
Abstract
Objectives
Sella turcica bridging occurs with fusion or calcification of the anterior and posterior clinoid processes in the middle cranial region. This study aimed to compare the cephalometric parameters among normal shape, partial bridge, and total bridge of the sella turcica in adolescent and young adult subjects.
Methods
This retrospective study was performed on the lateral cephalometric radiographs of 410 Turkish adolescent and young adult subjects. The subjects were divided into three groups: normal sella turcica shape (128 females, 32 males; mean age: 17.7 ± 1.54 years), partial sella turcica bridge (129 females, 32 males; mean age: 17.8 ± 2.15 years), and total sella turcica bridge (66 females, 23 males; mean age: 18.2 ± 1.82 years). Thirteen angular and eight linear cephalometric measurements were performed using a cephalometric software program. The data were analyzed by one-way analysis of variance, and the Kruskal–Wallis test with the Bonferroni correction.
Results
Significant differences were found for Nperp–A distance, Nperp–Pg distance, and palatal plane-to-anterior cranial base angle among the groups (p < 0.016). There were no significant differences in the cephalometric parameters between the partial and total sella turcica bridging groups (p > 0.05).
Conclusions
This study evaluated a large amount of data for cephalometric measurements focusing on the degree of calcification of the sella turcica in adolescent and young adult subjects. The maxilla and mandible were located in a sagittally retrusive position in the partial and total sella turcica bridge subjects compared with the normal sella turcica shape subjects.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The sella turcica, which hosts the pituitary gland, is a saddle-shaped anatomical region in the sphenoid bone located in the middle cranial fossa of the skull [1]. It consists of anterior and posterior clinoid extensions and the central pituitary gland. The clinoid extensions are connected to one another by a dura mater horizontal layer defined as the interclinoid dural layer, interclinoid ligament, or fibrous ligament [2]. Regarding the name, the word “Sella” is derived from the Latin word “sedes” or “sedula”, meaning armchair, stool or saddle, and the word “Turcica” means Turkish [3]. The sella point, which is located in the geometric center of the sella turcica, is frequently used as an anatomical reference point in orthodontic and orthognathic surgery planning. The sella turcica morphology is important for not only evaluation of cranial morphology and late-period growth changes, but also orthodontic and orthognathic treatment results [4].
Studies have shown that the sella turcica morphology does not undergo any significant changes after 12 years of age, and that its anterior wall is stable from 5 years of age [5]. Many researchers who examined lateral cephalometric radiographs of children and adults have described morphological variations of the sella turcica, including calcification of the interclinoid ligaments or sella turcica bridging (STB) [6]. STB occurs when the anterior and posterior clinoid extensions become merged. The anatomy of the sella turcica can vary among individuals, and the sizes and shapes of the clinoid extensions can also vary [5].
While the prevalence of STB generally ranges from 1.1 to 13%, its incidence is increased in people with severe craniofacial deviation [7, 8]. Changes in the sella turcica morphology frequently arise through congenital malformations. Syndromes may be present in patients with altered sella turcica morphology or STB [9]. Severe morphological variations of the sella turcica are more frequently observed in syndromic patients such as those with Down syndrome, Williams syndrome, Seckel syndrome, and Axenfeld–Rieger syndrome [1, 9].
The sella turcica and teeth originate and develop from neural crest cells. The anterior part of the sella turcica develops completely from neural crest cells, while the progenitor cells for tooth epithelia differentiate through consecutive and mutual interactions with the neural crest-derived mesenchyme. There may be correlations between anatomic deviations in the sella turcica and craniofacial structure or dental anomalies. This possibility has led many researchers to investigate the relationships between STB and dental anomalies. Studies have proven the presence of associations between STB and palatally impacted canine teeth and dental transposition [7]. Furthermore, any cranial structural deviation in the anterior wall of the sella turcica is considered to be associated with deviation in the craniofacial anatomy because it develops from neural crest cells in the early embryonic period in the anterior wall area of sella turcica.
The development of the craniofacial region may be related to the development of the sella turcica. Malformations in sella turcica development may affect the maxillary, mandibular, and nasal anatomic regions and other related craniofacial structures [10]. The purpose of the present study was to compare the orthodontic cephalometric values in adolescent and young adult subjects with partial or total STB with those in individuals with a normal sella turcica shape.
Methods
This retrospective study was carried out on Turkish adolescent and young adult subjects by selecting pretreatment records containing digital lateral cephalometric radiographs for measurement of the sella turcica dimensions in the Orthodontics Department archive of Ordu University, Ordu, from November 2012 to June 2017. The inclusion criteria were good-quality lateral cephalometric radiographs. The exclusion criteria were history of orthodontic treatment or orthognathic surgery, craniofacial anomaly, congenital syndrome, history of facial trauma, skull surgery, and poor-quality lateral cephalometric radiographs.
The sample size was calculated by a power analysis using G*Power Software version 3.1.9.2 (Universität Düsseldorf, Düsseldorf, Germany) for the SN–GoMe angle with an alpha error probability of 0.05 and a power of 85% [11]. The power analysis showed that a minimum of 85 subjects per group was required for the study. The study subjects were divided into three groups according to the calcification of the anterior and posterior processes of the sella turcica as normal sella turcica shape (128 females, 32 males; mean age: 17.7 ± 1.54 years), partial STB (129 females, 32 males; mean age: 17.8 ± 2.15 years), and total STB (66 females, 23 males; mean age: 18.2 ± 1.82 years).
The lateral cephalometric radiographs were obtained by the same technician using the same cephalometric film device (Kodak 8000C Digital Panoramic and Cephalometric System, Cephalostat; Corestream Health Inc., Rochester, NY, USA). All participants were positioned in the cephalostat with the sagittal plane at a right angle to the X-ray path, the Frankfort plane parallel to the ground plane, the teeth in centric occlusion, and the lips in the rest position.
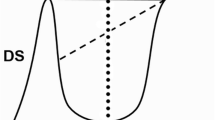
In this study, the standard scale developed by Leonardi et al. [12] was used to evaluate the degree of STB. According to the sella turcica anatomical shape, the sella turcica was divided into three groups (Fig. 1): normal sella turcica shape (no calcification), length greater than three-quarters of the diameter; partial STB (partial calcification), length less than or equal to three-quarters of the diameter; total STB (complete calcification), visible contact between the tuberculum sella and the dorsum sella.

a Normal sella turcica (no calcification). b Partial sella turcica bridge (partial calcification). c Total sella turcica bridge (complete calcification)
All lateral cephalometric radiographs were traced, landmarked, and measured by the same researcher (A.K.) with 4 years of experience in orthodontics. The craniofacial parameters were evaluated with Facad trial version 3.8 software (Ilexis AB, Linkoping, Sweden) as shown in Fig. 2.

Lateral cephalometric orthodontic parameters. (1) Nperp–A distance; (2) Nperp–Pg distance; (3) palatal plane-to-anterior cranial base angle
Statistical analysis
All measurements were analyzed by entering the data into SPSS for Windows version 20.0 software (IBM Corp., Armonk, NY, USA). After performing a normal distribution test, non-parametric tests were applied to parameters with a non-normal distribution, and parametric tests were applied to parameters with a normal distribution. The data were analyzed by one-way analysis of variance, and the Kruskal–Wallis test with the Bonferroni correction for multiple comparisons. Values of p < 0.05 were considered significant.
Results
The study was carried out on lateral cephalometric radiographs of 410 individuals (323 females and 87 males) with randomly selected normal sella turcica shape, partial STB, and total STB according to the inclusion criteria among a total of 2918 lateral cephalometric radiographs. The demographic characteristics of the subjects in the three groups are shown in Table 1. There was no significant difference in age among the groups (p > 0.05).
The cephalometric parameters are shown in Table 2. Nperp–A distance, palatal plane-to-SN angle, and anterior facial height differed significantly between the subjects with normal sella turcica shape and partial STB (p < 0.05). Nperp–A distance and palatal plane-to-SN angle also differed significantly between subjects with normal sella turcica shape and total STB (p < 0.016). Nperp–Pg distance differed significantly among the groups (p < 0.016). There were no significant differences in the cephalometric parameters between the partial and total STB groups (p > 0.05).
Discussion
When STB is considered in terms of etiology, the bridge forms in cartilage during early developmental stages, and subsequently undergoes ossification during early childhood. The ossification may change depending on the complex embryology of the sphenoid bone. According to this theory, STB can be considered a developmental anomaly. In addition, because the anterior wall of the sella turcica is predominantly composed of neural crest cells during the early embryological period, it is considered that structural deviations in the anterior wall arise through certain deviations in the facial skeleton [10].
There are several possible reasons for STB observation. The most important is apparent fusion between the anterior and posterior structures observed on lateral cephalometric radiographs by superposition of the structures, although there is no real bone fusion between these structures. The second is that STB is a malformation arising during the prenatal period. The whole cranial base is formed from a cartilage structure around the fifth fetal week. Platzer [13] reported that there was a connection between the cartilage primordium and STB. Lang and Tisch-Rottensteiner [14] reported that STB was even observed in a newborn.
Müller [15] conducted a study on 1040 radiographs to determine the relationships between STB and ophthalmic symptoms and found direct bone STB at a rate of 3.85% and pseudo-bridging at a rate of 3.2%. However, the author did not report any relationships between existence of STB and ophthalmologic symptoms. In another study, the sella turcica area was examined by direct inspection, and the STB incidence was between 1.75 and 6% [2]. Although the prevalence of STB varied between 1.1 and 13% in the general population [7], the incidence was increased in individuals with severe craniofacial anomaly [8]. In our study, the incidence of partial STB was 5.52%, while the incidence of total STB was 3.05%.
Recent studies have examined the associations among STB, craniofacial structures, and genetic and developmental syndromes that affect systemic disorders. Earlier studies showed that many dental anomalies like tooth transposition, hypodontia, and mandibular second premolar agenesis were associated with interclinoid calcification. Ali et al. [16] found that the incidence of STB was increased in patients with palatally impacted canine teeth, and that the incidence of partial and total STB was 54.8% and 25.8%, respectively. However, Leonardi et al. [9] found the incidence of total STB was 17.6% in adolescents with dental anomalies, compared with 9.9% in control subjects. Similarly, Scribante et al. [7] described that STB was frequently found in patients with dental anomalies. They reported that the prevalences of partial and total STB were 56% and 13%, respectively, in patients with palatally impacted canines. They further reported that the prevalences of partial and total STB were 57% and 9%, respectively, in patients with upper lateral incisor agenesis.
The occurrence of STB in very early periods of life can alert clinicians to the possible development of dental anomalies and craniofacial deviations in later periods of life because these phenomena are associated with one another. Changes in sella turcica size are frequently associated with pathology and syndromes. While the majority of these conditions are not associated with life-threatening situations, some may cause pituitary apoplexies (necrosis and hemorrhage) that require urgent treatment [3].
The type of skeletal malocclusion appears to play an important role in the prevalence of STB. Abdel-Kader [17] reported that higher percentages of STB were found in subjects with skeletal class III than in subjects with skeletal class II and bimaxillary protrusion orthognathic surgery. Moreover, Meyer-Marcotty et al. [18] concluded that skeletal class III patients presented a significantly higher STB rate of 16.8% compared with the rate of 9.4% in skeletal class I patients. Patients with surgically repaired unilateral cleft lip and palate also had a higher incidence of STB [19]. We found significant differences for Nperp–A distance, Nperp–Pg distance, and palatal plane-to-anterior cranial base angle measurements among the groups. We consider that STB can affect the development of the maxilla, mandible, and other craniofacial structures, because the sella turcica and craniofacial region originate from neural crest cells.
In conclusion, the degree of calcification of the sella turcica in orthodontic adolescent subjects can provide information about the cephalometric parameters of these subjects. This study is the first to compare the degree of calcification of the sella turcica in adolescent and young adult subjects with respect to their cephalometric parameters. The maxilla and mandible were located in a sagittal retrusive position in partial and total STB subjects compared with normal shape sella turcica subjects.
References
Jones R, Faqir A, Millett D, Moos K, McHugh S. Bridging and dimensions of sella turcica in subjects treated by surgical-orthodontic means or orthodontics only. Angle Orthod. 2005;75:714–8.
Perez IE, Chavez KA, Ponce D. Frequency of sella turcica bridge and clinoid enlargement in lateral cephalometric plain film radiography from Peruvians. Int J Morphol. 2013;31:373–7.
Tekiner H, Acer N, Kelestimur F. Sella turcica: an anatomical, endocrinological, and historical perspective. Pituitary. 2015;18:575–8.
Sathyanarayana HP, Kailasam V, Chitharanjan AB. Sella turcica—its importance in orthodontics and craniofacial morphology. Dent Res J. 2013;10:571–5.
Melsen B. The cranial base: the postnatal development of the cranial base studied histologically on human autopsy material. Acta Odontol Scand. 1974;32:9–126.
Cederberg RA, Benson B, Nunn M, English J. Calcification of the interclinoid and petroclinoid ligaments of sella turcica: a radiographic study of the prevalence. Orthod Craniofac Res. 2003;6:227–32.
Scribante A, Sfondrini MF, Cassani M, Fraticelli D, Beccari S, Gandini P. Sella turcica bridging and dental anomalies: is there an association? Int J Paediatr Dent. 2017;27:568–73.
Becktor JP, Einersen S, Kjær I. A sella turcica bridge in subjects with severe craniofacial deviations. Eur J Orthod. 2000;22:69–74.
Korayem M, AlKofide E. Size and shape of the sella turcica in subjects with Down syndrome. Orthod Craniofac Res. 2015;18:43–50.
Kjaer I. Orthodontics and foetal pathology: a personal view on craniofacial patterning. Eur J Orthod. 2010;32:140–7.
Erbay EF, Caniklioğlu CM, Erbay ŞK. Soft tissue profile in Anatolian Turkish adults: part I. Evaluation of horizontal lip position using different soft tissue analyses. Am J Orthod Dentofac Orthop. 2002;121:57–64.
Leonardi R, Barbato E, Vichi M, Caltabiano M. A sella turcica bridge in subjects with dental anomalies. Eur J Orthod. 2006;28:580–5.
Platzer W. Anatomy of taenia interclinoidea and its relation to the internal carotid artery. Fortschr Geb Röntgenstr Nuklearmed. 1957;87:613–6 (in German).
Lang J, Tisch-Rottensteiner K. Form and form variations of the sella turcica. Verh Anat Ges. 1977;71(Pt 2):1279–82 (in German).
Müller F. Die Bedeutung der Sellabruecke für das Auge. Klin Monatsbl Augenheilkd. 1952;120:298–302 (in German).
Ali B, Shaikh A, Fida M. Association between sella turcica bridging and palatal canine impaction. Am J Orthod Dentofac Orthop. 2014;146:437–41.
Abdel-Kader HM. Sella turcica bridges in orthodontic and orthognathic surgery patients. A retrospective cephalometric study. Aust Orthod J. 2007;23:30–5.
Meyer-Marcotty P, Reuther T, Stellzig-Eisenhauer A. Bridging of the sella turcica in skeletal class III subjects. Eur J Orthod. 2010;32:148–53.
Sundareswaran S, Nipun CA. Bridging the gap: sella turcica in unilateral cleft lip and palate patients. Cleft Palate Craniofac J. 2015;52:597–604.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Suleyman Kutalmış Buyuk, Ahmet Karaman, and Yasin Yasa declare that they have no conflict of interest.
Human rights statement
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions. The study was designed as a retrospective archival study.
Animal rights statement
This study does not contain any studies with animal subjects performed by any of the authors.
Rights and permissions
About this article

Cite this article
Buyuk, S.K., Karaman, A. & Yasa, Y. Relationship between sella turcica bridging and cephalometric parameters in adolescents and young adults. Oral Radiol 35, 245–250 (2019). https://doi.org/10.1007/s11282-018-0349-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11282-018-0349-5