
Abstract
Objective
This systematic review aims to assess the accuracy of the COMPASS-CAT tool in predicting venous thromboembolism (VTE) among cancer patients.
Methods
Relevant studies were searched in PubMed, Web of Science, The Cochrane Library, Embase, CINAHL, OVID, CBM, CNKI, WanFang Data, and VIP database from their inception up to April 19, 2023. The quality of studies was appraised using the diagnostic test accuracy study bias assessment tool (QUADAS-2). Quantitative analysis was performed using Stata MP 17.0.
Results
Thirteen studies involving 8,665 patients were included. Meta-analysis indicated that the COMPASS-CAT score had a pooled sensitivity of 0.76 [95%CI (0.61, 0.86)], specificity of 0.67 [95%CI (0.52, 0.79)], positive likelihood ratio of 2.3 [95%CI (1.7, 3.1)], negative likelihood ratio of 0.36 [95%CI (0.23, 0.54)], diagnostic odds ratio of 6 [95%CI (4, 10)], and an area under the Summary Receiver Operating Characteristic (SROC) curve (AUC) of 0.77 [95%CI (0.74, 0.81)]. Funnel plots indicated no publication bias. Meta-regression and subgroup analysis suggested that country and diagnostic setting might be potential sources of heterogeneity. The sensitivity of the COMPASS-CAT assessment tool in international outpatient settings was 0.94 with an AUC of 0.86, while in domestic inpatient settings, the sensitivity was 0.65 with an AUC of 0.78.
Conclusion
The COMPASS-CAT score had a certain diagnostic value for VTE in cancer patients and can effectively identify patients at risk of VTE. Most studies focus on patients with lung cancer. Future research should investigate more tumor types, and high-quality, large-sample, multi-center prospective studies on larger populations with cancers are warranted.
Highlights
The COMPASS-CAT thrombosis risk assessment model has been widely used to predict VTE risk in patients with solid tumors worldwide.
This study conducted a meta-analysis of 13 articles, and the results showed that the COMPASS-CAT thrombosis risk assessment model can effectively identify patients at risk of VTE, with a pooled sensitivity of 0.76 and specificity of 0.67. The area under the ROC curve is 0.77, indicating that the scale has certain accuracy.
It is helpful to select a suitable venous thrombosis risk assessment model for tumor patients.
Graphical Abstract
Accuracy of the COMPASS-CAT Thrombosis Risk Assessment Scale in Predicting Venous Thromboembolism in Cancer Patients: A Meta-Analysis.

Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
As is well known, venous thromboembolism (VTE), including deep vein thrombosis (DVT) and pulmonary embolism (PE), significantly affect patient health [1]. It is notably linked to malignant tumors, with cancer-associated VTE posing a common life-threatening complication for adult cancer patients. Such patients have a 4-6.5 times higher risk of developing VTE compared to non-cancer individuals [2, 3]. Furthermore, established cancer-associated VTE significantly contributes to morbidity and is the second leading cause of death among cancer patients [4]. National and international guidelines recommend routine assessment for individuals at high risk of VTE [5,6,7,8]; however, the recommended assessment tools are not specific to cancer patients. In 2017, Gerotziafas et al. developed the COMPASS-CAT risk assessment model based on cancer patients, incorporating tumor-related factors, laboratory characteristics, and clinical features [9]. Several domestic and international studies have applied the COMPASS-CAT assessment scale for solid tumor prediction. Although these studies suggest that the model can comprehensively assess VTE risk in cancer patients, variations in study subjects, regions, scenarios, sample sizes, and threshold values have resulted in diverse outcomes. Therefore, this study evaluates the predictive performance of the COMPASS-CAT thrombosis risk assessment scale for VTE in cancer patients through meta-analysis, aiming to provide a reference for clinical practitioners in selecting appropriate venous thrombosis assessment tools.
Materials and methods
Inclusion and exclusion criteria
Inclusion Criteria:
-
1.
Study Type: Diagnostic studies.
-
2.
Study Subjects: Individuals aged ≥ 18 years, diagnosed with cancer through histopathological or cytological examination.
-
3.
Assessment Tool: The COMPASS-CAT thrombosis risk assessment scale.
-
4.
Diagnostic Criteria: DVT is defined as a positive result in venous color ultrasound, venography, or magnetic resonance venography (MRV) (including central venous catheter (CVC)-associated VTE). For PE, a positive result in pulmonary arteriography, nuclear lung ventilation/perfusion scanning, or Magnetic Resonance Pulmonary Angiography (MRPA) [10, 11].
-
5.
Outcome Measures: Sensitivity (SEN), specificity (SPE), positive likelihood ratio (PLR), negative likelihood ratio (NLR), diagnostic odds ratio (DOR), and the area under the summary receiver operating characteristic curve (SROC AUC).
Exclusion Criteria:
-
1.
Cross-sectional studies, animal experiments, literature reviews, meta-analyses, and systematic reviews that are non-diagnostic in nature.
-
2.
Studies with incorrect methodology, incomplete data, or those where 2 × 2 table data cannot be extracted.
-
3.
Literature with duplicate publications or data.
-
4.
Non-Chinese and non-English literature.
Search strategy
A computerized search was conducted in PubMed, Web of Science, The Cochrane Library, Embase, CINAHL, OVID, Chinese Biomedical Literature Database (CBM), China National Knowledge Infrastructure (CNKI), WanFang Data, and VIP database from their inception up to April 19, 2023. The search terms in Chinese databases included thrombosis, venous thrombosis, venous thromboembolism, venous thromboembolism, deep vein thrombosis, deep vein thrombosis, pulmonary thromboembolism, pulmonary embolism, pulmonary thromboembolism; cancer, cancer, tumor, tumor, malignancy, leukemia, malignant diseases; COMPASS-CAT, COMPASS-CAT risk assessment, COMPASS-CAT thrombotic risk assessment scale, COMPASS-CAT thrombotic risk assessment model, COMPASS-CAT score, risk assessment. In English databases, the terms included “venous thrombosis, thrombosis, pulmonary embolism, venous thromboembolism, deep venous thrombosis, deep vein thrombosis, pulmonary thromboembolism, phlebothrombosis; neoplasms, cancer, tumor, carcinoma, malignancy, oncology, malignant neoplasm, benign neoplasm; COMPASS-CAT, COMPASS-CAT risk assessment model, COMPASS-CAT risk assessment scale, COMPASS-CAT risk score, risk assessment”. The search strategy was designed by combining MeSH terms and free text terms and was adjusted according to each database. Additionally, manual searches were conducted to trace the references of the included studies to avoid omissions. An example of the search strategy in PubMed is as follows:
#1 venous thrombosis OR thrombosis OR pulmonary embolism OR venous thromboembolism OR deep venous thrombosis OR deep vein thrombosis OR pulmonary thromboembolism OR phlebothrombosis.
#2 neoplasms OR cancer OR tumor OR carcinoma OR malignancy OR oncology OR malignant neoplasm OR benign neoplasm.
#3 COMPASS-CAT OR COMPASS-CAT risk assessment model OR COMPASS-CAT risk assessment scale OR COMPASS-CAT risk score.
#4 #1 AND #2 AND #3.
Literature screening and data extraction
Based on the objectives of this study and the inclusion and exclusion criteria, two researchers independently conducted a preliminary screening based on the titles and abstracts of the literature. In cases of disagreement, a decision was made in consultation with a third researcher. After excluding duplicate and irrelevant literature, the full texts were further reviewed, and those that could not be accessed or did not meet the inclusion and exclusion criteria were excluded. Data extracted included the first author, publication year, country, sample size, cancer type, gold standard, study type, cutoff values, true positives, false positives, false negatives, and true negatives. If data were incomplete, attempts were made to contact the original authors via email to obtain the relevant data. If relevant data were ultimately unobtainable, the literature was excluded.
Quality assessment
The quality of the included studies was independently assessed by two researchers according to the Cochrane-recommended diagnostic test accuracy study bias assessment tool (QUADAS-2), comprising 13 items. Each literature was evaluated against these items with three answers: “Yes,” “No,” and “Unclear.” A study was classified as high quality (Grade A) if it fully met the criteria; medium quality (Grade B) if it partially met the criteria; and low quality (Grade C) if it did not meet the criteria. In cases of disagreement, discussions were held, or a decision was made by a third researcher.
Statistical methods
In accordance with the QUADAS-2 criteria, RevMan 5.3 was used to fill in the quality of the included studies and to create diagrams. Meta-analysis of diagnostic studies was conducted using Stata MP 17.0, while the pooled SEN, SPE, PLR, NLR, DOR, and 95% confidence interval (CI) were calculated. Summary Receiver Operating Characteristic (SROC) curves were drawn, and the area under the ROC curve (AUC) was estimated. Heterogeneity analysis was performed using the I² test, with I² > 50% and P < 0.05 indicating significant heterogeneity, prompting further investigation into sources of heterogeneity. If I² < 50% and P > 0.05, heterogeneity among the included studies was considered low. Sensitivity analysis was conducted to evaluate the stability of the study results by assessing the impact of excluding any one study on the overall effect size. Deeks’ funnel plot asymmetry test was used to assess publication bias, with P > 0.05 indicating no publication bias.
Results
Literature search results
A systematic search yielded a total of 4,948 related articles. After deduplication using EndNote X9.1 software, 4,007 articles remained. Upon reading titles and abstracts, 3,987 articles were excluded, including 3,792 articles irrelevant to the topic, 3 conference abstracts, and 9 reviews. Full-text review further excluded 7 studies for incomplete or duplicate data. Ultimately, 13 studies [9, 12,13,14,15,16,17,18,19,20,21,22,23] were included. The literature screening process and results are shown in Fig. 1.

Literature screening process and results
Basic characteristics of included literature
The 13 included articles comprised a total of 8,665 cases, among which VTE occurred in 1,089 cases. The basic characteristics of the included literature are presented in Table 1.
Quality assessment of included literature
The quality assessment results of the included literature are shown in Fig. 2.

Risk of bias assessment results
Meta-analysis results
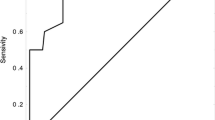
The 13 studies were quantitatively meta-analyzed. The pooled SEN was 0.76 [95%CI (0.61, 0.86)], with high heterogeneity among the studies (I² = 96.23%). The pooled SPE was 0.67 [95%CI (0.52, 0.79)], with high heterogeneity (I² = 99.69%). Pooled PLR was 2.3 [95%CI (1.7, 3.1)]; Pooled NLR was 0.36 [95%CI (0.25, 0.52)]; DOR was 6 [95%CI (4, 10)]; and the AUC was 0.77 [95%CI (0.74, 0.81)]. The forest plots for sensitivity and specificity are shown in Fig. 3, and the SROC fitting curve is in Fig. 4.

Sensitivity and specificity forest plots

SROC fitting curve
Sensitivity analysis
Sensitivity analysis of the included studies revealed anomalies in two papers [14, 21], as seen in Fig. 5. After excluding these two anomalous studies, the quantitative synthesis showed that pooled SEN was 0.77 [95%CI (0.60, 0.88)], with I² = 97.48%; Pooled SPE was 0.66 [95%CI (0.48, 0.80)], with I² = 99.69%. Pooled PLR, NLR, DOR, and AUC were 2.2 [95%CI (1.6, 3.2)], 0.36 [95%CI (0.23, 0.54)], 6 [95%CI (4, 10)], and 0.78 [95%CI (0.74, 0.81)], respectively. The minimal changes in values after exclusion indicate good stability of the meta-analysis results.

Sensitivity analysis
Publication bias
The Deeks’ test result showed no significant publication bias in the included studies (P = 0.48). The publication bias result is presented in Fig. 6.

Publication bias test
Meta-regression and subgroup analysis
Meta-regression was used to identify potential sources of heterogeneity among the included literature, considering factors like country and diagnostic setting, cancer type, study type, and sample size. Results showed that country and diagnostic setting significantly influenced the heterogeneity of the combined sensitivity results (P < 0.001), suggesting that they were potential sources of heterogeneity. Subgroup analysis based on country and diagnostic setting, cancer type, study type, and sample size revealed that the sensitivity of the COMPASS-CAT scale in non-Chinese outpatient settings was 0.94, with an AUC of 0.85, whereas diagnostic accuracy of the COMPASS-CAT thrombosis risk assessment scale was higher in foreign outpatient settings., The specificity of this scale in assessing venous thrombosis risk was higher in lung cancer patients (specificity: 0.75). In prospective studies, sensitivity, specificity, DOR, and AUC were all higher than those in retrospective studies. The results of the subgroup analysis are presented in Table 2.
Discussion
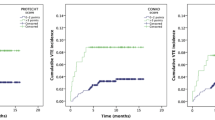
The incidence, recurrence rate, and mortality of VTE in patients with active cancer are high, making it a common and life-threatening complication and the second leading cause of death. Therefore, preventing VTE is crucial [24]. Early identification of high-risk patients for VTE and targeted prevention and treatment require reliable assessment tools [25]. Guidelines recommend the Caprini and Padua thrombosis risk assessment scales [5, 10], but both scales are based on non-cancer patients and do not consider the impact of cancer-related factors on thrombosis risk. The Khorana thrombosis risk assessment scale, designed for outpatient chemotherapy patients, predicts VTE risk based on cancer site and pre-chemotherapy blood cell counts. However, multiple reports indicate poor predictive ability of this scale across various cancer types [26,27,28]. PROTECHT and CONKO scores refine the Khorana scale for assessing thrombosis risk. PROTECHT incorporates chemotherapy agents like gemcitabine and platinum-based drugs [29], while CONKO, focusing on advanced pancreatic cancer patients treated with low molecular weight heparin, opts for performance status (PS) over BMI. Although PS scores have been shown to be associated with an increased risk of venous thromboembolism in hospitalized cancer patients [30], the CONKO score is almost identical to the Khorana score. A study by Van Es [31] on 876 cancer patients found PROTECHT seems to be potentially more effective in distinguishing between low and high-risk groups. The COMPASS-CAT thrombosis risk assessment scale, tailored for cancer patients, has been used in many domestic and international studies to predict VTE risk in solid tumor patients. Yan AR et al. [32] focused on outpatient lung cancer patients. Their results showed that the COMPASS-CAT score showed a significantly better discriminatory capability, but the pooled data was obtained from only three studies, with high heterogeneity. Furthermore, sensitivity and specificity analyzes were not performed in their study. Conversely, our study conducted a meta-analysis of eligible 13 studies, involing 8665 patients with lung cancer, breast cancer, colorectal cancer, or ovarian cancer showed that the COMPASS-CAT assessment scale had a pooled sensitivity of 0.76 and a pooled specificity of 0.67 for VTE prediction, with a false negative rate of 0.24% and a false positive rate of 0.33%, indicating that its clinical use could easily identify at-risk patients, but also lead to false positives for VTE risk. The AUC was 0.77, which was between 0.7 and 0.9, indicating a certain level of accuracy for this assessment.
Subgroup analysis in our study showed that the pooled sensitivity and AUC of the COMPASS-CAT assessment scale in foreign outpatient settings was 0.94 and 0.86, respectively, which were significantly higher than those in domestic inpatients. This may be due to the scale being originally developed based on foreign outpatient data, making it better at identifying VTE risk in these patients, and thus having higher diagnostic value. The AUC of 0.78 in inpatients suggests that the COMPASS-CAT assessment scale also has a certain level of accuracy in domestic inpatient settings.
This study has several limitations. First, the included studies are highly heterogeneous. Although factors such as country and diagnostic setting, cancer type, study type, and sample size have explained the sources of heterogeneity to some degree, heterogeneity remains high. This may be related to differences in case selection, gold standards, and tumor treatment protocols among the studies. Not all studies used consistent thresholds. Despite only two employing different ones and the ‘shoulder-arm’ shape of the sROC curve is not prominent, threshold effects on outcomes can’t be disregarded. Therefore, sensitivity analysis was conducted to address this issue, and the results demonstrated good stability. Future research should aim to define optimal risk stratification thresholds. Second, the study focuses on lung cancer, limiting broader applicability. Third, most of the included literature is retrospective, with fewer prospective studies. This may be because patients require regular ultrasound and imaging examinations, increasing the workload of medical staff. Furthermore, patients need to visit hospitals repeatedly, leading to reduced compliance, and they pay less attention to VTE, making it difficult to conduct prospective studies. Last, only Chinese and English literature was included, potentially introducing selection bias.
In conclusion, the COMPASS-CAT thrombosis risk assessment scale is a relatively objective tool for predicting VTE risk in cancer patients. It has good sensitivity and specificity, and it holds a diagnostic value in identifying the risk of VTE in cancer patients, aiding healthcare professionals in early identification of patients at high risk for VTE. However, the number of studies included in this research is limited and the heterogeneity among them is significant. Therefore, large-scale, multicenter, high-quality prospective studies are still needed to validate these findings.
Data availability
Data sharing not applicable to this article as no datasets were generated or analysed during the current study.
References
Yang X, Ma S, Xu H et al (2023) Construction and validation of the prediction model for venous thromboembolism risk in elderly non-surgical patients in ICU. Chin Nurs Res 37(05):791–799
Trousseau A (1865) Clinique médicale de l’Hôtel-Dieu de Paris v, vol 3. JB Baillière
Ay C, Pabinger I, Cohen AT (2017) Cancer-associated venous thromboembolism: Burden, mechanisms, and management. Thromb Haemost 117(2):219–230
Gerotziafas GT, Mahé I, Lefkou E et al (2020) Overview of risk assessment models for venous thromboembolism in ambulatory patients with cancer. Thromb Res 191(Suppl 1):S50–s7
Key NS, Khorana AA, Kuderer NM et al (2020) Venous thromboembolism prophylaxis and treatment in patients with Cancer: ASCO Clinical Practice Guideline Update. J Clin Oncol 38(5):496–520
Farge D, Frere C, Connors JM et al (2019) 2019 international clinical practice guidelines for the treatment and prophylaxis of venous thromboembolism in patients with cancer. Lancet Oncol 20(10):e566–e81
Streiff MB, Holmstrom B, Angelini D et al (2021) Cancer-Associated venous thromboembolic Disease, Version 2.2021, NCCN Clinical Practice guidelines in Oncology. J Natl Compr Canc Netw 19(10):1181–1201
Ma J, Qin S, Wu Y et al (2019) Guidelines for the Prevention and Treatment of Tumor-related venous thromboembolism (2019 Edition). Chin J Clin Oncol 46(13):653–660
Gerotziafas GT, Taher A, Abdel-Razeq H et al (2017) A predictive score for thrombosis Associated with breast, colorectal, lung, or ovarian Cancer: the prospective COMPASS-Cancer-Associated thrombosis study. Oncologist 22(10):1222–1231
PEaPVDGotRDBotCMA (CMA), Pulmonary Embolism and Pulmonary Vascular Disease Working Committee RPB, Chinese Medical Association (CMA), Disease NCGfPaToPEaPV (2018) guidelines for the diagnosis, treatment and prevention of pulmonary thromboembolism. Natl Med J China 98(14): 1060–1087
Vascular Surgery Group CSoS, Chinese Medical Association (2017) Guidelines for the diagnosis and treatment of deep vein thrombosis (Third Edition). Chin J Gen Surg 32(9):807–812
Wang Y, Ma F, Liu B et al (2020) Risk prediction of venous thromboembolism in non-small cell lung cancer patients based on COMPASS-CAT risk assessment model. Chin J Oncol 42(4):340–345
Wang Y, Yang K, Zhang M et al (2020) Comparison of predictive value of different risk assessment models for venous thromboembolism in elderly patients with lung cancer. Chin J Geriatr 39(4):430–434
Tan K, Liu D, Liu H, Tang X (2021) Risk prediction of venous thromboembolism associated with gynaecologic cancer on the basis of the COMPASS-CAT risk assessment model. Chin J Gen Pract 19(12):2132–2540
Zhao L (2022) Comparison of the effectiveness of COMPASS-CAT, Padua and Khorana risk assessment models in predicting venous thromboembolism in lung cancer patients. Shanxi Med Univ
Xie L, Hang L, Zhang L et al (2022) Predictive value of the modified COMPASS-CAT Assessment Model for postoperative deep vein thrombosis in patients with gastrointestinal Ma?lignancies. Syst Med 7(22):27–30
Yuting Y, Qixia X, Yingying P et al (2021) Analysis of clinical characteristics of malignant tumors complicated with venous thromboembolism and evaluation of predictive models. Chin J Gen Pract 19(5):723–6808
Du C, Yu Z, Liu Z, Lv Y (2020) Risk factors of venous thromboembolism in lung cancer patients. Clin J Med Off 48(1):5–7
Spyropoulos AC, Eldredge JB, Anand LN et al (2020) External validation of a venous thromboembolic risk score for Cancer outpatients with solid tumors: the COMPASS-CAT venous thromboembolism risk Assessment Model. Oncologist 25(7):e1083–e90
Rupa-Matysek J, Lembicz M, Rogowska EK et al (2018) Evaluation of risk factors and assessment models for predicting venous thromboembolism in lung cancer patients. Med Oncol 35(5):63
Xiong W, Zhao Y, Du H et al (2021) Optimal authoritative risk assessment score of Cancer-associated venous thromboembolism for hospitalized medical patients with lung Cancer. Thromb J 19(1):95
Qi Q (2023) Clinical features and predictors of venous thromboembolism complicating lung cancer. Anhui South Med Coll
Syrigos K, Grapsa D, Sangare R et al (2018) Prospective Assessment of clinical risk factors and biomarkers of hypercoagulability for the identification of patients with lung adenocarcinoma at risk for Cancer-Associated thrombosis: the observational ROADMAP-CAT study. Oncologist 23(11):1372–1381
Cohen AT, Katholing A, Rietbrock S et al (2017) Epidemiology of first and recurrent venous thromboembolism in patients with active cancer. A population-based cohort study. Thromb Haemost 117(1):57–65
Patell R, Rybicki L, McCrae KR, Khorana AA (2017) Predicting risk of venous thromboembolism in hospitalized cancer patients: utility of a risk assessment tool. Am J Hematol 92(6):501–507
Mansfield AS, Tafur AJ, Wang CE et al (2016) Predictors of active cancer thromboembolic outcomes: validation of the Khorana score among patients with lung cancer. J Thromb Haemost 14(9):1773–1778
Rupa-Matysek J, Gil L, Kaźmierczak M et al (2017) Prediction of venous thromboembolism in newly diagnosed patients treated for lymphoid malignancies: validation of the Khorana risk score. Med Oncol 35(1):5
van Es N, Franke VF, Middeldorp S et al (2017) The Khorana score for the prediction of venous thromboembolism in patients with pancreatic cancer. Thromb Res 150:30–32
Verso M, Agnelli G, Barni S et al (2012) A modified Khorana risk assessment score for venous thromboembolism in cancer patients receiving chemotherapy: the Protecht score. Intern Emerg Med 7(3):291–292
Dou F, Li H, Zhu M et al (2018) Association between oncogenic status and risk of venous thromboembolism in patients with non-small cell lung cancer. Respir Res 19(1):88
van Es N, Di Nisio M, Cesarman G et al (2017) Comparison of risk prediction scores for venous thromboembolism in cancer patients: a prospective cohort study. Haematologica 102(9):1494–1501
Yan AR, Samarawickrema I, Naunton M et al (2024) Models for predicting venous thromboembolism in ambulatory patients with lung cancer: a systematic review and meta-analysis. Thromb Res 234:120–133
Funding
This study was funded by Scientific Research Project of Weifang Municipal Health Commission: wfwsjk-2019-181 The practice and effect evaluation of hospice care in the department of oncology in a Grade III general hospital. wfwsjs-2018-025 Analysis of clinical characteristics and prognosis of young individuals with myocardial infarction.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Writing - original draft preparation: Wei Zhou; Writing - review and editing: Shirong Fang; Conceptualization: Shujuan Chen; Methodology: Shujuan Chen; Formal analysis and investigation: Wei Zhou; Funding acquisition: Shirong Fang; Resources: Jinhong Yang; Supervision: Jinhong Yang, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
Not applicable.
Consent to participate
Not applicable.
Consent to publish
Not applicable.
Competing interests
The authors have no relevant financial or non-financial interests to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Zhou, W., Chen, S., Yang, J. et al. Accuracy of the COMPASS-CAT thrombosis risk assessment scale in predicting venous thromboembolism in cancer patients: a meta-analysis. J Thromb Thrombolysis (2024). https://doi.org/10.1007/s11239-024-03011-z
Accepted:
Published:
DOI: https://doi.org/10.1007/s11239-024-03011-z