
Abstract
Enoxaparin is a hydrophilic drug with obesity having little effect on its apparent volume of distribution, therefore patients with obesity receiving standard 1 mg/kg dosing may be at a higher risk of supratherapeutic dosing. Conversely, dose reducing patients with obesity could place already at risk patients at higher risk of a thrombotic event. Data and recommendations are variable for the most appropriate weight-based dose of therapeutic enoxaparin in obese patients, particularly those a weight > 100 kg or a body mass index (BMI) ≥ 40 kg/m2. The purpose of this systematic review was to globally evaluate these data to surmise optimal dosing recommendations for patients with obesity. A systematic review of English language studies was conducted and identified articles via Pubmed, EMBASE, and the Cochrane Central Register of Controlled Trials (CENTRAL) searches. Studies were included if they reported therapeutic enoxaparin use in adult patients with a BMI ≥ 40 kg/m2 or body weight > 100 kg and the percentage of patients achieving a therapeutic anti-Xa based on a weight-based dose or the weight-based dose required to produce a therapeutic anti-Xa level. Therapeutic attainment of anti-Xa levels were assessed across enoxaparin weight-based dosing categories including a very low dose group: < 0.75 mg/kg, low dose group: 0.75–0.85 mg/kg, and standard dose group: ≥ 0.95 mg/kg. Rates of bleeding and thrombosis were also evaluated. A total of eight studies were included. For anti-Xa level assessment, 682 patients were included. A total of 62% of anti-Xa levels were therapeutic in the very low dose group, 66% in the low dose group, and 42% in the standard dose group. Overall rates of total bleeding and thrombosis were assessed in 798 patients. A total of 29 bleedings (3.6%) occurred, and 27 reported a relationship to dose. Most bleedings, 85.2% (n = 23/27), occurred with doses in the standard dose group (≥ 0.95 mg/kg). Thrombosis occurred in 5 patients (0.6%). Utilization of a reduced weight-based dosing strategy for therapeutic enoxaparin in obese patients may increase the percentage of patients with a therapeutic anti-Xa level.
Key points
1. Current evidence for therapeutic enoxaparin use in obese patients mainly consists of small, retrospective data, but inappropriate dosing may lead to bleeding or thrombotic events.
2. This review identified eight studies that assessed therapeutic enoxaparin dosing in patients with a BMI ≥ 40 kg/m2 or > 100 kg and determined that patients with a reduced dosing regimen (0.75–0.85 mg/kg) achieved goal anti-Xa levels 66% of the time compared to 43% of the time with full weight-based dosing (≥ 0.95 mg/kg).
3. Rates of bleeding occurred in 3.6% of patients, most of which (> 85%) were in the full weight-based dosing group.
4. Use of a reduced weight-based dose of enoxaparin (0.75–0.85 mg/kg) may result in more obese patients with a BMI ≥ 40 kg/m2 or body weight > 100 kg achieving goal anti-Xa levels than full weight-based dosing.
5. Prospective randomized-controlled trials are required to verify clinical outcomes in this population.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Enoxaparin is commonly used for the treatment of acute coronary syndromes, venous thromboembolism, and stroke prevention in patients with atrial fibrillation; though it is a high-risk medication that can lead to bleeding events [1,2,3]. In 2016, almost 2 billion adults worldwide were overweight, with over 650 million of those being obese [4]. The pharmacokinetic properties of enoxaparin are predictable in most patients, which informed the traditional treatment dose of enoxaparin to be based on actual body weight, typically 1 mg/kg twice daily. However, in obese patients there is concern for supratherapeutic plasma concentrations with full weight-based dosing as obesity has little effect on the apparent volume of distribution of enoxaparin due to its hydrophilicity [1]. Though routine laboratory monitoring with anti-Xa assays is not necessary in most patients, it may be of benefit in this population due to supratherapeutic levels being observed [2]. Target peak anti-Xa levels for twice daily dosing are typically 0.5 or 0.6-1.0 IU/mL and can be utilized as a surrogate marker of therapeutic effectiveness and safety [3, 5,6,7]. Large registry data suggests full weight-based dosed enoxaparin in obese patients is associated with an increase in major bleeding and coupled with the pharmacokinetic profile of the drug, some experts advocate use of a reduced enoxaparin dose (< 1 mg/kg twice daily) [8,9,10].
Current guidelines either suggest against dose reductions or do not comment on dose adjustments in the obese population [11,12,13]. The CHEST guidelines for treatment of VTE do not make a recommendation regarding enoxaparin dosing and the American Society of Hematology (ASH) guidelines suggest obese patients receive enoxaparin full weight-based dosing without a dose maximum. This is a conditional recommendation based on very low certainty of evidence with the main concern being the potential serious impact of underdosing and treatment failure if lower than full weight-based doses are utilized.
To date, there have been several studies seeking to define optimal therapeutic enoxaparin dosing in obesity but these are generally small, single center, retrospective studies, some of which have conflicting conclusions [14,15,16,17,18,19,20,21,22,23]. This is likely why guidelines have not recommended reduced dosing in patients with obesity using full dose enoxaparin despite the pharmacokinetic profile of the drug. Due to risk of bleeding or thrombotic events associated with supra or subtherapeutic dosing, attention needs to be drawn to appropriate dosing in this population. To better align and assess the evidence available, a systematic review of therapeutic enoxaparin dosing strategies in obese patients based on resultant anti-Xa levels was conducted.
Methods
Search strategy and study selection
An electronic literature search was performed in PubMed, EMBASE, and the Cochrane Central Register of Controlled Trials (CENTRAL). The parameters utilized for the database search included: “obesity” OR “obese” AND “low molecular weight heparin” OR “enoxaparin” from the January 1st, 2000 through April 27th, 2022. Filters were set to include studies written in English and exclude animal studies.
Studies met inclusion criteria if they reported therapeutic enoxaparin use in adult patients with a BMI ≥ 40 kg/m2 or body weight > 100 kg and reported an outcome of interest. Trials were included if the dosages in the inclusion criteria were ≤ 1 mg/kg twice daily for CrCl ≥ 30 ml/min and ≤ 1 mg/kg daily for non-hemodialysis patients with a CrCl < 30 ml/min for therapeutic indications such as DVT or PE. Outcomes of interest included the percentage of patients achieving a therapeutic anti-Xa based on a weight-based dose and the weight-based dose required to produce a therapeutic anti-Xa. Therapeutic attainment of anti-Xa levels was assessed across enoxaparin weight-based dosing categories including a very low dose group: < 0.75 mg/kg, low dose group: 0.75–0.85 mg/kg, and standard dose group: ≥ 0.95 mg/kg. These dosing categories were chosen after visual inspection of the data in an attempt to assimilate the data into dosage groups used in clinical practice while taking into consideration the spread of the data to ensure the results of the systematic review were reflective of the individual study data. In studies that utilized and evaluated a set, weight-based dose, that dose determined the category grouping. When the enoxaparin weight-based dose was reported as a median and interquartile range (IQR), the median and interquartile range (IQR) were used to determine the dosing category. When this occurred, the median dose and IQR was required to be 0.02 mg/kg from the upper or lower range of the dose group, to ensure the data included was representative of dosages in that specific weight-based group. In cases of multiple anti-Xa level assessments and/or dose adjustments, the first dose and anti-Xa level reported was utilized for systematic review purposes. Each institution’s determination of anti-Xa sampling time and laboratory specific therapeutic anti-Xa levels were used. Review articles, case reports/series, articles on LMWHs other than enoxaparin (i.e., dalteparin and tinzaparin), hemodialysis, and articles on pediatric and pregnant patients were excluded.
Six reviewers (MC, KZ, UA, AD, SR, AS) working in pairs of two independently screened each abstract for relevance. The full-length text of each eligible study was examined by the assigned reviewer pair and reasons for exclusion were documented. Any disagreement between abstract and full-text selection was resolved by a third reviewer. After identifying eligible studies, the same investigators independently searched through the reference lists of included studies to identify articles that may not have been captured by the database search.
Outcomes
The primary outcome was the percentage of patients achieving a goal anti-Xa level based on the weight-based enoxaparin dose in mg/kg. The secondary outcome was an evaluation of effectiveness and safety as determined by rates of thrombosis and bleeding while receiving enoxaparin therapy. Thrombotic events were defined in alignment with the reporting paper. When bleeding events were described, they were categorized into the International Society of Thrombosis and Haemostasis (ISTH) definition of major bleeding as determined by initial paper definition or a decrease in hemoglobin of at least 2 g/dL [24].
Data extraction and risk of Bias Assessment
Data extraction of included full-text articles was divided among six reviewers (MC, KZ, UA, AD, SR, AS) which were synthesized into two summary tables for trial design and outcomes. Reviewers recorded available data on trial design, inclusion/exclusion criteria, anti-Xa monitoring procedures, sample size, patient characteristics (weight/BMI, creatinine clearance/glomerular filtration rate), weight-based doses of enoxaparin (mg/kg), percentage of patients achieving goal anti-Xa, dose required to achieve therapeutic anti-Xa levels, bleeding, and thromboembolic outcomes.
Two independent reviewers (MC, AW) assessed risk of bias for included studies. The Newcastle-Ottawa scale was used for observational studies while the Cochrane Collaboration’s Risk of Bias 2.0 tool was used for randomized clinical trials (RCTs) [25, 26]. Disagreements were resolved by a third reviewer.
Data synthesis
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist was used (Supplementary Fig. 1). Due to the heterogeneity in patient populations and outcomes, data was summarized descriptively, and qualitative synthesis of the data was performed (Supplementary Tables 1–2).
Results
Search results
The database search produced 1191 manuscripts and 551 were included in the initial screening after the removal of duplicate papers. Sixteen full length papers were reviewed, and after applying inclusion and exclusion criteria, a total of eight manuscripts were included in the systematic review (Fig. 1) [14,15,16,17,18,19,20,21].

Flow diagram of included studies
Study characteristics
Of the included articles, seven evaluated a set enoxaparin mg/kg dose and one evaluated prescribing practices in their institution and described dose retrospectively in relationship to goal attainment of anti-Xa levels (Tables 1 and 2). Included studies were published between 2015 and 2021 and evaluated 798 patients. Two studies were conducted in Australia with the remaining being conducted in the US. Six studies were single-centered, retrospective studies; one was a multicenter, retrospective study; and one was a randomized controlled trial. Study durations followed patients while hospitalized and receiving enoxaparin therapy or until first goal anti-Xa level was attained. Patients were monitored for thrombosis and bleeding outcomes until therapeutic anti-Xa level or the duration of enoxaparin therapy in four studies, were assessed for five days after therapy in one study, 30 days in two studies, and 90 days in one study.
Percent anti-xa goal attainment
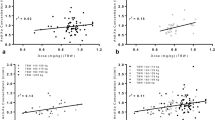
A total of 682 patients in eight studies with reported anti-Xa levels were assessed. There were 37 patients who received a dose < 0.75 mg/kg and 62% (n = 23/37) had anti-Xa levels that were therapeutic at their institution, 27% (n = 10/37) subtherapeutic, and 11% (n = 4/37) supratherapeutic. There were 88 patients who received dose between 0.75 and 0.85 mg/kg, of which 66% (n = 58/88) were therapeutic, 13% (n = 11/88) subtherapeutic and 22% (n = 19/88) supratherapeutic. There were 557 patients who received a dose greater than or equal to 0.95 mg/kg and 42% (n = 232/557) were therapeutic, 7% (n = 39/557) subtherapeutic, and 51% (n = 286/557) supratherapeutic. Figure 2 depicts the anti-Xa results by dosing group.

Comparison of therapeutic anti-Xa levels by weight-based dosage group
Clinical outcomes
There were 798 patients across the eight included studies who were evaluated for bleeding and thrombosis outcomes. Overall rates of total bleeding were 3.6% (n = 29/798). Two bleeding events were not defined, and of the 27 bleeding events that were, rates of ISTH major bleeding were 77.8% (n = 21/27). Of the 29 total bleeding events, 27 were reported in relationship to the weight-based enoxaparin dose received and 85.2% (n = 23/27) occurred with doses ≥ 0.95 mg/kg. Of these 29 bleeding events, 22 had anti-Xa levels documented of which, 13 (59%) were supratherapeutic. Rates of thrombosis were 0.6% (n = 5/798). Three thrombotic events were described in relation to their weight-based enoxaparin group, and one occurred in the 0.75-0.85 mg/kg (33.3%) dosing group and two occurred in the ≥ 0.95 mg/kg (66.7%) dosing group. Of the five thrombotic events, four anti-Xa levels were reported of which three (75%) were therapeutic and one (25%) was supra-therapeutic.
Discussion
In this systematic review, anti-Xa levels, bleeding and thrombotic events were evaluated in obese patients receiving full dose enoxaparin therapy at standard (≥ 0.95 mg/kg) versus reduced dosages that were grouped into < 0.75 mg/kg (very low) and 0.75–0.85 mg/kg (low) categories. Patients receiving 0.75–0.85 mg/kg experienced more therapeutic anti-Xa results without an apparent increase in thrombotic risk while patients receiving ≥ 0.95 mg/kg had fewer therapeutic anti-Xa levels with an apparent increase in bleeding events. In patients with obesity with a BMI ≥ 40 kg/m2 or a body weight > 100 kg, it may be prudent to use a dose of 0.75–0.85 mg/kg when utilizing full dose enoxaparin to optimize clinical outcomes.
One study in this review was not in alignment with the conclusion to adjust the dose of enoxaparin in obese patients [17]. In the Machlachlan study, the authors concluded that full, weight-based dosing should be utilized in obese patients as anti-Xa levels and clinical outcomes were not statistically significantly different between obese and non-obese groups receiving 1 mg/kg of enoxaparin every 12 h [17]. Importantly, this study was not powered to assess clinical outcomes with a small number of enrolled patients (n = 166). Additionally, there was a trend in increasing numbers of patients with a supratherapeutic anti-Xa result with increasing weight. 50% of patients weighing 130 kg or greater with a BMI over 45 kg/m2 had supratherapeutic levels and 59% of patients with a BMI over 50 kg/m2 had supratherapeutic levels. This suggests that as body weight and BMI increase, the weight-based dose required to elicit the same PD effect decreases, which is also supported by the other studies presented in this review [16, 18, 21]. Lastly, anti-Xa levels were drawn 2–6 h after the 2nd dose in this analysis. Pharmacokinetic data supports that max anti-Xa activity (Tmax) and time to steady state are prolonged in obese patients which could result in an underestimation of true pharmacodynamics of enoxaparin in this study [2]. With the trend in increasing supratherapeutic anti-Xa levels with increasing BMI as well as potential for anti-Xa levels to be drawn prior to steady state, it is challenging to conclude that a full weight-based dosing strategy is best for obese patients.
While anti-Xa levels are a surrogate measure of therapeutic activity, clinical outcomes, namely thrombosis and bleeding should also be considered. Data suggests improved clinical outcomes in obese patients when using reduced doses. [8, 9] In an analysis of 2846 patients weighing > 100 kg who received capped doses (18,000 IU/d) versus uncapped doses (> 18,000 IU/d) of LMWH for VTE, capped doses were associated with a reduction in the composite endpoint of VTE reoccurrence, major bleeding, or death at 15 days after adjusting for multiple confounders using multivariable logistic regression (odds ratio, 0.17; 95% CI, 0.04–0.71). This significance was largely driven by unadjusted major bleeding which was significantly higher in the uncapped treatment group [n = 26 (1.1%) vs. n = 0, p = 0.026] while recurrent VTE and death at 15 days were not significantly different between groups [9]. Of note, these data were from the Canadian RIETE registry, and the majority of uncapped patients were treated with enoxaparin (91%) compared to tinzaparin in the capped dose group (55%).
Further safety data can be ascertained from two large registry databases evaluating enoxaparin use in patients with acute coronary syndrome (ACS), the Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with Early Implementation of the American College of Cardiology-American Heart Association Guidelines (CRUSADE) national quality improvement initiative and Pitié-Salpêtrière Registry on Ischemic Coronary Syndromes (PARIS) [6, 8]. Enoxaparin dosing was grouped into recommended dosing (0.95–1.05 mg/kg) versus reduced dosing (< 0.95 mg/kg) to evaluate major bleeding unrelated to CABG in the CRUSADE registry [8]. Patients weighing > 150 kg who received recommended dosing had a higher risk of bleeding compared to those weighing > 150 kg who received a lower dose (adjusted OR 2.42, 95% CI 0.70–8.37). Patients in the PARIS registry were assessed for clinical outcomes associated with three anti-Xa level categories: < 0.5 IU/mL, ≥ 0.5 IU/mL - < 1.2 IU/mL, and ≥ 1.2 IU/mL [6]. Patients in the group with anti-Xa levels < 0.5 IU/mL had increased rates of mortality, death, and major bleeding compared to the other groups however this group also had baseline characteristics associated with poor outcomes including older age, impaired renal function, more ST-segment depression, and higher TIMI risk scores which prompted use of lower doses of enoxaparin accordingly. It is difficult to determine if these poor outcomes were related to baseline characteristics of this group or the anti-Xa level directly, as measures of left ventricular function, older age, and non-Q-wave myocardial infarctions were also associated with these worse outcomes.
The results of our analysis support the RIETE and CRUSADE evaluations. In this systematic review, almost all bleeds occurred in the ≥ 0.95 mg/kg group. Of note, over half of this weight-based dosing group had supratherapeutic anti-Xa levels. Additionally, rates of thrombosis were not increased at lower weight-based doses. This data should be interpreted with caution however as the majority of patients included in this systematic review received full dose (≥ 0.95 mg/kg) enoxaparin making comparisons across dosing groups significantly imbalanced. Both rates of bleeding and thrombosis were low in this systematic review making conclusions harder to draw but when taken into consideration with registry data it would appear that obese patients have higher rates of untoward outcomes when using full weight-based dosing and that a reduced dosing strategy may be more optimal.
Some studies have suggested a most appropriate dose of enoxaparin for patients with obesity based on the dose required to achieve therapeutic anti-Xa levels in the population studied [15,16,17,18, 28]. The first study to define an optimal dose was a case series completed by Deal et al. and determined an ideal dose of 0.74 mg/kg in patients with an average BMI of 49.5 kg/m2 [27]. Subsequent studies have defined optimal doses ranging from 0.70 to 0.81 mg/kg per dose. This variability is likely due to multiple factors. First, it appears that even within a population of obese patients, those with higher BMIs require less drug to achieve similar anti-Xa levels, particularly in patients with a BMI over 50 kg/m2 [16, 18, 21]. Consequently, the study by Thompson-Moore et al. with an average BMI of 46.6 kg/m2 suggests a higher optimal dose around 0.8 mg/kg, but the Lee study determined a lower optimal dose of approximately 0.70 mg/kg in those with a BMI between 50 and 70 kg/m2 [16, 17]. Second, timing of anti-Xa level obtainment impacts the likelihood the drug is at steady state. Obese patients may take longer to reach steady state as a previous pharmacokinetic and pharmacodynamic study found that on visual inspection of concentration/time curves, normal weight patients require two doses of enoxaparin to reach steady state, but obese patients require three [2]. Similarly, the time to max anti-Xa activity (Tmax) was one hour later in obese vs. non-obese patients (4 vs. 3 h, p = 0.005). If drawn too early (i.e. after the second dose) or within a few hours after dose administration, the anti-Xa inhibition may not yet be at maximal, steady state effect, making it appear that higher doses would be required which correlate with studies that assessed levels after the second dose. [17, 18] Therefore, the degree of obesity and timing of anti-Xa level sampling likely account for some of the variation and it is important to consider these factors when selecting an appropriate dose and anti-Xa monitoring strategy.
Based on our results, anti-Xa levels were most optimally distributed in obese patients at a dose of 0.75–0.85 mg/kg, which aligns with the optimal doses reported within the included studies and clinical data. [8, 9, 15,16,17,18, 27] As a pragmatic approach to consolidate dosing strategies, we recommend the following for use with therapeutic enoxaparin dosing: In patients with a BMI over 40 kg/m2 and less than 200 kg, enoxaparin should be dosed at 0.75–0.85 mg/kg twice daily for CrCl ≥ 30 ml/min and daily for non-hemodialysis patients with a CrCl < 30 ml/min. In patients with a BMI ≥ 40 kg/m2 and < 50 kg/m2, the higher end of the dosing range should be used, and in patients with a BMI ≥ 50 kg/m2, the lower end of the dosing range should be used. Anti-Xa levels should be obtained approximately 4 h after at least three doses of enoxaparin to account for the longer time to steady state and Tmax in patients with obesity. As this dosing recommendation is not supported by guidelines and based on limited data, monitoring anti-Xa levels is recommended. Based on a paucity of data, recommendations cannot be made in patients greater than 200 kg.
It is important to note that these recommendations only apply to enoxaparin and not other LMWHs. Based on the variation of factor Xa and IIa inhibition with each of the LMWHs, the anti-Xa levels will not necessarily be the same for therapeutically equivalent doses [28]. In the limited data that exists evaluating dalteparin and tinzaparin in patients with obesity it appears that anti-Xa levels may not be correlated with body weight [29,30,31]. It is possible that dalteparin and tinzaparin behave differently in obese patients and further research with these agents would be needed before dosing recommendations from this systematic review could be extrapolated to dalteparin or tinzaparin use. Additionally, the recommendations cannot be used for patients with renal dysfunction, liver dysfunction, pediatric, or pregnant patients. In patients with renal dysfunction, it is clear that accumulation occurs, and it may be pertinent to be more conservative with dosing and monitoring anti-Xa levels. [32, 33] Furthermore, in patients with cirrhosis the changes in the coagulation cascade may make interpretation of anti-Xa levels variable. [34, 35] Pregnant patients have a different volume of distribution than an obese patient, and there is variation in anti-Xa levels throughout pregnancy [36]. Due to the general lack of data and outcomes in these populations, the current review did not investigate these groups.
Guidance surrounding agent selection for therapeutic anticoagulation tends to favor direct acting oral anticoagulants (DOAC) in most patients over LMWH [11,12,13]. Interestingly, the risk of using non-weight based dosing for DOACs in patients with obesity draws concern for subtherapeutic dosing and potential treatment failure while enoxaparin is concerned with supratherapeutic dosing and bleeding based on differences in volume of distribution. Despite this potential concern, rivaroxaban and apixaban have been studied in patients with obesity and subsequently the ISTH recommends that rivaroxaban, apixaban, vitamin K antagonists, weight-based LMWH, and fondaparinux can be used in patients with a BMI over 40 kg/m2 or weight ≥ 120 kg [37]. Though DOACs are often selected in obese patients, in the cancer population LMWH are still readily used, with over half of this population prescribed LMWH in 2017 [38]. Though this number is likely declining with guidance for DOAC use in this population, accuracy of dosing is still warranted [39].
There are important limitations to consider. While obesity is an important factor to consider when dosing and monitoring enoxaparin, renal function will affect enoxaparin concentrations, likely to an even greater degree [22]. The inclusion criteria for this systematic review was careful to take renal function into consideration and removed studies that included patients with concomitant extremes of renal function and body weight so as to try to remove the confounding factor of renal function from obesity. However, renal function was not documented in every study and when provided it was not translatable across studies (e.g., CrCl calculated with lean vs. actual body weight, eGFR, SCr). It is possible that varied renal function could have affected anti-Xa levels that were used to compute the recommendations in this review. Other variables such as co-morbidities and concomitant medications (e.g., warfarin, antiplatelets) were also minimally documented in these studies. It is possible this could have impacted the individual studies especially with regards to bleeding outcomes.
Most studies included in this systematic review were retrospective with a relatively small number of participants and less patients received adjusted dosing compared to full weight-based dosing. This may have influenced clinical outcomes such as bleeding which appear higher in those who received full weight-based dosing but likely driven by the differences in population size between groups. However, based on the reproducibility of results between studies, with reasonable explanations for variation (levels of BMI, timing of laboratory draws), it is possible to make recommendations from the totality of data. A limitation of note is an omission of a 0.86–0.95 mg/kg group, this was due to minimal data in this dosing range so conclusions cannot be drawn regarding use of this dosage. More data is required to validate the clinical findings associated with anti-Xa levels to confirm the anti-Xa ranges selected as therapeutic, but with the information available, an adjusted dosing regimen in obese patients is reasonable and may decrease bleeding events.
Conclusion
Evidence suggests that more obese patients achieve therapeutic anti-Xa levels with a reduced weight-based therapeutic enoxaparin strategy. As weight and/or BMI increases within the obese category, reduced weight-based dosing may become critical to prevent adverse outcomes. Based on the current evidence, it is reasonable to use a reduced weight-based dose of enoxaparin in obese patients.
References
Sebaaly J, Covert K (2018) Enoxaparin dosing at extremes of weight: literature review and dosing recommendations. Ann Pharmacother 52:898–909. https://doi-org.gate.lib.buffalo.edu/10.1177/1060028018768449
Sanderink GJ, Le Liboux A, Jariwala N, Harding N, Ozoux ML, Shukla U, Montay G, Boutouyrie B, Miro A (2002) The pharmacokinetics and pharmacodynamics of enoxaparin in obese volunteers. Clin Pharmacol Ther 72:308–318. https://doi.org/10.1067/mcp.2002.127114
Package insert : https://www.accessdata.fda.gov/drugsatfda_docs/label/2009/020164s085lbl.pdf
World Health Organization (2023) Obesity and Overweight. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight. Accessed 17 November 2023
Levine MN, Planes A, Hirsh J, Goodyear M, Vochelle N, Gent M (1989) The relationship between anti-factor xa level and clinical outcome in patients receiving enoxaparine low molecular weight heparin to prevent deep vein thrombosis after hip replacement. Thromb Haemost 62:940–944. https://doi.org/10.1055/s-0038-1651032
Montalescot G, Collet JP, Tanguy ML et al (2004) Anti-xa activity relates to survival and efficacy in unselected acute coronary syndrome patients treated with enoxaparin. Circulation 110:392–398. https://doi.org/10.1161/01.CIR.0000136830.65073.C7
Nieuwenhuis HK, Albada J, Banga JD, Sixma JJ (1991) Identification of risk factors for bleeding during treatment of acute venous thromboembolism with heparin or low molecular weight heparin. Blood 78:2337–2343. https://doi.org/10.1182/blood.V78.9.2337.2337
Spinler SA, Ou FS, Roe MT, Gibler WB, Ohman EM, Pollack CV, Alexander KP, Peterson ED (2009) Weight-based dosing of enoxaparin in obese patients with non‐ST‐segment elevation acute coronary syndromes: results from the CRUSADE initiative. Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy 29:631–638. https://doi.org/10.1592/phco.29.6.631
Barba R, Marco J, Martin-Alvarez H, Rondon P, Fernandez‐Capitan C, Garcia‐Bragado F, Monreal M, RIETE investigators (2005) The influence of extreme body weight on clinical outcome of patients with venous thromboembolism: findings from a prospective registry (RIETE). J Thromb Haemost 3:856–862. https://doi.org/10.1111/j.1538-7836.2005.01304.x
Lexicomp, Online, July (2021) 30, https://online.lexi.com
Kearon C, Akl EA, Ornelas J, Blaivas A, Jimenez D, Bounameaux H, Huisman M, King CS, Morris TA, Sood N, Stevens SM (2016) Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. Chest 149:315–352. https://doi.org/10.1016/j.chest.2015.11.026
Stevens SM, Woller SC, Kreuziger LB, Bounameaux H, Doerschug K, Geersing GJ, Huisman MV, Kearon C, King CS, Knighton AJ, Lake E (2021) Antithrombotic therapy for VTE disease: second update of the CHEST guideline and expert panel report. Chest 160:e545–608. https://doi.org/10.1016/j.chest.2021.07.055
Witt DM, Nieuwlaat R, Clark NP, Ansell J, Holbrook A, Skov J, Shehab N, Mock J, Myers T, Dentali F, Crowther MA (2018) American Society of Hematology 2018 guidelines for management of venous thromboembolism: optimal management of anticoagulation therapy. Blood advances. 2018;2:3257-91. https://doi.org/10.1182/bloodadvances.2018022954
Berger O, Sebaaly J, Crawford R, Rector K, Anderson W (2021) Evaluation of a treatment-dose enoxaparin protocol for patients with obesity. J Pharm Pract 36:74–78. https://doi.org/10.1177/08971900211022300
Lalama JT, Feeney ME, Vandiver JW, Beavers KD, Walter LN, McClintic JR (2015) Assessing an enoxaparin dosing protocol in morbidly obese patients. J Thromb Thrombolysis 39. https://doi.org/10.1007/s11239-014-1117-y. :516 – 21
Lee YR, Palmere PJ, Burton CE, Benavides TM (2020) Stratifying therapeutic enoxaparin dose in morbidly obese patients by BMI class: a retrospective cohort study. Clin Drug Investig 40:33–40. https://doi.org/10.1007/s40261-019-00855-9
Maclachlan KH, Stevens HP, Tran HA, Chunilal SD (2019) Weight-based enoxaparin for venous thromboembolism in obesity gives similar anti-xa levels to patients < 100 kg, with no increase in major bleeding. InSeminars in Thrombosis and Hemostasis 45:094–099. https://doi.org/10.1055/s-0038-1677019
Thompson-Moore NR, Wanat MA, Putney DR, Liebl PH, Chandler WL, Muntz JE (2015) Evaluation and pharmacokinetics of treatment dose enoxaparin in hospitalized patients with morbid obesity. Clin Appl Thromb Hemost 21:513–520. https://doi.org/10.1177/1076029614568713
van Oosterom N, Winckel K, Barras M (2019) Evaluation of weight based enoxaparin dosing on anti-xa concentrations in patients with obesity. J Thromb Thrombolysis 48. https://doi.org/10.1007/s11239-019-01847-4. :387 – 93
Lee YR, Vega JA, Duong HN, Ballew A (2015) Monitoring enoxaparin with antifactor xa levels in obese patients. Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy 35:1007–1015. https://doi.org/10.1002/phar.1658
Curry MA, LaFollette JA, Alexander BR, Evans KS, Tran RH, Kempton CL (2019) Evaluation of treatment-dose enoxaparin in acutely ill morbidly obese patients at an academic medical center: a randomized clinical trial. Ann Pharmacother 53. https://doi-org.gate.lib.buffalo.edu/https://doi.org/10.1177/1060028018821149. :567 – 73
Bazinet A, Almanric K, Brunet C, Turcotte I, Martineau J, Caron S, Blais N, Lalonde L (2005) Dose of enoxaparin among obese and renal impairment patients. Thromb Res 116:41–50. https://doi.org/10.1016/j.thromres.2004.10.004
Sacha GL, Greenlee KM, Ketz JM (2016) The use of anti-factor xa monitoring in a selection of patients receiving enoxaparin at a large academic medical center. J Thromb Thrombolysis 42. https://doi.org/10.1007/s11239-016-1384-x. :479 – 85
Khorsand N, Majeed A, Sarode R, Beyer-Westendorf J, Schulman S, Meijer K, Subcommittee on Control of Anticoagulation (2016) Assessment of effectiveness of major bleeding management: proposed definitions for effective hemostasis: communication from the SSC of the ISTH. J Thromb Haemost 14:211–214. https://doi.org/10.1111/jth.13148
Wells GA, Shea B, O’Cnnell D et al (2023) The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. The Ottawa Hospital Research Institute website. Accessed November 16, https://www.ohri.ca//programs/clinical_epidemiology/oxford.asp
Cochrane Methods Bias. RoB 2: a revised Cochrane risk-of-bias tool for randomized trials. Cochrane Methods website. Accessed November 16 (2023) https://methods.cochrane.org/bias/resources/rob-2-revised-cochrane-risk-bias-tool-randomized-trials
Deal EN, Hollands JM, Riney JN, Skrupky LP, Smith JR, Reichley RM (2011) Evaluation of therapeutic anticoagulation with enoxaparin and associated anti-xa monitoring in patients with morbid obesity: a case series. J Thromb Thrombolysis 32:188–194. https://doi.org/10.1007/s11239-011-0584-7
Samama MM, Gerotziafas GT (2000) Comparative pharmacokinetics of LMWHs. InSeminars in Thrombosis and Hemostasis 26:031–038. https://doi.org/10.1055/s-2000-9497
Smith J, Canton M (2003) Weight-based administration of dalteparin in obese patients. Am J Health-Syst Pharm 60:683–687
Wilson JS, Wilbur K, Burton E, Anderson D (2001) Effect of patient weight on the anticoagulant response to adjusted therapeutic dosage of low-molecular weight heparin for the treatment of venous thromboembolism. Haemostasis 31:42–48
Hainer JW, Barrett JS, Assaid CA, Fossler MJ, Cox DS, Leathers T, Leese PT (2002) Dosing in heavy-weight/obese patients with the LMWH, tinzaparin: a pharmacodynamic study. Thromb Haemost 87:817–823
DeCarolis DD, Thorson JG, Clairmont MA, Leuthner AM, Rector TS, Johnson GJ (2012) Enoxaparin outcomes in patients with moderate renal impairment. Arch Intern Med 172:1713–1718. https://doi.org/10.1001/2013.jamainternmed.369
Nagge J, Crowther M, Hirsh J (2002) Is impaired renal function a contraindication to the use of low-molecular-weight heparin? Arch Intern Med 162:2605–2609. https://doi.org/10.1001/archinte.162.22.2605
Ha NB, Regal RE (2016) Anticoagulation in patients with cirrhosis: caught between a rock-liver and a hard place. Ann Pharmacother 50:402–409. https://doi.org/10.1177/1060028016631760
Bechmann LP, Sichau M, Wichert M, Gerken G, Kröger K, Hilgard P (2011) Low-molecular‐weight heparin in patients with advanced cirrhosis. Liver Int 31:75–82. https://doi.org/10.1111/j.1478-3231.2010.02358.x
Friedrich E, Hameed AB (2010) Fluctuations in anti-factor xa levels with therapeutic enoxaparin anticoagulation in pregnancy. J Perinatol 30:253–257. https://doi.org/10.1038/jp.2009.164
Martin KA, Beyer-Westendorf J, Davidson BL, Huisman MV, Sandset PM, Moll S (2021) Use of direct oral anticoagulants in patients with obesity for treatment and prevention of venous thromboembolism: updated communication from the ISTH SSC Subcommittee on Control of Anticoagulation. J Thromb Haemost 19:1874–1882. https://doi.org/10.1111/jth.15358
Delate T, Charlu M, Zhu S, Pai A, Clark NP, Witt DM, King JM, King JB (2020) Temporal trends in first-line outpatient anticoagulation treatment for cancer-associated venous thromboembolism. Thromb Res 196:367–370. https://doi.org/10.1016/j.thromres.2020.09.008
Key NS, Khorana AA, Kuderer NM, Bohlke K, Lee AY, Arcelus JI, Wong SL, Balaban EP, Flowers CR, Gates LE, Kakkar AK (2023) Venous thromboembolism prophylaxis and treatment in patients with cancer: ASCO guideline update. J Clin Oncol 41:3063–3071. https://doi.org/10.1200/JCO.19.01461
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Consent for publication
The authors have no financial or non-financial interests that are directly or indirectly related to the work submitted for publication.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Chilbert, M.R., Zammit, K., Ahmed, U. et al. A systematic review of therapeutic enoxaparin dosing in obesity. J Thromb Thrombolysis 57, 587–597 (2024). https://doi.org/10.1007/s11239-024-02951-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11239-024-02951-w