
Abstract
Hand, foot, and mouth disease (HFMD) is a viral illness that is considered a critical public health challenge worldwide. Previous studies have demonstrated that meteorological parameters are significantly related to the incidence of HFMD in children; however, few studies have focused only on female children. This study quantified the associations of HFMD incidence with meteorological parameters and PM10 (particulate matter with an aerodynamic diameter of 10 μm) among female children. Data were collected on daily HFMD cases, meteorological variables, and PM10 levels in Ningbo, China, from January 2012 to December 2016. Data were assessed using a distributed lag nonlinear model (DLNM) with Poisson distribution. A total of 59,809 female children aged 0−15 years with HFMD were enrolled. The results showed that highest relative risk (RR) of HFMD for temperature was 3 °C and the lag effect was 3 days. The highest RR for PM10 was 80 mg/m3 and the lag effect was 5 days. Spatial analysis showed that female HFMD incidence was mainly concentrated in the suburban of Ningbo city indicating that female children in this area should be more paid attention on avoiding this disease outbreak. Our findings suggest that HFMD prevention strategies should focus more attention on local meteorological parameters.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Background
Hand, foot, and mouth disease (HFMD) is a viral illness that is considered a critical public health challenge worldwide (Howard and Vu 2015; AbuBakar et al. 1999; Dwibedi et al. 2010; Wang et al. 2016a; Wu et al. 2014). HFMD is caused mainly by infection with coxsackievirus A16 and enterovirus 71 (Clark et al. 2015; Nassef et al. 2015). These viruses are spread through direct contact with the mucus, saliva, or feces of an infected person. Most cases of HFMD in children are not serious, beginning with a mild fever and then proceeding to a rash of flat discolored spots, bumps, and blisters on the skin of the hands, feet, mouth, and sometimes the buttocks and genitalia (Nassef et al. 2015). However, serious neurological and other complications may occur (Ooi et al. 2010), especially in infants and young children (Zhu et al. 2012). Scientists worldwide are struggling to find effective ways to protect the health of the younger generations, including the use of novel high-speed real-time PCR methods to diagnosis adenovirus (Fujimoto et al. 2010) and investigations into children’s immunity level to HFMD (Zhang et al. 2017; Du et al. 2016).
Large outbreaks of HFMD have been reported in Asia in recent years (Gui et al. 2015; Chen et al. 2015; Zha and Ma 2015), especially in China, Japan, and India (Gui et al. 2015; Chen et al. 2015; Zha and Ma 2015). In China, HFMD was first reported in the 1980s, and beginning in March 2008, a single outbreak in Fuyang (Anhui province) resulted in over 25,000 cases and 42 deaths (Zhang et al. 2010). Since then, the number of cases has increased dramatically. From 2008 to the end of July 2012, China as a whole reported 1,520,274 HFMD cases and 431 deaths. In 2013, and 2014, over 4.5 million cases were identified by China’s national surveillance system.
As of 2010, there were 130 million female children in China, representing 46.3% of all children in China. The societal position of female children is strongly associated with their overall health. Despite the availability of some vaccines in the Chinese market last year, prevention strategies and early warning methods are particularly important for governmental efforts aimed at integrated, large-scale disease control. According to a report from Zhejiang Province, the average incidence of HFMD was 172.98 (range 72.61−270.04) per 100,000 individuals (Gui et al. 2015). A study by Hongxiao Ni conducted in Ningbo from 2008 to 2011 found that 95.6% of HFMD cases occurred in children under 5 years of age (Ni et al. 2012).
Studies carried out in several different regions of China have shown that the incidence of HFMD is sensitive to meteorological changes (Guo et al. 2011; Zhu et al. 2015; Liu et al. 2015). For instance, an investigation by Yin et al. conducted in Chengdu found that temperature played an important role in HFMD incidence, with non-linear and delayed effects (Yin et al. 2016). Wang et al. also found that HFMD incidence among children in China was positively associated with meteorological parameters, as well as being influenced by overall climate type (Yin et al. 2016). A study by Liao et al. in Sichuan Province showed heterogeneous spatial-temporal mapping of HFMD and found that temperature was the primary risk factor for infection in wealthier counties (Liao et al. 2016). A study by Hii et al. showed that the incidence of HFMD was positively associated with temperature: The incidence of HFMD increased by 36% per degree above 32 °C (Hii et al. 2011). Another study conducted in Beijing revealed that the relationship between temperature and HFMD incidence was non-linear in most age groups (the exception being children aged 6 to 15 years), with a peak at 25 to 27 °C (Xu et al. 2015).
Air pollution, which causes adverse health effects in large populations, is of increasing concern worldwide. Of particular concern is particulate matter, such as PM10 (particulate matter with an aerodynamic diameter of 10 μm). PM10 can enter the respiratory system and penetrate pulmonary alveoli, through which it can enter the circulatory system, resulting in serious health problems. Ye et al. found that PM10 concentrations were positively associated with the relative risk (RR) of rotavirus infection, with a 1- to 1.5-day lag (Ye et al. 2016). Souza et al. found a strong positive association between exposure to PM10 and hospitalization for pneumonia among children. The percentage increase in relative risk was 15% to PM10 in lag 0 (Souza 2016). Furthermore, Dr. Wangjian Zhang et al. reported that younger children and those from the Pearl River Delta region were more sensitive to weather changes and that temperature showed the largest contribution to HFMD epidemics (Zhang et al. 2016). Spatial pattern is also the concern on the effect to the incidence of HFMD. A study by Wu et al. showed that HFMD incidence from 2009 to 2015 in Hunan Province was a spatiotemporal clustering tendency (Wu et al. 2017). Xu et al. have drawn spatiotemporal risk mapping of HFMD and found that some cities such as Beijing and Tianjin have higher incidence than other moderate cities (Xu and Xiao 2017).
We focused our attention on female HFMD incidence since some recent studies have been indicated that female children have a higher relative risk (RR) of HFMD in the association with meteorological changes. Yang et al. reported that the effects of relative humidity (RH) on female children HFMD incidence were higher than those of male children (female RR 2.00 vs. male RR 1.55) (Ye et al. 2016). A study by Gaihuan et al. analyzed the risk factors for HFMD death and indicated that gender was a risk factor and, in particular, female sex with odds ratio (OR 17.38) was identified as independent risk factors for death (Souza 2016). However, authors declared that due to limited studies on the gender risk factor, no plausible explanation was available for their finding. Based on the previous reports, we hypothesized that the female children were more sensitive to the meteorological changes and air pollution, specifically PM10. Thus, the incidence of respiratory diseases, such as HFMD, in female children would be influenced by meteorological parameters and air pollutants, specifically PM10. The goal of this study was to assess the effects of temperature and PM10 on the incidence of HFMD in female children in Ningbo. Ningbo is a city on the east coast of China (see Fig. 1) with a population of 7.81 million as of 2014. The climate consists of hot summers and cool, wet winters. The city has seen a disproportionately high incidence of HFMD in recent years. The first death due to HFMD in Ningbo occurred in 2009; since then, many severe HFMD cases have occurred in children, resulting in neurogenic pulmonary edema and several deaths. We hypothesized that meteorological parameters, including temperature, humidity and wind, may influence HFMD virus reproduction and concentration. Additionally, PM10 is typically suspended in the air and persists for a long period, where it can reflect and absorb ultraviolet rays. This characteristic has been shown to influence virus reproduction and survival, as well as affect meteorological variables. We investigated the effects of meteorological changes, air pollution, and spatial characteristics on HFMD incidence in female children, and our findings may lead to appropriate strategies to decrease the incidence of HFMD in female children.

Map of Ningbo City, Zhejiang Province, China
Methods
Data collection
All data on HFMD cases in Ningbo from January 2012 to December 2016 were collected by the Ningbo Centre for Disease Control and Prevention through the National Notifiable Disease Reporting System. All HFMD cases were diagnosed by the standards of the Chinese Ministry of Health (Zhou et al. 2015). Daily data from January 2012 to December 2016 on meteorological variables, including mean temperature, relative humidity, wind velocity, and PM10 concentration, were collected from the China Meteorological Data Sharing Service System founded by the Chinese Meteorological Bureau.
Data analysis
The statistical analysis was carried out in two steps. First, descriptive statistics were commenced by displaying the distribution of meteorological factors, PM10, and HFMD cases. Additionally, Spearman’s correction test was performed to explore the relationships between meteorological factors, PM10, and HFMD. Second, according to our previous study, there was a lag effect on the incidence of HFMD: The number of HFMD cases on any given day was shown to be affected by the meteorological conditions over the past few days. For sufficient flexibility to describe the additional time dimension of the exposure-response relationship, a distributed lag nonlinear model (DLNM) was used in this study. Furthermore, this model, which has previously been used to investigate the impact of heat waves on daily mortality and temperature variation between neighboring days and morbidity (Ban et al. 2017; Phung et al. 2016), was shown to be an effective model to investigate associations of HFMD incidence with meteorological parameters and PM10. The DLNM model was generated with R software (R Development Core Team, Vienna, Austria) and showed nonlinear relationships and delayed time effects simultaneously.
The model is described by the following formula:\( {\displaystyle \begin{array}{l}{Y}_{t\sim } Poisson\left({\mu}_{\mathrm{t}}\right)\\ {}\log \left[\mathrm{E}\left(\mathrm{Y}\right)\right]=\alpha + ns\left({T}_{t,l}, df\right)+\varphi pressure+ ns\left(P{\mathrm{M}}_{10t,l}, df\right)+\sigma windspeed+ ns\left({HM}_{t,l}, df\right)\\ {}+\lambda {DOW}_t+\kappa Strata\end{array}} \) where E(Y) refers to the expected daily numbers for HFMD on a certain day; t is the day of the observation; α is the model intercept; l is the lag days; Tt,l is the daily average temperature in Celsius; HMt,l is the daily average percent ns(RHt, l, df) humidity; PM10t,l is the daily PM10 concentration; a natural cubic spline DLNM was used to model the nonlinear temperature, humidity PM10 association with 5 degrees of freedom (df), and the lagged association using 4 df; k and j are vectors of coefficients; DOWt is the week parameter; and Strata is a categorical variable for the year and calendar month used to control for long-term trends and seasonality, with 36 strata in total (Xu et al. 2015).
Given that some meteorological factors and HFMD relationships can be nonlinear and that the association can be delayed (Huang et al. 2016), and assuming that HFMD has an incubation period that typically ranges from 3 to 12 days, the maximum lag was set to 13 days to explore the whole lag structure of effect. Spline knots were designed for the same intervals in meteorological variables and PM10 ranges, as well as in the log scale of lag days. Analyses were conducted using R software (ver. 3.1.0); the “dlnm” package was used to conduct stratified analysis (Gasparrini 2011). Spearman’s correlation tests were two-sided. P values less than 0.05 were considered statistically significant. Corresponding 95% confidence intervals (CI) were used to describe all risk estimates. Sensitivity analyses were carried out, changing the maximum lag days for DLNM from 13 to 20 days and the df from 4 to 7. This study was approved by the Institutional Review Board of the Ningbo Centre for Disease Control. Data analyses were de-identified (number 201601).
To illustrate the spatiotemporal characteristics of female HFMD incidence, meteorological factors, and PM10 levels, and to investigate the presence of spatial stratified heterogeneity in the strata mentioned in this study, we used a geographical information system (GIS) (Gasparrini 2011)and the spatial stratified heterogeneity q-statistic (Wang et al. 2016b; Wang et al. 2010) for analysis. GIS is used to store, display, and analyze geographically referenced data (locations) (Smith et al. 2017). Spatial stratified heterogeneity, which is available on the website http://www.geodetector.org/, is a universal driver of biological diversity and evolution, environmental patterns and dominance, and inter-regional conflicts and cooperation (Wang et al. 2011; Wang et al. 2013; Shi et al. 2014; Bo et al. 2014; Huang et al. 2015). Based on the hypothesis that the philosophy of geographical detector is that variable Y is associated with variable X if their spatial distributions tend to be identical,
where σ2 stands for the variance of Y, N stands for the size of study population of Y (the size of study area or the size of study human population, for example), and the study population of Y is composed of L strata (h = 1, 2, …, L). The strata of Y may exist already, may be constructed by classification, or may be formed by laying Y over X, which consists of strata. q = [0, 1], q = 0 indicates that Y is not a spatially stratified heterogeneous or that there is no association between Y and X; q = 1 indicates that Y is perfectly spatially stratified heterogeneous or that Y is completely determined by X; and the value of the q-statistic indicates the degree of spatial stratified heterogeneity of Y or how much Y is interpreted by X.
In this study, the female HFMD incidence is represented as Y, while temperature, wind speed, relative humidity, and PM10 represent risk factors. First, we divided Ningbo City into 2 × 2-km grids, producing 1003 grids, and then we added the grid to female HFMD incidence and exacted the incidence from each grid. Then, we used the formula mentioned above to calculate the stratified heterogeneity. A portion of the population data was drawn from the 2014 statistical yearbook, 2010 census data, and the resident population, while other data were obtained from villages and towns, streets, government networks, or geographical names network mentioned in the 2010 resident population.
Data availability
The data used in this study are available from Ningbo Municipal Center for Disease Control and Prevention, Ningbo, Zhejiang Province, China, but restrictions apply to the availability of these data, which were used under license for the current study and are not publicly available. Data are, however, available from the authors upon reasonable request and with permission of Ningbo Municipal Center for Disease Control and Prevention, Ningbo, Zhejiang Province, China.
Results
Study characteristics
Table 1 includes all female HFMD cases from 2012 to 2016 and provides the number of cases by age range. In Ningbo, this period contained a total of 59,809 HFMD cases, of which 7.06% of patients were aged < 1 year, 52.25% were aged 1–3 years, 31.63% were aged 3–6 years, and 9.06% were aged 6–15 years. Notably, 99.94% of all confirmed cases occurred in children under 15 years of age. Female children aged 1–6 years accounted for 83.88% of all reported female pediatric cases and should be given special attention.
Table 2 reveals the conditions of meteorological variables and PM10 levels in Ningbo during the period from January 2012 to December 2016. The daily averages for temperature, relative humidity, atmospheric pressure, wind speed, and PM10 were 18.14 °C, 74.07%, 1014.51 hPa, 12.88 m/s, and 94.49 mg/m3, respectively.
Baseline information for Ningbo, meteorological factors, and female HFMD cases
Figure 1 illustrates the location of Ningbo on a map. Ningbo is a sub-provincial city in northern Zhejiang Province in China. This city comprises the urban districts of Ningbo proper, three satellite cities, and 80 rural counties. According to the 2010 census, Ningbo has a population of 7.6 million, with 3.5 million residing in the six urban districts of Ningbo proper.
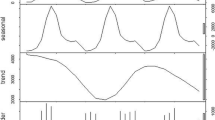
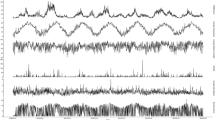
Figure 2 illustrates the daily distributional trends of HFMD cases and meteorological variables from 2012 to 2016. The results indicate significant seasonal variation in the incidence of female HFMD cases from January 2012 to December 2016 in Ningbo. The incidence of female HFMD cases peaked in April, June, and July and was lowest in January. This seasonal variation in female HFMD cases was most significantly related to temperature. The daily concentration of PM10 did not show as much seasonal variation as did the incidence of female HFMD cases and temperature; however, it can be seen in Fig. 2 that the PM10 concentration was higher in fall than in summer. The peak PM10 concentration of 605 mg/m3 was recorded in December. The daily humidity and wind speed were fairly homogenous, without significant peaks during the period of data collection.

Daily distribution of hand, foot, and mouth disease (HFMD) incidence and mean temperature, humidity, wind speed, and PM10 (particulate matter with an aerodynamic diameter 10 μm) level in Ningbo, 2012–2016
DLNM illustrations
Figure 3 shows a three-dimensional (3D) plot generated to display the associations among relative risk (RR), temperature in degrees Celsius, and lag days (n = 13). This plot revealed a nonlinear relationship between temperature and the incidence of HFMD, as well as a different lag pattern between temperature and the incidence of HFMD. The incidence of HFMD was relatively high at low temperatures and highest near 3 °C.

Three-dimensional (3D) plot generated to display the associations among relative risk (RR), temperature in degrees Celsius, and lag days (n = 13)
Figure 4 shows the RR of female HFMD cases at different lag days and temperatures. The highest RR was seen at 3 °C. At this temperature, the RR of HFMD was high at the 0-day lag and highest at the 3-day lag, before showing a steady decrease for 10 days. In contrast, the high temperature (31 °C) showed the lowest RR.

The RR of female HFMD cases at different lag days and temperatures
Figure 5 shows a 3D plot generated to display the associations among RR, PM10, and lag days (n = 13). This plot shows a nonlinear relationship between the PM10 concentration and incidence of HFMD, as well as a different lag pattern than that between temperature and the incidence of HFMD. When the PM10 concentration was 35 mg/m3, the highest RR for the incidence of female HFMD cases was observed at a lag 5 of days.

Three-dimensional plot generated to display the associations among RR, PM10, and lag days (n = 13)
Figure 6 presents the RR of female HFMD cases by PM10 concentration at specific lag days (0, 3, 7 days). The highest PM10 concentration, approximately 80 mg/m3, showed a high risk relative to female HFMD cases on the fifth lag day.

The RR of female HFMD cases by PM10 concentration at specific lag days (0, 3, 7 days)
Spatiotemporal pattern
Table 3 presents significant spatial stratified heterogeneity in the risk factors analyzed, including average temperature, average wind speed, relative humidity, and PM10 level. The spatial stratified heterogeneity of relative humidity was largest (q = 0.2977), indicating that the influence of this risk factor was greater than that of the other three risk factors on female HFMD.
Figure 7 shows the spatiotemporal pattern of the incidence of female HFMD, temperature, wind speed, relative humidity, and PM10 level in Ningbo for 2014. A high female HFMD incidence was mainly concentrated in the suburban areas, while the female HFMD incidence was smaller in the city center and tended to decrease in the outer suburbs. The yearly average temperature in the eastern and southern urban areas was higher than in other areas, while the yearly average wind speed was lower in the center and eastern urban region. In the urban west region, the yearly average level of PM10 was higher than in the eastern and south-eastern portion of the city.

spatiotemporal pattern of incidence of female HFMD, temperature, wind speed, relative humidity, and PM10 in 2014, Ningbo City
Discussion
In this study, we conducted a DLNM analysis to investigate the effects of meteorological variables and PM10 levels on the incidence of HFMD among female children in the city of Ningbo. After controlling for confounders, the outcomes displayed nonlinear relationships. The results showed that the highest relative risk (RR) of HFMD for temperature was 3 °C and the lag effect was 3 days. The highest RR for PM10 was 80 mg/m3 and the lag effect was 5 days. Spatial analysis showed that female HFMD incidence was mainly concentrated in the suburban of Ningbo city. Our study conducted to provide some baseline information for further taking measures or strategies to reduce the incidence HFMD in female children or help official institutes to control HFMD outbreaks among female children. Here, although many researchers have indicated that the case number of male children is even more than that of the female ones (Huang et al. 2018), in this study, we focused our attention on the female children based on the following considerations. First, some previous studies have reported that female children were more sensitive to HFMD with meteorological changes. Yang et al. reported that the effects of relative humidity (RH) on female children HFMD incidence were higher than those of male children (female RR 2.00 vs. male RR 1.55) (Ye et al. 2016). A study by Gaihuan et al. analyzed the risk factors for HFMD death and indicated that gender was risk factor and, in particular, female sex with odds ratio (OR 17.38) was identified as independent risk factors for death (Souza 2016). Second, in China, as well as in some other developing countries, due to the traditional preference for boys, female children are usually neglected, in particular, in the rural areas. Our study results showed that female children in the rural Ningbo areas have a higher RR of HFMD mentioning their parents or researchers to pay more attention on prevent female children from HFMD damage.
In recent years, HFMD has become well-known for causing severe complications in infants and children, including pulmonary edema, myocarditis, or even death (Aswathyraj et al. 2016). Epidemiological data indicate that the incidence of HFMD continues to increase in Ningbo, which presents a great challenge. In particular, these outbreaks of HFMD are occurring with increasing frequency among children (Ni et al. 2012). Lin Zhu reported a relationship between HFMD and temperature in 17 cities in China (Zhu et al. 2016). In addition, a study by Xu et al. suggested that differences in temperature between neighboring days, and by diurnal temperature, may impact the incidence of HFMD among children in Huainan Province, China (Xu et al. 2016). Zhu et al. showed that the effect of temperature on HFMD incidence was significant and that impact patterns change according to geography (Zhu et al. 2015). Xu et al. applied DLNM analysis and reported a nonlinear association between ambient temperature and HFMD (Xu et al. 2015); his outcomes also showed a positive relationship between temperature and the incidence of HFMD cases in female children, and our study generated similar results. A study by Jinju Wu also showed that females were more vulnerable to temperature increases (Wu et al. 2016). Kim et al. used a generalized additive model and found that when the temperature increased by 1°, the HFMD rate increased by 10.3% (Kim et al. 2016), and Jiang et al. used Spearman’s rank correlation analysis to show that HFMD incidence was also positively correlated with temperature (Jiang et al. 2016). Thus, different statistical models have all demonstrated that temperature contributes to the incidence of HFMD. We chose to apply DLNM analysis because it produces a detailed representation of nonlinear exposure–response relationships while avoiding the co-linearity issues among lagging exposure variables that occur in other models. Our female-specific analyses indicated that there existed associations between high temperatures and the incidence of HFMD; however, besides this, a high RR of female HFMD incidence was associated with low temperatures as well. The incidence of HFMD cases was relatively high at low temperatures, and it was highest near 3 °C. Thus, our results differ from those of some previous studies, and the reason for the higher RR observed at lower temperatures may be explained as follows. First, Ningbo is a coastal city, with a different location compared to previous studies regarding female HFMD, such as Beijing and Hefei. Thus, different locations may show different meteorological patterns. Second, the city of Ningbo is located in the mid-latitudes in the monsoon region, and the climate is cool and wet in winter but hot and rainy in summer. According to some previous studies, high humidity has a positive effect on HFMD incidence (Yang et al. 2017; Wu et al. 2016; Onozuka and Hashizume 2011), as the HFMD virus can aerosolize more easily in low temperatures with high humidity. Indeed, the HFMD virus can survive for an extended period as an aerosol. Thus, increased viral replication facilitates the spread of HFMD throughout the population such that the odds of infection increase dramatically. For these reasons, we believe that the higher relative risk of infection in winter in Ningbo, compared to summer, may be due to the high humidity present in winter. However, further studies involving other female HFMD cases in other cities or counties should be carried out to verify the effect of temperature on this disease. Furthermore, children spend much time studying in classrooms. Due to the rapid increase in the child population, the available classroom space for children is insufficient; as this phenomenon of “short supply” continues to intensify, increasing numbers of classrooms will be crammed with children. As a result, these conditions may increase the infection opportunity of HFMD; particularly if some schools keep the doors and windows closed during cold periods, the spread of HFMD could become more rapid. Thus, these conditions increase the risk of infection due to both proximity and lack of air flow. Furthermore, lab experiments have shown that enteroviruses thrive in wet environments. Ningbo, as a coastal city, has a high number of precipitation days and high humidity, especially in the spring, which may exacerbate HFMD epidemics. There is also increased haze during cold seasons due to low-pressure systems, and evidence has shown that haze can collect bacteria and viruses in the air, leading to human infections as a result of inhaling the haze. In contrast, Kim et al. used a generalized additive model and found that when the temperature increased by 1°, the HFMD rate increased by 10.3% (Kim et al. 2016), and Jiang et al. used Spearman’s rank correlation analysis to show that HFMD incidence was also positively correlated with temperature (Jiang et al. 2016). Thus, different statistical models have all demonstrated that temperature contributes to the incidence of HFMD. We chose to apply DLNM analysis because it produces a detailed representation of nonlinear exposure–response relationships while avoiding the co-linearity issues among lagging exposure variables that occur in other models.
The influence of other meteorological factors upon the incidence of HFMD has been shown by numerous studies. For instance, Wang et al. investigated the spatial dynamic patterns of HFMD disease in China and found that HFMD was spatially dispersed across China (Wang et al. 2013; Wang et al. 2011; Hu et al. 2012). Liao assessed the association between weekly HFMD cases and meteorological data on different temporal and spatial scales in Shandong Province from May 2008 to July 2008 and September 2008 to October 2008 (Liao et al. 2015). These studies have contributed to understanding the mechanisms of HFMD incidence from the perspectives of physiologic and demographic determinants. Our results, showing that the city of Ningbo in eastern China had a higher incidence of HFMD during 2012–2014 and that this incidence was influenced by meteorological factors, support these previous findings. According to our analysis of spatial stratified heterogeneity q-statistics, one meteorological factor, relative humidity, was found to have significant stratified heterogeneity (q = 0.2977, p = 0.00) as well as the highest influence on female HFMD incidence among all of the risk factors investigated. Indeed, a study by Yang et al. indicated that the effect of relative humidity on childhood HFMD increased above a humidity of 84%, with a 0.34% (95% CI 0.23–0.45%) increase of childhood HFMD per 1% increment of relative humidity (Yang et al. 2017). As a coastal city, Ningbo experiences high humidity throughout the year, with an average humidity of approximately 73.17%. Humidity benefits viral survival and spread, and changes in humidity should be considered important for the development of HFMD control programs. Together, our findings may contribute to government efforts aimed at effective preventive strategies to control HFMD outbreaks in various seasons and areas with different meteorological factors.
Few studies have investigated the effects of PM10 concentration on HFMD incidence. It is interesting to note that while PM10 was positively associated with HFMD incidence in female children, the RR peaked at a 6-day lag with the PM10 level at 90 mg/m3. These results may be due to increasing industrial activities in recent years, which may have increased the level of air pollution. At this point, there is more than sufficient evidence for a relationship between air pollution and respiratory diseases. In recent years, studies on the relationships between PM10 and various diseases have increased markedly. One study showed positive and significant coefficients for PM10 during periods when asthma medication was administered to school children (Gordian and Choudhury 2003). PM10 has also demonstrated an adverse effect on the pulmonary function of normal children (Kim et al. 2005). Reyes-Zarate et al. found that PM10 was a risk factor for the development of lung cancer (Reyes-Zarate et al. 2016), and a study in Australia found that geogenic PM10 exposure increased inflammation, impaired lung function, and increased viral load, thereby exacerbating the response to respiratory viral infection (Smith et al. 2006). Another study reported that PM10 seems to play an important role in the transmission of Q fever from infected animals to humans. It has also been shown that more severe respiratory symptoms, including cough, phlegm, and dyspnea, can be caused by air pollution. Indeed, in the presence of air pollution, including PM10, the entire respiratory system remains under attack. Thus, it can be inferred that with greater damage to the respiratory system, the risk of infection with pathogens such as HFMD increases. Female children living in developing countries are the most vulnerable population in terms of total deaths attributable to indoor and outdoor air pollution because their bodies are immature and their organs are more sensitive to air pollution. Thus, protective strategies against HFMD in children should be immediately implemented in China, and the association between ambient air pollution and the incidence of HFMD warrants further investigation.
Several limitations of this study should be acknowledged. First, we considered only certain meteorological variables and PM10. Other major risk factors for HFMD include season, urban or suburban living, aggregated ultraviolet radiation, socioeconomic status, and environmental PM2.5, and these factors should be considered or adjusted for in future studies. Second, the data in our study were fixed environmental data rather than individual exposure data, which may have led to measurement error. Third, because this study covered only a single city, the results may not be applicable to other cities with different climates.
In conclusion, our study revealed a nonlinear relationship between temperature, PM10 levels, and the incidence of HFMD among female children in a coastal city in China. Although the complexity of HFMD incidence cannot be fully explained by weather or air pollution, our results provide new quantitative evidence for the influence of weather factors and air pollution on HFMD infections in female children. Further studies are required to investigate the mechanism underlying the effect of climate and ambient air pollution on the incidence of HFMD in children.
References
AbuBakar S, Chee HY, al-Kobaisi MF, Xiaoshan J, Bing Chua K, Kit Lam S (1999) Identification of enterovirus 71 isolates from an outbreak of hand, foot and mouth disease (HFMD) with fatal cases of encephalomyelitis in Malaysia. Virus Res 61(1):1–9
Aswathyraj S, Arunkumar G, Alidjinou EK, Hober D (2016) Hand, foot and mouth disease (HFMD): emerging epidemiology and the need for a vaccine strategy. Med Microbiol Immunol 205:397–407
Ban J, Xu D, He MZ, Sun Q, Chen C, Wang W, Zhu P, Li T (2017) The effect of high temperature on cause-specific mortality: a multi-county analysis in China. Environ Int 106:19–26
Bo YC, Song C, Wang JF, Li XW (2014) Using an autologistic regression model to identify spatial risk factors and spatial risk patterns of hand, foot and mouth disease (HFMD) in mainland China. BMC Public Health 14:358
Chen, G.P., et al. (2015) Epidemiological characteristics and influential factors of hand, foot and mouth disease (HFMD) reinfection in children in Anhui province. Epidemiol Infect 1–8
Clark CM, Silverberg NB, Weinberg JM (2015) What is your diagnosis? Onychomadesis following hand-foot-and-mouth disease. Cutis 95(6):312 319-20
Du Z et al (2016) The threshold effects of meteorological factors on hand, foot, and mouth disease (HFMD) in China, 2011. Sci Rep 6:36351
Dwibedi B, Kar BR, Kar SK (2010) Hand, foot and mouth disease (HFMD): a newly emerging infection in Orissa, India. Natl Med J India 23(5):313
Fujimoto T, Konagaya M, Enomoto M, Tsuboi K, Hashimoto K, Taniguchi K, Kodama T, Okabe N (2010) Novel high-speed real-time PCR method (hyper-PCR): results from its application to adenovirus diagnosis. Jpn J Infect Dis 63(1):31–35
Gasparrini A (2011) Distributed lag linear and non-linear models in R: the package dlnm. J Stat Softw 43(8):1–20
Gordian ME, Choudhury AH (2003) PM10 and asthma medication in schoolchildren. Arch Environ Health 58(1):42–47
Gui J, Liu Z, Zhang T, Hua Q, Jiang Z, Chen B, Gu H, Lv H, Dong C (2015) Epidemiological characteristics and spatial-temporal clusters of hand, foot, and mouth disease in Zhejiang Province, China, 2008-2012. PLoS One 10(9):e0139109
Guo Y, Barnett AG, Pan X, Yu W, Tong S (2011) The impact of temperature on mortality in Tianjin, China: a case-crossover design with a distributed lag nonlinear model. Environ Health Perspect 119(12):1719–1725
Hii YL, Rocklov J, Ng N (2011) Short term effects of weather on hand, foot and mouth disease. PLoS One 6(2):e16796
Howard CT, Vu PD (2015) You’re the flight surgeon: hand, foot, and mouth disease. Aerosp Med Hum Perform 86(5):497–500
Hu M, Li Z, Wang J, Jia L, Liao Y, Lai S, Guo Y, Zhao D, Yang W (2012) Determinants of the incidence of hand, foot and mouth disease in China using geographically weighted regression models. PLoS One 7(6):e38978
Huang JX, Wang JF, Li ZJ, Wang Y, Lai SJ, Yang WZ (2015) Visualized exploratory spatiotemporal analysis of hand-foot-mouth disease in southern China. PLoS One 10(11):e0143411
Huang R, Bian G, He T, Chen L, Xu G (2016) Effects of meteorological parameters and PM10 on the incidence of hand, foot, and mouth disease in children in China. Int J Environ Res Public Health 13(5). https://doi.org/10.3390/ijerph13050481
Huang J, Liao Q, Ooi MH, Cowling BJ, Chang Z, Wu P, Liu F, Li Y, Luo L, Yu S, Yu H, Wei S (2018) Epidemiology of recurrent hand, foot and mouth disease, China, 2008–2015. Emerg Infect Dis 24(3). https://doi.org/10.3201/eid2403.171303
Jiang FC et al (2016) Meteorological factors affect the hand, foot, and mouth disease epidemic in Qingdao, China, 2007-2014. Epidemiol Infect 144(11):2354–2362
Kim JH, Lim DH, Kim JK, Jeong SJ, Son BK (2005) Effects of particulate matter (PM10) on the pulmonary function of middle-school children. J Korean Med Sci 20(1):42–45
Kim BI, Ki H, Park S, Cho E, Chun BC (2016) Effect of climatic factors on hand, foot, and mouth disease in South Korea, 2010-2013. PLoS One 11(6):e0157500
Liao Y, Ouyang R, Wang J, Xu B (2015) A study of spatiotemporal delay in hand, foot and mouth disease in response to weather variations based on SVD: a case study in Shandong Province, China. BMC Public Health 15:71
Liao J, Qin Z, Zuo Z, Yu S, Zhang J (2016) Spatial-temporal mapping of hand foot and mouth disease and the long-term effects associated with climate and socio-economic variables in Sichuan Province, China from 2009 to 2013. Sci Total Environ 563-564:152–159
Liu Y, Wang X, Pang C, Yuan Z, Li H, Xue F (2015) Spatio-temporal analysis of the relationship between climate and hand, foot, and mouth disease in Shandong province, China, 2008-2012. BMC Infect Dis 15:146
Nassef C, Ziemer C, Morrell DS (2015) Hand-foot-and-mouth disease: a new look at a classic viral rash. Curr Opin Pediatr 27(4):486–491
Ni H, Yi B, Yin J, Fang T, He T, du Y, Wang J, Zhang H, Xie L, Ding Y, Gu W, Zhang S, Han Y, Dong H, Su T, Xu G, Cao G (2012) Epidemiological and etiological characteristics of hand, foot, and mouth disease in Ningbo, China, 2008-2011. J Clin Virol 54(4):342–348
Onozuka D, Hashizume M (2011) The influence of temperature and humidity on the incidence of hand, foot, and mouth disease in Japan. Sci Total Environ 410-411:119–125
Ooi MH, Wong SC, Lewthwaite P, Cardosa MJ, Solomon T (2010) Clinical features, diagnosis, and management of enterovirus 71. Lancet Neurol 9(11):1097–1105
Phung D, Guo Y, Thai P, Rutherford S, Wang X, Nguyen M, Do CM, Nguyen NH, Alam N, Chu C (2016) The effects of high temperature on cardiovascular admissions in the most populous tropical city in Vietnam. Environ Pollut 208(Pt A):33–39
Reyes-Zarate E et al (2016) Atmospheric particulate matter (PM10) exposure-induced cell cycle arrest and apoptosis evasion through STAT3 activation via PKCzeta and Src kinases in lung cells. Environ Pollut 214:646–656
Shi RX, Wang JF, Xu CD, Lai SJ, Yang WZ (2014) Spatiotemporal pattern of hand-foot-mouth disease in China: an analysis of empirical orthogonal functions. Public Health 128(4):367–375
Smith KR, Veranth JM, Kodavanti UP, Aust AE, Pinkerton KE (2006) Acute pulmonary and systemic effects of inhaled coal fly ash in rats: comparison to ambient environmental particles. Toxicol Sci 93(2):390–399
Smith MR, Davis RL, Phillips PA, Shvilkina T, Kaur K, Tabolt HK, Krause M, Galdi V (2017) Geographical information system evaluation and trends of nonaccidental trauma at a level I trauma center, pilot study. Ann Surg 265(2):418–423
Souza LS, Nascimento LF (2016) Air pollutants and hospital admission due to pneumonia in children: a time series analysis. Rev Assoc Med Bras 62:151–156
Wang J et al (2010) Geographical detectors-based health risk assessment and its application in the neural tube defects study of the Heshun Region, China. Int J Geogr Inf Sci 24(1):107–127
Wang JF, Guo YS, Christakos G, Yang WZ, Liao YL, Li ZJ, Li XZ, Lai SJ, Chen HY (2011) Hand, foot and mouth disease: spatiotemporal transmission and climate. Int J Health Geogr 10:25
Wang JF, Xu CD, Tong SL, Chen HY, Yang WZ (2013) Spatial dynamic patterns of hand-foot-mouth disease in the People’s Republic of China. Geospat Health 7(2):381–390
Wang C, Cao K, Zhang Y, Fang L, Li X, Xu Q, Huang F, Tao L, Guo J, Gao Q, Guo X (2016a) Different effects of meteorological factors on hand, foot and mouth disease in various climates: a spatial panel data model analysis. BMC Infect Dis 16(1):233
Wang J, Zhang T, Fu B (2016b) A measure of spatial stratified heterogeneity. Ecol Indic 67:250–256
Wu X, Sun Y, Lin C, Jia L, Wu Q, Li X, Wang Q (2014) A case-control study to identify environmental risk factors for hand, foot, and mouth disease outbreaks in Beijing. Jpn J Infect Dis 67(2):95–99
Wu J, Cheng J, Xu Z, Zhao K, Zhao D, Xie M, Yang H, Wen L, Li K, Su H (2016) Nonlinear and interactive effects of temperature and humidity on childhood hand, foot and mouth disease in Hefei, China. Pediatr Infect Dis J 35(10):1086–1091
Wu X et al (2017) Spatio-temporal clustering analysis and its determinants of hand, foot and mouth disease in Hunan, China, 2009–2015. BMC Infect Dis 17(1):645
Xu CD, Xiao GX (2017) Spatiotemporal risk mapping of hand, foot and mouth disease and its association with meteorological variables in children under 5 years. Epidemiol Infect 145(14):2912–2920
Xu M, Yu W, Tong S, Jia L, Liang F, Pan X (2015) Non-linear association between exposure to ambient temperature and children’s hand-foot-and-mouth disease in Beijing, China. PLoS One 10(5):e0126171
Xu J, Zhao D, Su H, Xie M, Cheng J, Wang X, Li K, Yang H, Wen L, Wang B (2016) Impact of temperature variability on childhood hand, foot and mouth disease in Huainan, China. Public Health 134:86–94
Yang H, Wu J, Cheng J, Wang X, Wen L, Li K, Su H (2017) Is high relative humidity associated with childhood hand, foot, and mouth disease in rural and urban areas? Public Health 142:201–207
Ye Q, Fu JF, Mao JH, Shen HQ, Chen XJ, Shao WX, Shang SQ, Wu YF (2016) Haze is an important medium for the spread of rotavirus. Environ Pollut 216:324–331
Yin F, Zhang T, Liu L, Lv Q, Li X (2016) The association between ambient temperature and childhood hand, foot, and mouth disease in Chengdu, China: a distributed lag non-linear analysis. Sci Rep 6:27305
Zha J, Ma Z (2015) Epidemiological and genetic analysis concerning the coxsackievirus A6 related endemic outbreak of hand-foot-mouth disease in Taizhou, China, during 2013. J Med Virol 87(12):2000–2008
Zhang Y, Zhu Z, Yang W, Ren J, Tan X, Wang Y, Mao N, Xu S, Zhu S, Cui A, Zhang Y, Yan D, Li Q, Dong X, Zhang J, Zhao Y, Wan J, Feng Z, Sun J, Wang S, Li D, Xu W (2010) An emerging recombinant human enterovirus 71 responsible for the 2008 outbreak of hand foot and mouth disease in Fuyang city of China. Virol J 7:94
Zhang W, du Z, Zhang D, Yu S, Hao Y (2016) Boosted regression tree model-based assessment of the impacts of meteorological drivers of hand, foot and mouth disease in Guangdong, China. Sci Total Environ 553:366–371
Zhang D et al (2017) Enterovirus 71 neutralizing antibodies Seroepidemiological research among children in Guangzhou, China between 2014 and 2015: a cross-sectional study. Int J Environ Res Public Health 14(3)
Zhou L et al (2015) Clinical feature of severe hand, foot and mouth disease with acute pulmonary edema in pediatric patients. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue 27(7):563–567
Zhu FC, Liang ZL, Meng FY, Zeng Y, Mao QY, Chu K, Song XF, Yao X, Li JX, Ji H, Zhang YJ, Li L, Pan HX, Xu K, Dai WM, Zhang WW, Deng F, Wang H, Wang JZ (2012) Retrospective study of the incidence of HFMD and seroepidemiology of antibodies against EV71 and CoxA16 in prenatal women and their infants. PLoS One 7(5):e37206
Zhu L, Yuan Z, Wang X, Li J, Wang L, Liu Y, Xue F, Liu Y (2015) The impact of ambient temperature on childhood HFMD incidence in inland and coastal area: a two-city study in Shandong Province, China. Int J Environ Res Public Health 12(8):8691–8704
Zhu L, Wang X, Guo Y, Xu J, Xue F, Liu Y (2016) Assessment of temperature effect on childhood hand, foot and mouth disease incidence (0-5years) and associated effect modifiers: a 17 cities study in Shandong Province, China, 2007-2012. Sci Total Environ 551-552:452–459
Funding
This study was supported by the Graduate students’ independent exploration of innovative projects, Central South University (2018zzts849), Health and Medical Science and Technology Scheme of Zhejiang Province (2014KYA202), the Science and Technology Scheme of Ningbo (2014C50027), the Science and Technology Scheme of Health and Family Planning Commission of Hunan Province (BZ2016085), supported by and the Innovation Team of Science and Technology Bureau of Ningbo (2012B82018), the Social Development Research Program of Ningbo (2014C50025), Science and Technology Innovation, Science Popularization Guidance Project of Hunan Province (2016ZK3002).
Author information
Authors and Affiliations
Contributions
H RX, B GL, and H TF conceived and designed the experiments; H RX, B GL, and H TF performed the experiments; H TF and HC N analyzed the data; H RX, HC N, H JA, and X GZ drafted the paper. All authors contributed to the interpretation of the analysis, reviewing the manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study has been approved by the Institutional Review Board of the Ningbo Center for Disease Control. Data analyses were de-identified (number 201601).
Consent for publication
Not applicable.
Conflict of interest
The authors declare that they have no conflicts of interest.
Additional information
Responsible editor: Philippe Garrigues
Rights and permissions
About this article

Cite this article
Huang, R., Ning, H., He, T. et al. Impact of PM10 and meteorological factors on the incidence of hand, foot, and mouth disease in female children in Ningbo, China: a spatiotemporal and time-series study. Environ Sci Pollut Res 26, 17974–17985 (2019). https://doi.org/10.1007/s11356-018-2619-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-018-2619-5