
Abstract
Purpose
Cyclosporine (CsA) is often prescribed to patients with glucocorticoid (GC)-dependent nephrotic syndrome. Although it is well known that long-term administration of GC causes osteoporosis, the effects of CsA on bone metabolism are not fully established. Therefore, we examined the effects of CsA on bone metabolism in patients with GC-dependent nephrotic syndrome in remission.
Methods
We followed 23 patients treated with prednisolone alone (GC alone group) and 17 patients treated with CsA in combination with prednisolone (GC + CsA group). Bone mineral density (BMD) was measured by dual-energy X-ray absorptiometry, and biochemical markers of bone metabolism were simultaneously measured in serum and urine samples.
Results
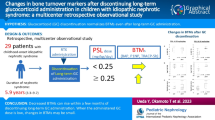
BMD decreased significantly in the GC group from 752 to 623 mg/cm2 but non-significantly in the GC + CsA group from 751 to 684 mg/cm2. Although the cumulative dose of GC increased in both groups, there were no significant differences in biochemical markers at either the start or the end of the study. Vertebrate bone fracture and other side effects associated with CsA treatment did not occur in our study.
Conclusions
Our results indicate that CsA does not accelerate GC-induced osteoporosis in patients with nephrotic syndrome. We conclude that CsA is appropriate for the treatment of GC-dependent nephrotic syndrome, because it does not adversely affect bone metabolism and has favorable glomerular effects.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Nephrotic syndrome (NS), defined as proteinuria >3.5 g/day, is caused by several glomerular diseases and is characterized by edema, hypoproteinemia, and hyperlipidemia. Generally, NS is treated with glucocorticoids (GC), which continues until the resolution of proteinuria. Once complete remission has been achieved, the GC dose may be tapered. However, inadequate tapering of GC may lead to relapse, known as GC-dependent NS. Patients who do not respond to GC therapy are classified as having GC-resistant NS.
Immunosuppressive agents, such as cyclosporine A (CsA), are often used to treat GC-resistant or GC-dependent NS [1, 2]. However, it was reported that high doses of CsA can induce osteoporosis after organ transplantation [3, 4]. Long-term use of GC can also cause osteoporosis because of unbalanced or a higher rate of bone remodeling [5, 6]. Administration of CsA at doses similar to those used after organ transplantation accelerate bone turnover, increase bone absorption, and cause inadequate bone remodeling in oophorectomized rats [7]. However, this phenomenon was not observed in patients treated with CsA, and the results of some studies are controversial [8, 9]. In organ transplantation, CsA is often administered concomitantly as part of a multi-drug regimen. This makes it difficult to assess the contribution of each drug to bone loss. Therefore, in this study, we investigated the role of CsA in bone metabolism in patients with NS in remission.
Materials and methods
Patients
Forty patients with GC-dependent NS in prednisolone-induced remission, a representative form of GC, for >12 months were enrolled in this study (mean duration of remission, 62 ± 107 months). With the goal of reducing the existing dose of prednisolone, we offered all patients an additional prescription of CsA. Of the 40 patients, 17 agreed with our proposal and comprised the GC + CsA group. The other 23 did not accept CsA, but did continuous prednisolone therapy (GC group). The clinical characteristics of the two groups are shown in Table 1. All of the patients were <50 years of age, and all females were before menopause. Characteristics of NS, duration remission, relapse frequency, and daily prednisolone doses were not uniform among the two groups (Table 1). However, all of the patients required long-term treatment with GC, increasing the risk of osteoporosis. There were no significant differences in the cumulative dose of prednisolone or bone mineral density (BMD) at the second to fourth lumbar spine (L2–L4) between the two groups at the start of the study. All of the patients were prescribed with 1.0 μg of 1,25-(OH)2-D3, an active vitamin D3 analog, from the start of GC treatment. They were not using any concomitant drugs, including supplemental calcium, estrogen-like agents, fluoride salts, or bisphosphonates. Patients with a history of vertebrate bone fracture were excluded from this study, because of inaccurate measurement of BMD in these patients. Our hospital’s ethics committee approved the study, and all 40 patients gave informed consent to participate.
Study design
The BMD of the lumbar spine was measured by lateral projection in all patients at the start of the study. We administered CsA at doses in accordance with C2 values, which were between 600 and 800 ng/ml. Because orally administered doses are not accurately reflected by their serum concentrations, the dose of CsA was not identical in the patients in the GC + CsA group. All 17 patients in the GC group continued their previous doses of GC, which were not uniform among the group, throughout the study. Twelve months later, BMD and biochemical markers of bone metabolism were measured in all patients. The cumulative dose of GC was determined and compared between the start and end of the study.
Measurement of BMD
The mean BMD and the % of young adult mean BMD (%YAM) at L2–L4 were measured by dual-energy X-ray absorptiometry using a DQR 4500A (HOLOGIC, Waltham, MA) [10]. The %YAM of BMD is more widely used than the actual BMD value in clinical settings and is useful to compare data between individual patients with scattered values. We mainly used the %YAM value in statistical analysis.
Measurement of biochemical markers for bone metabolism
Serum osteocalcin (OC) was measured using a radioimmunoassay [11] to evaluate osteogenesis. Urinary deoxypyridinoline (Dpd) was measured using an enzyme immunoassay [12] to evaluate bone resorption. Data were adjusted for urinary creatinine concentrations to account for possible aberrations caused by changes in urine volume. All assays were conducted by a contracted laboratory (SRL Inc., Tokyo, Japan). The intra-assay and inter-assay coefficients of variability were reported to be <10 %. Serum calcium and phosphorus concentrations were measured at our hospital’s central laboratory by the ortho-cresolphthalein complexone method and by direct measurement of molybdic acid concentrations, respectively.
Statistical analysis
Continuous variables are presented as mean ± standard error (SE) and were compared using the Mann–Whitney U test. Correlations between BMD %YAM and cumulative dose of GC at the start and end of the study were analyzed separately in both groups, plotted on the same graph, and individual regression equations were produced. Correlations between pairs of variables were estimated by Spearman’s rank correlation test. Two-sided P values were calculated, and P values <0.05 were considered statistically significant. Statistical analyses were performed using StatView software version 5.0 (SAS Institute Japan, Tokyo, Japan).
Results
None of the patients enrolled in this study experienced radiologically new bone fracture during the follow-up period. Changes in mean BMD at L2–L4 from the start to the end of the values were determined in both groups of patients. Mean BMD at L2–L4 decreased to 82.5 % during the study in the GC group and to 90.7 % in the GC + CsA group (Table 1). The %YAM decreased significantly from 87 ± 9 to 69 ± 21 % (P < 0.001) during the study in the GC group and non-significantly from 85 ± 9 to 79 ± 5 % (P = 0.065) in the GC + CsA group (Fig. 1). The cumulative dose of GC increased from 516 ± 281 to 609 ± 375 mg/kg in the GC group and from 504 ± 258 to 601 ± 306 mg/kg in the GC + CsA group (Table 1). The correlations between BMD and cumulative dose of GC (i.e., prednisolone) were determined in both groups. The rate of change in BMD was correlated with the cumulative dose of GC and could be expressed using the equations y = −1.387x + 1,468 (P < 0.05) in the GC group and as y = −0.691x + 1,099 (P < 0.05) in the GC + CsA group. The decrease in slope in the GC + CsA group was shallower than that in the GC group despite the continuous administration of prednisolone in both groups (Fig. 2). The serum OC concentrations at the start and end of the study were 5.8 ± 4.1 and 5.7 ± 2.8 ng/ml in the GC group, and 5.3 ± 3.9 and 5.1 ± 3.6 ng/ml in the GC + CsA group; the changes in both groups were not statistically significant. The urinary Dpd concentrations at the start and end of the study were 5.8 ± 4.1 nmol/mmol-Cr and 5.7 ± 2.8 nmol/mmol-Cr in the GC group, and 5.3 ± 3.9 nmol/mmol-Cr and 5.1 ± 3.6 nmol/mmol-Cr in the GC + CsA group, which were not significantly different. Even though the cumulative dose of GC increased in both groups, there were no significant changes in the biochemical markers between the start and end of the study (Table 1). Vertebrate bone fracture and other side effects associated with CsA did not occur in any patient. These results indicate that treatment with CsA for 1 year does not accelerate GC-induced osteoporosis or interfere with bone mineralization in patients with nephrotic syndrome at <50 years of age before menopause.

Changes in mean bone mineral density (BMD) of the 2nd to 4th lumbar spines between the start and end of the study in patients with glucocorticoid (GC)-dependent nephrotic syndrome treated with GC alone (GC group) or in combination with cyclosporine (GC + CsA group). The percent of young adult mean BMD (%YAM) decreased significantly during the study period in the GC group, while the decrease in %YAM BMD was not statistically significant in the GC + CsA group

Correlation between bone mineral density (BMD) and the cumulative glucocorticoid dose (prednisolone) in patients with nephrotic syndrome treated with prednisolone alone (GC group) or in combination with CsA (GC + CsA group). The decrease in the slope in the GC + CsA group was shallower than that in the GC group despite the continuous treatment with prednisolone
Discussion
In this study, we demonstrated that CsA combined with GC attenuated the rate of decrease in BMD in patients with nephrotic syndrome compared with GC monotherapy. Although many patients with NS respond initially to GC therapy, relapse requires repeated courses of GC, which may result in significant GC toxicity. Therefore, patients with frequent relapses who develop GC dependency require alternative treatment [1]. CsA allows for reductions in GC doses during the initial period of treatment, although the need for prolonged GC administration after remission is associated with an increased risk of osteoporosis [2, 5]. CsA is frequently used to treat relapsing NS, and previous reports have documented the beneficial effects of CsA in this setting [1, 13, 14]. Eguchi et al. [15] reported that GC combined with CsA would facilitate early remission and allow reductions of the GC dose in patients with NS. However, because long-term treatment with both agents is necessary to maintain remission, side effects may accumulate.
Previous reports examining the effects of CsA on bone metabolism raised some controversy. For example, immunosuppressive therapy in transplant patients was reported to accelerate the development of severe osteoporosis, increasing the risk of fracture [16, 17]. Administration of CsA at doses similar to those used in transplantation causes acceleration of bone turnover, loss of trabecular bone, increased bone resorption, and inadequate remodeling [7, 18]. CsA is known to cause acute, rapid, and severe bone loss [7, 16]. Bone loss is dose-dependent and reversible after discontinuation of CsA [19]. However, this phenomenon, characterized by extremely high turnover in terms of bone loss and increased resorption, was not seen in other studies [8, 20]. Recipients of renal transplant who were treated with CsA without GC showed a significant improvement in BMD, suggesting that CsA did not interfere with bone mineralization, consistent with our results. T lymphocytes are critical for bone loss, as the occurrence of bone loss cannot be reproduced in T lymphocyte-deficient nude rats [21]. Rat studies have shown that osteoblasts express mRNA and protein for all isoforms of calcineurin [22]. The Ca2+/calmodulin-sensitive phosphatase calcineurin is a necessary downstream mediator controlling osteoclast differentiation [9]. Calcineurin is necessary for the formation of osteoclasts from their precursors, and this occurs via an NFATc1-dependent mechanism [3]. Consequently, CsA, a calcineurin inhibitor, is thought to inhibit bone resorption by isolated osteoclasts [23]. Considering the findings of these previous reports, the effects of CsA on bone metabolism have yet to be established in patients with nephrotic syndrome.
Here, we showed that the use of CsA mitigated the rate of decrease in BMD and that it did not significantly promote the decrease of BMD in patients with nephrotic syndrome. CsA is often used in combination with GC, which is known to compound this effect. While GC is associated with a low rate of turnover and bone loss, CsA promotes a high rate of turnover [3]. Therefore, combination therapy did not significantly influence bone metabolism, based on the changes in biochemical markers, in patients with nephrotic syndrome. In fact, none of the patients in our study experienced vertebrate bone fracture during the 1-year follow-up. Although the two groups of subjects included in this study differed in terms of age and sex, the excess prevalence of younger males with minimal change NS is unlikely to bias our results in terms of bone metabolism. These concepts lead us to consider that treatment with CsA for 1 year did not accelerate GC-induced osteoporosis in patients with nephrotic syndrome aged <50 years old and before menopause. In conclusion, we postulate that CsA is suitable for the treatment of GC-dependent NS, because it did not adversely affect bone metabolism and had favorable glomerular effects.
References
van Husen M, Kemper MJ (2011) New therapies in steroid-sensitive and steroid-resistant idiopathic nephrotic syndrome. Pediatr Nephrol 26:881–892
Ito K, Fujita T, Satomura A, Matsumoto K (2006) Useful therapy of cyclosporine A for adult steroid-dependent nephrotic syndrome. J Nihon Univ Med Ass 65:326–332 (in Japanese)
Tamler R, Epstein S (2006) Nonsteroid immune modulators and bone disease. Ann NY Acad Sci 1068:284–296
Sessa A, Esposito A, Iavicoli GD, Lettieri E, Dente G, Costa C, Bergallo M, Rossano R, Capuano M (2010) Immunosuppressive agents and bone disease in renal transplant patients with hypercalcemia. Transpl Proc 42:1148–1155
Mitchell DR, Lyles KW (1990) Glucocorticoid-induced osteoporosis: mechanisms for bone loss; evaluation of strategies for prevention. J Gerontol 45:M153–M158
Fujita T, Satomura A, Hidaka M, Ohsawa I, Endo M, Ohi H (2000) Acute alteration in bone mineral density and biochemical markers for bone metabolism in nephritic patients receiving high-dose:glucocorticoid and one-cycle etidronate therapy. Calcif Tissue Int 66:195–199
Movsowitz C, Epstein S, Ismail F, Fallon M, Thomas S (1989) Cyclosporin A in the oophorectomized rat: unexpected severe bone resorption. J Bone Miner Res 4:393–398
Stein B, Halloran B, Reinhardt T, Engstrom GW, Bales CW, Drezner MK, Currie KL, Takizawa M, Adams JS, Epstein S (1991) Cyclosporin-A increases synthesis of 1,25-dihydroxyvitamin D3 in the rat and mouse. Endocrinology 128:1369–1373
Sun L, Peng Y, Zaidi N, Zhu LL, Iqbal J, Yamoah K, Wang X, Liu P, Abe E, Moonga BS, Epstein S, Zaidi M (2007) Evidence that calcineurin is required for the genesis of bone-resorbing osteoclasts. Am J Physiol Renal Physiol 292:F285–F291
Krolner B, Pors Nielsen S (1980) Measurement of bone mineral content (BMC) of the lumbar spine. I. Theory and application of a new two-dimensional dual-photon attenuation method. Scand J Clin Lab Invest 40:653–663
Garnero P, Grimaux M, Demiaux B, Preaudat C, Seguin P, Delmas PD (1992) Measurement of serum osteocalcin with a human-specific two-site immunoradiometric assay. J Bone Miner Res 7:1389–1398
Robins SP, Woitge H, Hesley R, Ju J, Seyedin S, Seibel MJ (1994) Direct, enzyme-linked immunoassay for urinary deoxypyridinoline as a specific marker for measuring bone resorption. J Bone Miner Res 9:1643–1649
Hulton SA, Neuhaus TJ, Dillon MJ, Barratt TM (1994) Long-term cyclosporin A treatment of minimal-change nephrotic syndrome of childhood. Pediatr Nephrol 8:401–403
Hodson EM, Willis NS, Craig JC (2008) Non-corticosteroid treatment for nephrotic syndrome in children. Cochrane Database Syst Rev 23:CD002290
Eguchi A, Takei T, Yoshida T, Tsuchiya K, Nitta K (2010) Combined cyclosporine and prednisolone therapy in adult patients with the first relapse of minimal-change nephrotic syndrome. Nephrol Dial Transpl 25:124–129
Ponticelli C, Aroldi A (2001) Osteoporosis after organ transplantation. Lancet 357(9268):1623
Moreno A, Torregrosa JV, Pons F, Campistol JM, Martínez de Osaba MJ, Oppenheimer F (1999) Bone mineral density after renal transplantation: long-term follow-up. Transpl Proc 31:2322–2323
Movsowitz C, Epstein S, Fallon M, Ismail F, Thomas S (1988) Cyclosporine A in vivo produces severe osteopenia in the rat: effect of dose and duration of administration. Endocrinology 123:2571–2577
Schlosberg M, Movsowitz C, Epstein S, Ismail F, Fallon MD, Thomas S (1989) The effect of cyclosporin A administration and its withdrawal on bone mineral metabolism in the rat. Endocrinology 124:2179–2184
Grotz W, Mundinger A, Gugel B, Exner V, Reichelt A, Schollmeyer P (1994) Missing impact of cyclosporine on osteoporosis in renal transplant recipients. Transpl Proc 26:2652–2653
Buchinsky FJ, Ma Y, Mann GN, Rucinski B, Bryer HP, Romero DF, Jee WS, Epstein S (1996) T lymphocytes play a critical role in the development of cyclosporin A induced osteopenia. Endocrinology 137:2278–2285
Sun L, Blair HC, Peng Y, Zaidi N, Adebanjo OA, Wu XB, Wu XY, Iqbal J, Epstein S, Abe E, Moonga BS, Zaidi M (2005) Calcineurin regulates bone formation by the osteoblast. Proc Natl Acad Sci USA 102:17130–17135
Aroldi A, Tarantino A, Montagnino G, Cesana B, Cocucci C, Ponticelli C (1997) Effects of three immunosuppressive regimens on vertebral bone density in renal transplant recipients. Transplantation 63:380–386
Conflict of interest
The authors have no conflicts of interest to declare.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Shimizu, C., Fujita, T., Fuke, Y. et al. Effects of cyclosporine on bone mineral density in patients with glucocorticoid-dependent nephrotic syndrome in remission. Int Urol Nephrol 45, 803–808 (2013). https://doi.org/10.1007/s11255-012-0264-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-012-0264-3