
Abstract
In this study, we investigated drug resistance levels in human immunodeficiency virus (HIV)-1-infected patients in Suzhou by retrospectively analyzing this property and the characteristics of circulating HIV-1 strains collected from 2009 to 2014. A total of 261 HIV-1-positive plasma samples, confirmed by the Suzhou CDC, were collected and evaluated to detect HIV-1 drug resistance genotypes using an in-house method. The pol gene fragment was amplified, and its nucleic acid sequence was determined by Sanger sequencing. Drug resistance mutations were then analyzed using the Stanford University HIV resistance database (https://hivdb.stanford.edu). A total of 216 pol gene fragments were amplified and sequenced with 16.7% (36/216) of sequences revealing these mutations. The drug resistance rates of protease, nucleoside reverse transcriptase, and non-nucleoside reverse transcriptase inhibitors (NNRTIs) were 4/36 (11.1%), 2/36 (5.6%), and 30/36 (83.3%), respectively. Five surveillance drug resistance mutations were found in 36 sequences, of which, three were found among specimens of men who have sex with men. Potential low-level resistance accounted for 33% of amino acid mutations associated with NNRTIs. Two of the mutations, M230L and L100I, which confer a high level of resistance efavirenz (EFV) and nevirapine (NVP) used as NNRTIs for first-line antiretroviral therapy (ART), were detected in this study. Therefore, when HIV-1 patients in Suzhou are administered fist-line ART, much attention should be paid to the status of these mutations that cause resistance to EVP, EFV, and NVP.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Antiretroviral therapy (ART) is among the most effective methods for treating acquired immune deficiency syndrome (AIDS), which is caused by human immune deficiency virus (HIV) infection [1]. The implementation of ART can not only inhibit viral replication and reconstitute immune function in HIV-infected persons, but also significantly improves their quality of life and effectively reduces the morbidity and mortality of HIV-related diseases [2, 3]. Six categories of antiretroviral drugs have been approved by the Food and Drug Administration in the USA, including protease inhibitors (PIs), nucleoside RT inhibitors (NRTIs), non-nucleoside RT inhibitors (NNRTIs), integrase strand transfer inhibitors, fusion Inhibitors, and HIV co-receptor antagonists [4]. The first-line treatment program freely offered in China is a combination of two types of NRTIs with one NNRTI. Compared to the first-line treatment program, the recommended second-line ART program replaces NNRTIs with PIs in addition to two NRTIs [5, 6]. However, because of the intrinsic high variation of HIV and the influence of drug selection pressure, the emergence of HIV drug-resistant strains is the main limitation to effective ART treatment [7]. In a retrospective study of the molecular epidemiology of HIV-1 in Suzhou from 2009 to 2014, we previously showed that multiple HIV-1 subtypes are circulating mainly via sexual transmission, represented by CRF01_AE as the dominant strain [8]. Since the beginning of 2005, a free ART program for patients with AIDS has been conducted in Suzhou [9]. To investigate the drug resistance level of HIV-1 in infected individuals in Suzhou, it is necessary to analyze the drug resistance characteristics of circulating HIV-1 strains and understand the impact of drug resistance mutations on HIV-1 ART. Therefore, our HIV drug resistance study might be helpful to formulate a reasonable and effective ART scheme to minimize the epidemic of HIV-1 drug-resistant strains.
Materials and methods
Patients
A retrospective study was conducted according to the principle of informed consent. Blood samples and epidemiological data were collected by trained investigators according to a unified questionnaire. Based on this, 261 HIV-1 antibody-positive plasma samples were obtained from hospital patients, men who have sex with men (MSM), blood donors, and detainees, collected by the Suzhou Center for Disease Control from 2009 to 2014. Each sample had a unique identification number. Blood samples used in the study were first screened by enzyme linked immunosorbent assay (ELISA) and then confirmed by western blotting.
Blood sample collection, transportation, and storage
Venous blood (8 ml) was collected in vacuum tubes with EDTA-K3 clotting. The blood and anticoagulant were mixed immediately to prevent agglutination. Samples were stored and transported at room temperature, and were centrifuged for 15 min at 1500–3000 rpm/min to separate plasma within 6 h of collection. The plasma aliquot was stored in sterile, RNA-free, and polypropylene screw tubes marked with the sample number and separation time. The plasma was temporarily stored at 4 °C for 4 days and was kept below − 80 °C for long-term storage.
Drug resistance genotypic assay
We analyzed plasma samples by an in-house method for HIV-1 drug resistance genotypic assays. Viral RNA was extracted from 140-μl plasma samples using the Qiagen QIAamp Viral RNA Mini kit. cDNA was synthesized by RT-PCR using the Takara One Step RNA PCR kit. The pol gene fragment (HXB2, 2147–3462nt) was amplified by nested PCR. The primers MAW26 (5′-TTGGAAATGTGGAAAGGAAGGAC-3′) and RT21 (5′-CTGTATTTCTGCTATTAAGTCTTTTGATGGG-3′) were used for the first round of PCR, and the primers Pro-1 (5′-CAGAGCCAACAGCCCCACCA-3′) and RT20 (5′-CGCCAGTTCTAGCTCTGCTTC-3′) were used for the second round PCR. The 1316-bp PCR fragment was then purified using a Qiagen gel extraction kit and sequenced with an automated ABI 377 DNA Sequencer (Applied Biosystems) as previously described [8]. The quality of sequences obtained by Sanger sequencing was preliminarily evaluated and the splicing of these sequences was analyzed with the ContigExpress module in Vector NTI 6.0 software [10]. BioEdit 7.0 (https://www.mbio.ncsu.edu/BioEdit/ bioedit.html) software was used for nucleic acid sequence comparisons, editing, adjustment, and analysis. The HIV-1 drug resistance mutation level was divided into five types according to the following criteria: sensitive susceptible (S, 0–9 points), potential low-level resistance (P, 10—14 points), low-level resistance (L, 15–29 points), intermediate resistance (I, 30–59 points), and high-level resistance (H, > 60 points) (https://hivdb.stanford.edu/page/release-notes#resistance.summary). The edited sequences were pasted into the HIV resistance database of Stanford University (HIVDB, https://hivdb.stanford.edu) to determine the site and type of the drug resistance mutations, and the drug resistance scores were automatically assigned by the HIVdb Program in the database. In this study, we mainly analyzed the resistance mutation sites related to PIs [ATV (atazanavir), DRV (darunavir), LPV (lopinavir), r (ritonavir)], NRTIs [abacavir, AZT (zidovudine), emtricitabine, 3TC (lamivudine), TDF (tenofovir)], and NNRTIs [DOR (doravirine), EFV (efavirenz), ETR (etravirine), NVP (nevirapine), RPV (rilpivirine)], as shown in supplementary Table 1.
HIV-1 subtype analysis
The subtype analysis in the study was based on the pol-gene sequences. HIV-1 subtypes were analyzed using HIV BLAST online from the Los Alamos HIV Database (https://www.hiv.lanl.gov/content/sequence /BASIC_BLAST) combined with results from the phylogenetic analysis with the comparison of reference subtypes.
Results
Epidemiological analysis of HIV-1 drug resistance sites
A total of 216 pol gene fragments were amplified and sequenced from 261 HIV-1-positive plasma samples collected in Suzhou from 2009 to 2014. The drug resistance sites for protease, nucleoside, and non-nucleoside inhibitors were analyzed using the HIVDB program in Stanford University’s HIV resistance database (supplementary Table 1). We analyzed the correlation between drug resistance sites and ethnicity, age, sex, sample source, and HIV-1 subtype, as shown in Table 1. Most drug resistance mutation sequences were found in samples of 20 hospital patients, followed by 12 from the MSM group.] The frequency of drug resistance in the Han ethnicity was 16.8% (32/190), whereas it was 15.4% (4/26) in minorities. HIV-infected persons aged ≥ 30 years were associated with a frequency of drug resistance mutations of 19.5% (22/113). The frequency of drug resistance mutations in females (25.6%, 10/39) was higher than that in males (14.7%, 26/177). Drug resistance mutations occurred in the HIV-1 subtypes CRF07/08_BC, CRF01_AE, and subtype B, with subtype B showing the highest frequency 52.6% (10/19).
Overview of HIV-1 drug resistance mutations in Suzhou
Among the 216 sequences, 36 (16.7%) contained drug resistance mutations. Further, 4/36 (11.1%) sequences were related to PI resistance mutations and 2/36 (5.6%) sequences were related to NRTI resistance mutations; 30/36 (83.3%) sequences were related to NNRTI resistance mutations. Two sequences associated with PI or NNRTI resistance mutations contained two different resistance mutation sites each. A total of 40 mutations comprising 16 mutation sites were identified in these 36 sequences (Table 2). The drug mutations were analyzed, and the resistance level score was automatically assigned according to specific drug inhibitors by the HIVDB program (Table 2). Susceptible and potential low-level resistance comprised the major types of drug resistance mutations, with a frequency of 70.6% (48/68) corresponding to a total of 68 inhibitor-related sites, particularly corresponding to PI- and NRTI-related mutations.
A standard list of surveillance drug resistance mutations (SDRMs) is used to characterize the epidemiology of transmitted drug resistance [11, 12]. Five SDRMs were found in the identified 16 mutation sites, among which M46L and V82S were related to PIs in the MSM population infected by HIV-1 CRF01_AE, whereas L100I, P225H, and M230L were related to NNRTIs found in hospital patients (L100I and P225H) or the MSM population (M230L) infected by CRF07/08_BC. However, SDRMs in NRTIs were not detected.
Analysis of PI-, NRTI-, and NNRTI-related drug resistance levels
There were six mutation sites related to PIs. The degree of resistance of each site to the three PIs is shown in Table 2. M46L and V82S, which are SDRMs, were the major resistance mutations (M). M46L was a potential low-level resistance mutation for ATV/r and LPV/r, whereas V82S exhibited intermediate resistance to ATV/r and LPV/r. The three drug resistance mutations, M46V, I50M, and T74P, were accessory resistance mutations (A). The mutation G73R, which has not been well-studied, was also identified in a CRF01_AE-infected hospital patient.
The resistance degree analysis with respect to the three PIs is shown in Fig. 1a. It is shown that susceptible mutations summed up to 61.1% (11/18) of total analyzed mutation sites in the three PIs, whereas potential low-level resistance and intermediate resistance rates were 22.2% (4/18) and 11.1% (2/18), respectively (Fig. 1a). No low- or high-level resistance was detected. All mutations detected in PIs conferred sensitivity to DRV/r, whereas V82S resulted in intermediate resistance to ATV/r and LPV/r. Only two mutations, A62V and T215I, were found to be related to NRTI-related drug resistance, and their levels were all indicative of sensitivity to the five listed NRTIs, suggesting that the resistance level of NRTI-related drug mutations was very low in Suzhou (Table 2).

Pie chart analysis of the occurrence of protease inhibitor (PI)-related drug resistance levels (a) and non-nucleoside reverse transcriptase inhibitor (NNRTI)-related drug resistance levels (b) in HIV-1 from infected individuals from 2009 to2014 in Suzhou, China. The rate was determined as follows (from Table 2): the number of mutation sites in each type of resistance level/total number of analyzed PI or NNRTI resistance mutation sites
Eight drug resistance mutation sites were determined to be associated with NNRTIs, of which, L100I, P225H, and M230L were SDRMs. Among the three SDRMs, M230L showed high resistance to the listed NNRTIs, followed by L100I and P225H for the five NNRTIs. The other five drug resistance mutations did not affect the activity of all five NNRTIs. We further analyzed the occurrence of different drug resistance levels associated with NNRTI-related mutations (Fig. 1b). The results revealed that potential low-level resistance was the most frequent resistance level, accounting for 32.5% (13/40) of analyzed drug resistance mutations, followed by sensitivity (27.5%; 11/40), intermediate resistance (15.0%; 6/40), high-level resistance (15.0%; 6/40), and low-level resistance (10.0%; 4/40).
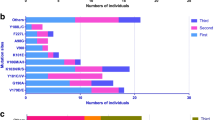
The number of NNRTI-related mutations was 32 among 30 sequences, including two sequences containing two different mutation sites each. An analysis of drug resistance levels for each NNRTI showed that the levels of DOR-related mutations were mostly susceptible (46.8%; 15/32) and low-level resistance (40.6%; 13/32). For EFV, the mutation levels were mostly susceptible (43.8%; 14/32) and potential low-level resistance (46.8%; 15/32). Analysis of the resistance level of the mutations related to the remaining three NNRTIs, ETR, NVP, and RPV, showed that they were mostly potential low-level resistance (Fig. 2).

The percentage of each non-nucleoside reverse transcriptase inhibitor (NNRTI)-related resistance level for DOR (doravirine), EFV (efavirenz), ETR (etravirine), NVP (nevirapine), and RPV (rilpivirine)
Discussion
Suzhou is an early HIV epidemic area in China Jiangsu Province with a complex epidemic situation [8]. The free anti-HIV treatment for AIDS was launched in early 2005 [9]. Studies have shown that in an untreated HIV-1-infected individual, 104–105 single-point mutations can occur every day, and double-point mutations often occur [13, 14]. Under the combined effects of high variations in the HIV genome and drug selection pressure, HIV drug resistance gene mutations develop, leading to a drug-resistant strain [7]. The effect of drug resistance gene mutation sites on antiviral drugs used for treatment in Suzhou remains unclear. In this study, to identify the mutations in drug resistance genes in circulating HIV-1 strains, we retrospectively analyzed 216 pol gene fragment sequences from 261 positive samples in Suzhou collected from 2009 to 2014.
We analyzed the drug resistance level of HIV circulating strains in Suzhou with respect to three PIs, five NRTIs, and five NNRTIs. Among the three types of antiretroviral drugs, drug resistance mutations were associated with the highest susceptibility to NRTIs, followed by PIs, whereas NNRTI resistance was not higher than 6%. Five SDRMs were detected in our study. M46L and V82S are related to PIs. Studies have shown that M46L can reduce virological responses [15] and cause the protease inhibitor nelfinavir to become ineffective [16]. Three other SDRMs, L100I, P225H, and M230L, are related to NNRTIs, among which L100I and P225H often appear in conjunction with K103N through synergy, thus reducing the sensitivity to NVP and EFV [17]. M230L often occurs alone and reduces the sensitivity to all NNRTIs [18]. An analysis of the population distribution of SDRMs revealed three of the five SDRMs in the MSM population. Therefore, to effectively control the spread of drug-resistant strains, the MSM population should be given more attention in Suzhou. Further analysis of the subtype distribution of SDRMs revealed that SDRMs were subtype-specific and that PI-related SDRMs were distributed in the CRF01_AE strain, with NNRTI-related SDRMs distributed in the CRF07/08_BC strain. Notably, the resistance level of L100I and M230L was relatively high, corresponding to each inhibitor of NNRTIs, indicating that first-line antiviral treatment should be replaced with second-line antiviral treatment once patients with HIV show the L100I and M230L mutations, which are associated with highly resistance to most currently used NNRTIs.
Epidemiological analysis of drug resistance sites revealed that the frequency of drug resistance in the MSM population was high (20.7%, 12/58), confirming the view that the MSM population should be closely monitored for drug resistance. We previously found an eight-member cluster in the MSM population [8], but no drug-resistant strains were found in that cluster, indicating that the drug-resistant strains remain scattered in the MSM population and that no cross-transmission of drug resistance mutations occurs in that cluster. A dynamic follow-up survey of the MSM population should be conducted to clarify the transmission characteristics of HIV-resistant strains.
Similar to the SDRMs mentioned previously herein, the drug resistance rate was also subtype-specific. The CRF01_AE subtype showed a high drug resistance rate. Differences in the pol gene among different subtypes results in differences in the amino acid sequence of the strain, showing polymorphisms in the amino acid locus [19]. This polymorphism is the main origin of the drug resistance genetic barrier [20]. Therefore, exploring the subtype specificity of the genetic barrier with respect to ART treatment is important to formulate targeted treatment, prevention, and control programs. We also found that the frequency of drug resistance in women (25.6%; 10/39) was higher than that in men (14.7%; 26/177), which is consistent with previous findings [21].
Currently, the standard first-line ART for HIV-infected adults and adolescents in China is either TDF or AZT and 3TC and either EFV or NVP. If there is no contraindication, TDF or EFV is preferred. Only the first-line drug replacement standard that meets the failure of treatment can be replaced with the second-line treatment plan. Based on our results, we found that HIV drug resistance mutations in Suzhou were still associated with susceptibility to 3TC and TDF among the five NRTIs. However, the M230L and L100I mutations in our study are linked to high resistance to EFV and NVP, and the intermediate and high-level resistance mutations accounted for 22.5% (9/40) of NNRTI-related mutations in our analysis. Above all, results indicated that the first-line ART therapy might still be a suitable regimen in the Suzhou area; however, when treating patients with HIV in Suzhou using first-line ART, attention should be paid to determine if their HIV strains carry the NNRTI-related drug mutations. Recently, Zuo et al. systematically reviewed the trend in HIV-1 drug resistance in China from 2001 to 2017 by meta-analysis [22], and they found that a few NRTI-associated (M184V/I) and NNRTI-associated (K103N/S, Y181C/I and G190A/S) SDRMs were responsible for most cases of drug resistance. These data suggest that the current available first-line ART regimens containing 3TC and/or EFV or NVP should be urgently amended or promptly switched to the second-line regimens. However, these SDRMs Zuo et al. found didn’t appear in our analysis.
In summary, we retrospectively analyzed HIV-1 drug resistance mutations in 216 patients infected with HIV in Suzhou using samples collected from 2009 to 2014. The drug resistance level of the detected mutations was still low or associated with susceptibility to PIs and NRTIs, but not to NNRTIs supplied in the free HIV ART program. Thus, before applying the first-line ART currently used in Suzhou, we should consider the specific situation of the patients and whether their HIV strain is resistant to NNRTIs, in addition to making appropriate personal treatment plans including second-line ART.
References
Yoshimura K (2017) Current status of HIV/AIDS in the ART era. J Infect Chemother 23:12–16
Group ISS, Lundgren JD, Babiker AG, Gordin F, Emery S, et al. (2015) Initiation of antiretroviral therapy in early asymptomatic HIV infection. N Engl J Med 373: 795–807.
Lifson AR, Grund B, Gardner EM, Kaplan R, Denning E et al (2017) Improved quality of life with immediate versus deferred initiation of antiretroviral therapy in early asymptomatic HIV infection. AIDS 31:953–963
Gunthard HF, Aberg JA, Eron JJ, Hoy JF, Telenti A et al (2014) Antiretroviral treatment of adult HIV infection: 2014 recommendations of the international antiviral society-USA panel. JAMA 312:410–425
Zhang F, Dou Z, Ma Y, Zhang Y, Zhao Y et al (2011) Effect of earlier initiation of antiretroviral treatment and increased treatment coverage on HIV-related mortality in China: a national observational cohort study. Lancet Infect Dis 11:516–524
Sun J, Liu L, Shen J, Qi T, Wang Z et al (2015) Reasons and risk factors for the initial regimen modification in Chinese treatment-Naive patients with HIV Infection: a retrospective cohort analysis. PLoS ONE 10:e0133242
Hertogs K, Bloor S, Kemp SD, Van den Eynde C, Alcorn TM et al (2000) Phenotypic and genotypic analysis of clinical HIV-1 isolates reveals extensive protease inhibitor cross-resistance: a survey of over 6000 samples. AIDS 14:1203–1210
Yuan Y, Tang S, Li Y, Yan D, Peng Q et al (2018) Characteristics of HIV-1 molecular epidemiology in Suzhou, China, from 2009 to 2014. Virol Sin 33:209–212
Zhang FJ, Pan J, Yu L, Wen Y, Zhao Y (2005) Current progress of China's free ART program. Cell Res 15:877–882
Lu G, Moriyama EN (2004) Vector NTI, a balanced all-in-one sequence analysis suite. Brief Bioinform 5:378–388
Shafer RW, Rhee SY, Pillay D, Miller V, Sandstrom P et al (2007) HIV-1 protease and reverse transcriptase mutations for drug resistance surveillance. AIDS 21:215–223
Clutter DS, Jordan MR, Bertagnolio S, Shafer RW (2016) HIV-1 drug resistance and resistance testing. Infect Genet Evol 46:292–307
Preston BD, Poiesz BJ, Loeb LA (1988) Fidelity of HIV-1 reverse transcriptase. Science 242:1168–1171
Coffin JM (1995) HIV population dynamics in vivo: implications for genetic variation, pathogenesis, and therapy. Science 267:483–489
Moura ME, da Guarda Reis MN, Lima YA, Eulalio KD, Cardoso LP et al (2015) HIV-1 transmitted drug resistance and genetic diversity among patients from Piaui State, Northeast Brazil. J Med Virol 87:798–806
Rhee SY, Liu TF, Holmes SP, Shafer RW (2007) HIV-1 subtype B protease and reverse transcriptase amino acid covariation. PLoS Comput Biol 3:e87
Basson AE, Rhee SY, Parry CM, El-Khatib Z, Charalambous S et al (2015) Impact of drug resistance-associated amino acid changes in HIV-1 subtype C on susceptibility to newer nonnucleoside reverse transcriptase inhibitors. Antimicrob Agents Chemother 59:960–971
Xu HT, Quan Y, Schader SM, Oliveira M, Bar-Magen T et al (2010) The M230L nonnucleoside reverse transcriptase inhibitor resistance mutation in HIV-1 reverse transcriptase impairs enzymatic function and viral replicative capacity. Antimicrob Agents Chemother 54:2401–2408
Nomaguchi M, Miyake A, Doi N, Fujiwara S, Miyazaki Y, et al. (2014) Natural single-nucleotide polymorphisms in the 3' region of the HIV-1 pol gene modulate viral replication ability. J Virol 88: 4145–4160.
Giannini A, Vicenti I, Materazzi A, Boccuto A, Dragoni F et al (2019) The HIV-1 reverse transcriptase E138A natural polymorphism decreases the genetic barrier to resistance to etravirine in vitro. J Antimicrob Chemother 74:607–613
WHO (2017) HIVDR Report; https://www.who.int/hiv/pub/ drugresistance/hivdr-report-2017 /en/
Zuo L, Liu K, Liu H, Hu Y, Zhang Z et al (2020) Trend of HIV-1 drug resistance in China: a systematic review and meta-analysis of data accumulated over 17 years (2001–2017). E Clin Med 18:100238
Acknowledgements
We gratefully acknowledge the contribution of the HIV-1 patients who participated in this study and also wish to thank the staff of the local CDC for recruiting participants, collecting samples, and technical assistance.
Funding
This work was supported by The National Natural Science Foundation of China (81802083, 31870867), State Key Laboratory of Veterinary Biotechnology Foundation (SKLVBF201916), Open Research Fund Program of the State Key Laboratory of Virology of China (2020IOV003), the Jiangsu Province Medical Innovation Team (CXTDB2017009), the Jiangsu Province's Key Discipline of Prenatal Diagnosis (FXK201746), and Jiangsu Provincial Key Research and Development Program (BE2019656).
Author information
Authors and Affiliations
Contributions
RL and XY collected the samples. YS and JHu designed the study, YS, JH, JH, YY, and YL performed the experiments. YS analyzed the data. YS and CD wrote the manuscript.
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare that they have no conflicts of interest regarding this work.
Ethical approval
This study has been approved by the Ethics Committee of the First Affiliated Hospital of Soochow University.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Sequence data
The 216 pol sequences analyzed in the study have been submitted to GenBank with the accession number MN601502-601717.
Additional information
Edited by Wolfram H. Gerlich.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Song, Y., Hu, J., He, J. et al. Retrospective analysis of HIV-1 drug resistance mutations in Suzhou, China from 2009 to 2014. Virus Genes 56, 557–563 (2020). https://doi.org/10.1007/s11262-020-01774-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11262-020-01774-0