
Abstract
Purpose
Continuous positive airway pressure (CPAP) is the primary therapy for obstructive sleep apnea (OSA); however the effectiveness of CPAP remains suboptimal. We describe the Novel PhysIologiC prEdictors of Positive Airway Pressure Effectiveness (NICEPAP) study. Its purpose is to determine whether physiological traits of OSA contribute to CPAP effectiveness.
Methods
NICEPAP (NCT05067088) is a prospective, observational cohort study conducted at an academic sleep center. Adults newly diagnosed with OSA (n = 267) are assessed for OSA traits of loop gain, arousal threshold, pharyngeal collapsibility, and muscle compensation from baseline polysomnography. We perform a comprehensive assessment of covariates relevant to CPAP adherence, efficacy, and patient-centered outcomes. Participants are followed for 12 months. Primary outcomes include (1) CPAP adherence (hours/night), (2) CPAP efficacy (apneas-hypopneas/hour), and (3) quality of life at six months measured by objective CPAP data and Functional Outcomes of Sleep Questionnaire. Secondary outcomes include sleep quality, sleepiness, insomnia, and neurocognitive function.
Results
Data on covariates, including demographics, sleep symptoms, medical history, medications, sleep quality, OSA and treatment self-efficacy, decisional balance, and socio-economic and social and partner support, are collected using validated instruments. The analysis for primary outcomes includes a generalized linear mixed model for an outcome (e.g., CPAP adherence) with OSA traits as exposures followed by the addition of relevant covariates.
Conclusion
The findings of the NICEPAP study will inform research aimed to enhance CPAP effectiveness. Understanding the role of physiological OSA traits in CPAP effectiveness is a crucial step toward a precision medicine approach to OSA.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Obstructive Sleep Apnea (OSA) affects over 950 million individuals worldwide [1]. It is associated with hypertension, diabetes, stroke, heart failure and morbidity and mortality from these conditions [2]. Continuous Positive Airway Pressure therapy (CPAP) is prescribed to 80% of people diagnosed with OSA [3]. Most, however, do not receive effective treatment for several reasons. First, only about 50% of patients adhere to CPAP long-term, [4] and therefore are unable to reap the benefits of therapy. Second, approximately 20–40% of patients experience residual OSA on CPAP therapy (poor efficacy), defined as a high residual apnea-hypopnea index (AHI) [5]. Improvements in symptoms are inconsistent even among those who adhere and have low residual AHI [6]. Taken together, poor adherence, imperfect efficacy, and variable response to CPAP limit the effectiveness of this therapy.
Sleep medicine experts have worked towards making CPAP a more effective treatment. Psychological and social factors, such as treatment self-efficacy and peer support, are key predictors of CPAP adherence (Fig. 1) [7]. However, the behavioral interventions addressing these barriers show limited benefits [8, 9] and have not translated to clinical care due to feasibility and cost [10]. Moreover, these factors explain only a fraction (11–58%) of variance in CPAP adherence [7]. Technological advances such as new masks, auto-titrating CPAP, and remote monitoring have not significantly improved CPAP efficacy, sleepiness, or quality of life [11]. Therefore, novel approaches are needed to address the effectiveness of CPAP therapy, including adherence to treatment, and improvements in symptoms, function, and quality of life.

Biopsychosocial model of CPAP adherence. Each domain (e.g. “Social” with examples of factors influencing PAP use on three levels: P- person; I- Illness; T-Treatment). Our proposal is focused on the factors in biomedical domain that have not been explored prospectively and in context of the psychological and social domains: physiologic OSA traits. Adapted from Crawford et al., Sleep Med Rev. 2014. The variables and instruments assessing factors in each of the bio-psycho-social domains of CPAP adherence are noted in Table 4. PAP – positive airway pressure, OSA – obstructive sleep apnea
Study rationale
CPAP addresses a major cause of OSA, the anatomic susceptibility of the upper airway to collapse. However, it is now recognized that the interplay of anatomic and non-anatomic traits plays a key role in OSA pathogenesis. These non-anatomic or physiologic traits include easy arousability, unstable ventilatory control, and poor pharyngeal muscle compensation [12]. For example, a low arousal threshold (ArTH, the propensity to awaken easily) and loop gain (LG, a metric of ventilatory control instability) that is higher than that in controls occur in up to 50% and 40% of OSA patients, respectively [13]. In addition to predisposing to OSA, these traits may also affect response to treatment. For instance, a low ArTH contributes to lighter and less continuous sleep and may affect a patient’s ability to tolerate and adhere to CPAP. Recent retrospective analyses show that a low ArTH is associated with reduced (45–120 min/night) CPAP adherence (Fig. 1) [14, 15]. In addition to a low ArTH, very high or very low muscle compensation is reported as associated with poor adherence [15] while a high LG is associated with longer CPAP use [16]. Similarly, high LG can cause treatment-emergent central apneas, contributing to poor CPAP efficacy (high residual AHI) [17].
Understanding the physiologic determinants of an individual’s OSA may inform a precision medicine approach by (1) identifying those at high risk for CPAP failure and (2) incorporating adjunctive therapies with CPAP to modify an individual’s physiologic traits. For example, individuals with low a ArTH may be at higher risk of CPAP non-adherence. Targeting those individuals for treatment with a sedative-hypnotics which increase ArTH, [18]may improve CPAP adherence [19]. Similarly, acetazolamide attenuates LG [20] and reduces AHI [21] which may be particularly useful in those with high LG undergoing CPAP treatment [22] Such approaches may improve treatment for those who are not responding to CPAP, or to proactively ensure the effectiveness of CPAP therapy from the start.
However, data supporting the targeting physiologic traits in CPAP therapy are limited by (1) retrospective designs, (2) failure to account for critical psychosocial covariates known to impact CPAP adherence (e.g., insomnia, self-efficacy, partner support), and (3) failure to consistently assess patient-centered outcomes [23]. To understand whether the OSA traits are relevant for clinical outcomes it is critical to address these gaps. For example, retrospective analyses show disparate results, with ArTH and pharyngeal muscle compensation associated with CPAP adherence [14, 15] in some studies, while others show associations with LG and pharyngeal collapsibility [16]. These finding may be due to disparate populations in the studies like patients with stroke (n = 60) or coronary artery disease (n = 249) [14, 15] vs. sleep clinic (n = 87), [16] inconsistent and incomplete adherence covariates, differing analytic approaches (continuous [14, 15] vs. dichotomized traits), [16] and objective [14, 15] vs. subjective assessments of CPAP adherence [16]. Likewise, while meta-analyses [21] and retrospective interventional studies [22] in those with putative high LG show improvements in AHI with acetazolamide, baseline high LG however does not consistently predict AHI reduction [20, 24].
The objective of the NICEPAP study is to overcome these limitations by gathering detailed, prospective data to evaluate the role of physiologic traits in the effectiveness of CPAP therapy (Fig. 2).

Aims of the NICEPAP study, including exposures and outcomes. PAP – positive airway pressure, OSA – obstructive sleep apnea, UA – upper airway
Study aims
Aim 1
Determine whether physiologic traits explain variability in CPAP adherence independently of established psychological and social predictors. We hypothesize that low ArTH will be associated with poor CPAP adherence independently of the established psychological and social covariates such as insomnia, self-efficacy, outcome expectancy, and social support.
Aim 2
Evaluate whether physiologic traits are associated with CPAP efficacy. We hypothesize that individuals with high LG will exhibit poor CPAP efficacy after accounting for known covariates such as age, sex, pharyngeal collapsibility, sleep position, atrial fibrillation, and heart failure.
Aim 3
Ascertain the contribution of physiologic traits to sleep quality, residual symptoms of sleepiness, insomnia, daytime function, and quality of life in patients on CPAP therapy. We hypothesize that low ArTH and high LG will be associated with subjective poor sleep quality, worse residual symptoms, and lower quality of life.
Methods
Study design
The Novel physIologiC prEdictors of Positive Airway Pressure Effectiveness (NICEPAP) is a prospective, observational study that is integrated with the clinical structure at an American Academy of Sleep Medicine (AASM) accredited academic practice. Research contacts occur at baseline (prior to PAP initiation), at 1 week, then at 1-, 3-, 6- and 12-months post PAP start date. The study is approved by Yale University’s Human Investigations Committee (HIC # 2,000,024,615).
Study population
The NICEPAP study will include patients referred for OSA evaluation at the Yale New Haven Hospital (YNHH) Sleep Center. The YNHH sleep center is in the New Haven metropolitan area. It is representative of the U.S. as a whole based on age, education, race, and ethnicity, [25] ensuring a diverse patient population. Patients are screened for initial eligibility (inclusion criteria 1–2 and no exclusion criteria) as noted in Table 1.
Screening, recruitment, enrollment and follow-up
Patients referred for polysomnography (PSG) or Home Sleep Apnea Test (HSAT) using a type III device at YNHH Sleep Center are screened for eligibility. This approach avoids selection bias by test type, as individuals with a high pre-test probability of OSA typically undergo HSAT. If initially eligible (Fig. 3), potential participants are offered the consent process during or after their diagnostic sleep study encounter. Participants are enrolled after diagnosis of OSA and CPAP prescription (Table 1, AHI > 5/hour and referred for CPAP management). At enrollment, participants completed baseline measures. Research staff complete each follow-up visit virtually (video or phone call) or in person for participant convenience at 1-, 3-, 6- and 12-months.

Overview of patient recruitment from the YNHH Centers for Sleep Medicine population. CPAP – continuous positive airway pressure, HSAT – home sleep apnea test, PSG – polysomnography, YNHH – Yale New Haven Health
Educational interventions in clinical care
Variability in the educational interventions in clinical settings may influence CPAP adherence. The research team provides OSA and CPAP education sessions to minimize the potential confounding of this phenomenon. Each lasting 45 min, these sessions are conducted by trained personnel (MD or MD-trained research associate). They are completed before PAP initiation and include education about OSA, a visual review of participants’ sleep study data, and a description of PAP therapy and its benefits. Participants are also instructed on the operation of PAP, conducting a virtual mask fitting and monitoring using cloud-based systems (e.g. AirView™ for ResMed devices and CareOrcestrator© for Philips devices).
Each participant undergoes CPAP/APAP pressure selection, assessment of residual AHI, and mask leak assessment by the clinicians caring for the patients (participants in our study). If the research team observes pressure intolerance, elevated residual AHI, or mask leak, research staff will encourage participants to address these issues with their clinical provider and durable medical equipment company and will notify the clinical provider if permitted by the participant. Physical visits with durable medical equipment company for mask fitting will be completed as part of clinical care as deemed necessary by sleep medicine providers.
Study measurements
Outcomes
Study outcomes and their measurement are noted in Table 2. Primary outcomes include nightly CPAP use data (Aim 1), ascertained from the cloud-based remote monitoring adherence systems (e.g., CareOrchestrator© AirView ™). CPAP adherence will be determined by daily measures of CPAP use (hours/night) from the date of initiating CPAP use to the end of follow-up at six months. Daily average CPAP use is the during this period is the primary outcome. Daily CPAP usage will be monitored for 6 months, using a dichotomized metric of > 4 h/ night for 70% of nights. Those that are missing CPAP usage for 1 < week due to reasons other than lack of supplies, medical condition or death will be encoded as “0”. Residual AHI data (Aim 2) is measured analogously. Quality of life, the primary outcome for Aim 3, is measured by the Functional Outcomes of Sleep Questionnaire (FOSQ) short form, a validated metric sensitive to CPAP treatment and adherence.
Secondary outcomes (Table 2) include sleep quality and residual symptoms (e.g., insomnia, sleepiness, depression, and anxiety). Neurocognitive function is assessed using a 3-min smartphone-based psychomotor vigilance test [26] with participants’ median reaction time and mean slowest 10% reaction time as key outcome metrics.
Polysomnographic recordings
For individuals undergoing clinical in-laboratory PSG (Nihon Kohden, Irvine CA, USA) this data is used to collect the polysomnographic metrics (e.g., total sleep duration, apnea hypopnea index, arousal index etc.) and exposures (see below) in our study. Acquisition is performed according to the AASM standards. Individuals diagnosed with OSA via a clinical HSAT undergo a NOX Self-Applied Somnography (SAS, NOX Medical, Suwanee, GA, USA) at home prior to PAP initiation. This is a validated alternative for collecting sleep data in participant’s home while obtaining a valid sleep assessment [27]. The SAS uses 8 frontal electrodes to capture frontal electroencephalography (EEG) and right and left electrooculograms (EOG). SAS also collects data from frontalis muscle electromyogram (EMG), the electrocardiogram, nasal canula airflow, oxygen saturation, chest, and abdominal respiratory inductance plethysmography bands, and right and left anterior tibialis EMG. Acquisition is performed for one night, assisted by a research associate who provides instructions, including a video demonstration for the SAS device set-up. All studies are manually scored by an AASM certified sleep technologist. NOX-SAS has been used for in-home polysomnography assessments in a large clinical cohort with good interscorer reliability for sleep stages, arousal and respiratory events (ICC of 0.86–0.99) with lowest reliability of REM arousals (ICC 0.68) [27]. The manual scoring of sleep stages using SAS montage data compared to conventional polysomnography shows a high accuracy (0.82 [NREM 2] – 0.96 [REM]) [28]. We define the SAS adequacy criteria which includes a minimum of 3 h of sleep with artifact-free signals in at least 2 EOGs, 2 EEG, pulse oximetry, nasal pressure, and 1 EMG. The NOX SAS has been used to determine the physiological traits of OSA [29].
Exposures
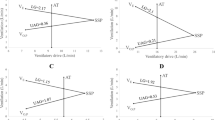
Physiological OSA traits (LG, ArTH, pharyngeal collapsibility [Vpassive], and Vcomp) differentially contribute to the causation of OSA in each individual (Table 3) [13]. LG reflects ventilatory control stability (elevated LG signifies an exaggerated ventilatory drive response to reduced airflow and the associated hypoxia and hypercapnia). ArTH reflects the amount of ventilatory drive required to cause arousal from sleep (a small rise in the ventilatory drive to terminate sleep represents a low ArTH). Vpassive reflects the ventilation at the eupneic ventilatory drive (higher values reflect lower pharyngeal collapsibility). Finally, the Vcomp is determined by calculating the difference between the ventilation at the maximum and eupneic ventilatory drives (higher values reflect better pharyngeal muscle compensation).
The OSA physiologic traits are measured using a validated method from polysomnography as previously described [15]. Median trait values across non-REM sleep are used for each individual. Respiratory events are identified using AASM standards, including a definition of hypopnea as a decrement in nasal flow of 30–90% associated with a 3% oxygen desaturation or an arousal. The traits obtained by this method are related to clinical outcomes, including PAP adherence [15]. An AASM-accredited scorer scores all studies and a more detailed description of physiologic trait assessment is available in the Online Resource 1.
Covariates
A comprehensive collection of covariates and their measurement tools are shown in Table 4 and Online Resource 2. These include psychosocial factors influencing adherence and patient-centered outcomes such as demographics, OSA and CPAP knowledge, outcome expectancy, self-efficacy, decisional balance, bed-partner status, partner-specific support, lifestyle factors, anxiety, depression, claustrophobia among others (Table 4). The covariates will be used to create a model using established predictors for each primary outcome to assess the impact of physiologic traits above and beyond established factors (see Statistical Analysis below).
Survey instruments
Surveys are completed over the phone, in person, or using electronic-surveys per patient preference. Each survey instrument is a validated tool as shown in Online Resource 2.
Data management
To optimize data quality and completeness, the study procedures include: (1) a detailed data dictionary, (2) quality assurance within the data management system, (3) quality assurance of key variables within the case report forms (CRF) and (4) regular written and video training for research staff. An audit is conducted on cases quarterly. A HIPPA-compliant database software, Research Electronic Data Capture (RedCap, captures all participant data. To facilitate participant stipends, a Yale internal clinical trials management system, “OnCore” (Advarra System, Columbia, MD, USA) is used to track study progress and issue payments as a debit card.
Statistical analysis
Sample size
The sample size assessment is based on the most conservative outcome: CPAP adherence. We define a clinically meaningful change in CPAP use as one hour/night [8]. Based on our preliminary data [15] and generalized linear mixed models (GLMM) with Monte-Carlo simulations (R package simR), we estimate a sample size of 245. This sample will allow us to detect a change of on hour/night (slope of 0.024 h/night/%ArTH) in adherence with 80% power at a = 0.05. Allowing for 10% patient loss (conservative estimate in observational studies at our center) we estimate that the final sample will be 267 participants.
Primary analysis aim 1 example: CPAP adherence
First, we will build a “physiologic CPAP adherence model” using OSA traits. Then we will assess whether trait associations with CPAP adherence are independent of other covariates.
-
Step (1) Physiologic CPAP adherence model. We will use general linear mixed model (GLMM) with auto-regressive covariance matrix of repeated measures. The GLMM will account for the correlation of repeated adherence measures within an individual over time [30]. CPAP adherence is measured in (hours/night). For participants who are lost to follow-up, CPAP use will be imputed as 0 h/night from the last contact [31]. Traits are used as continuous variables. The primary prespecified analysis is an adherence model over 6 months of follow-up. Statistical significance is defined as p < 0.05.
-
Step (2) Physiologic traits and “established” adherence factors. Relevant predictors will be identified using variable selection from each covariate domain using significant factors on bivariate associations and Bayesian Information Criterion in domains with > 10 factors (e.g., OSA PSG metrics) [14]. The significant factors from each domain will be added to create the adherence model based on “established” predictors. Finally, we will add the factors from Step 1 (physiologic model) to the above model to assess whether the traits are associated with adherence independently of the established factors. We will use a likelihood ratio test to assess whether the traits significantly improve the fit of the “established” CPAP adherence model [32]. Analogous analyses will be performed for CPAP efficacy (Aim 2) and patient-centered outcomes (Aim 3).
Results
Study population
Through March 1, 2024, 169 participants are enrolled in this study with a mean age of 52.1 +/- 14.2 years. 46% of participants are women, 67% are White, 20% are Black, 6% are Asian, 5% are more than one race. 11% are Hispanic.
Transparency and dissemination of results
This study is registered at ClinicalTrials.gov (NCT05067088) and the protocol can be obtained for review by contact of the principal investigator. The study is designed and will be reported according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines as shown in Online Resource 3. The study is funded by the NIH (1K23HL159259-01). The data gathered for this study will be available to other investigators after de-identification. In the short-term, those who wish to use the data will be asked to sign a data use agreement. Ultimately, the study team plans to incorporate the data set into The National Sleep Research Resource (NSRR). NSRR is an NIH-funded resource designed to host and share data from major sleep cohort studies and clinical trials.
Discussion
A greater understanding of the factors that affect CPAP effectiveness (adherence, efficacy, and improvement in outcomes) will allow clinicians to make better decisions in caring for the millions of patients suffering from OSA. The goal of the NICEPAP study is to determine whether the novel, physiological factors that combine in different ways to cause OSA in each individual (ArTH, LG, pharyngeal collapsibility and compensation) contribute to CPAP effectiveness. This knowledge may enable clinicians to predict PAP adherence, efficacy, and improve patient-centered outcomes such as residual sleepiness, insomnia, daytime function and to intervene based on the traits of OSA in each individual.
Such a precision medicine approach to CPAP therapy can help shift OSA treatment away from the “one size fits all” paradigm. For example, if physiological traits such as a low ArTH are associated with poor adherence, the ArTH can then be used to predict which patients are at risk. Targeting those individuals with proven interventions, such as motivational enhancement therapy [8] prior to initiating CPAP may help people succeed with treatment. Moreover, the physiological traits are modifiable and may be targeted for individualized treatments. For example, patients with a low ArTH at risk of non-adherence, may benefit from using a sedative-hypnotic in conjunction with their CPAP treatment [19]. Alternatively, those with high LG, a potential determinant of high residual AHI, may benefit from incorporating acetazolamide to reduce LG and improve CPAP efficacy [22]. Implementing such strategies can be a first step in precision medicine approach to OSA management.
There are several key strengths of the NICEPAP study. It will be the first prospective, observational cohort to assess the relationship between physiological factors that cause OSA and CPAP effectiveness. The NICEPAP study uses a non-invasive signal analysis tool to measure the OSA traits from sleep studies obtained in real-world clinical care. This will allow implementation across clinical settings. The NICEPAP study will for the first time determine whether the physiologic traits associated with CPAP effectiveness, such as ArTH and LG, affect CPAP outcomes independently of the established psychological (e.g., self-efficacy, claustrophobia) and social factors (e.g., education, bed-partner status). This is critical if physiological traits are to be used for effective prediction of CPAP adherence or efficacy. Similarly, to our knowledge, the NICEPAP study will for the first time examine the relationship between OSA traits and patient-centered outcomes, such as sleep quality, psychomotor function, and quality of life. Knowing whether OSA traits influence these outcomes is vital to success of CPAP therapy. In summary, the study should rigorously evaluate whether the traits that cause OSA in each individual, also affect the effectiveness of CPAP.
There are limitations of the NICEPAP study. First, while the research design includes a sample of patients recruited from the Yale New Haven Hospital (YNHH) Sleep Center, which are reflective of the sociodemographic average U.S. city on-average [25], the findings may not extend to other populations, including those with predominantly Black, LatinX populations or those outside of the U.S. Additionally, insomnia, a known predictor of CPAP use, may be a stronger predictor of OSA adherence than physiologic traits. It is not known whether low ArTH leads to insomnia, or the ArTH is a manifestation of insomnia. Addressing causality is critical for developing interventions.
There are a multitude of potential psychosocial determinants of CPAP adherence and other studies focusing on metrics not measured in our study (e.g., home-work conflict, mindful awareness) complement this work [33]. While we aim to collect representative determinants of the biopsychosocial model of adherence to determine whether OSA traits are independently related to CPAP adherence, we do not measure all potential confounders. Our study uses PAP device derived indices of CPAP efficacy (machine generated residual AHI, Aim 2 outcome). This metric exhibits a high correlation with the AHI derived from PSG (r = 0.82–0.92), [34, 35] reliability (ICC 0.79) [36] and is a feasible outcome in our relatively large observational study integrated into the clinical structure of a sleep medicine practice. A limitation of this measure is that both under- [37] and overestimation [36] of the AHI by the PAP device algorithm occurs. Thus, in addition to our secondary outcome cut-off of AHI > 10/hour, we will assess the impact of higher and lower AHI cut-offs on associations with the traits. Our study focuses on the four OSA traits as potential predictors of CPAP effectiveness. These four traits may not capture all physiology relevant for CPAP outcomes that can be extracted from a polysomnography. Future studies focusing on factors such as arousal intensity, ventilatory and hypoxic burden represent a natural continuation of this line of research. It is also plausible that anatomic traits of OSA (e.g., tongue fat, pharyngeal airway volume) may be important determinants of CPAP effectiveness, not measured in our study. Such measures require tools like Magnetic Resonance Imaging, the use of which is beyond the scope of this study. Future work on CPAP effectiveness should incorporate anatomic measures once less intrusive and costly metrics of anatomical determinants of OSA become available for use in clinical studies. Lastly, due to the study’s longitudinal design, participant attrition is expected, which could diminish the statistical power of the analysis. To mitigate this, the study procedures mimic the current recommendations for management of patients with OSA and accounts for this participant attrition in our sample size.
The results obtained from this study will provide vital insights for the development of precision medicine approaches to treat the millions of patients burdened by OSA. This research will provide valuable data to identify the vulnerable patients at risk for poor CPAP effectiveness prior to therapy initiation. Tailoring intervention strategies to the individual’s determinants of CPAP therapy effectiveness, including physiological traits, is imperative to improve the patient-centered health outcomes of those suffering from OSA.
Data availability
The data gathered for this study will be available to other investigators after de-identification. In the short-term, those who wish to use the data will be asked to sign a data use agreement. Ultimately, the study team plans to incorporate the data set into The National Sleep Research Resource (NSRR). NSRR is an NIH-funded resource designed to host and share data from major sleep cohort studies and clinical trials.
Abbreviations
- ArTH:
-
Arousal threshold
- CPAP:
-
Continuous Positive Airway Pressure
- Dx:
-
Diagnostic
- HSAT:
-
Home Sleep Apnea Test
- LG:
-
Loop Gain
- OSA:
-
Obstructive Sleep Apnea
- PSG:
-
Polysomnography
- Vcomp:
-
Ventilatory Compensation
- Vpassive:
-
Passive Pharyngeal Collapsibility
- YNHH:
-
Yale New Haven Hospital
References
Benjafield AV, Ayas NT, Eastwood PR et al (2019) Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir Med 7(8):687–698
Kendzerska T, Mollayeva T, Gershon AS, Leung RS, Hawker G, Tomlinson G (2014) Untreated obstructive sleep apnea and the risk for serious long-term adverse outcomes: a systematic review. Sleep Med Rev 18(1):49–59
Frost S, Sullivan D (2016) Hidden health crisis costing America billions. Underdiagnosing and undertreating obstructive sleep apnea draining healthcare system. American Academy of Sleep Medicine, Darien
Pandey A, Mereddy S, Combs D et al (2020) Socioeconomic inequities in adherence to Positive Airway Pressure Therapy in Population-Level analysis. J Clin Med. ;9(2)
Mulgrew AT, Lawati NA, Ayas NT et al (2010) Residual sleep apnea on polysomnography after 3 months of CPAP therapy: clinical implications, predictors and patterns. Sleep Med 11(2):119–125
Pien GW, Ye L, Keenan BT et al (2018) Changing faces of Obstructive Sleep Apnea: Treatment effects by Cluster Designation in the Icelandic sleep apnea cohort. Sleep. ;41(3)
Crawford MR, Espie CA, Bartlett DJ, Grunstein RR (2014) Integrating psychology and medicine in CPAP adherence–new concepts? Sleep Med Rev 18(2):123–139
Bakker JP, Wang R, Weng J et al (2016) Motivational enhancement for increasing adherence to CPAP: a Randomized Controlled Trial. Chest 150(2):337–345
Parthasarathy S, Wendel C, Haynes PL, Atwood C, Kuna S (2013) A pilot study of CPAP adherence promotion by peer buddies with sleep apnea. J Clin Sleep Med 9(6):543–550
Bakker JP, Weaver TE, Parthasarathy S, Aloia MS (2019) Adherence to CPAP: what should we be Aiming for, and how can we get there? Chest 155(6):1272–1287
Patil SP, Ayappa IA, Caples SM, Kimoff RJ, Patel SR, Harrod CG (2019) Treatment of adult obstructive sleep apnea with positive Airway pressure: an American Academy of Sleep Medicine Systematic Review, Meta-analysis, and GRADE Assessment. J Clin Sleep Med 15(2):301–334
Sands SA, Terrill PI, Edwards BA et al (2018) Quantifying the arousal threshold using polysomnography in Obstructive Sleep Apnea. Sleep. ;41(1)
Owens RL, Edwards BA, Eckert DJ et al (2015) An integrative model of physiological traits can be used to Predict Obstructive Sleep Apnea and Response to non positive Airway pressure therapy. Sleep 38(6):961–970
Eckert DJ, White DP, Jordan AS, Malhotra A, Wellman A (2013) Defining phenotypic causes of obstructive sleep apnea. Identification of novel therapeutic targets. Am J Respir Crit Care Med 188(8):996–1004
Zinchuk AV, Redeker NS, Chu JH et al (2020) Physiological traits and adherence to obstructive sleep apnea treatment in patients with stroke. Am J Respir Crit Care Med 201(12):1568–1572
Zinchuk AV, Chu JH, Liang J et al (2021) Physiological traits and adherence to Sleep Apnea Therapy in individuals with coronary artery disease. Am J Respir Crit Care Med 204(6):703–712
Cheng WJ, Finnsson E, Agustsson JS, Sands SA, Hang LW (2024) Continuous positive airway pressure and adherence in patients with different endotypes of obstructive sleep apnea. J Sleep Res 33(1):e13999
Stanchina M, Robinson K, Corrao W, Donat W, Sands S, Malhotra A (2015) Clinical use of Loop Gain measures to determine continuous positive Airway pressure efficacy in patients with Complex Sleep Apnea. A pilot study. Ann Am Thorac Soc 12(9):1351–1357
Eckert DJ, Owens RL, Kehlmann GB et al (2011) Eszopiclone increases the respiratory arousal threshold and lowers the apnoea/hypopnoea index in obstructive sleep apnoea patients with a low arousal threshold. Clin Sci (London England: 1979) 120(12):505–514
Lettieri CJ, Shah AA, Holley AB et al (2009) Effects of a short course of eszopiclone on continuous positive airway pressure adherence: a randomized trial. Ann Intern Med 151(10):696–702
Edwards BA, Sands SA, Eckert DJ et al (2012) Acetazolamide improves loop gain but not the other physiological traits causing obstructive sleep apnoea. J Physiol 590(Pt 5):1199–1211
Schmickl CN, Landry SA, Orr JE et al (2020) Acetazolamide for OSA and Central Sleep Apnea: a comprehensive systematic review and Meta-analysis. Chest 158(6):2632–2645
Ni YN, Holzer RC, Thomas RJ (2023) Acute and long-term effects of acetazolamide in presumed high loop gain sleep apnea. Sleep Med 107:137–148
Gray EL, McKenzie DK, Eckert DJ (2017) Obstructive sleep apnea without obesity is common and difficult to treat: evidence for a distinct pathophysiological phenotype. J Clin Sleep Med 13(1):81–88
Sands SA, Collet J, Gell LK et al (2024) Combination pharmacological therapy targeting multiple mechanisms of sleep apnoea: a randomised controlled cross-over trial. Thorax 79(3):259–268
Kolko J (2016) Normal America’ is not a small town of White People. FiveThirtyEight. fivethirtyeight.com ABC News
Grant DA, Honn KA, Layton ME, Riedy SM, Van Dongen HPA (2017) 3-minute smartphone-based and tablet-based psychomotor vigilance tests for the assessment of reduced alertness due to sleep deprivation. Behav Res Methods 49(3):1020–1029
Punjabi NM, Brown T, Aurora RN et al (2022) Methods for home-based self-applied polysomnography: the Multicenter AIDS Cohort Study. Sleep Adv 3(1):zpac011
Christensen ME, Montazeri K, Jonsson SA, Arnardottir E, Hugosdottir R, Sigmarsdottir PB, Helgason S, Riney H, Kramer F, Agustsson JS Abstract: epoch-level atreement of Manual Sleep Stage and Arousal Scoring using a reduced montage versus Conventional Polysomnography. SLEEP. 2024;SLEEP/APSS 2024 Abstract Volume.
Finnsson E, Olafsdottir GH, Loftsdottir DL et al (2021) A scalable method of determining physiological endotypes of sleep apnea from a polysomnographic sleep study. Sleep. ;44(1)
Babbin SF, Velicer WF, Aloia MS, Kushida CA (2015) Identifying longitudinal patterns for individuals and subgroups: an example with adherence to treatment for obstructive sleep apnea. Multivar Behav Res 50(1):91–108
Kushida CA, Nichols DA, Holmes TH et al (2012) Effects of continuous positive airway pressure on neurocognitive function in obstructive sleep apnea patients: the apnea positive pressure long-term efficacy study (APPLES). Sleep 35(12):1593–1602
Pepe MS, Kerr KF, Longton G, Wang Z (2013) Testing for improvement in prediction model performance. Stat Med 32(9):1467–1482
Bailly S, Foote A, Mendelson M et al (2024) Sociological determinants of adherence to continuous positive airway pressure in the management of sleep apnoea syndrome: protocol for a transdisciplinary, prospective observational study. BMJ Open 14(3):e079765
Ueno K, Kasai T, Brewer G et al (2010) Evaluation of the apnea-hypopnea index determined by the S8 auto-CPAP, a continuous positive airway pressure device, in patients with obstructive sleep apnea-hypopnea syndrome. J Clin Sleep Med 6(2):146–151
Ikeda Y, Kasai T, Kawana F et al (2012) Comparison between the apnea-hypopnea indices determined by the REMstar Auto M series and those determined by standard in-laboratory polysomnography in patients with obstructive sleep apnea. Intern Med 51(20):2877–2885
Berry RB, Kushida CA, Kryger MH, Soto-Calderon H, Staley B, Kuna ST (2012) Respiratory event detection by a positive airway pressure device. Sleep 35(3):361–367
Reiter J, Zleik B, Bazalakova M, Mehta P, Thomas RJ (2016) Residual events during use of CPAP: prevalence, predictors, and detection accuracy. J Clin Sleep Med 12(8):1153–1158
Patil SP, Ayappa IA, Caples SM, Kimoff RJ, Patel SR, Harrod CG (2019) Treatment of adult obstructive sleep apnea with positive Airway pressure: an American Academy of Sleep Medicine Clinical Practice Guideline. J Clin Sleep Med 15(2):335–343
Funding
This study is funded by NHLBI grant HL159259.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
The protocol for the reported study was approved by Yale University IRB.
Conflict of interest
Andira I. Anwar – no conflicts of interest. Sean Byrne – no conflicts of interest. Akanksha Sharma – no conflicts of interest. Scott Sands* is a consultant for NOX Medical, Apnimed, Lily, LingualFlex, Inspire, Respicardia, Forepont, Achaemenid. He received Industry grants from Prosomnus, Dynaflex and Apnimed. He has academic grants from National Institutes of Health (NIH) National Heart Lung and Blood Institute (NHLBI), American Academy of Sleep Medicine Foundation and American Heart Association. Andrew Wellman* works as a consultant for Apnimed, SomniFix and Nox, and has received grants from SomniFix and Sanofi. He has a financial interest in Apnimed, a company developing pharmacological therapies for sleep apnea. He has academic grants from NIH. Nancy S. Redeker – no conflicts of interest. Henry Yaggi - receives grant funding from NIH NHLBI. Henry Yaggi - receives grant funding from NIH NHLBI. Andrey V. Zinchuk has a financial interest in Restful Robotics, a company developing robotic solutions to positive airway pressure therapy and receives grant funding from NIH NHLBI as well as Parker B Francis Fellowship award. * The interests of Drs. Sands and Wellman are managed by Brigham and Women’s Hospital and Partners HealthCare in accordance with their conflict of interest policies.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Anwar, A.I., Byrne, S., Sharma, A. et al. Novel physiologic predictors of positive airway pressure effectiveness (NICEPAP) study: rationale, design and methods. Sleep Breath (2024). https://doi.org/10.1007/s11325-024-03099-w
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11325-024-03099-w