
Abstract
Angiotensin-converting enzyme (ACE) gene has been reported to be one of the candidate genes for endurance performance. The ACE gene insertion/deletion (I/D) polymorphism (rs4646994) is responsible for the variation in the ACE plasma level. The insertion (I allele) of ACE I/D gene polymorphism decreases the level of ACE plasma, thus reducing skeletal muscle vasoconstriction. Skeletal muscle vasoconstriction increases oxygenated blood supply to working muscles for endurance performance. On the other hand, the D allele of ACE I/D gene polymorphism increases the level of ACE plasma, leading to skeletal muscle hypertrophy. Therefore, the D allele may be helpful for strength or power performance. However, evidence for the involvement of these alleles in improving endurance performance and muscle strength is inconsistent and warrants further studies. These inconsistencies may be attributed to the small sample size and the potential causes of the racial and ethnic differences used in the previous studies. Therefore, this brief review reported a summary of the current literature on the association of the ACE I/D gene polymorphism on human physical performance across populations. The findings of this review may serve as a reliable platform and guidance for future research to provide a better understanding of the potential role of this variant on human physical performance concerning ethnicity.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Athletic performance may be affected by various factors, such as skills, training, and genetics. Among these factors, the genetic factor is more likely to have a significant effect on athletic performance, as it influences innate human ability [1]. For instance, Pérusse [1] provided strong evidence that the genetic factor significantly contributes to performance-related traits, including cardiorespiratory endurance and muscle strength. Additionally, the genetic factor accounts for 40–60% variations in aerobic and cardiac functions, 50–90% variations in anaerobic performance, 30% to 70% variations in muscular fitness, and 20–30% variations in cardiac performance [1]. Genetic influence on the physical trait is important for endurance performance, especially for an athlete to excel in sports. For example, sprint performance depends on genetic factors that adapt the body to build strong leg muscles. This body adaptation provides the athlete with several advantages, such as overcoming inertia at the beginning of the sprint, taking long strides, and allowing the calf muscles to work effectively for sprint acceleration [2].
It is an intricate task to understand the genetics of human performance. Solomon et al. [3] defined genetics as a branch of science that studies heredity (genes) and how individuals inherit and transfer the genetic traits from one generation to the next. In other words, humans inherit hereditary characters such as height and skin colour from their parents. A gene is a fundamental component in genetics [4], and it is a part of deoxyribonucleic acid (DNA) that contains particular codes to synthesise a specific protein [5]. The protein is used to build tissues, organs, and finally, an organism [5]. The primary sequence of DNA molecules in the gene sequence encodes the information needed to synthesise a specific protein in the human body [6]. Genes are substantially different in size, where the size ranges from less than 100 base pairs to more than several million base pairs [6]. Many genes exist in various forms (known as an allele) due to mutation that affects the DNA base sequence [7]. Every person has two copies of the alleles of a given gene, whereby each allele is inherited from each parent [7]. Each allele of a given gene (at the same locus or position on the chromosome) has minor differences in its DNA base sequence [7]. Each pair of alleles is the genotype of a specific gene that expresses an individual’s phenotype [6]. An individual that carries the same pair of alleles of a given gene is called homozygous [7]. On the contrary, an individual with a different pair of alleles is called heterozygous [7]. Additionally, different versions of alleles contribute to the various phenotypes or physical characteristics [7]. For instance, previous studies suggested that the differences in physical performance between athletes and non-athletes may be due to genetic variations in specific allele genes [7]. In the future, the knowledge about an individual’s genetic profile will help both athletes and coaches to identify the right sports discipline and prepare a personalised athlete training programme.
Several studies have shown a link between specific genes or variants and human physical performance [8,9,10]. Additionally, the findings from twin studies (controlled for environmental factor) demonstrated that genetic was the main factor that contributed to the physical characteristic needed for a specific sport [11,12,13,14]. To date, 239 genes consisting of 214 autosomal gene entries, plus seven other on the X chromosomes, and 18 mitochondrial genes have been associated with sports performance [15]. Among these candidate genes, it has been suggested that the angiotensin I-converting enzyme (ACE) gene is the most potent candidate gene-related to endurance performance [16].
The ACE gene
In humans, the ACE gene can be found on the long arm (q) of chromosome 17 (17q23.3). As shown in Fig. 1, this gene is 21 kb long and consists of 26 exons and 25 introns [17]. The ACE gene produces ACE [17], which is a key element in the renin-angiotensin (RAS) system that regulates blood pressure, water fluid balance, and tissue growth [18]. In a circulating RAS system, the primary role of ACE is to produce angiotensin II (ANG II) [19], as illustrated in Fig. 2. The ANG II is a potent vasopressor and aldosterone that stimulates angiotensin I peptide (ANG I) [19]. In addition, the ANG II decomposes bradykinin, which is a potent vasodilator [19]. It is also important to note that each individual has different levels of ACE in plasma. However, family members have a similar level of ACE plasma, suggesting that the interindividual variability in the ACE plasma level is determined by genetic factors [20]. Among several polymorphisms of the ACE gene, the ACE I/D gene polymorphism (rs4646994) has a strong association with the ACE plasma level, which accounts for 47% of the overall phenotypic variance of the ACE activity [21] (Figs. 1, 2).

The genomic organization of the ACE gene on the long arm (q) of chromosome 17 on band 23.3. The ACE gene consists of 26 exons and 25 introns

The role of ACE in the circulating renin-angiotensin system (RAS)
The ACE I/D gene polymorphism
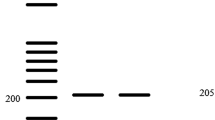
The polymorphism of the ACE I/D gene refers to the insertion (I allele) or deletion (D allele) of 287 base pairs in intron 16 of chromosome 17 [22]. The ACE level in people with two copies of the I allele was reported to be low [21]. The reduced level of ACE led to a decrease in the conversion of ANG I to ANG II, which resulted in less vasoconstriction and increased oxygenated blood circulation to the working muscles [17, 23]. Conversely, individuals with two copies of the D allele had a high ACE level [21]. A high ACE level resulted in a higher ANG II level, increased vasoconstriction, and reduced oxygenated blood flow to the working muscles [17, 23].
The ACE I/D gene polymorphism has three genotypes: (i) the II genotype (low serum ACE levels), (ii) the ID genotype (intermediate ACE serum levels), and (iii) the DD genotype (high ACE serum levels) [21]. Several studies that examined the distribution of ACE I/D gene polymorphism have shown that the allele and genotype frequencies vary across different racial groups [24,25,26,27].
The distribution of ACE I/D gene polymorphism across ethnicity
There has been a difference in the distribution of the ACE I/D gene polymorphism in various racial and ethnic groups in the current literature (Table 1). Among the racial groups, the Black (Australian Aboriginal) population has the highest frequency of the I allele (0.97) [28], whereas the Caucasian population has the highest frequency of the D allele (0.77) [29]. The distribution patterns of the I and D alleles in the Black community were approximately 0.97 to 0.27 and 0.73 to 0.03, respectively. Additionally, the Australian Aboriginal minority ethnic group in the Black population was found to have the highest prevalence of I allele than other Black ethnic groups [28]. Also, the D allele was the most common among Nigerians [25] and Somalis [30]. The trend among Amerindians [31], on the other hand, was closely similar to that of Pima Indians [32], Coastal Papua New Guineans [33], Sothos [34], Mulattos [35], and Alaska Natives [34].
For the Caucasian population, the concentrations of I and D alleles ranged from 0.78 to 0.23 and 0.77 to 0.22, respectively. Among the Caucasians, the highest frequency of the I allele was observed for the Mexicans [31], whereas the highest frequency of the D allele was observed for the Europeans [29]. Nevertheless, the presence of I allele was uncommon among the European [29] and the Middle East populations, such as the Egyptians [36] and Omanis [37]. Besides, the presence of I allele among Mexicans [31] was observed to be closely related to the European population [38]. Also, the highest frequency of the D allele observed among Europeans [29] was relatively similar to that reported for Egyptians [36] and Omanis [37]. The ACE I/D gene polymorphism trend in the Australian population [28, 39] was the same as that reported for the Brazilian [35] and European [40] populations. Nevertheless, findings from several studies of the same ethnic group, such as Turkish, have been consistently similar [41,42,43,44]. However, research on the European population has shown inconsistent results. For example, the frequency of the I allele in the European population reported by Cambien et al. [38] was inconsistent with other studies; 0.23 [29], 0.43 [45], and 0.51 [26].
In the Asian population, the I and D alleles ranged from 0.76 to 0.42 and 0.58 to 0.24, respectively. The highest frequency of the I allele was observed for the Javanese ethnic group [46], whereas the highest frequency of the D allele was observed for the Kazakh ethnic group [47]. In a study by Jayapalan et al. [27], they investigated the various ethnic groups in Malaysia. It was observed that the highest frequency of the I allele was among the Malays, whereas the highest frequency of the D allele was among the Indians [27]. Furthermore, the frequency of the I allele observed among the Malays was significantly comparable to Thai [48], Singaporean Chinese [49], and Javanese [46]. In contrast, the frequency of the D allele observed among the Malaysian Indians was equivalent to other Indian ethnic groups in Asia [50, 51].
The trend observed among the Chinese population in Malaysia has also been significantly similar to the trend observed for the Hong Kong Chinese [52], Taiwanese [53], and Japanese [54]. The study by Yusof et al. [55] on the Malaysian population supports previous findings on ACE I/D gene polymorphism distribution across ethnic groups. Specifically, Yusof et al. [55] found that both the Malay and Chinese ethnic groups had a higher frequency of the D allele than the Indian and other native groups. The results reported by Yusof et al. [55] differ from the previous study carried out on the Malaysian population [27]. Additionally, Yusof et al. [55] reported that the frequency of the I allele in the Malaysian population was highest among the Malay ethnic group (0.66), followed by the Chinese ethnic group (0.53), Indian ethnic group (0.46), and the lowest frequency in the other native groups (0.41). The distribution pattern of ACE I/D gene polymorphism reported by Yusof et al. [55] for the Malay ethnic group was remarkably similar to that of Japanese [56] and Taiwanese [53] populations. The frequency of the I allele in other native groups was among the lowest reported among Asians and was similar to the rate observed among the Caucasian population [42, 57]. Concerning current evidence for ACE I/D gene polymorphism, ethnicity appears to play an essential role in the distribution of ACE I/D polymorphism, as suggested by Barley et al. [24]. Overall, these findings indicate that ACE I/D gene polymorphism may have a different effect on human physical performance or health in other populations, as documented for the Caucasian population.
The various distribution patterns of ACE I/D gene polymorphism in different ethnic groups are consistent with the previous studies on the effects of ACE I/D gene polymorphisms on disease sensitivities [54,55,56,57,58,59,60]. For example, Ng et al. [58] found that the association of ACE I/D gene polymorphism with diabetic nephropathy was more prevalent in the Asian population than the Caucasian population. Based on the data from the distributions of ACE I/D gene polymorphism in general populations across the world and research on the effects of ACE I/D gene polymorphism on susceptibility to diseases, it can be assumed that the effect of ACE I/D gene polymorphism on human physical performance may also vary depending on ethnicity. However, this assumption remains inconclusive due to insufficient comparative analysis across ethnic groups [16, 59]. A recent meta-analysis study has shown that the effect of ACE I/D gene polymorphism on human physical performance has been documented mostly for the Caucasian population and less for the Asian population [16].
Therefore, further studies involving the Asian population are warranted to understand the differences of ACE I/D gene polymorphism across ethnic groups. This effort is important as preliminary data indicated that the differential effects of ACE I/D gene polymorphism may influence individual variation in response to training [60,61,62,63,64]. For example, the ACE I/D gene polymorphism has affected adaptation to weight-lifting and walking [64], isometric, and dynamic leg training [61], as well as aerobic exercise [60, 62, 63]. These studies showed that people with the same ACE I/D polymorphism genotype had similar responses to training. Additionally, several studies have shown that blood pressure varies among people with different ACE I/D alleles or genotypes during a health management exercise training [60, 63, 66]. For example, Hagberg et al. [60] showed that the I allele carriers had a lower systolic and diastolic blood pressure after 9 months of exercise training than the D allele carriers [60]. Additionally, the maximum oxygen intake capacity (VO2 max) measured during incremental exercise was 75% to 85% more for the I allele carriers than the D allele carriers [60]. In relation to these findings, more studies should be done to obtain the prevalence data of ACE I/D gene polymorphism in different ethnic groups to confirm the interactive effects of ethnicity and ACE I/D gene polymorphism on human physical performance, especially among the Asian population.
I allele and endurance performance
Several studies have reported the additive effect of I allele on human physical performance. A study by Gayagay et al. [66] on 64 Australian national rowers was the first study to successfully show the additive effect of the I allele on endurance performance. They found that the frequency of the I allele was more prevalent in rowers compared with the controls. In another study, Montgomery et al. [67] reported a similar result for 33 elite high-altitude male mountaineers and 1,906 British military male recruits. They found that the recruits with the II genotype displayed an 11 fold improvement after a 10-week general physical training programme relative to the DD genotype carriers [67]. Since the discovery, the ACE gene has attracted worldwide attention as a candidate gene for endurance performance [3].
The presence of the I allele was more prominent among endurance athletes [68,69,70,71], rowers [66, 72], triathletes [73, 74], and long-distance swimmers [75]. It has also been reported that individuals with the I allele have higher VO2 max [76, 77], higher slow-twitch muscle fibre [78], higher cardiac output [79], and higher heat tolerance [80] compared to individuals with the D allele. Also, some studies have attempted to determine whether the possession of I allele would improve training adaptations. In contrast to the D allele carriers, studies have shown that the I allele carriers can improve their mechanical performance after 11-week of the aerobic training programme [62], enhance aortic distensibility through chronic long-term training [81], increase adherence to 6-month training by 60% and increase the mean exercise capacity by up to 85% [82], and expand training progress up to 6 months [83].
Although the results mentioned above are convincing, the impact of the I allele on endurance performance has not been well-established, as several studies failed to replicate the link between I allele and the status of endurance athletes [84,85,86,87,88,89,90,91]. Moreover, several cross-sectional studies have shown that people with D alleles have better endurance [89] and VO2 max values [92] than those with I alleles. Also, the VO2 max of individuals with the DD genotype increased by 14% to 38% after the exercise training programme compared to those with the II genotype [93].
There is no known reason for these inconsistent findings. The ethnicity factor could be one of the factors that contributed to these inconsistencies. Furthermore, previous reports show that the distribution of ACE I/D gene polymorphism varies between ethnic groups. Therefore, to control for potential bias, population-specific research is warranted to confirm the impact of I allele possession on endurance performance. Furthermore, to date, there are only a few studies on the additive effect of I allele on endurance performance among Asians (e.g. Malaysian population) compared to the Caucasian population [16]. This limited set of data raises the question of whether the effect of I allele possession on endurance performance that was previously reported for Caucasians will also be seen for the Asian population (e.g. Malaysian population). In a previous study, Goh et al. [77] studied the impact of Asian ethnicity (i.e. Singaporean) on the effect of ACE I/D gene polymorphism on aerobic capacity. From the study, it has been suggested that the ACE I/D gene polymorphism can have a universal impact on human physical performance, irrespective of ethnicity.
Nonetheless, Yusof et al. [94] found that the presence of I allele is not a predictor of endurance performance in a multi-ethnic group of Malaysians, although the presence of I allele was consistent with the stamina status among the Malaysian population. This finding was based on the results of the Yo-Yo intermittent level 2 test [94]. Specifically, it was found that the score for the Yo-Yo intermittent recovery level 2 was similar in all three ACE I/D genotype groups [94]. However, the results of Geisterfer et al. [96] contradict those of earlier Asian [77] and Caucasian [83, 95] studies, indicating that individuals with the II genotype have greater durability than those with other genotypes (Table 2).
Given the above findings, future studies may extend the current research by running a larger sample size to confirm the possession of the I allele on endurance performance. Table 2 provides a summary of studies investigating the effect of I allele possession on endurance performance.
D allele and Strength/power performance
The D allele of ACE I/D gene polymorphism was thought to influence strength or power due to the increased level of ACE activity in a person with the D allele [96, 97]. The elevated ACE activity will increase the development of ANG II (a strong growth factor in cardiac and vascular tissue) in the skeletal muscle RAS, which is the potential mechanism for triggering muscle cell growth and hypertrophy [96, 97]. Several studies have, therefore, tried to assess the effect of D allele possession on strength or power output. The D allele carriers have been reported to have the highest muscle strength compared to the I allele carriers [98,99,100]. Additionally, several case–control studies have found that the prevalence of D allele was higher among athletes who participated in strength or power-oriented events [101,102,103,104,105,106].
Montgomery et al. [107] reported an increase in the left ventricular mass in male Caucasian military recruits after ten weeks of physical training. The development of the left ventricle was seen highest in the recruits with the DD genotype compared to other recruits with the II and ID genotypes [107]. The D allele possession may have damage protecting effects on the muscles as subjects with the DD genotype were reported to have lower blood creatine kinase values than other genotype carriers in response to eccentric contractions [108]. In the meantime, Folland et al. [61] reported that young adult men with a D allele have more strength gains after nine weeks of strength training than those with the I allele. Enhanced power following 18 months of walking and lightweight training has also been seen in older people with the DD genotype compared to other genotypes [64].
Taken together, the possession of the D allele on strength performance remains inconclusive as previous studies have shown inconsistent findings [90, 105, 109,110,111,112,113,114,115]. There are no known reasons for these inconsistencies, but they may be due to ethnicity and limited reports on the impact of D allele possession on strength or power performance from Asian populations, such as Malaysia [16]. A study by Yusof et al. [94] on the multiple ethnic groups of the Malaysian population showed that the D allele was over-represented among strength or power athletes compared to other groups of athletes. This finding was consistent with the previous observations from other Asian [104] and Caucasian [100, 101, 116] samples. Additionally, Yusof et al. [94] showed that athletes with the DD genotype exhibited greater leg strength than those with the II and ID genotypes. The results from Yusof et al. [94] were in line with the previous research reporting that the D allele has positive effects on the muscle strength parameters, such as muscle strength [99] and knee extensor strength [64]. These results provide promising evidence that the possession of the D allele could have a beneficial effect on short-term and high-intensity activities. The potential mechanism underlying the positive impact of the D allele possession on muscle strength is through the integration of the ANG II into the skeletal muscle [117]. It has been reported that greater production of local ANG II increases protein synthesis and cell hypertrophy in the skeletal muscle, thereby contributing to the maximum power of muscle contraction [118]. Table 3 summarises the list of studies that examined the effects of the D allele on strength or power output.
Discussion
The present review included the existing literature on the impact of ACE I/D gene polymorphism on human physical performance by considering the ethnicity factor. The distribution of ACE I/D gene polymorphism varies greatly between different ethnic groups. This finding suggests that the effects of ACE I/D gene polymorphism on human physical performance may differ between individuals of different ethnic groups. However, the results of the current literature should be interpreted with caution as other factors can influence the results. The first limitation of the previous studies was the small number of samples included in the analysis. Most studies did not use an adequate number of samples to detect a specified difference. Therefore, the current results cannot be generalised to the population as the sample size is small. The second limitation was that the previous studies did not control for gender. Most studies included both females and males, and therefore, it is not clear whether gender influences the ACE I/D gene polymorphism. The third limitation was that the findings reported in most studies could also be influenced by the exercise impact that masks gene-related effects on physical performance.
Therefore, future studies are needed to ensure that the study participants are sufficiently homogeneous in terms of age, gender, physical characteristics, and health conditions. Additionally, future studies should ensure that the ethnic effects are restricted and ethically regulated. Future studies must also follow the latest genomic studies and training recommendations. All experimental approaches including case studies, cross-sectional studies, and intervention studies must be implemented to demonstrate the relationship between human physical performance and ACE I/D gene polymorphism [119]. To ensure accurate and objective genetic evaluation, the genotype distributions of the ACE I/D gene polymorphism examined must be in Hardy Weinberg equilibrium.
Based on the current literature, future studies should address the following research questions:
1. Does ACE I/D gene polymorphism interact with other variants that affect human physical performance?
2. Does ACE I/D gene polymorphism vary in its effect on human physical performance?
3. What is the potential mechanism behind the impact of ACE I/D gene polymorphism on human physical performance?
References
Pérusse L (2011) Role of genetics factors in sport performance: evidence from family studies. In: Bouchard C, Hoffman E (eds) Genetic and molecular aspects of sport performance, vol XVIII. The Encyclopaedia of Sports Medicine an IOC Medical Commission Publication, Wiley-Blackwell Publishing Ltd
Coh M, Milanovic D, Kampmiller T (2001) Morphologic and kinematic characteristics of elite sprinters. Coll Antropol 25(2):605–610
Solomon EP, Berg LR, Martin DW (2010) Biology: cengage learning
Long M, Souza SJd (1998) Advances in genome biology genes and genomes. Part 1(5):169
Alcamo IE (2000) The roots of DNA research. DNA technology: the awesome skill, 2 edn. Gulf Professional Publishing
Winter PC, Hickey GI, Fletcher HL (2002) Instant notes in genetics, 2nd edn. BIOS Scientific Publishers Limited, Springer
Lodish H, Berk A, Matsudaira P, Kaiser CA, Krieger M, Scott MP, Zipursky L, Darnell J (2008) Molecular Cell Biology. Freeman, W. H
Bouchard C, Malina RM, Pérusse L (1997) Genetics of fitness and physical performance. Human Kinetics, Champaign, IL
MacArthur DG, North KN (2005) Genes and human elite athletic performance. Hum Genet 116(5):331–339. https://doi.org/10.1007/s00439-005-1261-8
Bouchard C, Hoffman E (2011) Genetic and molecular aspects of sport performance, vol XVIII. Blackwell Publishing Ltd. https://doi.org/10.1002/9781444327335
Chatterjee S, Das N (1995) Physical and motor fitness in twins. Jpn J Physiol 45(3):519–534
Calvo M, Rodas G, Vallejo M, Estruch A, Arcas A, Javierre C, Viscor G, Ventura JL (2002) Heritability of explosive power and anaerobic capacity in humans. Eur J Appl Physiol 86(3):218–225
Maridaki M (2006) Heritability of neuromuscular performance and anaerobic power in preadolescent and adolescent girls. J Sports Med Phys Fitness 46(4):540–547
Alonso L, Souza E, Oliveira M, do Nascimento L, Dantas P (2014) Heritability of aerobic power of individuals in northeast Brazil. Biol Sport 31(4):267–270. https://doi.org/10.5604/20831862.1120933
Bray MS, Hagberg JM, Pérusse L, Rankinen T, Roth SM, Wolfarth B, Bouchard C (2009) The human gene map for performance and health-related fitness phenotypes. Med Sci Sports Exerc 41(1):35–73. https://doi.org/10.1249/MSS.0b013e3181844179
Ma F, Yang Y, Li X, Zhou F, Gao C, Li M, Gao L (2013) The association of sport performance with ACE and ACTN3 genetic polymorphisms: a systematic review and meta-analysis. PLoS ONE 8(1):e54685. https://doi.org/10.1371/journal.pone.0054685
Sayed-Tabatabaei FA, Oostra BA, Isaacs A, van Duijn CM, Witteman JC (2006) ACE polymorphisms. Circ Res 98(9):1123–1133. https://doi.org/10.1161/01.RES.0000223145.74217.e7
Silverthorn DU (2007) Human physiology: an integrated approach, 4th edn. Pearson/Benjamin Cummings
Coates (2003) The angiotensin converting enzyme (ACE). Int J Biochem Cell Biol 35(6):769–773. https://doi.org/10.1016/s1357-2725(02)00309-6
Cambien F, Alhenc-Gelas F, Herbeth B, Andre JL, Rakotovao R, Gonzales MF, Allegrini J, Bloch C (1988) Familial resemblance of plasma angiotensin-converting enzyme level: the Nancy study. Am J Hum Genet 43(5):774–780
Rigat B, Hubert C, Alhenc-Gelas F, Cambien F, Corvol P, Soubrier F (1990) An insertion/deletion polymorphism in the angiotensin I-converting enzyme gene accounting for half the variance of serum enzyme levels. J Clin Investig 86(4):1343–1346. https://doi.org/10.1172/JCI114844
Rigat B, Hubert C, Corvol P, Soubrier F (1992) PCR detection of the insertion/deletion polymorphism of the human angiotensin converting enzyme gene (DCP1) (dipeptidyl carboxypeptidase 1). Nucleic Acids Res 20(6):1433
Jones A, Woods DR (2003) Skeletal muscle RAS and exercise performance. Int J Biochem Cell Biol 35(6):855–866
Barley J, Blackwood A, Carter ND, Crews DE, Cruickshank JK, Jeffery S, Ogunlesi AO, Sagnella GA (1994) Angiotensin converting enzyme insertion/deletion polymorphism: association with ethnic origin. J Hypertens 12(8):955–957
Batzer MA, Stoneking M, Alegria-Hartman M, Bazan H, Kass DH, Shaikh TH, Novick GE, Ioannou PA, Scheer WD, Herrera RJ et al (1994) African origin of human-specific polymorphic Alu insertions. Proc Natl Acad Sci USA 91(25):12288–12292
Batzer MA, Arcot SS, Phinney JW, Alegria-Hartman M, Kass DH, Milligan SM, Kimpton C, Gill P, Hochmeister M, Ioannou PA, Herrera RJ, Boudreau DA, Scheer WD, Keats BJ, Deininger PL, Stoneking M (1996) Genetic variation of recent Alu insertions in human populations. J Mol Evol 42(1):22–29
Jayapalan JJ, Muniandy S, Chan SP (2008) Angiotensin-1 converting enzyme I/D gene polymorphism: scenario in Malaysia. Southeast Asian J Trop Med Public Health 39(5):917–921
Lester S, Heatley S, Bardy P, Bahnisch J, Bannister K, Faull R, Clarkson A (1999) The DD genotype of the angiotensin-converting enzyme gene occurs in very low frequency in Australian Aboriginal. Nephrol Dial Transplant 14(4):887–890
Tiret L, Rigat B, Visvikis S, Breda C, Corvol P, Cambien F, Soubrier F (1992) Evidence, from combined segregation and linkage analysis, that a variant of the angiotensin I-converting enzyme (ACE) gene controls plasma ACE levels. Am J Hum Genet 51(1):197–205
Bayoumi RA, Simsek M, Yahya TM, Bendict S, Al-Hinai A, Al-Barwani H, Hassan MD (2006) Insertion deletion polymorphism in the angiotensin-converting enzyme (ACE) gene among Sudanese, Somalis, Emiratis, and Omanis. Hum Biol 78:103–108
Vargas-Alarcon G, Hernandez-Pacheco G, Rodriguez-Perez JM, Perez-Hernandez N, Pavon Z, Fragoso JM, Juarez-Cedillo T, Villarreal-Garza C, Granados J (2003) Angiotensin-converting enzyme gene (ACE) insertion/deletion polymorphism in Mexican populations. Hum Biol 75(6):889–896
Foy CA, McCormack LJ, Knowler WC, Barrett JH, Catto A, Grant PJ (1996) The angiotensin-I converting enzyme (ACE) gene I/D polymorphism and ACE levels in Pima Indians. J Med Genet 33(4):336–337
Perna NT, Batzer MA, Deininger PL, Stoneking M (1992) Alu insertion polymorphism: a new type of marker for human population studies. Hum Biol 64(5):641–648
Rupert JL, Kidd KK, Norman LE, Monsalve MV, Hochachka PW, Devine DV (2003) Genetic polymorphisms in the renin-angiotensin system in high-altitude and low-altitude native American populations. Ann Hum Genet 67(1):17–25
Pereira AC, Mota GA, Bensenor I, Lotufo PA, Krieger JE (2001) Effect of race, genetic population structure, and genetic models in two-locus association studies: clustering of functional renin-angiotensin system gene variants in hypertension association studies. Braz J Med Biol Res 34(11):1421–1428
Ulu A, Elsobky E, Elsayed M, Yıldız Z, Tekin M, Akar N (2006) Frequency of five thrombophilic polymorphisms in the Egyptian population. Turk J Hematol 23:100–103
Wang JG, Staessen JA (2000) Genetic polymorphisms in the renin-angiotensin system: relevance for susceptibility to cardiovascular disease. Eur J Pharmacol 410(2–3):289–302
Cambien F, Poirier O, Lecerf L, Evans A, Cambou JP, Arveiler D, Luc G, Bard JM, Bara L, Ricard S, Tiret L, Amouyel P, Alhencs-Gelas F, Soubrier F (1992) Deletion polymorphism in the gene for angiotensin-converting enzyme is a potent risk factor for myocardial infarction. Nature 359(6396):641–644
Lea RA, Ovcaric M, Sundholm J, Solyom L, Macmillan J, Griffiths LR (2005) Genetic variants of angiotensin converting enzyme and methylenetetrahydrofolate reductase may act in combination to increase migraine susceptibility. Brain Res Mol Brain Res 136(1–2):112–117. https://doi.org/10.1016/j.molbrainres.2005.01.006
Renner W, Pabst E, Paulweber B, Malaimare L, Iglseder B, Wascher TC, Pilger E (2002) The angiotensin-converting-enzyme insertion/deletion polymorphism is not a risk factor for peripheral arterial disease. Atherosclerosis 165(1):175–178
Erdoğan H, Mir S, Serdaroğlu E, Berdeli A, Aksu N (2004) Is ACE gene polymorphism a risk factor for renal scarring with low-grade reflux? Pediatr Neurol 19(7):734–737
Cam FS, Colakoglu M, Sekuri C, Colakoglu S, Sahan C, Berdeli A (2005) Association between the ACE I/D gene polymorphism and physical performance in a homogeneous non-elite cohort. Can J Appl Physiol 30(1):74–86
Sipahi T, Budak M, Şen S, Ay A, Şener S (2006) Association between ACE gene insertion (I)/deletion (D) polymorphism and primary hypertension in Turkish patients of Trakya region. Biotechnol Biotec Eq 20(2):104–108
Berdeli A, Cam FS (2009) Prevalence of the angiotensin I converting enzyme gene insertion/deletion polymorphism in a healthy Turkish population. Biochem Genet 47(5–6):412–420. https://doi.org/10.1007/s10528-009-9240-8
Vassilikioti S, Doumas M, Douma S, Petidis K, Karagiannis A, Balaska K, Vyzantiadis A, Zamboulis C (1996) Angiotensin converting enzyme gene polymorphism is not related to essential hypertension in a Greek population. Am J Hypertens 9(7):700–702
Sasongko TH, Sadewa AH, Kusuma PA, Damanik MP, Lee MJ, Ayaki H, Nozu K, Goto A, Matsuo M, Nishio H (2005) ACE gene polymorphism in children with nephrotic syndrome in the Indonesian population. Kobe J Med Sci 51(3–4):41–47
Aĭtkhozhina NA, Liudvikova EK (2003) Polymorphism of the promoter region of the angiotensinogen gene and the gene for angiotensin I-converting enzyme in arterial hypertension and cardiovascular disease of the Kazakh ethnic group. Genetika 39(2):293–299
Nitiyanant W, Sriussadaporn S, Ploybutr S, Watanakejorn P, Tunlakit M, Bejrachandra S (1997) Angiotensin converting enzyme gene polymorphism in healthy Thais and patients with non-insulin dependent diabetes mellitus. J Med Assoc Thai 80(12):747–752
Lee EJD (1994) Population genetics of the angiotensin-converting enzyme in Chinese. Br J clin Pharmac 37:212–214
Saha N, Talmud PJ, Tay JSH, Humphries SE, Basair J (1996) Lack of association of angiotensin converting enzyme (ACE). Gene insertion/deletion polymorphism with CAD in two Asian populations. Clin Genet 50:121–125
Movva S, Alluri RV, Komandur S, Vattam K, Eppa K, Mukkavali KK, Mubigonda S, Saharia S, Shastry JC, Hasan Q (2007) Relationship of angiotensin-converting enzyme gene polymorphism with nephropathy associated with Type 2 diabetes mellitus in Asian Indians. J Diabetes Complicat 21(4):237–241. https://doi.org/10.1016/j.jdiacomp.2006.07.001
Young RP, Sanderson JE, Tomlinson B, Woo KS, Critchley JA (1995) Angiotensin converting enzyme insertion-deletion polymorphism in Chinese. J Hypertens 13(12 Pt 1):1479–1480
Chuang LM, Chiu KC, Chiang FT, Lee KC, Wu HP, Lin BJ, Tai TY (1997) Insertion/deletion polymorphism of the angiotensin I-converting enzyme gene in patients with hypertension, non-insulin-dependent diabetes mellitus, and coronary heart disease in Taiwan. Metab Clin Exp 46(10):1211–1214
Tamaki S, Nakamura Y, Tsujita Y, Nozaki A, Amamoto K, Kadowaki T, Kita Y, Okamura T, Iwai N, Kinoshita M, Ueshima H (2002) Polymorphism of the angiotensin converting enzyme gene and blood pressure in a Japanese general population (the Shigaraki Study). Hypertens Res 25(6):843–848
Yusof HA, Zainuddin Z, Rooney K, Muhamed AMC (2017) Distributions of ace I/D and ACTN3 R/X gene polymorphisms in multi-ethnic Malaysian and Australian populations. Inte J Public Health Clin Sci 4(5):125–138
Matsubara M, Suzuki M, Fujiwara T, Kikuya M, Metoki H, Michimata M, Araki T, Kazama I, Satoh T, Hashimoto J, Hozawa A, Ohkubo T, Tsuji I, Katsuya T, Higaki J, Ogihara T, Satoh H, Imai Y (2002) Angiotensin-converting enzyme I/D polymorphism and hypertension: the Ohasama study. J Hypertens 20(6):1121–1126
Ferrieres J, Ruidavets JB, Fauvel J, Perret B, Taraszkiewicz D, Fourcade J, Nieto M, Chap H, Puel J (1999) Angiotensin I-converting enzyme gene polymorphism in a low-risk European population for coronary artery disease. Atherosclerosis 142(1):211–216
Ng DP, Tai BC, Koh D, Tan KW, Chia KS (2005) Angiotensin-I converting enzyme insertion/deletion polymorphism and its association with diabetic nephropathy: a meta-analysis of studies reported between 1994 and 2004 and comprising 14,727 subjects. Diabetologia 48(5):1008–1016. https://doi.org/10.1007/s00125-005-1726-2
Zilberman-Schapira G, Chen J, Gerstein M (2012) On sports and genes. Recent Pat DNA Gene Seq 6:180–188
Hagberg JM, Ferrell RE, Dengel DR, Wilund KR (1999) Exercise training-induced blood pressure and plasma lipid improvements in hypertensives may be genotype dependent. Hypertension 34(1):18–23
Folland J, Leach B, Little T, Hawker K, Myerson S, Montgomery H, Jones D (2000) Angiotensin-converting enzyme genotype affects the response of human skeletal muscle to functional overload. Exp Physiol 85(5):575–579
Williams AG, Rayson MP, Jubb M, World M, Woods DR, Hayward M, Martin J, Humphries SE, Montgomery HE (2000) The ACE gene and muscle performance. Nature 403(6770):614. https://doi.org/10.1038/35001141
Zhang B, Sakai T, Miura S, Kiyonaga A, Tanaka H, Shindo M, Saku K (2002) Association of angiotensin-converting-enzyme gene polymorphism with the depressor response to mild exercise therapy in patients with mild to moderate essential hypertension. Clin Genet 62(4):328–333 (cge620414[pii])
Giaccaglia V, Nicklas B, Kritchevsky S, Mychalecky J, Messier S, Bleecker E, Pahor M (2008) Interaction between angiotensin converting enzyme insertion/deletion genotype and exercise training on knee extensor strength in older individuals. Int J Sports Med 29(1):40–44
Kim K (2009) Association of angiotensin-converting enzyme insertion/deletion polymorphism with obesity, cardiovascular risk factors and exercise-mediated changes in Korean women. Eur J Appl Physiol 105(6):879–887. https://doi.org/10.1007/s00421-008-0973-6
Gayagay G, Yu B, Hambly B, Boston T, Hahn A, Celermajer DS, Trent RJ (1998) Elite endurance athletes and the ACE I allele - the role of genes in athletic performance. Hum Genet 103(1):48–50. https://doi.org/10.1007/s004390050781
Montgomery HE, Marshall R, Hemingway H, Myerson S, Clarkson P, Dollery C, Hayward M, Holliman DE, Jubb M, World M, Thomas EL, Brynes AE, Saeed N, Barnard M, Bell JD, Prasad K, Rayson M, Talmud PJ, Humphries SE (1998) Human gene for physical performance. Nature 393(6682):221–222. https://doi.org/10.1038/30374
Myerson S, Hemingway H, Budget R, Martin J, Humphries S, Montgomery H (1999) Human angiotensin I-converting enzyme gene and endurance performance. J Appl Physiol 87(4):1313–1316
Alvarez R, Terrados N, Ortolano R, Iglesias-Cubero G, Reguero JR, Batalla A, Cortina A, Fernandez-Garcia B, Rodriguez C, Braga S, Alvarez V, Coto E (2000) Genetic variation in the renin-angiotensin system and athletic performance. Eur J Appl Physiol 82(1–2):117–120. https://doi.org/10.1007/s004210050660
Hruskovicova H, Dzurenkova D, Selingerova M, Bohus B, Timkanicova B, Kovacs L (2006) The angiotensin converting enzyme I/D polymorphism in long distance runners. J Sports Med Phys Fitness 46(3):509–513
Min S-K, Takahashi K, Ishigami H, Hiranuma K, Mizuno M, Ishii T, Kim C-S, Nakazato K (2009) Is there a gender difference between ACE gene and race distance? Appl Physiol Nutr Metab 34(5):926–932. https://doi.org/10.1139/h09-097
Ahmetov II, Popov DV, Astratenkova IV, Druzhevskaya AM, Missina SS, Vinogradova OL, Rogozkin VA (2008) The use of molecular genetic methods for prognosis of aerobic and anaerobic performance in athletes. Hum Physiol 34(3):338–342. https://doi.org/10.1134/s0362119708030110
Collins M, Xenophontos SL, Cariolou MA, Mokone GG, Hudson DE, Anastasiades L, Noakes TD (2004) The ACE gene and endurance performance during the South African Ironman Triathlons. Med Sci Sports Exerc 36(8):1314–1320
Shenoy S, Tandon S, Sandhu J, Bhanwer AS (2010) Association of angiotensin converting enzyme gene polymorphism and Indian army triathletes performance. Asian J Sports Med 1(3):143–150
Tsianos G, Sanders J, Dhamrait S, Humphries S, Grant S, Montgomery H (2004) The ACE gene insertion/deletion polymorphism and elite endurance swimming. Eur J Appl Physiol 92(3):360–362. https://doi.org/10.1007/s00421-004-1120-7
Hagberg JM, Ferrell RE, McCole SD, Wilund KR, Moore GE (1998) VO2 max is associated with ACE genotype in postmenopausal women. J Appl Physiol 85(5):1842–1846
Goh KP, Chew K, Koh A, Guan M, Wong YS, Sum CF (2009) The relationship between ACE gene ID polymorphism and aerobic capacity in Asian rugby players. Singapore Med J 50(10):997–1003
Zhang B, Tanaka H, Shono N, Miura S, Kiyonaga A, Shindo M, Saku K (2003) The I allele of the angiotensin-converting enzyme gene is associated with an increased percentage of slow-twitch type I fibers in human skeletal muscle. Clin Genet 63:139–144
Hagberg JM, McCole SD, Brown MD, Ferrell RE, Wilund KR, Huberty A, Douglass LW, Moore GE (2002) ACE insertion/deletion polymorphism and submaximal exercise hemodynamics in postmenopausal women. J Appl Physiol 92(3):1083–1088. https://doi.org/10.1152/japplphysiol.00135.2001
Heled Y (2004) Human ACE I/D polymorphism is associated with individual differences in exercise heat tolerance. J Appl Physiol 97(1):72–76. https://doi.org/10.1152/japplphysiol.01087.2003
Tanriverdi H, Evrengul H, Kaftan A, Dursunoglu D, Turgut S, Akda B, Kiliç M (2005) Effects of angiotensin-converting enzyme polymorphism on aortic elastic parameters in athletes. Cardiology 104:113–119
Thompson PD, Tsongalis GJ, Ordovas JM, Seip RL, Bilbie C, Miles M, Zoeller R, Visich P, Gordon P, Angelopoulos TJ, Pescatello L, Moyna N (2006) Angiotensin-converting enzyme genotype and adherence to aerobic exercise training. Prev Cardiol 9(1):21–24
Cam S, Colakoglu M, Colakoglu S, Sekuri C, Berdeli A (2007) ACE I/D gene polymorphism and aerobic endurance development in response to training in a non-elite female cohort. J Sports Med Phys Fitness 47(2):234–238
Taylor RR, Mamotte CD, Fallon K, van Bockxmeer FM (1999) Elite athletes and the gene for angiotensin-converting enzyme. J Appl Physiol 87(3):1035–1037
Rankinen T, Wolfarth B, Simoneau JA, Maier-Lenz D, Rauramaa R, Rivera MA, Boulay MR, Chagnon YC, Pérusse L, Keul J, Bouchard C (2000) No association between the angiotensin-converting enzyme ID polymorphism and elite endurance athlete status. J Appl Physiol 88:1571–1575
Scott RA, Moran C, Wilson RH, Onywera V, Boit MK, Goodwin WH, Gohlke P, Payne J, Montgomery H, Pitsiladis YP (2005) No association between Angiotensin converting enzyme (ACE) gene variation and endurance athlete status in Kenyans. Comp Biochem Physiol A Mol Integr Physiol 141(2):169–175. https://doi.org/10.1016/j.cbpb.2005.05.001
Oh SD (2007) The distribution of I/D polymorphism in the ACE gene among Korean male elite athletes. J Sports Med Phys Fitness 47(2):250–254
Amir O, Amir R, Yamin C, Attias E, Eynon N, Sagiv M, Meckel Y (2007) Human, environmental & exercise: the ACE deletion allele is associated with Israeli elite endurance athletes. Exp Physiol 92(5):881–886. https://doi.org/10.1113/expphysiol.2007.038711
Tobina T, Michishita R, Yamasawa F, Zhang B, Sasaki H, Tanaka H, Saku K, Kiyonaga A (2010) Association between the angiotensin I-converting enzyme gene insertion/deletion polymorphism and endurance running speed in Japanese runners. J Physiol Sci 60(5):325–330. https://doi.org/10.1007/s12576-010-0100-4
Gineviciene V, Pranculis A, Jakaitiene A, Milasius K, Kucinskas V (2011) Genetic variation of the human ACE and ACTN3 genes and their association with functional muscle properties in Lithuanian elite athletes. Medicina (Kaunas) 47(5):284–290 (1105-06e[pii])
Ash GI, Scott RA, Deason M, Dawson TA, Wolde B, Bekele Z, Teka S, Pitsiladis YP (2011) No association between ACE gene variation and endurance athlete status in Ethiopians. Med Sci Sports Exerc 43(4):590–597. https://doi.org/10.1249/MSS.0b013e3181f70bd6
Zhaoa B, Moochhalaa SM, Thama S-y, Lua J, Chiab M, Byrnea C, Hub Q, Leea LKH (2003) Relationship between angiotensin-converting enzyme ID polymorphism and VO2max of Chinese males. Life Sci 73:2625–2630
Rankinen T, Pérusse L, Gagnon J, Chagnon YC, Leon AS, Skinner JS, Wilmore JH, Rao DC, Bouchard C (2000) Angiotensin-converting enzyme ID polymorphism and fitness phenotype in the HERITAGE Family Study. J Appl Physiol 88(3):1029–1035
Yusof HA, Singh R, Zainuddin Z, Rooney K, Muhammed AMC (2015) The angiotensin I-converting enzyme I/D gene polymorphism in well-trained Malaysian athletes. Sport Sci Health 11:187. https://doi.org/10.1007/s11332-015-0222-4
Voroshin IN, Astratenkova IV (2008) Dependence of endurance performance on ACE gene polymorphism in athletes. Hum Physiol 34(1):117–119. https://doi.org/10.1134/s0362119708010180
Geisterfer AAT, Peach MJ, Owens GK (1998) Angiotensin II induces hypertrophy, not hyperplasia, of cultured rat aortic smooth muscle cells. Circ Res 62(4):749–756
Kai T, Shimada S, Sugimura K, Kurooka A, Takenaka T, Fukamizu A, Murakami K, Ishikawa K (1998) Tissue-localized angiotensin II enhances cardiac and renal disorders in Tsukuba hypertensive mice. J Hypertens 16(12 Pt 2):2045–2049
Hopkinson NS, Nickol AH, Payne J, Hawe E, Man WD, Moxham J, Montgomery H, Polkey MI (2004) Angiotensin converting enzyme genotype and strength in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 170(4):395–399. https://doi.org/10.1164/rccm.200304-578OC
Williams AG, Day SH, Folland JP, Gohlke P, Dhamrait S, Montgomery HE (2005) Circulating angiotensin converting enzyme activity is correlated with muscle strength. Med Sci Sports Exerc 37(6):944–948
Costa AM, Silva AJ, Garrido ND, Louro H, Marinho DA, Marques MC, Breitenfeld L (2009) Angiotensin-converting enzyme genotype affects skeletal muscle strength in elite athletes. J Sports Sci Med 8:410–418
Nazarov IB, Woods DR, Montgomery HE, Shneider OV, Kazakov VI, Tomilin NV, Rogozkin VA (2001) The angiotensin converting enzyme I/D polymorphism in Russian athletes. Eur J Hum Genet 9(10):797–801. https://doi.org/10.1038/sj.ejhg.5200711
Paulauskas A, Danileviciutė A, Povilaitis T, Poderis J (2009) Genetic variability associated with angiotensin converting enzyme (ACE) gene polymorphism in sportsmen pursuing different sports. Proc Latv Acad Sci B Nat Exact Appl Sci 63(1–2):9–13. https://doi.org/10.2478/v10046-009-0012-y
Costa AM, Silva AJ, Garrido ND, Louro H, de Oliveira RJ, Breitenfeld L (2009) Association between ACE D allele and elite short distance swimming. Eur J Appl Physiol 106(6):785–790. https://doi.org/10.1007/s00421-009-1080-z
Kikuchi N, Min SK, Ueda D, Igawa S, Nakazato K (2012) Higher frequency of the ACTN3 R allele + ACE DD genotype in Japanese elite wrestlers. J Strength Cond Res 26(12):3275–3280
Wang G, Mikami E, Chiu LL, Dep A, Deason M, Fuku N, Miyachi M, Kaneoka K, Murakami H, Tanaka M, Hsieh LL, Hsieh SS, Caporossi D, Pigozzi F, Hilley A, Lee R, Galloway SD, Gulbin J, Rogozkin VA, Ahmetov II, Yang N, North KN, Ploutarhos S, Montgomery HE, Bailey ME, Pitsiladis YP (2013) Association analysis of ACE and ACTN3 in elite Caucasian and East Asian swimmers. Med Sci Sports Exerc 45(5):892–900. https://doi.org/10.1249/MSS.0b013e31827c501f
Eidera J, Cieszczykb P, Ficeka K, Leonska-Duniecb A, Sawczuka M, Maciejewska-Karlowskaa A, Zarebskaba A (2013) The association between D allele of the ACE gene and power performance in Polish elite athletes. Sci Sports 28:325–330
Montgomery HE, Clarkson P, Dollery CM, Prasad K, Losi MA, Hemingway H, Statters D, Jubb M, Girvain M, Varnava A, World M, Deanfield J, Talmud P, McEwan JR, McKenna WJ, Humphries S (1997) Association of angiotensin-converting enzyme gene I/D polymorphism with change in left ventricular mass in response to physical training. Circulation 96(3):741–747
Yamin C, Amir O, Sagiv M, Attias E, Meckel Y, Eynon N, Amir RE (2007) ACE ID genotype affects blood creatine kinase response to eccentric exercise. J Appl Physiol 103(6):2057–2061. https://doi.org/10.1152/japplphysiol.00867.2007
Thomis MI, Huygens W, Heuninckx S, Chagnon M, Maes HM, Claessens A, Vlietinck R, Bouchard C, Beunen G (2004) Exploration of myostatin polymorphisms and the angiotensin-converting enzyme insertion/deletion genotype in responses of human muscle to strength training. Eur J Appl Physiol 92(3):267–274. https://doi.org/10.1007/s00421-004-1093-6
Kasikcioglu E, Kayserilioglu A, Ciloglu F, Akhan H, Oflaz H, Yildiz S, Peker I (2004) Angiotensin-converting enzyme gene polymorphism, left ventricular remodeling, and exercise capacity in strength-trained athletes. Heart Vessels 19(6):287–293
Moran CN, Vassilopoulos C, Tsiokanos A, Jamurtas AZ, Bailey ME, Montgomery HE, Wilson RH, Pitsiladis YP (2006) The associations of ACE polymorphisms with physical, physiological and skill parameters in adolescents. Eur J Hum Genet 14(3):332–339. https://doi.org/10.1038/sj.ejhg.5201550
Charbonneau D (2007) Association between ACE genotype and skeletal muscle strength and volume, and their response to strength training in older adults. Masters of Arts Theses and Dissertations, University of Maryland
Eynon N, Alves AJ, Yamin C, Sagiv M, Duarte JA, Oliveira J, Ayalon M, Goldhammer E, Meckel Y (2009) Is there an ACE ID: ACTN3 R577X polymorphisms interaction that influences sprint performance? Int J Sport Med 30(12):888–891. https://doi.org/10.1055/s-0029-1238291
Rodríguez-Romo G, Ruiz JR, Santiago C, Fiuza-Luces C, González-Freire M, Gómez-Gallego F, Morán M, Lucia A (2010) Does the ACE I/D polymorphism, alone or in combination with the ACTN3 R577X polymorphism, influence muscle power phenotypes in young, non-athletic adults? Eur J Appl Physiol 110(6):1099–1106
Scott RA, Irving R, Irwin L, Morrison E, Charlton V, Austin K, Tladi D, Deason M, Headley SA, Kolkhorst FW, Yang N, North K, Pitsiladis YP (2010) ACTN3 and ACE genotypes in elite Jamaican and US sprinters. Med Sci Sports Exerc 42(1):107–112. https://doi.org/10.1249/MSS.0b013e3181ae2bc0
Mayne I (2006) Examination of the ACE and ACTN3 genes in UTC varsity athletes and sedentary students. Honors paper-University of Tennessee at Chattanooga, Biological and Environmental Sciences
Charbonneau DE, Hanson ED, Ludlow AT, Delmonico MJ, Hurley BF, Roth SM (2008) ACE genotype and the muscle hypertrophic and strength responses to strength training. Med Sci Sports Exerc 40(4):677–683. https://doi.org/10.1249/MSS.0b013e318161eab9
Rattigan S, Dora KA, Tong AC, Clark MG (1996) Perfused skeletal muscle contraction and metabolism improved by angiotensin II-mediated vasoconstriction. Am J Physiol 271(1 Pt 1):E96-103
Guilherme J, Tritto A, North K, Lancha A Jr, Artioli G (2014) Genetics and sport performance: current challenges and directions to the future. Rev Brasi Educ Física Esporte 28:177–193. https://doi.org/10.1590/s1807-55092014000100177
Huang W, Xie C, Zhou H, Yang T, Sun M (2004) Association of the angiotensin-converting enzyme gene polymorphism with chronic heart failure in Chinese Han patients. Eur J Heart Fail 6(1):23–27. https://doi.org/10.1016/j.ejheart.2003.09.004
Koh WP, Yuan JM, Sun CL, van den Berg D, Seow A, Lee HP, Yu MC (2003) Angiotensin I-converting enzyme (ACE) gene polymorphism and breast cancer risk among Chinese women in Singapore. Cancer Res 63(3):573–578
Lau YK, Woo KT, Choong HL, Zhao Y, Tan HB, Cheung W, Yap HK (2002) ACE gene polymorphism and disease progression of IgA nephropathy in Asians in Singapore. Nephron 91(3):499–503
Kario K, Kanai N, Nishiuma S, Fujii T, Saito K, Matsuo T, Matsuo M, Shimada K (1997) Hypertensive nephropathy and the gene for angiotensin-converting enzyme. Arterioscler Thromb Vasc Biol 17(2):252–256. https://doi.org/10.1161/01.atv.17.2.252
Yoshida H, Mitarai T, Kawamura T, Kitajima T, Miyazaki Y, Nagasawa R, Kawaguchi Y, Kubo H, Ichikawa I, Sakai O (1995) Role of the deletion of polymorphism of the angiotensin converting enzyme gene in the progression and therapeutic responsiveness of IgA nephropathy. J Clin Investig 96(5):2162–2169. https://doi.org/10.1172/JCI118270
Yoo JH (2005) Deletion polymorphism in the gene for angiotensin-converting enzyme is associated with essential hypertension in men born during the Pacific War. Mech Ageing Dev 126(8):899–905. https://doi.org/10.1016/j.mad.2005.03.011
Stephens JW, Dhamrait SS, Cooper JA, Acharya J, Miller GJ, Hurel SJ, Humphries SE (2005) The D allele of the ACE I/D common gene variant is associated with Type 2 diabetes mellitus in Caucasian subjects. Mol Genet Metab 84(1):83–89. https://doi.org/10.1016/j.ymgme.2004.09.002
Mattace-Raso FU, van der Cammen TJ, Sayed-Tabatabaei FA, van Popele NM, Asmar R, Schalekamp MA, Hofman A, van Duijn CM, Witteman JC (2004) Angiotensin-converting enzyme gene polymorphism and common carotid stiffness. The Rotterdam study. Atherosclerosis 174(1):121–126. https://doi.org/10.1016/j.atherosclerosis.2004.01.012
Sprovieri SR, Sens YA (2005) Polymorphisms of the renin-angiotensin system genes in Brazilian patients with lupus nephropathy. Lupus 14(5):356–362
van Bockxmeer FM, Mamotte CD, Burke V, Taylor RR (2000) Angiotensin-converting enzyme gene polymorphism and premature coronary heart disease. Clin Sci (Lond) 99(3):247–251
Marre M, Jeunemaitre X, Gallois Y, Rodier M, Chatellier G, Sert C, Dusselier L, Kahal Z, Chaillous L, Halimi S, Muller A, Sackmann H, Bauduceau B, Bled F, Passa P, Alhenc-Gelas F (1997) Contribution of genetic polymorphism in the renin-angiotensin system to the development of renal complications in insulin-dependent diabetes: Genetique de la Nephropathie Diabetique (GENEDIAB) study group. J Clin Investig 99(7):1585–1595. https://doi.org/10.1172/JCI119321
Salem AH (2008) Distribution of angiotensin converting enzyme insertion/deletion gene polymorphism among two Arab populations. Suez Canal Univ Med J 11(1):125–130
Abdi Rad I, Bagheri M (2011) Angiotensin-converting enzyme insertion/deletion gene polymorphism in general population of west Azarbaijan. Iran Iran J Kidney Dis 5(2):86–92
Eleni S, Dimitrios K, Vaya P, Areti M, Norma V, Magdalini G (2008) Angiotensin-I converting enzyme gene and I/D polymorphism distribution in the Greek population and a comparison with other European populations. J Genet 87(1):91–93
Zorc-Pleskovic R, Teran N, Pleskovic A, Terzic R, Milutinovic A (2005) Deletion/deletion genotype of angiotensin-I converting enzyme gene is not associated with coronary artery disease in Caucasians with type 2 diabetes. Coll Antropol 29(1):149–152
Mondry A, Loh M, Liu P, Zhu AL, Nagel M (2005) Polymorphisms of the insertion / deletion ACE and M235T AGT genes and hypertension: surprising new findings and meta-analysis of data. BMC Nephrol 6(1):1–11. https://doi.org/10.1186/1471-2369-6-1
Hohenfellner K, Wingen A-M, Nauroth O, Wuhl E, Mehls O, Schaefer F (2001) Impact of ACE I/D polymorphism on congenital renal malformations. Pediatr Neurol 16(4):356–361
Barbalic M, Pericic M, Skaric-Juric T, Narancic NS (2004) Ace Alu insertion polymorphism in Croatia and its isolates. Coll Antropol 28(2):603–610
Yang N, MacArthur DG, Gulbin JP, Hahn AG, Beggs AH, Easteal S, North K (2003) ACTN3 genotype is associated with human elite athletic performance. Am J Hum Genet 73(3):627–631
Massidda M, Corrias L, Scorcu M, Vona G, Calò MC (2012) ACTN-3 and ACE genotypes in elite male Italian athletes. Anthropol Rev 75(1):51–59
Rigoli L, Chimenz R, di Bella C, Cavallaro E, Caruso R, Briuglia S, Fede C, Salpietro CD (2004) Angiotensin-converting enzyme and angiotensin type 2 receptor gene genotype distributions in Italian children with congenital uropathies. Pediatr Res 56(6):988–993. https://doi.org/10.1203/01.PDR.0000145252.89427.9E
Di Pasquale P, Cannizzaro S, Paterna S (2004) Does angiotensin-converting enzyme gene polymorphism affect blood pressure? Findings after 6 years of follow-up in healthy subjects. Eur J Heart Fail 6(1):11–16. https://doi.org/10.1016/j.ejheart.2003.07.009
Camelo D, Arboleda G, Yunis JJ, Pardo R, Arango G, Solano E, Lopez L, Hedmont D, Arboleda H (2004) Angiotensin-converting enzyme and alpha-2-macroglobulin gene polymorphisms are not associated with Alzheimer’s disease in Colombian patients. J Neurol Sci 218(1–2):47–51. https://doi.org/10.1016/j.jns.2003.10.008
Jalil JE, Piddo AM, Cordova S, Chamorro G, Braun S, Jalil R, Vega J, Jadue PL, Lavandero S, Lastra P (1999) Prevalence of the angiotensin I converting enzyme insertion/deletion polymorphism, plasma angiotensin converting enzyme activity, and left ventricular mass in a normotensive Chilean population. Am J Hypertens 12(7):697–704
Soodyall H, Vigilant L, Hill AV, Stoneking M, Jenkins T (1996) mtDNA control-region sequence variation suggests multiple independent origins of an “Asian-specific” 9-bp deletion in sub-Saharan Africans. Am J Hum Genet 58(3):595–608
Cieszczyk P, Maciejewska A, Sawczuk M, Ficek K, Eider J, Jascaniene N (2010) The angiotensin converting enzyme gene I/D polymorphism in ellite Polish and Lithuanian judo players. Biol Sport 27(2):119–122
Tanriverdi H, Evrengul H, Tanriverdi S, Turgut S, Akdag B, Kaftan HA, Semiz E (2005) Improved endothelium dependent vasodilation in endurance athletes and its relation with ACE I/D polymorphism. Circ J 69(9):1105–1110 (JST.JSTAGE/circj/69.1105[pii])
Tsianos G, Eleftheriou KI, Hawe E, Woolrich L, Watt M, Watt I, Peacock A, Montgomery H, Grant S (2004) Performance at altitude and angiotensin I-converting enzyme genotype. Eur J Appl Physiol 93(5–6):630–633. https://doi.org/10.1007/s00421-004-1284-1
Auerbach I, Tenenbaum A, Motro M, Stroh CI, Har-Zahav Y, Fisman EZ (2000) Blunted responses of doppler-derived aortic flow parameters during whole-body heavy isometric exercise in heart transplant recipients. J Heart Lung Transplant 19(11):1063–1070
Holdys J, Kryściak J, Stanisławski D, Gronek P (2011) ACE I/D gene polymorphism in athletes of various sports disciplines. Hum Mov 12(3):223–231. https://doi.org/10.2478/v10038-011-0022-x
Sonna LA, Sharp MA, Knapik JJ, Cullivan M, Angel KC, Patton JF, Lilly CM (2001) Angiotensin-converting enzyme genotype and physical performance during US Army basic training. J Appl Physiol 91(3):1355–1363
Maciejewska-Karlowska A, Sawczuk M, Cieszczyk P, Zarebska A, Sawczyn S (2013) Association between the Pro12Ala polymorphism of the peroxisome proliferator-activated receptor gamma gene and strength athlete status. PLoS ONE 8(6):e67172. https://doi.org/10.1371/journal.pone.0067172
Cerit M, Colakoglu M, Erdogan M, Berdeli A, Cam FS (2006) Relationship between ace genotype and short duration aerobic performance development. Eur J Appl Physiol 98(5):461–465
Hernández D, de la Rosa A, Barragán A, Barrios Y, Salido E, Torres A, Martín B, Laynez I, Duque A, De Vera A, Lorenzo V, González A (2003) The ACE/DD genotype is associated with the extent of exercise-induced left ventricular growth in endurance athletes. J Am Coll Cardiol 42(3):527–532
Graf C, Diet F, Palma-Hohmann I, Mahnke N, Böhm M, Rost R, Predel H-G (2001) Correlations of the renin-angiotensin-system (RAS) gene polymorphisms with cardiac growth factors endothelin-1 and angiotensin II in high performance athlete. Eur J Sport Sci 1(5):1–7
Myerson SG, Montgomery HE, Whittingham M, Jubb M, World MJ, Humphries SE, Pennell DJ (2001) Left ventricular hypertrophy with exercise and ACE gene insertion/deletion polymorphism: a randomized controlled trial with losartan. Circulation 103(2):226–230
Woods D, Hickman M, Jamshidi Y, Brull D, Vassiliou V, Jones A, Humphries S, Montgomery H (2001) Elite swimmers and the D allele of the ACE I/D polymorphism. Hum Genet 108(3):230–232
Acknowledgements
The authors thank the Universiti Sains Malaysia for providing facilities that made this review article work possible. This article is a part of the work funded by Universiti Sains Malaysia (304.CIPPT.6315037).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that this review was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ahmad Yusof, H., Che Muhamed, A.M. Angiotensin-converting enzyme (ACE) insertion/deletion gene polymorphism across ethnicity: a narrative review of performance gene. Sport Sci Health 17, 57–77 (2021). https://doi.org/10.1007/s11332-020-00712-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11332-020-00712-9