
Abstract
Purpose
The purpose of the research is to study the effect of acute inhibition of intravascular lipolysis on myocardial substrate selection during hypertriglyceridemia using in vivo radiotracer analysis and positron emission tomography.
Procedures
We induced acute hypertriglyceridemia in vivo using an intravenous infusion of Intralipid 20% (IL) without and with acute inhibition of fatty acid delivery from circulating triglycerides with injection of Triton WR-1339 (TRI) during a euglycemic–hyperinsulinemic clamp in Wistar rats. We determined the effect of TRI on myocardial uptake of circulating triglycerides and free fatty acids using intravenous injection of [3H]-triolein and [14C]-bromopalmitate, respectively. Myocardial blood flow, oxidative metabolism, and metabolic rate of glucose (MMRG) were determined using micro-positron emission tomography (μPET) with [13N]-ammonia, [11C]-acetate, and 2-deoxy-2-[F-18]fluoro-d-glucose (FDG).
Results
TRI reduced myocardial incorporation of [3H]-triolein but not [14C]-bromopalmitate showing that it selectively reduces myocardial fatty acid delivery from circulating triglycerides but not from free fatty acids. IL reduced myocardial blood flow and MMRG by 37% and 56%, respectively, but did not affect myocardial oxidative metabolism. TRI did not abolish the effect of IL on myocardial blood flow and MMRG.
Conclusions
Hypertriglyceridemia acutely reduces myocardial blood flow and MMRG in rats, but this effect is not explained by increased myocardial fatty acid delivery through intravascular triglyceride lipolysis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Approximately 60% to 70% of energy is derived from oxidation of fatty acids in the adult heart, while the rest is being provided mostly by glucose and lactate. Insulin resistant states and type 2 diabetes are associated with increased circulatory free fatty acid (FFA) and triglyceride fluxes [1] and with a very important increase in myocardial fatty acid utilization at the expense of reduced glucose utilization [2]. More reliance on fatty acid oxidation with reduced oxidation of glucose is associated with reduced energetic efficiency, more oxygen being required from the same cardiac workload [3]. This may pose a problem in critical situations such as during ischemia.
Increased FFA delivery to lean tissues, including the heart, reduces glucose utilization [4] (see [1] for review). Another potentially very important source of fatty acids to the heart is circulating triglyceride-rich lipoproteins. Because triglycerides circulate in the millimolar range and contain three fatty acids per molecule and because the heart highly expresses lipoprotein lipase (LpL) [5], this has been proposed as the major source of fatty acids to the heart [6]. Experimental evidence in perfused heart models [7, 8] and from in vivo studies in rodents [9, 10] have suggested that the heart is a major user of fatty acids derived from circulating triglycerides. Several genetically modified mouse models with either reduced [11–13] or increased [14, 15] myocardial LpL activity have demonstrated the potential of chronic modulation of myocardial fatty acid delivery from circulating triglycerides to change substrate selection and induce cardiomyopathy. However, changes in circulating triglyceride levels occur acutely after dietary fat intake. The impact of very acute changes in fatty acid delivery from circulating triglycerides on myocardial energy substrate selection is currently unknown.
The aim of the present study was to study the impact of myocardial fatty acid delivery from circulating triglycerides on myocardial glucose utilization in the presence or absence of intravenous infusion of Intralipid, a triglyceride emulsion, to simulate a hypertriglyceridemic state. Our hypothesis was that inhibition of myocardial fatty acid delivery from circulating triglycerides would lead to reversal of Intralipid-induced reduction of myocardial glucose utilization if this is a major source of fatty acid delivery to the heart in vivo (Fig. 1).

Myocardial fatty acid uptake from circulating triglycerides (TG) vs. circulating free fatty acids (FFA). TG contained in lipoproteins are hydrolyzed by lipoprotein lipase (LpL), a process that may contribute to myocardial fatty acid delivery with consequent reduction in myocardial glucose metabolism during acute hypertriglyceridemia. Triton WR-1339 is a detergent that binds circulating TG and prevents LpL-mediated triglyceride hydrolysis (intravascular lipolysis). The physiological processes that are described by the multi-compartmental analysis of fluoro-deoxyglucose (FDG) (i.e., K 1, k 2, k 3, and myocardial metabolic rate of glucose—MMRG) are also depicted.
Materials and Methods
Animals
Male Wistar rats (Charles River, Quebec, Canada) weighting 350–400 g were acclimatized to 12 h/day light cycle at constant temperature (22°C) for 7 days. A total of 63 rats were used for the experiments described herein. After a 12-h fasting period, animals were anesthetized with Isoflurane (Abbott laboratories, Montreal, Canada) delivered through a nose cone at a concentration of 2.0% (volume:volume). Anesthesia was maintained for the duration of the in vivo experiments. Catheters were placed into a carotid artery for blood sampling and into a jugular and two tail veins for intravenous infusions. The catheters were kept open with infusion of 0.9% saline. All animal protocols were approved by the Animal Ethics Committee of the Faculty of Medicine of the Université de Sherbrooke in accordance with the guidelines of the Canadian Council on Animal Care.
Experimental Protocols
All in vivo experiments described herein were initiated 60-min after insertion of catheters and performed under euglycemic–hyperinsulinemic conditions, as previously described [4]. At time 0 of the experiment, a primed (180 mU/kg) constant insulin infusion [12 mU/kg/min in 0.1% bovine serum albumin (BSA) in normal saline; Novolin®ge, Toronto, Canada] was started and continued for 2 h to standardize the metabolic condition in all in vivo protocols. Whole-blood glucose level was maintained using a variable 25% dextrose intravenous infusion according to the glucose level, determined every 10 min using a blood glucose monitor (Accusoft Advantage™, Roche, USA) [16]. Also at time 0, Triton WR-1339 (Tylaxapol, Sigma Chemicals, 400 mg/kg; referred to as the TRI group) vs. normal saline (referred to as the SAL group) was injected intravenously to inhibit intravascular triglyceride lipolysis during the experiment [17]. Our first set of in vivo experiments (Fig. 2a) was performed to validate the use of Triton WR-1339 to reduce fatty acid availability to tissues specifically derived from circulating triglycerides and not from plasma FFA. [1-14C]-2-bromopalmitate (a FFA tracer—injected in n = 18 animals) in 5% BSA (Moravek Biochemicals, California), 5 μCi, and 60 μCi of [1–3H]-triolein (a triglyceride tracer—injected in n = 15 animals) sonicated in 0.5 ml of Intralipid 20% were given intravenously at time 120 and 125 min, respectively, during the euglycemic–hyperinsulinemic clamp, as previously described [16], with and without intravenous administration of Triton WR-1339 as described above. Arterial blood samples were taken at time −0 and 0 min and at times 90, 100, 110, and 120 min to determine blood glucose and plasma insulin, FFA, and triglyceride levels. Blood samples were also taken at times 121, 123, and 125 to determine plasma [1-14C]-2-bromopalmitate and at times 126, 128, and 130 to determine plasma [1-3H]-triolein radioactivity, and organs were removed and processed to determine tissue tracer uptake as described below.

a Experimental protocol for the in vivo validation of Triton WR-1339 method. b Experimental protocol of the in vivo experiments using micro-positron emission tomography (μPET).
Imaging Protocols
Figure 2b depicts the imaging protocol used in our second set of in vivo experiments. To determine whether our in vivo imaging methods could detect change in myocardial metabolism with change in circulating lipids, we performed experiments using intravenous infusion of Intralipid 20% (20 μl/min) (IL) vs. saline (SAL) from time 0 and continued for the 2 h of the experiment. Intralipid is a chylomicron-like emulsion that may be employed to increase plasma triglyceride levels in vivo [18] and has been shown by others to be metabolized similarly as endogenous lipoproteins by the heart in rodents [6, 15]. In a third group of rats, we administered intravenous injection of Triton WR-1339 together with IL infusion (IL + TRI group) to determine the role of intravascular triglyceride lipolysis on any effect of IL on myocardial metabolism. Imaging experiments were performed with the avalanche photodiode-based small animal PET scanner (μPET) of the Sherbrooke Molecular Imaging Centre [19]. Before imaging, the heart position was localized with a Doppler probe (0.64 cm [1/4 in.], 9 MHz; Parks Medical Electronics). During imaging, the animals rested supine on the scanner bed and were kept warm with a heating pad. At time 50-min, approximately 5 mCi [13N]-ammonia in 0.5 ml of saline was administered intravenously over a period of 30 s using an automated injection system to determine myocardial blood flow [20]. This method had been shown to give similar estimates of myocardial blood flow when compared to the [15O]-water technique [21]. Image acquisition was performed using a 10-min list-mode dynamic acquisition. At time 70 min, an intravenous injection of approximately 3 mCi [11C]-acetate in 0.5 ml of saline was administered over 30 s to determine myocardial oxidative metabolic rate [22]. Image acquisition was also performed using a 10-min list-mode dynamic acquisition. At time 90-min, an intravenous injection of approximately 1 mCi 2-deoxy-2-[F-18]fluoro-d-glucose (FDG) in 0.5 ml of saline was given over a period of 30 s to determine myocardial glucose utilization. Image acquisition was performed using a 30-min list-mode dynamic acquisition. The PET imaging protocols were previously validated in other studies [23, 24]. Blood samples were taken at time 90, 100, 110, and 120-min to determine blood glucose and plasma FFA and TG.
Incorporation of Tracers into Plasma, Intracellular Lipids, and Mitochondria
Determination of uptake of plasma [1-3H]-triolein and [1-14C]-2-bromopalmitate into tissue lipids was performed as described previously [16]. Briefly, the heart was removed immediately and snap-frozen after thorough washing with 0.9% NaCl and blotting to remove excess water. Samples of heart (100 mg) were homogenized in a 0.9% NaCl solution. Plasma and tissue lipids were extracted according to the method described by Folch et al. [25] and were applied onto thin-layer chromatography plates (Silica Gel 60, F-254, Selecto Scientific, Suwanee, GA, USA) with standards for free fatty acids (FFA), triglycerides (TG), diglycerides (DG), monoglycerides (MG), cholesterol esters, and phospholipids. The plates were eluted in a hexane/diethyl ether/acetic acid (80:20:2) solution and stained with dichlorofluorescein (1 mg/mL ethanol). Relative uptake (%) of [14C] and [3H] in different tissue lipids was calculated by dividing the activity in each fraction by the total recovered in all fractions multiplied by 100.
Mitochondria from the heart were extracted by using the method previously described in [16, 25]. Briefly, 500 mg of the heart were homogenized on ice (PowerGen 125, Fisher Scientific International Inc., USA) in an ice-cold homogenization solution (0.075 M sucrose, 0.225 M sorbitol, 1 mM EGTA, 0.1% fatty-acid-free BSA, and 10 mM Tris–HCl, pH 7.4). The homogenates were centrifuged at 1,000 × g for 10 min at 4°C, and the supernatants were centrifuged again at 12,000 × g for 10 min at 4°C. The supernatants were then removed, and 1,000 μL of an incubation solution (10 mM Tris–HCl, 25 mM sucrose, 75 mM sorbitol, 100 mM KCl, 10 mM K2HPO4, 0.05 mM EDTA, 5 mM MgCl2, and 1 mg/mL FFA-free BSA) was added to the pellet containing mitochondria. Fifty microliters of the mitochondrial samples was kept frozen at −80°C for the measurement of glutamate dehydrogenase (GDH) activity to correct for the fractional recovery of mitochondria extracts from tissues [25]. The GDH activity was measured according to the Sigma quality control test procedure (EC 1.4.1.3, Enzymatic Assay of L-GDH) modified as previously described [16]. The fractional recovery of mitochondria was then calculated by dividing mitochondrial GDH activity (units per gram of tissue) by whole-tissue GDH activity (units per gram of tissue). Mitochondrial [14C] and [3H] activity were corrected by dividing by the fractional recovery to determine mitochondrial uptake of [1-14C]-2-bromopalmitate and [1-3H]-oleate from labeled triolein, respectively.
Imaging Data Analysis
For [13N]-ammonia and [11C]-acetate, dynamic series of 23 frames each were sorted out from the list mode data, using the following sequence: 1 × 30 s, 12 × 5 s, 8 × 30 s, 2 × 150 s. For FDG, a dynamic sequence series of 29 frames was sorted out using the following sequence: 1 × 30 s, 12 × 5 s, 8 × 30 s, 6 × 150 s, 2 × 300 s. Image planes were reconstructed on a 128 × 128 matrix with a 0.475 × 0.475 mm pixel size using the maximum likelihood expectation maximization algorithm with 15 iterations [26, 27]. Regions of interest (ROI) were drawn manually over the myocardium in the left ventricle and on the left ventricular cavity from the best frame image acquired with [13N]-ammonia acquisition and then used on all frames of the three tracers. Tissue time–activity curves were generated from the ROI on the myocardium, and the arterial tracer activity curve was obtained from the ROI drawn over the left ventricular cavity. The PET kinetic parameter values were assessed with the input function derived from the images. We used a three-compartment kinetic model for [13N]-ammonia that provides an estimate of blood flow from k 1 value [27]. For [11C]-acetate, we used a three-compartment kinetic model that estimates the generation of CO2 from the citric cycle in the myocardium using k 2 value [26]. For the modeling of myocardial uptake of FDG, we used the classical three-compartment model of Sokoloff [28]. According to this model, K 1 is an index of membrane glucose transport, k 2 is an index of FDG escape, k 3 is an index of glucose phosphorylation. The myocardial metabolic rate of glucose (MMRG) can be derived from these constants, the arterial blood glucose concentration, and the lumped constant (LC):
where LC is a term made up of six constants that relate the transport and phosphorylation kinetics of FDG to that for glucose [29].
Statistical Analysis
All data are reported as mean ± SE. Plasma glucose, insulin, FFA, and TG levels at steady state (baseline and between 90 to 120 min during the euglycemic clamp) were averaged for statistical analysis. Unpaired Student t test or one-way ANOVA with Tukey’s post hoc test were performed using GraphPad Prism version 5.00 for Windows (San Diego California USA). A P value of less than 0.05 was considered significant.
Results
Triton WR-1339 Selectively Reduces Myocardial Uptake of Circulating Triglycerides but not Circulating FFA
Blood glucose and plasma insulin, FFA, and triglyceride levels at baseline and during euglycemic–hyperinsulinemic clamp in rats injected with SAL vs. TRI are shown in Table 1. There was no significant difference in these parameters at baseline between the two groups. During the clamp, blood glucose and plasma FFA levels were similar between the two groups. As expected, plasma triglyceride levels were significantly increased approximately fourfold in TRI (P < 0.001). However, plasma insulin levels were lower in TRI vs. SAL (P = 0.04). This effect was explained by an in vitro interference of Triton WR1339 with the insulin immunoassay. This was further suggested by glucose infusion rates (GINF) that were virtually identical with and without TRI injection (Table 1).
Table 2 depicts the effect of injection of Triton WR-1339 on area under curve (AUC) of plasma 3H-triolein activity and on myocardial uptake and incorporation of 3H-triolein-derived 3H in cellular lipids and in mitochondria. TRI was associated with an ~168% increase of plasma 3H-triolein activity AUC (P = 0.02) and with ~48% (P = NS) and ~44% (P = 0.03) reductions in myocardial 3H-triolein-derived label uptake in cellular lipids and in mitochondria, respectively. However, TRI had no effect on relative uptake of 3H-triolein in the various cellular lipid fractions. Thus, Triton WR-1339 reduced myocardial fatty acid uptake from circulating triglycerides without change in partitioning into the different intracellular lipids.
In contrast, TRI had no significant effect on plasma [1-14C]-2-bromopalmitate AUC activity and on myocardial uptake of this tracer in cellular lipids and in mitochondria (Table 3). Furthermore, TRI did not affect relative uptake of [1-14C]-2-bromopalmitate into the various cellular lipid factions.
μPET Studies
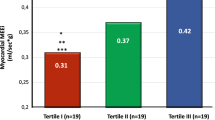
Weight of the animals was similar in SAL, IL, and IL + TRI experiments (387 ± 12, 387 ± 11, and 418 ± 14 g, respectively, P = 0.14). After surgery, heart rate and body temperature were also similar in all three groups (heart rate: 354 ± 14, 350 ± 21, and 303 ± 14 beats/min, respectively, P = 0.09; body temperature: 33.9 ± 0.7, 34.5 ± 0.4, and 35.1 ± 0.4°C, respectively, P = 0.30). Baseline blood glucose and plasma FFA levels were not significantly different between SAL, IL, and IL + TRI (blood glucose: 6.5 ± 0.7, 6.4 ± 0.7, and 5.9 ± 0.4 mmol/l, respectively, P = 0.81; baseline plasma FFA: 0.68 ± 0.12, 0.78 ± 0.06, and 0.72 ± 0.10 mmol/l, respectively, P = 0.81). Baseline plasma triglyceride levels were also not significantly different between the three groups (0.21 ± 0.02, 0.37 ± 0.09, and 0.25 ± 0.04 mmol/l, respectively, P = 0.17).
Table 4 shows the metabolic parameters of interest during the euglycemic–hyperinsulinemic clamp and μPET study. By design, plasma glucose levels were similar between the three experimental groups. Plasma FFA levels were significantly higher in IL and IL + TRI vs. SAL. Plasma triglyceride levels in IL and IL + TRI experiments were also significantly higher than SAL (P < 0.001). FDG K 1 and k 2 were similar in all three groups, whereas k 3 was significantly reduced in IL and IL + TRI compared with SAL (P = 0.02). MMRG (Fig. 3a) was significantly lower in IL and IL + TRI vs. SAL (P < 0.05). IL also significantly reduced myocardial blood flow ([13N]-ammonia k 1—Fig. 3b) vs. SAL (P < 0.05), whereas TRI did not significantly improve this IL-mediated reduction in blood flow. Total myocardial oxidative rate (11C-acetate k 2—Fig. 3c) was not significantly different between the three groups (P = 0.06), although it tended to be lower in the IL + TRI group vs. the two others. Figure 4 shows representative μPET scans after FDG injection in the three groups of rats.

a Myocardial metabolic rate of glucose (MMRG), b myocardial blood flow, and c total myocardial oxidative rate during euglycemic clamp in rats treated with saline (SAL, open bars), Intralipid 20% (IL, closed bars), and Intralipid 20% + Triton WR-1339 (IL + TRI, grey bars). a P < 0.05 vs. SAL group by ANOVA with Tukey’s post hoc test. Data are mean ± SE.

Representative myocardial transaxial μPET scan images after injection of [18F]FDG in the saline (SAL - upper panel), Intralipid 20% (IL - middle panel), and Intralipid 20% + Triton WR-1339 (IL + TRI - lower panel) groups.
Discussion
In the present study, IL resulted in increased plasma triglyceride and FFA levels together with significant reduction in MMRG and reduction in myocardial blood flow but no change in myocardial oxidative capacity, heart rate, or body temperature. In contrast to our initial hypothesis, we found no significant reversal of IL-induced reduction in MMRG with Triton WR-1339. Triton WR-1339 also did not reverse IL-induced reduction in myocardial blood flow. We demonstrated that Triton WR-1339 reduced clearance of circulating triglycerides and reduced myocardial uptake of triglycerides without significantly changing plasma FFA clearance and myocardial uptake. Thus, our results suggest that IL-induced reduction in blood flow and MMRG is not primarily caused by increased fatty acid delivery through increased intravascular triglyceride lipolysis during euglycemic–hyperinsulinemia in rats. Triton WR-1339 was not associated with change in insulin sensitivity, as assessed by lack of change in glucose infusion rates during euglycemic–hyperinsulinemic clamps. Plasma insulin levels were lower after injection of Triton WR-1339, but this effect was caused by interference of Triton WR-1339 with the insulin immunoassay used in the present study.
Our results are consistent with those of other investigators showing reduced myocardial glucose utilization with intravenous infusion of Intralipid in vivo [4, 30]. Intravenous infusion of lipids has also been previously shown to alter myocardial blood flow in other animal models [31, 32]. This lipid-induced reduction in myocardial blood flow could also be mediated by increased blood viscosity [33]. Interestingly, human LpL overexpression in aorta vascular smooth muscles in mice alters vascular reactivity [34], suggesting that lipolysis of triglycerides leads to endothelial dysfunction in vivo. However, injection of Triton WR-1339 did not blunt IL-induced reduction in myocardial blood flow. The lack of Intralipid-induced change in total myocardial oxidative metabolism that we observed in the present study is also consistent with results from other investigators [35].
One possible explanation for this finding may be compensatory increase in myocardial plasma FFA utilization in the presence of inhibition of myocardial utilization of fatty acids derived from circulating triglycerides. Indeed, this phenomenon has been shown to occur in mice using Langendorff ex vivo myocardial perfusion protocols in some [6, 15] but not all studies [7]. We found that blocking myocardial availability of fatty acids from circulating triglycerides did not affect myocardial 14C-bromopalmitate cellular and mitochondrial uptake. Thus, elevation of FFA levels seen with IL infusion may have been the primary cause of IL-mediated reduction in myocardial blood flow and MMRG. It is also possible that the hyperinsulinemic condition in our experiments reduced myocardial LpL activity [36], thus, minimizing the relative contribution of fatty acid uptake from circulating triglycerides. Finally, it is also possible that fatty acids delivered from circulating triglycerides do not acutely mix into the same intracellular fatty acid pool than that from plasma FFA [10], with different acute metabolic consequences. Intriguingly, total myocardial oxidative rate tended to be lower in the IL + TRI vs. IL group, an effect that may have been expected on the basis of reduced myocardial fatty acid delivery from circulating triglycerides in the face of no significant change in myocardial FFA uptake and similar MMRG.
Cardiac-specific LpL knockout and cardiac-specific LpL overexpression mouse models have illustrated the potential importance of prolonged lack or excess of fatty acid delivery from circulating triglycerides for the development of cardiomyopathy associated with change in myocardial glucose utilization [11–15]. However, the relative contribution of fatty acids derived from circulating triglycerides vs. plasma FFA pool as a substrate for the heart is controversial in physiological conditions. Results from some investigators have suggested that utilization rate of circulating triglyceride-derived fatty acids in the mouse heart is quantitatively lower [37], similar [7], or greater [6] to plasma FFA. These disparities are likely explained by different experimental and physiological conditions since myocardial fatty acid delivery from circulating triglycerides may depend on its lipoprotein source, and cardiac LpL function is modified in various conditions [38]. Interestingly, a recent human study has shown that plasma FFA contribute to more than 80% of fatty acids utilized by the heart in vivo in humans with coronary artery disease during the fasting state, whereas circulating triglycerides contribute to less than 20% [39].
Conclusion
In conclusion, the results from the present study show that intravenous infusion of fat emulsion acutely reduces myocardial glucose utilization and blood flow in vivo during euglycemic–hyperinsulinemia in rats. However, these effects do not result from increased delivery of fatty acids from intravascular triglyceride lipolysis. Future studies will be needed to determine whether myocardial fatty acid delivery from circulating triglycerides may play a role in reduced myocardial glucose utilization in pathophysiological states such as type 2 diabetes.
References
Carpentier AC (2008) Postprandial fatty acid metabolism in the development of lipotoxicity and type 2 diabetes. Diabetes Metab 34:97–107
Zhou YT, Grayburn P, Karim A, Shimabukuro M, Higa M, Baetens D, Orci L, Unger RH (2000) Lipotoxic heart disease in obese rats: implications for human obesity. Proc Natl Acad Sci USA 97:1784–1789
Chandler MP, Stanley WC, Morita H, Suzuki G, Roth BA, Blackburn B, Wolff A, Sabbah HN (2002) Short-term treatment with ranolazine improves mechanical efficiency in dogs with chronic heart failure. Circ Res 91:278–280
Nuutila P, Koivisto VA, Knuuti J, Ruotsalainen U, Teras M, Haaparanta M, Bergman J, Solin O, Voipio-Pulkki LM, Wegelius U (1992) Glucose-free fatty acid cycle operates in human heart and skeletal muscle in vivo. J Clin Invest 89:1767–1774
O’Brien KD, Ferguson M, Gordon D, Deeb SS, Chait A (1994) Lipoprotein lipase is produced by cardiac myocytes rather than interstitial cells in human myocardium. Arterioscler Thromb 14:1445–1451
Augustus AS, Kako Y, Yagyu H, Goldberg IJ (2003) Routes of FA delivery to cardiac muscle: modulation of lipoprotein lipolysis alters uptake of TG-derived FA. Am J Physiol Endocrinol Metab 284:E331–E339
Mardy K, Belke DD, Severson DL (2001) Chylomicron metabolism by the isolated perfused mouse heart. Am J Physiol Endocrinol Metab 281:E357–E364
Hauton D, Bennett MJ, Evans RD (2001) Utilisation of triacylglycerol and non-esterified fatty acid by the working rat heart: myocardial lipid substrate preference. Biochim Biophys Acta 1533:99–109
Augustus A, Yagyu H, Haemmerle G, Bensadoun A, Vikramadithyan RK, Park SY, Kim JK, Zechner R, Goldberg IJ (2004) Cardiac-specific knock-out of lipoprotein lipase alters plasma lipoprotein triglyceride metabolism and cardiac gene expression. J Biol Chem 279:25050–25057
Teusink B, Voshol PJ, Dahlmans VE, Rensen PC, Pijl H, Romijn JA, Havekes LM (2003) Contribution of fatty acids released from lipolysis of plasma triglycerides to total plasma fatty acid flux and tissue-specific fatty acid uptake. Diabetes 52:614–620
Augustus AS, Yagyu H, Haemmerle G, Bensadoun A, Vikramadithyan RK, Park SY, Kim JK, Zechner R, Goldberg IJ (2004) Cardiac-specific knockout of lipoprotein lipase alters plasma lipoprotein triglyceride metabolism and cardiac gene expression. J Biol Chem 279:25050–25057
Augustus AS, Buchanan J, Park TS, Hirata K, Noh HL, Sun J, Homma S, D’armiento J, Abel ED, Goldberg IJ (2006) Loss of lipoprotein lipase-derived fatty acids leads to increased cardiac glucose metabolism and heart dysfunction. J Biol Chem 281:8716–8723
Noh HL, Okajima K, Molkentin JD, Homma S, Goldberg IJ (2006) Acute lipoprotein lipase deletion in adult mice leads to dyslipidemia and cardiac dysfunction. Am J Physiol Endocrinol Metab 291:E755–E760
Yagyu H, Chen G, Yokoyama M, Hirata K, Augustus A, Kako Y, Seo T, Hu Y, Lutz EP, Merkel M, Bensadoun A, Homma S, Goldberg IJ (2003) Lipoprotein lipase (LpL) on the surface of cardiomyocytes increases lipid uptake and produces a cardiomyopathy. J Clin Invest 111:419–426
Pillutla P, Hwang YC, Augustus A, Yokoyama M, Yagyu H, Johnston TP, Kaneko M, Ramasamy R, Goldberg IJ (2005) Perfusion of hearts with triglyceride-rich particles reproduces the metabolic abnormalities in lipotoxic cardiomyopathy. Am J Physiol Endocrinol Metab 288:E1229–E1235
Ci X, Frisch F, Lavoie F, Germain P, Lecomte R, van Lier JE, Benard F, Carpentier AC (2006) The effect of insulin on the intracellular distribution of 14(R,S)-[(18)F]fluoro-6-thia-heptadecanoic acid in rats. Mol Imaging Biol 8:237–244
Taghibiglou C, Carpentier A, Rudy D, Aiton A, Lewis GF, Adeli K (2000) Mechanisms of hepatic VLDL overproduction in insulin resistance: evidence for enhanced lipoprotein assembly, reduced intracellular ApoB degradation, and increased microsomal triglyceride transfer protein in a fructose-fed hamster model. J Biol Chem 275:8416–8425, Ref Type: Journal (Full)
Carpentier A, Frisch F, Cyr D, Genereux P, Patterson BW, Giguere R, Baillargeon JP (2005) On the suppression of plasma non-esterified fatty acids by insulin during enhanced intravascular lipolysis in humans. Am J Physiol Endocrinol Metab 289:E849–E856
Lecomte R, Cadorette J, Rodrigue S, Lapointe D, Rouleau D, Bentourkia M, Yao R, Msaki P (1996) Initial results from the Sherbrooke avalanche photodiode positron tomograph. IEEE Trans Nucl Sci 43:1952–1957
Chen BC, Huang SC, Germano G, Kuhle W, Hawkins RA, Buxton D, Brunken RC, Schelbert HR, Phelps ME (1991) Noninvasive quantification of hepatic arterial blood flow with nitrogen-13-ammonia and dynamic positron emission tomography [see comments]. J Nucl Med 32:2199–2206
Nitzsche EU, Choi Y, Czernin J, Hoh CK, Huang SC, Schelbert HR (1996) Noninvasive quantification of myocardial blood flow in humans. A direct comparison of the [13N]ammonia and the [15O]water techniques. Circulation 93:2000–2006
Ng CK, Huang SC, Schelbert HR, Buxton DB (1994) Validation of a model for [1–11C]acetate as a tracer of cardiac oxidative metabolism. Am J Physiol 266:H1304–H1315
Bentourkia M, Croteau E, Langlois R, Aliaga A, Cadorette J, Bénard F, Lesur O, Lecomte R (2002) Cardiac studies in rats with [11C]acetate and PET: a comparison with [13N]Ammonia. IEEE Trans Nucl Sci 49:2322–2327
Lecomte R, Croteau E, Gauthier ME, Archambault M, Aliaga A, Rousseau J, Cadorette J, Leroux JD, Lepage MD, Bénard F, Bentourkia M (2004) Cardiac PET imaging of blood flow, metabolism and function in normal and infarcted rats. IEEE Trans Nucl Sci 51:696–704
Takala TO, Nuutila P, Pulkki K, Oikonen V, Gronroos T, Savunen T, Vahasilta T, Luotolahti M, Kallajoki M, Bergman J, Forsback S, Knuuti J (2002) 14(R, S)-[(18)F]Fluoro-6-thia-heptadecanoic acid as a tracer of free fatty acid uptake and oxidation in myocardium and skeletal muscle. Eur J Nucl Med Mol Imaging 29:1617–1622
Bentourkia M (2003) PET kinetic modeling of 11C-acetate from projections. Comput Med Imaging Graph 27:373–379
Croteau E, Benard F, Bentourkia M, Rousseau J, Paquette M, Lecomte R (2004) Quantitative myocardial perfusion and coronary reserve in rats with 13N-ammonia and small animal PET: impact of anesthesia and pharmacologic stress agents. J Nucl Med 45:1924–1930
Sokoloff L, Reivich M, Kennedy C, Des Rosiers MH, Patlak CS, Pettigrew KD, Sakurada O, Shinohara M (1977) The [14C]deoxyglucose method for the measurement of local cerebral glucose utilization: theory, procedure, and normal values in the conscious and anesthetized albino rat. J Neurochem 28:897–916
Krivokapich J, Huang SC, Selin CE, Phelps ME (1987) Fluorodeoxyglucose rate constants, lumped constant, and glucose metabolic rate in rabbit heart. Am J Physiol 252:H777–H787
Vettor R, Fabris R, Serra R, Lombardi AM, Tonello C, Granzotto M, Marzolo MO, Carruba MO, Ricquier D, Federspil G, Nisoli E (2002) Changes in FAT/CD36, UCP2, UCP3 and GLUT4 gene expression during lipid infusion in rat skeletal and heart muscle. Int J Obes Relat Metab Disord 26:838–847
Liedtke AJ, Nellis SH, Mjos OD (1984) Effects of reducing fatty acid metabolism on mechanical function in regionally ischemic hearts. Am J Physiol 247:H387–H394
Prinzen FW, Van der Vusse GJ, Coumans WA, Kruger R, Verlaan CW, Reneman RS (1981) The effect of elevated arterial free fatty acid concentrations on hemodynamics and myocardial metabolism and blood flow during ischemia. Basic Res Cardiol 76:197–210
Rim SJ, Leong-Poi H, Lindner JR, Wei K, Fisher NG, Kaul S (2001) Decrease in coronary blood flow reserve during hyperlipidemia is secondary to an increase in blood viscosity. Circulation 104:2704–2709
Esenabhalu VE, Cerimagic M, Malli R, Osibow K, Levak-Frank S, Frieden M, Sattler W, Kostner GM, Zechner R, Graier WF (2002) Tissue-specific expression of human lipoprotein lipase in the vascular system affects vascular reactivity in transgenic mice. Br J Pharmacol 135:143–154
Brown MA, Myears DW, Bergmann SR (1989) Validity of estimates of myocardial oxidative metabolism with carbon-11 acetate and positron emission tomography despite altered patterns of substrate utilization. J Nucl Med 30:187–193
Sambandam N, Abrahani MA, St Pierre E, Al Atar O, Cam MC, Rodrigues B (1999) Localization of lipoprotein lipase in the diabetic heart: regulation by acute changes in insulin. Arterioscler Thromb Vasc Biol 19:1526–1534
Neitzel AS, Carley AN, Severson DL (2003) Chylomicron and palmitate metabolism by perfused hearts from diabetic mice. Am J Physiol Endocrinol Metab 284:E357–E365
Ruge T, Wu G, Olivecrona T, Olivecrona G (2004) Nutritional regulation of lipoprotein lipase in mice. Int J Biochem Cell Biol 36:320–329
Nelson RH, Prasad A, Lerman A, Miles JM (2007) Myocardial uptake of circulating triglycerides in nondiabetic patients with heart disease. Diabetes 56:527–530
Acknowledgements
A.C.C. was supported by a Junior 2 Scholarship from the Fonds de la recherche en santé du Québec (FRSQ). The Centre de recherche clinique Etienne-Le Bel is a FRSQ-funded research centre. This work was supported by grants from Association Diabète Québec, from the Heart and Stroke Foundation of Canada (the Jonathan-Ballon Award), and from the Canadian Institutes of Health Research (MOP 53094 and MOP 15348).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ménard, S.L., Ci, X., Frisch, F. et al. Mechanism of Reduced Myocardial Glucose Utilization During Acute Hypertriglyceridemia in Rats. Mol Imaging Biol 11, 6–14 (2009). https://doi.org/10.1007/s11307-008-0171-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11307-008-0171-2