
Abstract
Objectives
To evaluate the feasibility of using the pulp volume (Pv) to total volume (Tv) ratio (Pv:Tv), obtained from cone beam computed tomography (CBCT) scans of single-rooted teeth, for age estimation in a Brazilian population sample.
Methods
After obtaining approval from the ethics committee, the study commenced by applying inclusion criteria to screen CBCT scans, resulting in a probability-based sample of participants aged 18 years and older (ranging from 18 to 82 years, with a mean age of 46.44 years). A total of 517 single-rooted teeth, including maxillary central incisors (CI), mandibular canines (C), and mandibular first premolars (FP), were chosen based on excellent agreement values (> 0.9). Pv and Tv measurements were conducted using semi-automatic segmentation with ITK-SNAP 3.8 software. Statistical analysis was performed using Jamovi software, with a significance level set at 5% (α = 0.05).
Results
A strong negative correlation (r > −0.7) was observed between chronological age and the Pv:Tv ratio across all examined teeth. However, when conducting regression analysis with Pv:Tv data and chronological age as the independent variable, only the mandibular FP teeth exhibited a normal distribution. The resulting linear model demonstrated moderate predictive value (approximately 64%) in explaining the variance in chronological age, but caution should be exercised when interpreting these findings.
Conclusions
The method of measuring individual tooth volume using CBCT to estimate chronological age via Pv:Tv has been demonstrated as effective and reproducible within the Brazilian population sample.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In addition to DNA analysis and fingerprint comparisons, teeth play a crucial role in human identification due to their resilience to postmortem changes, both macroscopically and microscopically. Furthermore, the determination of chronological age holds significance in various legal domains, such as ascertaining the age of undocumented individuals to prevent child labor or address civil and criminal liability, determining eligibility for retirement and pension benefits, and aiding in forensic investigations [1].
Within the field of dentistry, multiple methods [2,3,4,5,6,7] have been employed to estimate age by evaluating bones and teeth. However, teeth exhibit greater resistance to external factors compared to bones, experiencing fewer changes and alterations over time. They serve as a primary focus in dental practice, monitored by dentists through clinical and radiographic examinations throughout an individual's lifespan. In children, age estimation has traditionally relied on assessing root development. For adults, alternative methods have been developed following the completion of root development.
One such method for age estimation in adults involves measuring pulp volume (Pv), serving as an indirect measure of the secondary dentin deposition that occurs in the oral cavity shortly after tooth eruption. However, variations in the pattern of dentin deposition over time have been noted in different populations, rendering age determination through dental analysis inaccurate when using regression models developed from populations with distinct characteristics [7]. Therefore, age estimation becomes more relevant when associated with the total volume (Tv) of the assessed tooth. External factors, such as diet consistency or parafunctional habits like bruxism or clenching, could influence dentin deposition and the overall size of the tooth. Additionally, the phenotypic characteristics of the tooth, which can vary in size, may also play a role, depending on the population's traits.
Despite various studies conducted on Brazilian adults [4, 8,9,10], which employed diverse methodologies and covered different regions of the country [11], there persists a need for research specifically focusing on the pulp/total volume ratio (Pv:Tv) within the Brazilian population. This is crucial to advance scientific evidence on the use of teeth for age estimation and to formulate an equation model tailored to the population's characteristics. Thus, the objective of this study is to assess the applicability of Pv:Tv derived from single-rooted teeth in cone beam computed tomography (CBCT) for age estimation within a sample to the Brazilian population. The study aims to rigorously test the hypothesis that there is no significant relationship between Pv:Tv and chronological age, serving as the null hypothesis.
Material and methods
The documentary research commenced after obtaining approval from the Human Research Ethics Committee (CAAE 39558720.7.0000.5626), adhering to the principles outlined in the Declaration of Helsinki. Subsequently, individuals with existing CBCT scans were approached and informed about the study. Those consenting to participate and permitting the utilization of their prior CBCT scans signed the Informed Consent Form (ICF). These CBCT scans, originally acquired for diverse dental purposes unrelated to this study, formed the basis of our research.
Inclusion criteria for screening CBCT scans for probability sampling included high resolution and sharpness, participants aged over 18 years, voluntary consent through the signed ICF, absence from vulnerable groups, capacity to comprehend and decide to participate, and inclusion of both maxillary and mandibular arches in the same scan. Further criteria encompassed a single-rooted tooth with no caries lesions, extensive restorations, prosthetic crown, endodontic treatment, pulp calcifications, or developmental/acquired anomalies affecting tooth shape. Chronological age was determined using the standard definition of age in full years, with months rounded following specified rules: 1–5 months rounded down, 6–11 months rounded up.
The minimum sample size required was determined based on a previous study in a Brazilian sample [4], which found a correlation between chronological age and pulp volume with approximate values of Pearson's r of −0.8 and a coefficient of determination (ρ2) of 0.7. Therefore, the sample size calculation was performed using G*Power 3.1.9.4 software (Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany). An a priori analysis with t-tests of correlation, point biserial model, assumed an effect size of one tail(s), effect size |ρ|= 0.84, α err prob = 0.05, power (1−β err prob) = 0.95, and the output was nocentrality parameter δ = 4.04, critical t = 2.01, Df = 5, defining a total sample size of 7 with an actual power of 0.96.
A probabilistically stratified sample by age was selected through sequential review of medical records with CBCT scans performed between 2019 and 2020. The review continued until all age groups in each tooth type by gender reached the required minimum sample size (N = 7), employing age stratification defined by quartiles.
All CBCT scans were acquired using the Pax i3D Smart Tomography system (Vatech Company Limited, South Korea) employing standardized exposure parameters: 84 kVp, 4–16 mA, 0.5 mm focal spot, 14-bit grayscale, 10 cm × 8.5 cm FOV, 18.2 s scan time, and 0.2 mm voxel slice thickness. Additionally, image processing and measurements were performed on an HP Ryzen 7 2700 computer (HP, Palo Alto, California, USA), equipped with 16 GB RAM, 256 GB SSD HD, an 8 GB graphics card, a mouse with 1000 dpi sensitivity, and a 23-inch monitor boasting a resolution of 1920 × 1080. The computer operated on the Windows 10 platform (Microsoft, Redmond, Washington, USA).
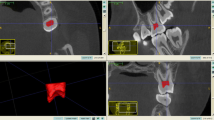
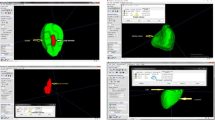
The resultant images were exported in DICOM format to the open-source software ITK-SNAP 3.8 (U.S. National Institute of Biomedical Imaging and Bioengineering, Philadelphia, Pennsylvania, USA). Single-rooted tooth measurements were obtained through semi-automatic segmentation using active contour methods, as depicted in Fig. 1, within ITK-SNAP 3.8 software (National Institute of Biomedical Imaging and Bioengineering). Adhering to the segmentation instructions outlined in the software manual, three-dimensional images were segmented, yielding Tv and Pv, expressed in cubic millimeters (mm3).

Illustration depicting the semi-automatic segmentation process using the active contour method. A represents the total volume (Tv), and B represents the pulp volume (Pv)
For statistical analysis, age, gender, and volume data (Pv and Tv) were collected from single-rooted tooth groups, encompassing both right and left sides, that exhibited excellent agreement (ICC > 0.9). Within the scope of all evaluated single-rooted teeth, these groups exclusively included the maxillary central incisors (CI) (teeth 11 and 21 in the FDI two-digit system), the mandibular canines (C) (teeth 33 and 43), and the mandibular first premolars (FP) (teeth 34 and 44). Subsequently, the volume ratio (Pv:Tv) was calculated. Measurement normality was assessed using the Shapiro–Wilk and Anderson–Darling tests. Statistical analyses, comprising ANOVA with Kruskal–Wallis test, Mann–Whitney test, Pearson correlation, and linear regression analyses, were performed using Jamovi software version 2.3, with a significance level of 5% (α = 0.05).
Results
The study included 130 CBCT scans (Table 1) collected from participants aged 18 to 82, with a mean age of 46.44, as illustrated in Table 2. A total of 517 teeth were sampled, employing the tooth as the sampling unit (N). The sample was stratified by gender, age group, and tooth type (Table 3). Age stratification into four groups by quartiles was essential to meet the minimum sample size requirement (N = 7) for each gender and tooth type, as depicted in Table 3. This was necessitated by a reduction in the number of teeth meeting the inclusion criteria as age increased (due to missing data).
A statistically significant decrease (p < 0.05) in Pv and Pv:Tv was observed with increasing age, as evidenced in Table 4. However, this progressive decrease was not evident in Tv (p > 0.05), except for mandibular FP teeth, where random statistical differences were noted. The variation of Pv and Pv:Tv between gender, as highlighted in Table 5, did not exhibit statistical significance (p > 0.05). Only Tv in mandibular C and mandibular FP teeth displayed a statistically significant variation (p < 0.05), being greater in volume in males. No statistical differences (p > 0.05) were identified when comparing contralateral teeth on the right side with those on the left side, as presented in Table 6.
In the correlation between chronological age and Pv:Tv, Pearson's correlation coefficient revealed a strong negative correlation (r > −0.7) across all studied teeth. This correlation was most pronounced in mandibular C (r ≅ −0.84), followed by mandibular FP (r ≅ −0.80) and maxillary CI (r ≅ −0.78) (Table 7). However, based on the normality analysis and residuals depicted in Fig. 2, only mandibular FP teeth exhibited a normal distribution, a prerequisite for conducting regression analysis. The regression analysis in Table 8 utilized Pv:Tv data from mandibular FP teeth, with chronological age as the independent variable. The resulting regression equation, presenting a linear model explaining 64% of the age variance, is illustrated in Fig. 3.

Assessment of normality assumptions for the Pv:Tv data through the Shapiro–Wilk test and Q–Q plot of the residuals, essential for conducting the regression analysis. Subplots depict the analysis for maxillary central incisor (CI) teeth (A), mandibular canine (C) teeth (B), and mandibular first premolar (FP) teeth (C)

Scatterplot presenting the Pv:Tv data of mandibular FP teeth in relation to chronological age, along with the regression analysis equation
Discussions
Among all single-rooted teeth, only the maxillary CI, mandibular C, and mandibular FP were chosen for analysis in the present study. This selection was based on their established superior reproducibility calibration, as validated in prior investigations [3, 12]. The exclusion of mandibular incisors was necessitated by their limited volume, posing challenges in obtaining accurate and reproducible measurements. Maxillary lateral incisors were omitted due to their susceptibility to anatomical changes with volume variations. Additionally, considering the inclusion criteria, maxillary canines were excluded due to an insufficient number in this specific sample across all age groups. Consequently, mandibular FP teeth exhibited the most reliable characteristics, serving as the basis for proposing a regression model and proving to be an effective predictor of age. However, despite their high correlation with age, both maxillary CI and mandibular C did not demonstrate a normal distribution, violating a necessary condition for a regression model. Previous studies [13,14,15,16] consistently identified maxillary CI, mandibular C, and mandibular FP as teeth with the strongest correlations with age, aligning with our study results. Other studies [5, 12] also acknowledged molars as highly correlated with age estimation, primarily due to the uniform distribution of secondary dentin in their pulp chambers. However, molars' susceptibility to carious lesions over time makes them less suitable for age estimation, especially in older age groups. Premolars, while less robust than molars, have fewer variations that might render them unsuitable for analysis, such as carious lesions, restorations, or other shape-related confounding factors. This was confirmed in our sample, affirming that among the evaluated teeth, mandibular FP teeth are the most suitable for age estimation.
The decline in Pv with age is apparent in all measured teeth, attributed to the continuous deposition of secondary dentin in the pulp chamber post-tooth eruption. This process is influenced by physiological tooth wear, leading to an augmented deposition of secondary dentin [17]. The substantial reduction in pulp volume with chronological age enhances the accuracy of age estimation. However, relying solely on secondary dentin deposition for chronological age estimation in cross-sectional studies is a mistake. Establishing the true relationship between Pv and Tv over time would necessitate a cohort study tracking the same teeth. Unfortunately, such cohort studies are lacking in the literature [1, 7, 12], making Pv:Tv the preferred method for cross-sectional studies like ours. Pv:Tv not only considers secondary dentin formation but also maintains a direct relationship with the Tv. While a decrease in Pv:Tv was observed with aging, the decline in Pv was more pronounced than in Tv [18]. Thus, Pv:Tv accommodates interpersonal variation in Pv arising from larger or smaller tooth sizes.
In the current investigation, the Pv:Tv ratio of mandibular FP single-rooted teeth demonstrated a robust fit for age prediction based on CBCT measurements, satisfying the necessary normality condition for regression analysis. Nevertheless, despite literature reviews [7, 12] indicating the effectiveness of age prediction methods using teeth, there exists substantial methodological variation among the included studies, and there is a lack of clarity regarding statistical controls for regression analysis. Additionally, a refined methodology for sample selection, with a precise definition of factors included as sampling units or specifying the number of units per age, is notably absent [19]. This proved to be particularly challenging in our study due to the introduced randomness and defined inclusion criteria.
Furthermore, while there are no specific guidelines for CBCT use in forensic practice, adherence to an in vivo dose limit for biosafety and the ALADAIP principle, "As Low As Diagnostically Acceptable being Indication-oriented and Patient-specific," should be a steadfast practice in dental and maxillofacial radiology [20]. Regardless of the application, there must be a justified limit for patient exposure in all instances. For instance, CBCT scans for population screening based on specific characteristics may lack justification. Moreover, the percentage of variation explained by linear regression models in a prior study [9] reached a maximum of approximately 85% when applied to single-rooted teeth, consistent with our current findings (approximately 84%). Most studies [7] reported results below this threshold, a trend also confirmed by our study in other dental groups. These outcomes underscore the imperative need and scientific importance of developing more accurate age estimation methods tailored to particular populations.
The studies [21, 22], which employed micro-CT with superior resolution compared to the present study, demonstrated similar results, despite achieving increased accuracy in detecting the border between the pulp and hard tissues for segmentation. They also found that age estimation using micro-CT is effective. However, the use of CBCT in the present study is more applicable in cases where higher resolution imaging, such as micro-CT, is unavailable or impractical, particularly when extracted teeth are not an option or previous images of living patients are used.
A noteworthy aspect of our study is the consideration of age estimation in scenarios where biological sex is unavailable during the initial examination, such as when teeth serve as the best-preserved evidence or when opting for a more conservative and less expensive method. Consequently, sex was not differentially weighted in the estimates. Pv:Tv did not exhibit statistically significant differences between females and males in any evaluated tooth type, as determining sex during early age screening events proves challenging [4]. In the adult phase, before resorting to more expensive analyses like DNA testing, age determination becomes the most crucial identifying factor. Thus, utilizing CBCT is clinically relevant as a widely available diagnostic method applicable in various settings and for forensic purposes.
Contrary to our expectations, changes in Tv with age did not follow a progressive pattern, challenging the assumption of a consistent decrease in tooth size due to natural aging. The observed random fluctuations in Tv suggest that individual characteristics, such as genetically inherited tooth size and habits acquired during occlusal development, may play a more significant role than age itself. Additionally, no variation was detected between contralateral teeth on the right and left sides of CBCT images, dispelling any indications of parafunctional habits as reported in a prior study [13]. This outcome can be attributed to the characteristics of our sampled population, deliberately avoiding ethnic or sexual clustering, and replicating a realistic practical situation that requires age determination irrespective of these factors.
Furthermore, creating more homogenous clusters in highly miscegenated populations, like the Brazilian one [11, 12], would necessitate larger samples, rendering the study impractical, especially when adhering to principles of randomness. While the study's limitation lies in sample size, our strategy to overcome this involved age stratification until the required minimum N was reached, maintaining randomness according to established inclusion criteria. This meticulous control has not been observed in previous studies.
Given the limitations of our study, we advise caution in applying the method of measuring individual tooth volume by CBCT to derive Pv:Tv for chronological age estimation, despite its demonstrated effectiveness and reproducibility within a Brazilian population sample. The formula derived from the regression model demonstrates a moderate predictive value of approximately 64%. Then, it is crucial to note that this formula can only explain approximately 64% of the variability in estimated age, leaving 36% unaccounted for, introducing a margin of error in age estimation. Consequently, inaccuracies in estimated age may arise, especially in cases with high variability where unconsidered factors could impact results. The method's limited precision makes it unsuitable for precise age determination, but it may be useful for age group categorization. Additionally, it is important to emphasize that the predictive capability for age is not universally applicable across all studied teeth but is specifically attributed to the mandibular FP tooth. Therefore, we recommend employing this method selectively in targeted scenarios, particularly for differentiating age groups among individuals.
Conclusion
Based on the findings of this study, our conclusion supports the acceptance of the alternative hypothesis. The relationship between the Pv:Tv, derived from single-rooted teeth using CBCT, and chronological age was found to be significant within the sample of the evaluated Brazilian population. The data obtained suggest that this measurement can effectively estimate age, with moderate precision, utilizing the mandibular FP tooth and the regression model-derived formula, especially in scenarios where biological sex is unavailable during the initial assessment, underscoring its potential value in forensic and diagnostic contexts.
These results contribute to the growing body of scientific evidence regarding the applicability of tooth-based imaging methods with CBCT for age estimation, particularly in a particular population. However, it is essential to acknowledge the study's limitations and advocate for further research to enhance the understanding of this relationship in diverse populations and clinical contexts.
References
Verma M, Verma N, Sharma R, Sharma A. Dental age estimation methods in adult dentitions: an overview. J Forensic Dent Sci. 2019. https://doi.org/10.4103/jfo.jfds_64_19.
Patil V, Saxena J, Vineetha R, et al. Age assessment through root lengths of mandibular second and third permanent molars using machine learning and artificial neural networks. J Imaging. 2023. https://doi.org/10.3390/jimaging9020033.
Gulsahi A, Kulah CK, Bakirarar B, Gulen O, Kamburoglu K. Age estimation based on pulp/tooth volume ratio measured on cone-beam CT images. Dentomaxillofac Radiol. 2018. https://doi.org/10.1259/dmfr.20170239.
Andrade VM, Fontenele RC, de Souza AC, et al. Age and sex estimation based on pulp cavity volume using cone beam computed tomography: development and validation of formulas in a Brazilian sample. Dentomaxillofac Radiol. 2019. https://doi.org/10.1259/dmfr.20190053.
Zheng Q, Ge Z, Du H, Li G. Age estimation based on 3D pulp chamber segmentation of first molars from cone-beam-computed tomography by integrated deep learning and level set. Int J Legal Med. 2021. https://doi.org/10.1007/s00414-020-02459-x.
Kazmi S, Mânica S, Revie G, Shepherd S, Hector M. Age estimation using canine pulp volumes in adults: a CBCT image analysis. Int J Legal Med. 2019. https://doi.org/10.1007/s00414-019-02147-5.
Merdietio Boedi R, Shepherd S, Mânica S, Franco A. CBCT in dental age estimation: a systematic review and meta analysis. Dentomaxillofac Radiol. 2022. https://doi.org/10.1259/dmfr.20210335.
Porto LV, Celestino da Silva Neto J, Anjos Pontual AD, Catunda RQ. Evaluation of volumetric changes of teeth in a Brazilian population by using cone beam computed tomography. J Forensic Leg Med. 2015. https://doi.org/10.1016/j.jflm.2015.07.007.
Miranda JC, Azevedo ACS, Rocha M, Michel-Crosato E, Biazevic MGH. Age estimation in Brazilian adults by Kvaal’s and Cameriere’s methods. Braz Oral Res. 2020. https://doi.org/10.1590/1807-3107bor-2020.vol34.0051.
Dezem TU, Franco A, Machado Palhares CE, et al. Testing the Olze and Timme methods for dental age estimation in radiographs of Brazilian subadults and adults. Acta Stomatol Croat. 2021. https://doi.org/10.15644/asc55/4/6.
Calvo-González E, Ventura SR. Problematizing miscegenation: the fact/fiction of race in contemporary Brazil. J Anthropol Sci. 2018. https://doi.org/10.4436/JASS.96013.
Yousefi F, Mohammadi Y, Ahmadvand M, Razaghi P. Dental age estimation using cone-beam computed tomography: a systematic review and meta-analysis. Imaging Sci Dent. 2023. https://doi.org/10.5624/isd.20221226.
Uğur Aydın Z, Bayrak S. Relationship between pulp tooth area ratio and chronological age using cone-beam computed tomography images. J Forensic Sci. 2019. https://doi.org/10.1111/1556-4029.13986.
Santos MA, Muinelo-Lorenzo J, Fernández-Alonso A, Cruz-Landeira A, Aroso C, Suárez-Cunqueiro MM. Age Estimation using maxillary central incisor analysis on cone beam computed tomography human images. Int J Environ Res Public Health. 2022. https://doi.org/10.3390/ijerph192013370.
Nemsi H, Haj Salem N, Bouanene I, et al. Age assessment in canine and premolar by cervical axial sections of cone-beam computed tomography. Leg Med. 2017. https://doi.org/10.1016/j.legalmed.2017.07.004.
Cameriere R, De Luca S, Alemán I, Ferrante L, Cingolani M. Age estimation by pulp/tooth ratio in lower premolars by orthopantomography. Forensic Sci Int. 2012. https://doi.org/10.1016/j.forsciint.2011.07.028.
Agematsu H, Someda H, Hashimoto M, et al. Three-dimensional observation of decrease in pulp cavity volume using micro-CT: age-related change. Bull Tokyo Dent Coll. 2010. https://doi.org/10.2209/tdcpublication.51.1.
De Angelis D, Gaudio D, Guercini N, et al. Age estimation from canine volumes. Radiol Med. 2015. https://doi.org/10.1007/s11547-015-0521-5.
De Tobel J, Ottow C, Widek T, et al. Dental and skeletal imaging in forensic age estimation: disparities in current approaches and the continuing search for optimization. Semin Musculoskelet Radiol. 2020. https://doi.org/10.1055/s-0040-1701495.
Kühnisch J, Anttonen V, Duggal MS, et al. Best clinical practice guidance for prescribing dental radiographs in children and adolescents: an EAPD policy document. Eur Arch Paediatr Dent. 2020. https://doi.org/10.1007/s40368-019-00493-x.
Aboshi H, Takahashi T, Komuro T. Age estimation using microfocus X-ray computed tomography of lower premolars. Forensic Sci Int. 2010. https://doi.org/10.1016/j.forsciint.2010.03.024.
Asami R, Aboshi H, Iwawaki A, Ohtaka Y, Odaka K, Abe S, Saka H. Age estimation based on the volume change in the maxillary premolar crown using micro CT. Leg Med (Tokyo). 2019. https://doi.org/10.1016/j.legalmed.2018.12.001.
Acknowledgements
Thanks to the volunteer participants who provided their CBCT exams for use in the study and to the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES), which partially funded this study—Finance Code 001.
Funding
Coordenação de Aperfeiçoamento de Pessoal de Nível Superior, 001, Ana Beatriz Raposo SOUZA
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
We wish to disclose that there are no direct or potential conflicts of interest associated with this study. Furthermore, it is pertinent to mention that this research received partial funding through indirect support to the graduate program in which the study was conducted, as acknowledged in the acknowledgments section.
Ethical approval
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation Faculty of Dentistry of Nova Friburgo at the Federal Fluminense University and with the Helsinki Declaration of 1975, as revised in 2008 (5).
Informed consent
Informed consent was obtained from all patients for being included in the study. Identifying information of patients or human subjects is not included in the article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Souza, A.B.R., Cruz, A.D. & Aguiar, M.F. Age estimation by volumetric analysis of teeth using cone beam computed tomography. Oral Radiol 40, 436–444 (2024). https://doi.org/10.1007/s11282-024-00750-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11282-024-00750-w