from November to April)) were also conducted. Elderly was defined as older than 65 years old. Furthermore, we used two-pollutant models for all pollutants without interactions to determine the possible role of single pollutants.
The association between air pollutants and COPD mortality was reported as excess relative risk (ERR) with 95% confidence interval (CI) for 10μg/m3 increase in PM2.5, PM10, SO2, NO2, and O3 concentrations. All statistical analyses were performed using R (version 4.0.2) packages “mgcv” and “nlme.” Statistical significance was defined as a two-tailed P<0.05.
Results
Table 1 presented the descriptive statistics for daily number of COPD death, air pollutants, and meteorological data from January 1, 2014, to December 31, 2019. During the 6-year period, there were 16,150 deaths (7.37 deaths per day) from COPD in Wuhan. Daily death counts were higher in males than in females (4.81 vs. 2.56 deaths per day). 92.28% deaths were elderly, and the daily death count was 6.80. The daily mean concentrations of PM2.5, PM10, SO2, NO2, and O3 were 59.03, 90.48, 12.91, 48.84, and 91.77μg/m3, respectively. And the average of atmospheric pressure, relative humidity, and daily temperature were 1013.10kPa, 79.42%, and 17.18°C.
The daily concentrations of PM2.5, PM10, SO2, and NO2 were strongly and positively correlated with each other, as shown in Table 2. In contrast, the daily concentrations of O3 were moderately and negatively correlated with those of the other pollutants. In addition, air pressure was positive, and temperature was negatively correlated with all air pollutants except for O3 (rhpa-O3=−0.55, P<0.001; rtem-O3=0.68, P<0.001). Relative humidity was negatively correlated with the five air pollutants (P<0.01).
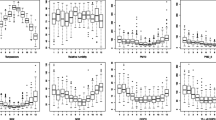
Figure 1 showed the time trends for air pollutants, and all showed relatively stable seasonal trends annually. The concentrations of PM2.5, PM10, SO2, and NO2 had similar characteristics of periodic fluctuation, which were higher in the cold season and lower in the warm season. However, the concentrations of O3 showed an inverse trend. The daily concentrations of PM2.5 and SO2 during 2017 to 2019 were lower than those of previous years. COPD mortality in the study period also showed a seasonal pattern with higher counts in winter and lower counts in summer.

Time-series of PM2.5 (a), PM10 (b), SO2 (c), NO2 (d), and O3 (e) and chronic obstructive pulmonary disease mortality (f) in Wuhan, China, during 2014–2019
Table 3 illustrated the EERs of COPD mortality for every 10μg/m3 increase of air pollutant concentrations with different lag days in single pollutant models. All the five pollutants were positively associated with COPD mortality. However, for the single-day lag effects, positive significant associations were observed only for SO2 at lag1 and lag 2, NO2 at lag 1 and lag2, and O3 at lag 3. The effects of the five pollutants on COPD mortality were highest at lag0 for PM2.5 (ERR: 0.472%, 95% CI: −0.059~1.006), at lag 1 for PM10 (ERR: 0.384%, 95% CI: −0.002~0.771) and SO2 (ERR: 2.958%, 95% CI: 0.665~5.303), at lag 2 for NO2 (ERR: 1.331%, 95% CI: 0.368~2.302), and at lag3 for O3 (ERR: 0.500%, 95% CI: 0.033~0.970). The effects of moving average lags were higher than single lags in different period. For the moving averages, positive significant associations were observed for PM10 at lag02 and lag03, SO2 at lag01–lag03, and NO2 at lag02–lag05. All pollutants showed the strongest estimates at lag03. For each increase of 10μg/m3 in PM2.5, PM10, SO2, NO2, and O3 concentrations, COPD mortality increased by 0.520% (95% CI: −0.217~1.263), 0.583% (95% CI: 0.055~1.113), 4.299% (95% CI: 0.978~7.729), 1.816% (95% CI: 0.515~3.133), and 0.495% (95% CI: −0.226~1.222) at lag03, respectively. The sensitive analysis was conducted by generalized additive Quasi-Poisson regression with a log-link function, and the results did not find great changes in the EERs (supplement Table 1).
The effects of the individual air pollutants on subjects by sex and age were performed in Fig. 2. SO2 had the greatest impact on each subgroup analysis. PM2.5, PM10, SO2, and NO2 estimates of females were higher than those for males, except for PM2.5 at lag5, SO2 at lag 3, and NO2 at lag 1, lag2 as well as lag01–lag03. In contrast, the associations of O3 were higher for males than females. Except for O3, all pollutant estimates of <65 year group was higher than those for older adults, but the estimates of <65 year group were almost nonsignificant (except for PM2.5 at lag2, SO2 at lag2 and lag3, and NO2 at lag3). For older adults, significant positive associations were observed for PM10 at lag1 and lag01–lag03; SO2 at lag1, lag2, as well as lag01–lag03; and NO2 at lag1, lag2, as well as lag02–lag04. As for seasonal effects, the effects of PM2.5 and O3 on COPD mortality were higher in warm period than cold period.

Age-, gender-, and season-specific estimated excess relative risks (ERRs) and 95% confidence intervals (95% CI) for daily deaths from chronic obstructive pulmonary disease with a 10μg/m3 increase in air pollutants using different lag days
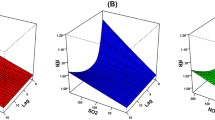
Figure 3 summarized the ERRs for COPD mortality associated with every 10μg/m3 increase of air pollutant concentrations in two pollutant models at lag03. The estimates for SO2 and NO2 were the most stable across all two-pollutant models. In contrast, the estimates of PM2.5, PM10, and O3 decreased after the inclusion of SO2 or NO2. Additionally, the estimates of PM2.5 decreased after the inclusion of PM10. The significant positive associations between SO2 and NO2 and COPD mortality remained after adjusting for PM2.5 or O3.

Estimated excess relative risks (ERRs) and 95% confidence intervals (95% CI) for daily deaths from chronic obstructive pulmonary disease with a 10μg/m3 increase in air pollutants using single- and two-pollutant models. Lag03 were used
Discussion
In our study, a population-based time-series model was used to investigate the associations between short-term air pollutants (PM2.5, PM10, SO2, NO2, and O3) exposure and COPD mortality in Wuhan, China, during January 1, 2014, to December 31, 2019. The results showed that the concentrations of PM10, SO2, and NO2 were significantly positively associated with COPD mortality.
During 2014 to 2019, the levels of ambient air pollution were relatively high in Wuhan, China. The daily mean concentrations of PM2.5 (59.03μg/m3), PM10 (90.48μg/m3), and NO2 (48.84μg/m3) exceeded the values of the WHO Air Quality Guidelines (10, 20, and 40 μg/m3, respectively). And the daily mean concentrations of SO2 and O3 were 12.91 and 91.77μg/m3, which were within the Air Quality Guidelines values (20, 100 μg/m3 respectively). The concentrations of air pollutants showed relatively stable trends. PM2.5, PM10, SO2, and NO2 peaked in winter. It was probable that coal-burning was still the important source of heat and energy in China. Furthermore, in winter, the dispersion of pollutants was poor. However, O3 was mostly formed by the conversion of nitrogen oxides and volatile organic compounds under high temperature, sufficient sunshine, and low humidity, which finally led to the peak values of O3 in summer. By the end of 2019, the number of motor vehicles exceeded 3.3 million in Wuhan, and vehicle emission also became one of the major sources of environmental air pollution.
Our results showed that ambient air pollutants were positively associated with COPD mortality in single pollutant models. The effects on COPD mortality peaked within 4 days (lag03), and the strongest association was observed for SO2. An increase of 10μg/m3 of PM10 was associated with a 0.583% (95% CI: 0.055–1.113%) increase in COPD mortality. Moolgavkar et.al reported a significantly positive association between PM10 and the risk of COPD mortality with an increase of 2.66% (95% CI: 0.12–5.20%) in COPD mortality per 25μg/m3 increase in PM10 (Moolgavkar 2000). And a meta-analysis by Zhu et al. also concluded that a 10μg/m3 increase in PM10 was associated with a 1.1% (95% CI: 0.8–1.4%) increase in COPD mortality (Zhu et al. 2013), while a case-crossover study in Cook city showed a lack of association between PM10 and the risk of death from COPD (Bateson and Schwartz 2004). We did not find significant associations between the concentrations of PM2.5 and COPD mortality, consistent with the results of a large population-based cohort study in Metropolitan Vancouver, Canada (Wen et al. 2013), which speculated that these null associations might reflect the lack of spatial variability of PM2.5 in intraurban study. But a meta-analysis concluded that a 10μg/m3 increase in daily PM2.5 was associated with a 2.5% (95% CI: 1.5–3.5%) increase in COPD mortality (Yang et al. 2016). And in a COPD cohort, Faustini et al. found that effects on respiratory mortality among COPD subjects were particularly elevated 11.6% (95% CI: 2.0–22.2%) from PM2.5 per 11 μg/m3 increase (Faustini et al. 2012). The source of PM2.5 varied in different cities which might be contributed to this inconsistence. The correlations between PM2.5 exposure and COPD mortality should be further confirmed in other cities.
Interestingly, our findings demonstrated that gaseous pollutants had stronger effects on COPD mortality than particulate matter. Similarly, other studies also suggested that compared to particulate matter, gaseous pollutant had stronger effects on COPD exacerbation and daily outpatient visits of respiratory diseases (Cheng et al. 2018; Li et al. 2016). Our estimates showed that a 10μg/m3 increase of NO2 was significantly associated with a 1.816% (95% CI: 0.515–3.133%) increase in COPD mortality. In a 6-year cohort study including all residents aged 51–90 years in Oslo, Norway, the results found that the concentrations of NO2 on COPD mortality appeared to have significantly linear effects (Næss et al. 2007), while Hart et al. found positive but nonsignificant associations of COPD mortality with NO2, PM2.5, and SO2 exposure in industry workers (Hart et al. 2011).
SO2 mainly came from burning of fossil fuels. With the promotion of clean fuels in Wuhan recently, the concentration of SO2 gradually decreased. The mean concentration of SO2 in Wuhan was 12.91μg/m3, which could be considered as low level compared with many other Chinese cities (Guan et al. 2016; Zhang et al. 2019; Zhang et al. 2017). But our results showed that every increase of 10μg/m3 of SO2 was associated with 4.299% (95% CI: 0.978–7.729%) increase in COPD mortality, which was higher than the values reported in several previous studies (Kan and Chen 2003). And Zhang et al. also demonstrated that SO2 had a stronger effect on cardiovascular mortality in Hefei, China (Zhang et al. 2017). The reason for this phenomenon was still unclear, but Samoli et al. found that when the concentration of SO2 is at a lower level, the impact of SO2 to mortality was greater (Samoli et al. 2001), which might partially explain the effects of SO2 in our study. Furthermore, similar with the results of a meta-analysis, we did not find significant associations between the concentrations of O3 and COPD mortality (Li et al. 2016). To sum up, the inconformity with our findings might be due to the different chemical compositions of PM10 or PM2.5 in different areas, which could result in different effects on COPD mortality. In addition, the meteorological factors might influence the effects of air pollutants, but the compositions of air pollutants and meteorological conditions varied in different regions (Jordi and Xavier 2001). Moreover, the age, socioeconomic status and education level, and so on were able to modify the effects of air pollutants.
Although the mechanical explanation of adverse effects of ambient air pollution on COPD mortality remains unclear, identifying the associations of ambient air pollution in different exposure windows is of great importance in the estimation of health risk. In our study, we found that exposure to air pollutants at lag03 yielded the strongest estimates on COPD mortality. Another time-series study in Hefei, China also found the similar phenomenon in the associations between ambient air pollution and cardiovascular mortality (Zhang et al. 2017).
Subgroup analysis showed that females seemed to suffer more risk of COPD mortality from ambient air pollution. In addition, the results showed that the air pollution estimates of <65 year group were higher than those for older adults, though the estimates were almost nonsignificant. Only 7.2% in our study were <65 year group; the sample size might be a strong confounder. A population-based cohort study also showed that the relative risks for COPD mortality associated with a 0.78μg/m3 elevation in black carbon concentrations were 1.06 (95% CI: 0.97–1.15) and 1.08 (95% CI: 0.97–1.20) for males and females and 1.31 (95% CI: 1.07–1.60) and 1.04 (95% CI: 0.97–1.12) for <65 and ≥65 year groups (Wen et al. 2013), similar with the results from a population-based UK Biobank study, which concluded that the adverse effects of PM2.5 and NO2 on COPD prevalence were stronger in females (Doiron et al. 2019). However, Naess et al documented that males were more susceptible to air pollution (PM10, PM2.5, SO2) than females (Næss et al. 2007). The reasons for our gender-specific findings were still unclear and needed further investigation. Furthermore, the concentrations of PM10, SO2, and NO2 were significantly associated with COPD mortality for older adults; effective public health prevention policies specified for older adults should be made to reduce the burden of COPD. Our results also demonstrated that the association between air pollutants and COPD mortality was stronger in the warm period than in cold period, partially consistent with the previous studies (Zhang et al. 2017; Tong et al. 2014). We speculated that the possible reasons of the inconsistence might due to the varied components of air pollutants in Wuhan in different season. In addition, the meteorological factors and pollutants were correlated with each other which might modify the correlation between air pollutants and COPD mortality.
Two-pollutant models were implemented in our study to explore the possible role of single pollutants. We concluded that the estimates of PM2.5, PM10, and O3 decreased after the inclusion of SO2 or NO2, consistent with the previous studies (Zhang et al. 2019; Nhung et al. 2018). These results revealed the relatively independent associations of SO2 and NO2. The associations of SO2 and NO2 on COPD mortality might better reflect the associations between air pollution and COPD mortality in Wuhan compared with other pollutants.
Though this study was a population-based time-series study which covered all population in Wuhan, there were some limitations. Firstly, the average of ten fixed sited monitoring data of air pollutant concentrations were used to infer exposures of individuals, which might lead to potential misclassification exposure and ignore the spatial impact of air pollution on COPD. Secondly, due to data unavailability, some factors including personal social information (such as tobacco use and body mass index) that could affect the effects were not controlled. Hence, we could not rule out the non-relevant death records due to obesity or other reasons than air pollution.
Conclusions
The results of this study suggested that exposure to PM10, SO2, and NO2 was significantly positively associated with a higher risk of COPD mortality in Wuhan, China. Moreover, female and elderly are more susceptible to air pollution. Our findings could provide evidences to help understand the adverse health effects of air pollution, which might have important implications for policy makers to curb and reduce ambient air pollution in Wuhan.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Astudillo-García CI, Rodríguez-Villamizar LA, Cortez-Lugo M, De La Cruz C, Fernández-Nio JA (2019) Air pollution and suicide in Mexico City: a time series analysis, 2000–2016. Int J Environ Res Public Health 16:2971
Bateson TF, Schwartz J (2004) Who is sensitive to the effects of particulate air pollution on mortality? A case-crossover analysis of effect modifiers. Epidemiology 15:143–149
Brugha R, Grigg J (2014) Urban air pollution and respiratory infections. Paediatr Respir Rev 15:194–199
Cheng Y, Tatiana E, Cao GY, Zheng X (2018) Health impacts of exposure to gaseous pollutants and particulate matter in Beijing—a non-linear analysis based on the new evidence. Int J Environ Res Public Health 15:1969
Doiron D, De Hoogh K, Probsthensch N, Fortier I, Cai Y, De Matteis S, Hansell AL (2019) Air pollution, lung function and COPD: results from the population-based UK Biobank study. Eur Respir J 54:1802140
Faustini A, Stafoggia M, Cappai G, Forastiere F (2012) Short-term effects of air pollution in a cohort of patients with chronic obstructive pulmonary disease. Epidemiology 24:177
Ghio, Andrew J (1999) Metals associated with both the water-soluble and insoluble fractions of an ambient air pollution particle catalyze an oxidative stress. Inhal Toxicol 11:37–49
Goldsmith CA, Frevert C, Imrich A, Sioutas C, Kobzik L (1997) Alveolar macrophage interaction with air pollution particulates. Environ Health Perspectives 105:1191–1195
Guan WJ, Zheng XY, Chung KF, Zhong NS (2016) Impact of air pollution on the burden of chronic respiratory diseases in China: time for urgent action. Lancet 388:1939–1951
Guo Y, Ma Y, Zhang Y, Huang S, Wu Y, Yu S, Zou F, Cheng J (2017) ‘Time series analysis of ambient air pollution effects on daily mortality. Environ Sci Pollut Res
Hart JE, Garshick E, Dockery DW, Smith TJ, Ryan L, Laden F (2011) Long-term ambient multipollutant exposures and mortality. Am J Respir Crit Care Med 183:73–78
Jordi S, Xavier B (2001) Particles, and not gases, are associated with the risk of death in patients with chronic obstructive pulmonary disease’. Int J Epidemiol 30:1138–1140
Kan H, Chen B (2003) A case-crossover analysis of air pollution and daily mortality in Shanghai. J Occup Health 45:119–124
Katsouyanni K, Zmirou D, Spix C, Sunyer J, Vigotti MA (1995) Short-term effects of air pollution on health: a European approach using epidemiological time-series data. The APHEA project: background, objectives, design. Eur Respir J 8:1030–1038
Khilnani GC, Tiwari P (2018) Air pollution in India and related adverse respiratory health effects: past, present, and future directions. Curr Opinion Pulmonary Med 24:1
Li J, Sun S, Tang R, Qiu H, Huang Q, Tonya M, Tian L (2016) Major air pollutants and risk of COPD exacerbations: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis 11:3079–3091
Luo L, Dai Y, Zhang F, Chen M, Chen F, Fang Q (2020) Time series analysis of ambient air pollution effects on dynamic stroke mortality. Int J Health Plann Manag 35:79–103
Mokoena KK, Ethan CJ, Yu Y, Shale K, Liu F (2019) Ambient air pollution and respiratory mortality in Xi’an, China: a time-series analysis. Respir Res 20:139
Moolgavkar SH (2000) Air pollution and daily mortality in three U.S. counties. Environ Health Perspect 108:777–784
Næss Ø, Nafstad P, Aamodt G, Claussen B, Rosland P (2007) Relation between concentration of air pollution and cause-specific mortality: four-year exposures to nitrogen dioxide and particulate matter pollutants in 470 neighborhoods in Oslo, Norway. Am J Epidemiol 165:435–443
Nhung NTT, Schindler C, Dien TM, Probst-Hensch N, Perez L, Kuenzli N (2018) Acute effects of ambient air pollution on lower respiratory infections in Hanoi children: an eight-year time series study. Environ Int 110:139–148
Samoli E, Schwartz J, Wojtyniak B, Touloumi G, Spix C, Balducci F, Medina S, Rossi G, Sunyer J, Bacharova L (2001) Investigating regional differences in short-term effects of air pollution on daily mortality in the APHEA project: a sensitivity analysis for controlling long-term trends and seasonality. Environ Health Perspect 109:349–353
Schraufnagel DE, Balmes JR, De Matteis S, Hoffman B, Wuebbles DJ (2019) Health benefits of air pollution reduction. Ann Am Thoracic Soc 16:1478–1487
Song Q, David C, Wang X, Ren J (2014) The global contribution of outdoor air pollution to the incidence, prevalence, mortality and hospital admission for chronic obstructive pulmonary disease: a systematic review and meta-analysis. Int J Environ Res Public Health 11:11822–11832
Tao F, Gonzalez-Flecha B, Kobzik L (2003) Reactive oxygen species in pulmonary inflammation by ambient particulates. Free Radical Biol Med 35:327–340
Tong L, Li K, Zhou Q (2014) Promoted relationship of cardiovascular morbidity with air pollutants in a typical Chinese urban area. PLoS One 9:e108076
Wen QG, Mark Fitzgerald J, Carlsten C, Sadatsafavi M, Brauer M (2013) Associations of ambient air pollution with chronic obstructive pulmonary disease hospitalization and mortality. Am J Respir Crit Care Med 187:721–727
WHO. 2014. ‘WHO fact sheet on ambient (outdoor) air quality guidelines: includes key facts, definition, health effects, guideline values and WHO response’.
Yang G, Yu W, Zeng Y, Gao GF, Liang X, Zhou M, Wan X, Yu S, Jiang Y, Naghavi M (2013) Rapid health transition in China, 1990-2010: findings from the Global Burden of Disease Study 2010. Lancet 381:1987–2015
Yang J-W, Fan L-C, Xu J-F, Cao W-J, Choi A (2016) ‘Short-term exposure to ambient fine particulate matter increases hospitalizations and mortality in COPD a systematic review and meta-analysis. Chest. 149(2):447–445
Yassin M, Jun Q, Zhengxuan Y, Fatuma N, Xiang Z (2019) Boundary layer perspective assessment of air pollution status in Wuhan city from 2013 to 2017. Environ Monit Assess 191(2):69
Zhang C, Ding R, Xiao C, Xu Y, Cheng H, Zhu F, Lei R, Di D, Zhao Q, Cao J (2017) Association between air pollution and cardiovascular mortality in Hefei, China: a time-series analysis. Environ Pollut 229:790
Zhang, Wang J, Cao H, Sun D, Qi Z, Guo C, Peng W, Sun Y, Xie Y, Liu X, Li B, Luo Y, Pan Y, Li Y, Zhang L (2019) Associations between ambient air pollution and mortality from all causes, pneumonia, and congenital heart diseases among children aged under 5 years in Beijing, China: a population-based time series study. Environ Res 176:108531–108531
Zhu R, Chen Y, Wu S, Deng F, Yao W (2013) The relationship between particulate matter (PM10) and hospitalizations and mortality of chronic obstructive pulmonary disease: a meta-analysis. COPD 10:307–315
Funding
This research was funded by the Basic Applied Research Project of Wuhan Science and Technology Bureau (grant number: 2015061701011631), Emergency Research Fund for Novel Coronavirus Pneumonia Prevention and Control of Wuhan Municipal Health Commission (grant number: EG20A04), Scientific Research Project of Hubei Provincial Health and Family Planning Commission (grant number: WJ2019F011), and Scientific Research Program of Hubei Education Department (grant number: B2020006). The funds of the study had no role in the study design, execution, analysis, data interpretation or writing of the report.
Author information
Authors and Affiliations
Contributions
YY: conceptualization, methodology, and funding acquisition. LS: formal analysis and writing–original draft preparation. YG: software and funding acquisition. YZ: data curation. PZ: software. BX: validation. JZ: data curation. MY: writing (reviewing and editing), conceptualization, and funding acquisition. LW: conceptualization. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The death data were surveillance data; there was no requirement for informed consent. This study was approved by the Ethical Committee of the Wuhan Center for Disease Control and Prevention.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Responsible editor: Lotfi Aleya
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
ESM 1
(DOCX 15 kb)
Rights and permissions
About this article

Cite this article
Yan, Y., She, L., Guo, Y. et al. Association between ambient air pollution and mortality from chronic obstructive pulmonary disease in Wuhan, China: a population-based time-series study. Environ Sci Pollut Res 28, 33698–33706 (2021). https://doi.org/10.1007/s11356-021-13180-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-021-13180-6