
Abstract
Hypertension, a major risk factor of many severe chronic diseases and leading cause of global disease burden, is reported to be associated with long-term exposure to PM2.5. China’s high PM2.5 pollution level has become a major public health issue. However, existing studies from China have got inconsistent results with very limited investigation into the multi-ethnic peoples. This study adds multi-ethnic evidence from Sichuan Province, southwestern China, and assesses ethnic differences of PM2.5 exposure effect on hypertension. We pooled large cross-sectional data from two surveys conducted in 2013 and 2018 to examine the association of long-term exposure to PM2.5 on prevalence of hypertension in adults aged 30 years old and above. Community-specified annual PM2.5 concentration was estimated using satellite data. Thirty-one thousand four hundred sixty-two participants with average exposure concentration of 32.8 μg/m3 were included. The proportions of the Han, the Tibetan, the Yi, and other ethnic people were 89.2%, 7.3%, 3.2%, and 0.3%, respectively. The adjusted odds ratio (OR) was 1.08 (95% CI, 1.04–1.12) for a 10 μg/m3 PM2.5 concentration increment. The adjusted ORs for the Han, the Tibetan, and the Yi were 1.08 (95% CI, 1.04–1.12), 0.03 (95% CI, 0.00–0.27), and 1.75 (95% CI, 1.28–2.38) for a 10 μg/m3 PM2.5 concentration increment, respectively. Stratification analysis found stronger associations in participants with chronic diseases and Yi minority population. The results showed that long-term exposure to PM2.5 may increase the risk of hypertension prevalence in Chinese multi-ethnic adults. The associations were different among ethnicities.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
High blood pressure and hypertension are recognized as the risk factors for many severe non-communicable diseases including cardiovascular disease, stroke, and kidney cancer (Benjamin et al. 2019). In 2017, high systolic blood pressure (SBP) was reported to be the first leading cause of global disease burden, accounting for 11.4 million deaths and 218 million disability-adjusted life years (DALYs) (Stanaway et al. 2018). The prevalence of hypertension in China has increased with the development of economy and aging of the population (Wang et al. 2018). In parallel, poor ambient air quality in China has become a serious public health issue. Previous studies have found that both short-term and long-term exposures to fine particulate matter (PM2.5) are associated with elevations in blood pressure. Short-term effect of PM2.5 was considered as a trigger of health events that occur within hours to days after exposure, while long-term effect would increase risk of health events over the long term after months to years of exposure (Brook et al. 2010). Compared to short-term exposure, long-term exposure seems to have stronger effects on high blood pressure and hypertension (Bai et al. 2018; Honda et al. 2018; Huang et al. 2019; Huang et al. 2018; Lin et al. 2017; Liu et al. 2017; Yang et al. 2018a).
However, the evidence from epidemiology study on the long-term effect of PM2.5 on hypertension remains inconsistent. Several recent studies suggested that long-term exposure of higher PM2.5 concentration was related to increased prevalence of hypertension (Bai et al. 2018; Honda et al. 2018; Huang et al. 2019; Lin et al. 2017; Liu et al. 2017) and that improvement of PM2.5 exposure was associated with a decreased incidence of hypertension (Sigaux et al. 2019), while other studies reported no significant association between long exposure of PM2.5 and hypertension (Adar et al. 2018; Zhang et al. 2019b). Variations in subject characteristics, geographical settings, pollutant sources and compositions, measurement of exposure, etc. may be responsible for the inconsistency. Thus, further study on diverse population is needed.
Striking ethnic/racial differences in abnormal blood pressure or other related adverse cardiovascular outcomes attributed to PM2.5 exposure have been reported, but the results were inconclusive. A study of 132,224 adults based on the USA 1995-2005 National Health Interview Survey showed that PM2.5 was positively associated with prevalent self-reported hypertension (OR of 1.05 for a 10 μg/m3 increase). This association varied from different race/ethnicity which was statistically significant in the White but not the Black or the Hispanic (Johnson and Parker 2009). But another American multi-ethnic (MESA) cohort study found that the Black showed stronger association than the White even after adjustment for socioeconomic status (SES) (Hicken et al. 2016).
Ethnicity/race is a synthetic index which can reflect accumulative information of multiple social and health-related factors. Researchers have noted that examining the cumulative effects of numerous factors is vital when investigating vulnerability to environmental health issues (Hicken et al. 2011). Ethnicity/race could be treated as a surrogate of a cluster of unmeasured confounders including genetic heterogeneity and cultural or religious differences. However, the relationship among long-term exposure, ethnicity/race, and hypertension is complicated. Ethnicity/race has interaction with many social, psychosocial, and environmental factors. In the USA and Europe, minority neighborhood tends to be exposed to heavier air pollution, indicating that ethnic/racial difference may result from residential segregation (Fairburn et al. 2019; Hicken et al. 2016; Jones et al. 2015). Meanwhile, racial segregations are often lower-income communities in which minority groups are often with lower SES and suffer higher levels of noise, poverty, and other stressors. This cluster of social, psychosocial, and environmental disadvantages would lead to poor health outcomes (Clougherty and Kubzansky 2009). As a result, it is particularly important to disentangle the combined effect of ethnicity/race, other social/ psychosocial factors, and environmental exposure, and identify modifiable exposures so as to understand how to best protect susceptible populations and improve overall population health (Clougherty and Kubzansky 2009).
Although studies based on Chinese population were conducted, the evidence from multi-ethnic population was limited. Most related studies conducted in China did not consider the ethnicity of subjects (Huang et al. 2019; Lin et al. 2017; Liu et al. 2017; Zhang et al. 2018a) or loosely divided subject into Han and non-Han groups (Yang et al. 2017). However, different ethnic groups have their own customs, culture, living habits, and geographic contexts. If combining all the minority groups together, the accuracy of study results would surely be lowered. Health inequality in relation to China’s disproportionate air pollution distribution has started to draw academic attention, and their studies reported that socioeconomic factors such as urbanization, health recourse, and house consumption could have impacts on both the health inequality and disproportionate air pollution distribution (Azimi et al. 2019; Zhao et al. 2019). Those studies were based on provincial level rather than individual level, so their results could be quite limited when exploring how social and environmental factors are related to ethnic/racial disparity from an individual perspective. Different from Western countries, China’s ethnic/racial minority groups generally live in low PM2.5 pollution areas but some of the groups are with high prevalence of hypertension (Yan Suijun 2017). In western China, the Tibetan and the Yi are two major ethnic minority groups. Compared with Han group, most of Tibetan and Yi groups live in rural areas and tend to be of lower education attainment and poorer economic level (Morales 2019). In addition, the main domestic fuel of rural areas is solid fuel including coal and biomass, which could create serious indoor air pollution and expose people to high health risks (Stanaway et al. 2018).
From the above discussion, this study aims to (1) evaluate the association between long-term exposure of PM2.5 and hypertension in an multi-ethnic population; (2) evaluate whether the association between PM2.5 exposure and hypertension are modified by social and psychosocial determinants of health, including ethnicity, SES (education, income), and health-related factors (comorbidity, anxiety/depression); (3) detect the potential causes of ethnic differences by exploring the interaction of ethnicity and other social and environmental factors. The results may shed clues on the ethnic disparity of long-term PM2.5 exposure effect on hypertension and provide knowledge for identifying vulnerable populations and targeting intervention measurements from an ethnic perspective.
Methods
Study area
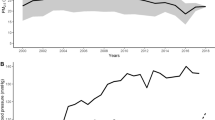
Sichuan Province is located in southwest China ranging from 26° 30′ to 34° 190′ N and from 97° 300′ to 108° 310′ E. Of its area, 73.56% is covered with mountains, of which an average height is over 5000 m above the sea level. This is a province surrounded by highlands and mountains, including Tibetan Plateau, Yunnan-Guizhou Plateau, Daba Mountains, and Wu Mountains (Kuang et al. 2016; Yearbook 2018). Its complex and unique geographic characteristics block pollutant diffusion, which leads to a gradient spatial PM2.5 distribution with the maximum in Sichuan Basin and the minimum in its northwest region (Xiong et al. 2019). Sichuan Basin, the eastern part of Sichuan Province, is one of the highest PM2.5 concentration regions in China. The annual average PM2.5 concentrations in Sichuan Basin during 2004 and 2013 are generally ≥ 85 μg/m3 (Ma et al. 2016). Because of the severe PM2.5 pollution, the government has taken a series of measures to prevent and control PM2.5 and its precursors (Li 2014). Nevertheless, PM2.5 remains the major pollutant which plays a dominant role in Sichuan region (Feng et al. 2019).
Sichuan is the home for about 5 million ethnic minority population (Statistics 2012). Yi (2.6 million), Tibetan (1.5 million), and Qiang (0.3 million) ethnic groups account for the majority (Zhang et al. 2019a). Their SESs, lifestyles and living conditions vary greatly. Sichuan is also a province with unbalanced social and economic developments. There is not only a megacity (the capital of Sichuan Province, Chengdu) but also remote rural areas with three minority autonomous prefectures (Liangshan Yi Autonomous Prefecture, Aba Tibetan Autonomous Prefecture, and Ganzi Tibetan Autonomous Prefecture). These conditions may exert a non-negligible effect on the association between PM2.5 exposure and hypertension prevalence, but related evidence from Sichuan Province and southwest China is hardly sufficient.
Data
The research data came from the Fifth and Sixth Health Services Surveys (HSSs) conducted in Sichuan Province in 2013 and 2018 which were part of National Health Services Surveys (NHSSs). NHSS is a regular survey implemented by national and local governments every 5 years. The purpose of NHSS is to understand the health status of the population, their needs and demands for healthcare services, and the utilization and costs of healthcare services in a systematic fashion. A multi-stage stratified random cluster sampling method had been adopted to draw 14 urban districts/rural counties randomly in Sichuan Province. In each district/county, 5 subdistricts/townships were randomly selected. In each subdistrict/township, 2 communities/villages were randomly selected. And in each community/village, 60 households were randomly selected. The sampling designs of the Fifth and Sixth HSS were the same, but Litang was replaced by Danba in 2018. Therefore, 15 districts/counties were included in this study.
Among the 15 districts/counties, there were 3 ethnic minority counties according to Chinese Government’s categorization (Statistics 2018): two Tibetan counties (Litang and Daba) and one Yi county (Yanyuan). The rest 12 were Han districts/counties.
The Fifth and Sixth HSS participants totaled 22,795 and 21,047. This study combined both survey data for analysis to detect the effect differences among Han, Tibetan, and Yi ethnic groups. Subjects aged 30 years and older were included.
Hypertension
Participants with at least one of the following characteristics were considered to be of hypertension: (1) being physician-diagnosed with hypertension within 6 months prior to the survey; (2) being physician-diagnosed with hypertension over 6 months prior to survey and having taken measures to control blood pressure within 6 months prior to survey.
Air pollution
Outdoor PM2.5 concentrations from 2008 to 2016 were estimated with the geographically weighted regression model developed by van Donkelaar et al. (2016). This model combined satellite-derived aerosol optical depth (AOD) data and surface monitor data, and conducted simulations with GEOS-Chem chemical transport model to provide a long-term average ambient PM2.5 concentration at around 1 km × 1 km resolution with R2 of 81%.
Outdoor PM2.5 concentrations in 2017 were estimated with Bayesian spatial model developed by Zhang et al. (the article is being submitted). Based on satellite-derived aerosol optical depth (AOD) data and surface monitor data, this model conducted simulations with hierarchical Bayesian approaches to estimate PM2.5 at 1 km × 1 km resolution. R2 and root mean squared error (RMSE) of 10-fold cross validation for the model were 87% and 1.167.
Community/village locations were geocoded with Google Earth. Estimated annual ambient PM2.5 concentrations were mapped to participants in the corresponding communities/villages.
The annual average PM2.5 concentrations for each location from 2008 to 2012 (the Fifth HSS) and from 2013 to 2017 (the Sixth HSS) were used as the estimated surrogate of exposure.
Covariates
Face-to-face interviews with paper (used in 2013) or electronic (used in 2018) questionnaires were applied to collect participants’ demographic, socioeconomic, and lifestyle information, such as age, sex, ethnicity, residence, marital status, education, annual household income, body mass index (BMI), smoking status, drinking status, and physical activity. Questionnaire structures of the Fifth HSS and the Sixth HSS were basically the same, but some items have been modified or deleted. The item about ethnicity in 2013 national questionnaires did not include the option of “Yi” as 2018 did. “Yi” was included into the option of “Others” in 2013. However, 2018 data showed that over 94% (675/717) of the people who chose “Others” belonged to the Yi minority group. On-site investigation experience also verified that the Yi accounted for most of the “Others.” Thus, “Others” in ethnic options from the 2013 questionnaire was coarsely treated as “Yi” in this study. The item about domestic fuel type was deleted in the questionnaire of 2018.
In this study, ethnicity options were organized into four categories: Han, Tibetan, Yi and Others.
BMI was divided into four categories: underweight (< 19.5 kg/m2), normal weight (19.5 kg/m2 ≤ BMI < 24.0 kg/m2), overweight (24.0 kg/m2 ≤ BMI < 28.0 kg/m2), and obesity (≥ 28.0 kg/m2) according to China’s weight criteria (National Health and Family Planning Commission 2013). EQ-5D-3L was used to collect information about health-related quality of life. Anxiety/depression symptom and visual analogue scale (VAS) were part of EQ-5D-3L. Anxiety/depression symptoms were divided into 3 levels as “not at all,” “moderate,” and “severe.” VAS ranged continuously from 0 to 100. Comorbidity was examined by a dyadic measure (“having other chronic diseases except hypertension” or “having no other chronic diseases except hypertension”).
Education status was categorized as “no formal education,” “primary school,” “middle school,” and “high school or above.” Per capital annual household income was divided in five categories by quintile (Q1: < 4444 RMB; Q2: 4444 RMB ≤ per capital household income < 7433 RMB; Q3: 7433 RMB ≤ per capital household income < 11,100 RMB; Q4: 11,100 RMB ≤ per capital household income < 18,750 RMB; Q5: ≥ 18,750 RMB).
Average annual salt sales volume of each district/county for 5 years preceding the survey and the population of each district/county were collected from Sichuan Provincial Statistics Yearbook, and then per capital annual salt sales volume was calculated by averaging annual salt sales volume per person in kg.
Statistical analysis
After univariate variable analyses, multivariate logistic regression models were fit to control potential confounding factors, including basic characteristics (age, sex, and ethnicity), health-related factors (BMI, anxiety/depression, comorbidity VAS, and per capital annual salt sales of each district/county), SES index (education status, per capital annual household income). The missing data was excluded as less than 5%.
Stratified analyses were conducted to examine whether the association between long-term exposure of PM2.5 and hypertension prevalence could be modified by age (< 60 and ≥ 60), sex (male and female), BMI (normal, overweight and obesity), comorbidity (yes and no), and ethnicity (Han, Tibetan, Yi).
Based on the results of stratified analyses by ethnicity, the potential causes of ethnic disparity were further explored. In this study, the 12 Han districts/counties together were regarded as Han area, 2 Tibetan counties as Tibetan area, and 1 Yi county as Yi area. It was assumed that environmental/social characteristics of the Han and minority groups who live in same area were similar. To control unobserved environmental/social factors, the different effects on the Han and minority groups were analyzed based on population who reside in the same Han, Tibetan, and Yi area, respectively. As few minority people reside in Han area, only population in Tibetan area and Yi area were taken into analysis in terms of ethnicity. In our sampled sites, Yi area had only one county (Yanyuan County) where the range of PM2.5 concentration is too narrow to test any association. As survey results indicated, except those from Yanyuan County, around 90% of the rest Yi people were from Xi District; this district is close to Yanyuan County and with a large number of Yi people, was included into the original Yi area.
Furthermore, previous studies suggested that domestic fuel type could modify the effect of ambient PM2.5 (Lin et al. 2017). Since clean domestic fuel was disproportionately distributed by ethnicity, it can be one of important factors in relation to ethnic differences. For no domestic fuel type data was collected in 2018, the synergy effect of ambient PM2.5 exposure and indoor fuel type was examined only based on the data of 2013.
Sensitivity analyses were performed. First, the association was tested using different measures of exposure, average PM2.5 concentrations for 1–4 years before the survey. Second, the association was tested after adjustment of residence location (urban or rural area) and survey year. Third, the association was tested by using the Fifth and Sixth HSS data separately. Finally, due to the familial clustering of hypertension prevalence, two-level logistic regression (individual-level and family-level) was applied to decompose the family-level variation.
Data analyses were conducted using R 3.5.3. P value < 0.05 to determine statistical significance.
Results
PM2.5 concentration and hypertension prevalence distribution
A total of 31,462 participants were included with hypertension prevalence of 15.7%. Twenty-eight thousand fifty participants were Han, 2288 participants were Tibetan, 1013 participants were Yi, and 111 participants belonged to other ethnic groups. The average age of participants was 55.6 years old with an annual mean PM2.5 exposure concentration of 32.8 μg/m3. Detailed PM2.5 exposure concentrations are listed in Table S1. Qingyang District, one the five main urban districts of the capital of Sichuan Province, was the most polluted area with average PM2.5 concentration of 55.3 μg/m3, which was also with highest hypertension prevalence of 23.7%. A low level of PM2.5 concentration was observed in minority sample sites. The average exposure concentration in Yanyuan County of Yi Autonomous Prefecture was 9.8 μg/m3. The concentrations of those two Tibetan counties were even lower. In Tibetan area, the concentrations of Danba and Litang were 5.3 μg/m3 and 2.4 μg/m3, respectively. The prevalence of hypertension in those three minority counties was also relatively low (Yanyuan County 5.6%; Danba County 13.8%; Litang County 15.9%). In general, PM2.5 concentration and hypertension prevalence of each sample district/county was positively related with a correlation coefficient of 0.54 (P = 0.04). PM2.5 exposure and hypertension prevalence distribution at a district/county level is shown in Fig. 1.

The PM2.5 concentration and prevalence of sample districts/counties
Basic characteristics of participants
Grouped by hypertension and non-hypertension (reference), basic characteristics of participants are presented in Table 1. The hypertension participants were older than the non-hypertension participants (65.4 years versus 53.7 years) and they were exposed to higher ambient PM2.5 (34.5 μg/m3 versus 32.5 μg/m3). Compared with the non-hypertension group, the urban residents and the Han population accounted for a higher proportion in hypertension group. The hypertension patients were more likely to be overweight (32.21% versus 23.46%) and obese (10.09% versus 4.89%), and they were more likely to have symptoms of anxiety/depression (19.31% versus 12.25% for moderate; 2.00% versus 1.17% for severe). Among hypertension patients, 59.9% took health checkup in the previous year, far exceeding non-hypertension people (45.6%). As for health-related behaviors, hypertension participants were less likely to brush teeth every day (81.20% versus 85.60%), smoke (20.86% versus 29.24%), and drink alcohol (18.33% versus 26.15%); on the contrast, they were more likely to do physical activities (41.97% versus 31.88%). The hypertension patients had a higher income than non-hypertension subjects (45.67% versus 42.35% for income > quantile 60).
Table 2 shows the results of comparison of sociodemographic and major risk factors among different ethnicities. The average annual PM2.5 concentrations of the Han, Yi, and Tibetan people were 35.9 μg/m3, 11.9 μg/m3, and 3.9 μg/m3, respectively (P < 0.0001). Distribution of PM2.5 concentrations for different ethnic groups is shown in Fig. 2. SES of the Han was higher than the other two minority groups. Yi minority group was of lowest SES among the three ethnic groups. Over 80% of Yi people had only primary school education attainment and per capital household income of over 50% Yi participants ranked below the 40th percentile of all participants. Besides, Yi minority group had a relatively higher proportion with adverse health-related behaviors like smoking, while a lower proportion with beneficial health-related behaviors like physical activities and health check.

Distribution of PM2.5 concentrations for the Han, Yi, and Tibetan people
The results of multivariate regression analysis
Table 3 shows the results of associations between PM2.5 and hypertension. In crude model, higher PM2.5 concentration was associated with increasing risk of hypertension with a crude odds ratio (OR) of 1.11 (95% CI, 1.09–1.14) for a PM2.5 increment of 10 μg/m3. After fully adjusted for covariates (model 4 in Table 3), the positive association remained statistically significant (OR 1.08; 95% CI, 1.04–1.12). Results of the fully adjusted model are listed in Table S2.
Stratified analyses
The associations between PM2.5 exposure and hypertension stratified by sex, age, BMI, ethnicity, and comorbidity are shown in Fig. 3. The ORs of hypertension with a 10 μg/m3 increment were significantly higher among comorbid participants (OR 1.18; 95% CI, 1.12–1.25) and Yi minority group (OR 1.75; 95% CI, 1.28–2.38). The detailed results of stratified analyses are listed in Table S3.

The results of estimated ORs of exposure to PM2.5 and hypertension based on stratified analysis
Analyses of ethnic disparity between Han and Yi population
Based on the above analysis results, Yi minority people were exposed to lower PM2.5 concentrations (Han, 35.9 μg/m3; Yi, 11.9 μg/m3) but suffered a stronger adverse effect on hypertension (OR for Han, 1.08; OR for Yi, 1.75) when compared to Han people. To detect whether the differences between Han and Yi populations were attributed to their heterogeneous responses to PM2.5 exposure or other socioeconomic/environmental factors, corresponding analysis was conducted based on 4571 participants (including 3581 Han people and 990 Yi people) in Yi area. Positive association between PM2.5 exposure and hypertension persisted and the interaction term between PM2.5 exposure and Yi minority group was not statistically significant. The results are shown in Table 4.
To further explore potential factors related to ethnic disparity, whether domestic fuel type had synergy effect on ambient PM2.5 exposure was tested using the data of 2013. Yi people were more likely to use unclean fuel type than their Han counterpart (76.1% versus 43.7%, P < 0.001) as shown in Table 5. The interaction term between ambient PM2.5 exposure and clean fuel type was not statistically significant. But the addition of interaction term tremendously changed the coefficient of PM2.5 exposure. The results are shown in Table 6.
Sensitivity analyses
Sensitivity analyses generated similar results that increasing PM2.5 concentration exposure was related to higher risk of hypertension. The results of sensitivity analyses are shown in Table S3.
Discussion
In China, differences in health effects of long-term air pollution exposure among subgroups defined by race/ethnicity have not been examined, nor have potential synergies of ethnicity clustered social, psychosocial, and environmental factors been disentangled. This is the first study to examine the effects of long-term exposure to PM2.5 and the prevalence of hypertension among Han, Tibetan, and Yi populations in China. It was found that higher long-term exposure to PM2.5 was associated with increased risk of hypertension in a multi-ethnic population. Comorbidity and ethnicity modify the effect of long-term PM2.5 exposure on the prevalence of hypertension. Comorbidity would intensify the effect. Compared with Han population, the association is stronger in the Yi population.
This study focuses on the relationship between long-term exposure to PM2.5 and the prevalence of hypertension. Five-year average PM2.5 concentrations are used to measure long-term exposure because the NHSS is conducted every 5 years. Hypertension is a chronic disease caused by the long-term effects of environmental and genetic factors. Sensitivity analyses provided similar results when using different exposure windows, which is consistent with the findings of Lin et al. (Lin et al. 2017). The effects of short-term exposure of PM2.5 on blood pressure are minor and can be easily reversed as the exposure is removed (Wu et al. 2017). Moreover, there are many other factors that can sway blood pressure. Therefore, the relationship between long-term exposure to PM2.5 and hypertension is more stable, so that effects of exposure are relatively certain.
The possible biological mechanism by which PM2.5 exposure affects hypertension involves systemic inflammation and oxidative responses (Brook et al. 2009; Zhang et al. 2018b). PM2.5 could elicit systemic oxidative stress and inflammation, thus increasing the circulation of activated immune cells and inflammatory cytokines. Consequently, vascular endothelial dysfunction could lead to an imbalance in vascular homeostatic responses (Brook and Rajagopalan 2009). PM2.5 also affects blood pressure by altering autonomic nervous system balance and activating the hypothalamus–pituitary–adrenal axis (Brook et al. 2009; Kodavanti 2016).
Positive associations between long-term exposure to PM2.5 and hypertension are inconsistent in existing epidemiologic studies. In this study, positive associations were obtained, consistently with several previous studies. A Canadian population-based cohort exhibited a 3% increase in incident hypertension associated with a 2.1 μg/m3 increase in PM2.5 (Bai et al. 2018). An observational study on older Americans found that a 3.91 μg/m3 increase in PM2.5 was strongly associated with increased prevalence of hypertension with an OR of 1.24 (Honda et al. 2018). A China’s cohort study reported that a PM2.5 concentration increment of 10 μg/m3 could increase the risk of hypertension by 11% (Huang et al. 2019). Another Chinese cross-sectional study among older adults reported that the OR of hypertension was 1.14 with a PM2.5 concentration increment of 10 μg/m3 (Lin et al. 2017). A Chinese nationwide cross-sectional study of middle-aged and elderly people reported a weaker association (41.7 μg/m3 increase in PM2.5) was associated with a higher prevalence of hypertension (OR = 1.11) (Liu et al. 2017). However, an American multi-ethnic cohort study found no association between long-term exposure to PM2.5 and blood pressure (Adar et al. 2018). A recent Chinese cross-sectional study also found a non-significant association (Zhang et al. 2019b). The inconsistency may be partially explained by the heterogeneity in study designs, study settings, constituents of particle matter, exposure assessments, population characteristics, and covariates included in models (Yearbook 2018).
Ethnicity has a complicated modification effect on the association between long-term PM2.5 exposure and hypertension. The association in the Tibetan group is negative, which is mostly due to their low exposure level, very close to the lower bound of the theoretical threshold of ambient PM2.5 concentration (2.4–5.9 μg/m3) (Stanaway et al. 2018). Meanwhile, Tibetans are reported to have a high prevalence of hypertension (Yan Suijun 2017). A high salt diet, residence at high elevation, and related genetic adaptation are recognized as major risks (Narvaez-Guerra et al. 2018; Shaopeng 2010; Yan Suijun 2017; Zhou et al. 2013) which may outweigh the effect of air pollution.
A stronger association is observed in the Yi population. The analysis for the in Yi area showed that the interaction of PM2.5 exposure and ethnicity was no longer statistically significant, indicating that the ethnic differences in hypertension prevalence are mainly caused by socioeconomic and environmental factors. Although the average age of Yi participants tends to be younger than that of the Han group, their education attainment and income level are likely to be lower than those of Han people. Compared with Han people, the Yi minority are less likely to have symptoms of anxiety/depression and comorbidity. Meanwhile, the health-related behaviors of the Yi minority people are poorer than those of the Han group. Yi people are more likely to smoke and less likely to engage in physical activities and brush their teeth every day. Except for the individual factors, the Yi area is less developed than the Han area both in economy and healthcare services (Zhang et al. 2019a). The findings of this study are consistent with those of a few previous studies (Erqou et al. 2018; Hicken et al. 2016). Erqou et al. found a 45% higher risk of cardiovascular events among Black people than White people, partly because of Black people’s higher chronic exposure to PM2.5. However, the association between cardiovascular events and race was no longer statistically significant after adjustments for SES (i.e., income and education) (Erqou et al. 2018). Hicken et al. reported that racial/ethnic differences could be partly adjusted by markers of socioeconomic, psychosocial, and environmental factors (Hicken et al. 2016).
Existing studies have suggested that the use of unclean domestic fuel could enhance the health risk related to PM2.5 exposure (Liu et al. 2017; Salvi et al. 2018). Over 76% of the Yi people used solid fuel to cook, including coal and forestry biomass, in 2013. The proportion was dramatically higher than that found among Han people. Exposure to household air pollution from indoor unclean fuel is a significant environmental health problem in low- and middle-income countries (Shupler et al. 2018). Previous studies found that unclean household fuel usage elevates the blood pressure of women (Alexander et al. 2017; Donee et al. 2017). Studies based on an Indian cohort indicated that indoor solid fuel enhanced the effect of PM2.5 exposure on insulin resistance (Salvi et al. 2018), but the enhancement was not significant on for SBP elevation due to insufficient statistical power (Curto et al. 2019). In another nationwide cross-sectional study in China, stronger associations between higher levels of ambient PM2.5 and higher SBP were observed in participants who used solid fuel for cooking. However, the modification effect was not significant for hypertension (Liu et al. 2017). In this study, with the uncollected data from 2018, data on domestic fuel from 2013 were used to test the modification effect of fuel type. These data are insufficient to test the interaction of PM2.5 exposure and domestic fuel type for hypertension prevalence in the Yi minority group. Even though the interaction between PM2.5 exposure and domestic fuel type is not significant, the use of an unclean fuel type would greatly increase the OR of PM2.5 exposure. The disproportionate distribution of unclean fuel by ethnicity is an important cause of ethnic disparity. Recently, the Chinese government has been committed to health poverty alleviation (Chen and Pan 2019). As universal access to clean energy for households can contribute to sustainable development goals (SDGs) for health and energy, measures should be taken to promote the use of clean household fuel (Rosenthal et al. 2018).
Other chronic diseases can enhance the effect of long-term PM2.5 exposure on hypertension. Studies have shown that participants with chronic diseases like hypertension and diabetes are more susceptible to long-term PM2.5 exposure (Chen et al. 2015; Zhang et al. 2020; Zhang et al. 2018a). Moreover, patients with preexisting coronary heart diseases, chronic lung diseases, or heart failure have also been recognized as susceptible populations (Brook et al. 2010). Age and BMI have been found to modify the effect of long-term PM2.5 exposure (Lin et al. 2017; Liu et al. 2017). In this study, stronger associations were found for elderly people (aged 60 and above), but the interaction term is non-significant. Additionally, a modification effect of BMI was not observed, which may be the result of the BMIs of participants being relatively low with a mean of 22.5 kg/m2. This finding is similar to that of another study (Zhang et al. 2019b).
This study has several strengths. It is based on representative large survey data from Sichuan Province featuring an ethnically diverse population. Additionally, individual information was collected including specific individual ethnicities, which made it possible to adjust a wide range of possible covariates and capture their susceptibility. The high-resolution satellite-based approach allows a precise allocation of the individual exposures to ambient PM2.5.
Despite these strengths, this study also has several limitations. First, the data used in this study comes from cross-sectional surveys, which makes it difficult to infer causal relationships between the long-term exposure to PM2.5 and hypertension. Second, the survey lacks individual dietary information which may be an important modifier for the associations between long-term exposure to PM2.5 and hypertension. The annual salt sales volume was used as a surrogate variable, but it was difficult to infer individual salt intake. Third, self-reported physician-diagnosed hypertension was used to define whether participants had hypertension rather than blood pressure measurements. Finally, similar to existing studies (Lin et al. 2017; Sarkar et al. 2019; Yang et al. 2018b), the annual ambient PM2.5 concentrations of communities/villages were mapped for the participants. By this procedure ignored the activity pattern of the participant was ignored, thus cannot depict variations of individual exposures could not be depicted precisely.
Conclusion
This study provides evidence that long-term exposure to PM2.5 is associated with a higher risk of hypertension in an ethnically diverse population. A stronger association is noticed in people belonging to the Yi minority people. The differences among multi-ethnic people are mainly due to socioeconomic and environmental factors, of which the use of an unclean domestic fuel type is an important contributor.
Available of data and materials
The data that support the findings of this study are available on request from the corresponding author Juying Zhang. The data are not publicly available due to national restrictions on participant privacy.
References
Adar SD et al (2018) Longitudinal analysis of long-term air pollution levels and blood pressure: a cautionary tale from the multi-ethnic study of atherosclerosis. Environ Health Perspect 126:107003. https://doi.org/10.1289/EHP2966
Alexander D et al (2017) Randomized controlled ethanol cookstove intervention and blood pressure in pregnant Nigerian women. Am J Respir Crit Care Med 195:1629–1639. https://doi.org/10.1164/rccm.201606-1177OC
Azimi M, Feng F, Zhou C (2019) Air pollution inequality and health inequality in China: an empirical study. Environ Sci Pollut Res Int 26:11962–11974. https://doi.org/10.1007/s11356-019-04599-z
Bai L et al (2018) Exposure to ambient ultrafine particles and nitrogen dioxide and incident hypertension and diabetes. Epidemiology 29:323–332. https://doi.org/10.1097/EDE.0000000000000798
Benjamin EJ et al (2019) Heart disease and stroke statistics-2019 update: a report from the American Heart Association. Circulation 139:e56–e528. https://doi.org/10.1161/CIR.0000000000000659
Brook RD, Rajagopalan S (2009) Particulate matter, air pollution, and blood pressure. J Am Soc Hypertens 3:332–350. https://doi.org/10.1016/j.jash.2009.08.005
Brook RD et al (2009) Insights into the mechanisms and mediators of the effects of air pollution exposure on blood pressure and vascular function in healthy humans. Hypertension 54:659–667. https://doi.org/10.1161/HYPERTENSIONAHA.109.130237
Brook RD, Rajagopalan S, Pope CA, Brook JR, Kaufman JDJC (2010) Particulate matter air pollution and cardiovascular disease: an update to the scientific statement from the American Heart Association. Circulation 121:2331–2378
Chen C, Pan J (2019) The effect of the health poverty alleviation project on financial risk protection for rural residents: evidence from Chishui City, China. Int J Equity Health 18:79. https://doi.org/10.1186/s12939-019-0982-6
Chen S-Y et al (2015) Associations between long-term air pollutant exposures and blood pressure in elderly residents of Taipei City: a cross-sectional study. Environ Health Perspect 123:779–784. https://doi.org/10.1289/ehp.1408771
Clougherty JE, Kubzansky LD (2009) A framework for examining social stress and susceptibility to air pollution in respiratory health. Environ Health Perspect 117:1351–1358. https://doi.org/10.1289/ehp.0900612
Curto A et al (2019) Ambient particulate air pollution and blood pressure in peri-urban India. Epidemiology 30:492–500. https://doi.org/10.1097/EDE.0000000000001014
Alexander D et al (2017) Randomized controlled ethanol cookstove intervention and blood pressure in pregnant Nigerian women. Am J Respir Crit Care Med 195:1629–1639. https://doi.org/10.1164/rccm.201606-1177OC
Erqou S et al (2018) Particulate matter air pollution and racial differences in cardiovascular disease risk. Arterioscler Thromb Vasc Biol 38:935–942. https://doi.org/10.1161/ATVBAHA.117.310305
Fairburn J, Schule SA, Dreger S, Karla Hilz L, Bolte G (2019) Social inequalities in exposure to ambient air pollution: a systematic review in the WHO European region. Int J Environ Res Public Health 16. https://doi.org/10.3390/ijerph16173127
Feng Y, Ning M, Lei Y, Sun Y, Liu W, Wang J (2019) Defending blue sky in China: effectiveness of the “Air Pollution Prevention and Control Action Plan” on air quality improvements from 2013 to 2017. J Environ Manag 252:109603. https://doi.org/10.1016/j.jenvman.2019.109603
Hicken M, Gragg R, Hu H (2011) ANALYSIS & COMMENTARY How cumulative risks warrant a shift in our approach to racial health disparities: the case of lead, stress, and hypertension. Health Aff 30:1895–1901. https://doi.org/10.1377/hlthaff.2010.1241
Hicken MT et al (2016) Air pollution, cardiovascular outcomes, and social disadvantage: the multi-ethnic study of atherosclerosis. Epidemiology 27:42–50. https://doi.org/10.1097/EDE.0000000000000367
Honda T, Pun VC, Manjourides J, Suh H (2018) Associations of long-term fine particulate matter exposure with prevalent hypertension and increased blood pressure in older Americans. Environ Res 164:1–8. https://doi.org/10.1016/j.envres.2018.02.008
Huang W et al (2018) Short-term blood pressure responses to ambient fine particulate matter exposures at the extremes of global air pollution concentrations. Am J Hypertens 31:590–599. https://doi.org/10.1093/ajh/hpx216
Huang K et al (2019) Long-term exposure to fine particulate matter and hypertension incidence in China. Hypertension 73:1195–1201. https://doi.org/10.1161/HYPERTENSIONAHA.119.12666
Johnson D, Parker JD (2009) Air pollution exposure and self-reported cardiovascular disease. Environ Res 109:582–589. https://doi.org/10.1016/j.envres.2009.01.001
Jones MR et al (2015) Ambient air pollution and racial/ethnic differences in carotid intima-media thickness in the Multi-Ethnic Study of Atherosclerosis (MESA). J Epidemiol Community Health 69:1191–1198. https://doi.org/10.1136/jech-2015-205588
Kodavanti UP (2016) Stretching the stress boundary: Linking air pollution health effects to a neurohormonal stress response. Biochim Biophys Acta 1860:2880–2890. https://doi.org/10.1016/j.bbagen.2016.05.010
Kuang F, Liu X, Zhu B, Shen J, Pan Y, Su M, Goulding K (2016) Wet and dry nitrogen deposition in the central Sichuan Basin of China. Atmos Environ 143:39–50. https://doi.org/10.1016/j.atmosenv.2016.08.032
Li W (2014) Controlling PM2.5 in Chengdu: analysis and recommendations from the China, U.S. and California experience. University of San Francisco
Lin HL et al (2017) Long-term effects of ambient PM2.5 on hypertension and blood pressure and attributable risk among older Chinese adults. Hypertension 69:806. https://doi.org/10.1161/Hypertensionaha.116.08839
Liu C et al (2017) Associations between ambient fine particulate air pollution and hypertension: a nationwide cross-sectional study in China. Sci Total Environ 584:869–874. https://doi.org/10.1016/j.scitotenv.2017.01.133
Ma Z et al (2016) Satellite-based spatiotemporal trends in PM2.5 concentrations: China, 2004-2013. Environ Health Perspect 124:184–192
Morales DX (2019) Geographic inequality and ethnic stratification in China, 2000 to 2010. Int J Sociol Soc Policy 39:535–549. https://doi.org/10.1108/Ijssp-03-2019-0057
Narvaez-Guerra O, Herrera-Enriquez K, Medina-Lezama J, Chirinos JA (2018) Systemic hypertension at high altitude. Hypertension 72:567–578. https://doi.org/10.1161/HYPERTENSIONAHA.118.11140
National Health and Family Planning Commission P (2013) BMI Industry standard of the people’s Republic of China WS/T 428-2013: criteria of weight for adults (ed. National Health and Family Planning Commission, PRC.). Beijing
Rosenthal J, Quinn A, Grieshop AP, Pillarisetti A, Glass RI (2018) Clean cooking and the SDGs: Integrated analytical approaches to guide energy interventions for health and environment goals(). Energy Sustain Dev 42:152–159. https://doi.org/10.1016/j.esd.2017.11.003
Salvi D, Lane KJ, Balakrishnan K, Thanikachalam S, Thanikachalam M (2018) Associations between ambient and indoor PM2.5 exposure and cooking fuel on insulin resistance in the PURSE-HIS cohort. In: ISEE Conference Abstracts, vol 1
Sarkar C, Zhang B, Ni M, Kumari S, Bauermeister S, Gallacher J, Webster C (2019) Environmental correlates of chronic obstructive pulmonary disease in 96 779 participants from the UK Biobank: a cross-sectional, observational study. Lancet Planet Health 3:e478–e490. https://doi.org/10.1016/S2542-5196(19)30214-1
Xu SP (2010) Investigation of prevalence of hypertension and risk factors in Changdu district of Tibet. Dissertation, Tianjin Medical University
Shupler M, Godwin W, Frostad J, Gustafson P, Arku RE, Brauer M (2018) Global estimation of exposure to fine particulate matter (PM2.5) from household air pollution. Environ Int 120:354–363. https://doi.org/10.1016/j.envint.2018.08.026
Sigaux J, Biton J, Andre E, Semerano L, Boissier MC (2019) Air pollution as a determinant of rheumatoid arthritis. Joint Bone Spine 86:37–42. https://doi.org/10.1016/j.jbspin.2018.03.001
Stanaway JD et al (2018) Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 392:1923–1994. https://doi.org/10.1016/S0140-6736(18)32225-6
Statistics NBo China statistical yearbook (2018) China Statistics Press, Bejing
Statistics PcoutscaDoPaE (2012) Tabulation on the 2010 population census of the People’s Republic of China. China Statistics Press, Beijing
van Donkelaar A et al (2016) Global estimates of fine particulate matter using a combined geophysical-statistical method with information from satellites, models, and monitors. Environ Sci Technol 50:3762–3772. https://doi.org/10.1021/acs.est.5b05833
Wang Z et al (2018) Status of hypertension in China: results from the China hypertension survey, 2012-2015. Circulation 137:CIRCULATIONAHA.117.032380. https://doi.org/10.1161/CIRCULATIONAHA.117.032380
Wu X et al (2017) Determination of air pollution-related biomarkers of exposure in urine of travellers between Germany and China using liquid chromatographic and liquid chromatographic-mass spectrometric methods: a pilot study. Biomarkers 22:525–536. https://doi.org/10.1080/1354750x.2017.1306753
Xiong J, Ye C, Zhou T, Cheng W (2019) Health risk and resilience assessment with respect to the main air pollutants in Sichuan. Int J Environ Res Public Health 16. https://doi.org/10.3390/ijerph16152796
Yan SJ, Li H (2017) Review of hypertension prevalence in Chinese minorities. Chinese Journal of Clinicians 11. https://doi.org/10.3877/cma.j.issn.1674-0785.2017.07.024
Yang BY et al (2017) Is prehypertension more strongly associated with long-term ambient air pollution exposure than hypertension? Findings from the 33 Communities Chinese Health Study. Environ Pollut 229:696–704. https://doi.org/10.1016/j.envpol.2017.07.016
Yang B-Y, Qian Z, Howard SW, Vaughn MG, Fan S-J, Liu K-K, Dong G-H (2018a) Global association between ambient air pollution and blood pressure: a systematic review and meta-analysis. Environ Pollut 235:576–588. https://doi.org/10.1016/j.envpol.2018.01.001
Yang BY et al (2018b) Ambient air pollution in relation to diabetes and glucose-homoeostasis markers in China: a cross-sectional study with findings from the 33 Communities Chinese Health Study. Lancet Planet Health 2:e64–e73. https://doi.org/10.1016/S2542-5196(18)30001-9
Yearbook S (2018) Geographic feature. The People’s Government of Sichuan Province network
Zhang Z et al (2018a) Long-term exposure to fine particulate matter, blood pressure, and incident hypertension in Taiwanese adults. Environ Health Perspect 126:017008. https://doi.org/10.1289/EHP2466
Zhang Z et al (2018b) Particulate matter air pollution, physical activity and systemic inflammation in Taiwanese adults. Int J Hyg Environ Health 221:41–47. https://doi.org/10.1016/j.ijheh.2017.10.001
Zhang J, Mou Y, Liao J, Xiong H, Duan Z, Huang Y, Ronsmans C (2019a) Uptake of maternal care and childhood immunization among ethnic minority and Han populations in Sichuan province: a study based on the 2003, 2008 and 2013 health service surveys. BMC Pregnancy Childbirth 19:250. https://doi.org/10.1186/s12884-019-2371-y
Zhang Z et al (2019b) Exposure to ambient particulate matter air pollution, blood pressure and hypertension in children and adolescents: a national cross-sectional study in China. Environ Int 128:103–108. https://doi.org/10.1016/j.envint.2019.04.036
Zhang Y et al (2020) Long-term exposure to ambient fine particulate matter and fasting blood glucose level in a Chinese elderly cohort. Sci Total Environ 717:137191. https://doi.org/10.1016/j.scitotenv.2020.137191
Zhao H et al (2019) Inequality of household consumption and air pollution-related deaths in China. Nat Commun 10:4337. https://doi.org/10.1038/s41467-019-12254-x
Zhou D et al (2013) Whole-genome sequencing uncovers the genetic basis of chronic mountain sickness in Andean highlanders. Am J Hum Genet 93:452–462. https://doi.org/10.1016/j.ajhg.2013.07.011
Acknowledgments
We would like to thank Professor Xiaohui Ren of School of Public Health, Sichuan University who provided valuable suggestions to the study. We also thank all the participant, coordinators, and administrators for their supports in this study.
Funding
Special fund for the 5th and 6th National Health Service Survey in Sichuan Province, supported by Health Commission of Sichuan Province. The funder had no role in the study design, data collection and analysis, interpretation of data, or writing the manuscript.
Author information
Authors and Affiliations
Contributions
Jiayue Xu, Minghong Yao, and Gonghua Wu participated the sixth National Health Service Survey in Sichuan Province, conducted data analysis, and drafted the first-version draft. Yuqin Zhang simulated the PM2.5 concentration in 2017. Zhanqi Duan, Xing Zhao, and Juying Zhang contributed to analysis and design and provided important comments while developing the manuscript. Jiayue Xu is substantively responsible to revise manuscript. The author(s) read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The NHSS is a national survey organized by the National Health and Family Planning Commission of China. The 2013 and 2018 National Health Services Surveys were all legal surveys approved and kept a record by the National Statistical Bureau. Oral consent of participate was obtained before the household survey.
Competing interests
The authors declare that they have no competing interests
Consent to public
Not applicable.
Additional information
Responsible editor: Lotfi Aleya
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 25 kb).
Rights and permissions
About this article

Cite this article
Xu, J., Zhang, Y., Yao, M. et al. Long-term effects of ambient PM2.5 on hypertension in multi-ethnic population from Sichuan province, China: a study based on 2013 and 2018 health service surveys. Environ Sci Pollut Res 28, 5991–6004 (2021). https://doi.org/10.1007/s11356-020-10893-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-020-10893-y