
Abstract
This study is concerned with evaluating cystic fibrosis (CF) annual review practice. More precisely, we wanted to know if we are utilizing genetic counseling services and identifying poor knowledge of sexual reproductive health at annual review. We conducted short interviews with 21 CF patients at annual review regarding genetic counseling knowledge and perception. Patient responses were documented, analyzed and coded using a simple thematic analysis to précis the content. Immediately post-interview, patients were asked to complete a CF questionnaire comprised of nine questions, testing knowledge of the science of Mendelian genetics, contraceptive needs and fertility. Knowledge was then compared to responses documented at annual review. Emerging themes from interviews included: poor knowledge and a need for more information regarding what genetic counseling involves, a positive perception and experience of genetic counseling for those who had attended, and partner anxiety related to carrier testing. The percentage of patients who reported they were aware of the CF fertility and genetic issues was 95%, however, questionnaire scores ranged from 0 to 9/9 (mean 4.8 SD [2.2]). 57% of patients had received genetic counseling. These patients had a statistically significantly higher score 6.2 (1.5) versus those who had not 2.9 (1.3) p < 0.001. The All Wales Adult CF Centre annual review practice is insufficient to identify patients who may benefit from further education on reproductive health. Traditionally these domains have been granted less significance. However, as life expectancy, quality of life and reproductive assistive techniques improve, ensuring appropriate patient knowledge is of greater importance.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Cystic fibrosis (CF) is an inherited autosomal recessive disorder, which causes malfunction of the cystic fibrosis transmembrane conductance regulator gene, affecting the body’s ability to control movement of salt and water. As a result, CF patients produce thick congestive mucus that disorders function of multiple organ systems, including the lungs, pancreas, liver, bowel and reproductive organs. Bilateral absence of the vas deferens causes infertility in approximately 98% of men. Women with CF have thicker cervical mucus and are more likely to have irregular ovulation, however the majority are fertile. Historically CF was considered a disease of childhood and as such, emphasis was given to lung, pancreatic and gastrointestinal manifestations of the disease, with little in regards to sexual reproductive health [1]. This is no longer the case, and it has been acknowledged with increases in CF life expectancy, sexual reproductive health must be granted greater significance [2].
CF patient demographic continues to shift; United Kingdom median life expectancy is 41 years old and over 60% of patients are more than 16 years old [3]. Despite this, CF sexual reproductive health continues to be insufficiently emphasized in clinical practice and guidelines, and under-represented in research [4]. As a result, poor patient knowledge of sexual reproductive health amongst adolescent and adult patients is consistently reported [5,6,7,8,9,10,11].
With the development of assisted reproductive techniques and novel treatments such as cystic fibrosis transmembrane conductor regulator modulators, an increasing number of patients desire to have children and are becoming pregnant [12]. To aid them in family planning, it is essential patients feel confident accessing genetic counseling and have appropriate knowledge of the reproductive implications of the disease. In addition to general sexual health knowledge, such as practicing safe sex. Genetic counseling is an important domain in CF sexual health, assisting patients to make informed reproductive decisions.
As part of increased efforts to improve knowledge, the All Wales Adult CF Centre (AWACFC) addresses sexual reproductive health formally in the CF annual review. The primary aim of the study is to evaluate annual review practice, with a secondary aim of identifying poor sexual reproductive health knowledge. More precisely, we wanted to know if we are utilizing genetic counseling services and identifying poor knowledge of genetic counseling, genetics and reproduction at annual review. Although there are many studies that have reported on patient knowledge of sexual reproductive health, few have included genetic counseling.
Methods
Utilization of Genetic Counseling
The AWACFC registry was searched to determine the number of patients in the service with children. The online and paper medical records of these patients were then retrospectively reviewed for evidence of genetic counseling attendance, including referral letters and correspondence with the service. Patient demographics including age, sex and dates of attendance were documented. Genetic counseling attendance dates were compared with child’s birth date.
Semi-Structured Interviews
Information on patient knowledge of genetic counseling was obtained by conducting short, semi-structured interviews with CF patients between September and December 2017. All AWACFC patients attending for their annual review in this period were eligible for inclusion. Baseline patient demographics were noted, however all patient identifiable data was anonymized. Interviews were conducted after the annual review clinic, once informed consent had been obtained. The information to discuss was reviewed by six members of the AWACFC, including physicians and nurse practitioners, and is shown in Table 1.
Patient responses were documented in writing at the time of discussion. Interview notes were transcribed to an electronic format and analyzed by the author. A content analysis method was employed. Patient interview responses were condensed, coded into descriptive labels of the condensed text, and organised into themes, of which five emerged.
Sexual Reproductive Health Questionnaire
Immediately post-interview patients were asked to complete a questionnaire testing their understanding of CF genetics and reproduction. The relevant section of a validated questionnaire developed by the CF team at St. Vincent’s University Hospital was employed [7]. The questionnaire comprised nine fixed-response questions detailing the science of Mendelian genetics, contraceptive needs and fertility.
Questions were marked with 1 for correct and 0 for incorrect. Results were inputted to Microsoft Excel 2011 version 14.1.0 and imported to Statistical Package for Social Sciences (SPSS for Windows, version 23) for statistical analysis. Descriptive statistics were used to summarize demographic and qualitative information. Two independent samples t test was used to calculate significance of mean score to participant characteristics. Differences were considered statistically significant if p < 0.05 (two-tailed).
Comparison with Annual Review
A specialist nurse practitioner collects the annual review sexual reproductive health data. Patient response to the series of questions shown in Table 2 is documented, initially on a written paper copy, then to a digital format by the medical secretaries and submitted to the patient’s online medical record. The full written paper copy is filed into the patient’s paper medical notes. The data recorded in the sexual reproductive health section of the written and typed annual review of all patients interviewed was compared to patients assessed knowledge of genetic counseling, genetics and reproduction from short interviews and the validated questionnaire.
Results
Utilization of Genetic Counseling
A total of 57 patients in the AWACFC have children, 50 (88%) have documented attendance at genetic counseling; 41 attended prior to having children and nine afterwards, all of which were female. Of the seven who did not attend, three were male, all late diagnoses. No reason was identified for the four females who did not attend (Table 3).
Knowledge of Genetic Counseling
We approached 21 patients for interview after annual review, all patients chose to participate. Eight patients were female, 13 male. The age range was 18–55 (mean 30.9 SD [9.1] years).
Table 4 illustrates participant’s characteristics.
Five themes emerged from the interviews;
Poor Knowledge of Genetic Counseling
Of the 21 patients, 12 were unable to answer questions about genetic counseling, including; what it is, what to expect at a session, or how to access the service. Three patients confused genetic counseling with psychological counseling services, and one patient thought it was a fertility test. Nine were aware of genetic counseling; all of these patients had attended genetic counseling previously. After prompting, a further three patients were able to recall having attended genetic counseling, although their knowledge and recall of the experience was limited.
Positive Perception of Genetic Counseling
Genetic counseling was thought to be important to allow for informed reproductive decisions by 20 of the 21 patients. Five patients highlighted the importance of discussing genetics with their children in the future and 17 patients reported they wanted to be fully informed of their options, including carrier testing. Three patients stated carrier testing was irrelevant, as they would have a child despite the risk. No patients expressed any worries or concerns about having genetic counseling themselves, however four patients reported their partners were anxious about carrier testing and the genetic counseling process.
Good Patient Experience of Genetic Counseling
Patients who attended genetic counseling described the experience as positive, responses included that it helped them to understand the risks of having a child with CF and what to do if their partner was a carrier. They stated it was positive for their partners to help them understand about CF and discuss their concerns. It also empowered patients to feel confident discussing the process with friends and family. No patients reported the experience as stressful or worrying.
Discussion with Family
A total of 12 patients had discussed genetic counseling with their family. Seven of these patients were female. Three patients, all of who were male did not think it was important to discuss genetic counseling with other family members. All, but two patients were unaware of whether family members had been for carrier testing, no patients conveyed concerns regarding family members being tested.
Need for More Information
Eight patients said they had never been offered genetic counseling or received any information about it. Patients who had attended for genetic counseling reported they were ill informed on what to expect at a session. The majority of patients conveyed leaflets and social media as useful resources for receiving information, and said they were useful to gain information about sensitive issues before discussing them in person. Three female patients said they had visited online forums for information and five patients enjoyed reading information that included ‘real life’ stories.
Knowledge of CF Genetics and Reproduction
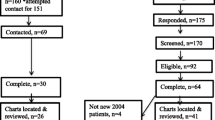
Knowledge scores ranged from 0 to 9/9 (mean 4.8 (53%) SD [2.2]). Only 14% of patients scored 5/5 in Mendelian genetics. Whilst 71% knew the chance of having a child with CF was one in four if both parents were carriers, only 38% knew the chance was one in two if one parent has CF and the other is a carrier. Only 48% were able to correctly identify whether CF affects female fertility and disease prevalence, 66% recognized how CF affects male fertility and that contraception is necessary.
Questionnaire scores are displayed in Table 5, score frequency and distribution is shown as a graph in Fig. 1.

Distribution of CF knowledge scores
The 12 patients who had received genetic counseling had a statistically significantly higher score 6.2 (1.5) vs those who had not 2.9 (1.3) p < 0.001. There was no statistically significant knowledge difference between those who had children 5.5 (1.8) and those without 4.5 (2.3) or between male and female scores in all of the above.
Results from Annual Review
Twenty of the patient’s online annual review reproductive section simply stated—they were “fully aware of the genetic and fertility issues in CF”. The paper written copy listed specific answers to annual review questions, the results of which are shown in Table 6.
The percentage of patients who reported they were aware of the CF fertility and genetic issues was 95%. The single patient who was not reported to be aware of CF fertility/genetic issues was an 18-year-old male with mild learning difficulties, who it had been documented, did not understand due to this. The number who reported they were using contraception was 71%, including; barrier contraceptives and hormonal contraceptives. A further 71% reported they were thinking about conceiving children, 57% had previously attended for genetic counseling and a further 10% stated they would like genetic counseling in the future.
Discussion
The AWACFC annual review practice is insufficient to identify patients who may benefit from further education on reproductive health. Whilst 95% of patients reported they were “fully aware of the genetics and fertility issues in CF” at their annual review, this does not correlate with questionnaire and interview results. Mean knowledge scores from a validated questionnaire were just 53%. Our patients lacked knowledge in all aspects of fertility and genetics. Only 66% of patients recognized the need for contraception and the affect of CF on male fertility, with even fewer understanding female fertility and CF genetics. Whilst poor knowledge is not unique to our centre; It is worrying as our patients appear to lack the knowledge needed to make informed sexual reproductive health decisions, which we are not identifying.
The annual review addresses and gives patients an opportunity to ask for genetic counseling, however, we are not fulfilling their knowledge needs. Interview data reports patients are ill informed on genetic counseling. They do not understand what it is, or what to expect at a session. Yet, once given more information patients were able to recognise the importance and role. Those who attended reported it to be a positive and informative process, supporting the evidence that genetic counseling is a valuable education resource, and has an integral role in assisting patients and their partners to make informed reproductive decisions [13]. In addition to this, it was the only factor amongst those analyzed, including age, sex and child bearing status, which was statistically significant in terms of greater sexual reproductive knowledge.
Despite poor genetic counseling knowledge, patients are utilizing the service for pre-conceptual counseling, with high attendance rates reported, 88% of those with children attended genetic counseling, 82% prior to conception. However, there is a clear need to provide more written and verbal information to patients prior to attendance. Counseling sessions are more effective in patients who are well educated and open to new ideas [13].
This was a small study of patients attending for annual review, which focused specifically on the process in the AWACFC. This may lead to issues of generalizability, as other CF centres employ different annual review processes. Data was collected over a 4-month period and only included patients attending for annual review. Those who did not attend for annual review during the period of study had no chance for participation. Patients attending for annual review are more likely to be physically well and engaged with the CF centre, therefore our sample may not be representative of the CF population, leading to over or underestimations in our findings.
This study identifies that annual review practice over-estimates patient knowledge. Ensuring we have a reliable review system in place is essential for good CF care, as 71% of the study sample reported they were thinking about having children. Our sexual reproductive health annual review system is misleading as it relies on patient’s to report their knowledge, rather than a frank and open discussion between patient and health care provider. In addition, we are not utilizing the information documented at annual review; the information recorded is inadequately documented in the online medical record, the most widely accessible information platform.
Patients are often reluctant to admit when they do not understand, or may have mismatched beliefs with health care providers on their understanding of being “fully informed”. Likewise, there are barriers to such discussions including patient and health care provider embarrassment, insufficient time, and training to deal with sensitive sexual reproductive health issues [14,15,16]. We must strive to ensure all patients receive sexual reproductive health education and adapt to our patients needs, learning difficulties for example should not be a barrier to discussions.
Annual reviews are an important method of measuring education targets, however they must be used in accordance with regular sexual reproductive discussions throughout the year [17]. There is no standardized annual review protocol in CF care; therefore it would be beneficial to reproduce this study in another centre to confirm the applicability of these results and investigate which annual review processes most accurately estimate patient sexual reproductive health knowledge. The cystic fibrosis team plays a huge role in ensuring sexual reproductive health care and are preferred point of contact for CF patients to discuss these issues with [15]. We need to be able to identify poor knowledge, overcome barriers to discussions, and continue encouraging the use of genetic counseling services, perhaps then we will see improvements in the sexual reproductive knowledge of CF patients.
References
Davis, P.B., Drumm, M., Konstan, M.W.: Cystic fibrosis. Am. J. Respir. Crit. Care Med. 154, 1229–1256 (1996)
Ahmad, A., Ahmed, A., Patrizio, P.: Cystic fibrosis and fertility. Curr. Opin. Obstet. Gynecol. 25, 167–172 (2013)
UK Cystic Fibrosis Registry 2016 Annual Data Report. Cystic Fibrosis Trust 2017
Heltshe, S.L., Taylor-Cousar, J.L.: Let’s talk about sex: behaviors, experience and health care utilization in young women with CF. J. Cyst. Fibros. (2017). https://doi.org/10.1016/j.jcf.2017.11.006
Sawyer, S.M., Farrant, B., Cerritelli, B., Wilson, J.: A survey of sexual and reproductive health in men with cystic fibrosis: new challenges for adolescent and adult services. Thorax 60, 326–330 (2005)
Rodgers, H.C., Baldwin, D.R., Knox, A.J.: Questionnaire survey of male infertility in cystic fibrosis. Respir. Med. 94, 1002–1003 (2000)
Siklosi, K.R., et al.: Development, validation, and implementation of a questionnaire assessing disease knowledge and understanding in adult cystic fibrosis patients. J. Cyst. Fibros. 9, 400–405 (2010)
Korzeniewska, A., Grzelewski, T., Jerzynska, J., Majak, P., Soloniewicz, A., Stelmach, W., et al.: Sexual and reproductive health knowledge in cystic fibrosis female patients and their parents. J. Sex. Med. 6(3), 770–776 (2009)
Conway, S.P., Pond, M.N., Watson, A., Hamnett, T.: Knowledge of adult patients with cystic fibrosis about their illness. Thorax 51, 34–38 (1996)
Madge, S.L., Carr, S.B.: Reproductive health in males with cystic fibrosis: knowledge, attitudes, and experience of patients and parents. Pediatr. Pulmonol. 27, 293 (1999)
Sawyer, S.M., Tully, M.A., Dovey, M.E., Colin, A.A.: Reproductive health in males with cystic fibrosis: knowledge, attitudes, and experiences of patients and parents. Pediatr. Pulmonol. 25, 226–230 (1998)
Heltshe, S.L., Godfrey, E.M., Josephy, T., et al.: Pregnancy among cystic fibrosis women in the era of CFTR modulators. J. Cyst. Fibros. 16(6), 687–694 (2017)
Dodge, J.A., Burton, L., Cull, A., McCrae, W.M.: Effectiveness of counselling in cystic fibrosis. Patient Couns. Health Educ. 1, 8–12 (1978)
Kazmerski, T.M., Sawicki, G.S., et al.: Sexual and reproductive health behaviors and experiences reported by young women with cystic fibrosis. J. Cyst. Fibros. 14, 57–60 (2018)
Kazmerski, T.M., Sawicki, G.S., et al.: Sexual and reproductive health care utilization and preferences reported by young women with cystic fibrosis. J. Cyst. Fibros. 17, 64–70 (2018)
Kazmerski, T.M., Borrero, S., Tuchman, L.K., Weiner, D.J., Pilewski, J.M., Orenstein, D.M., et al.: Provider and patient attitudes regarding sexual health in young women with cystic fibrosis. Pediatrics (2016). https://doi.org/10.1542/peds.2015-4452
Frayman, K.B., Sawyer, S.M.: Sexual and reproductive health in cystic fibrosis: a life-course perspective. Lancet Respir. Med. 3, 70–86 (2015)
Acknowledgements
Thank you to all the members of staff at the All Wales Adult Cystic Fibrosis Unit.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Wilson, C., Duckers, J., Speight, L. et al. Assessment of Sexual Reproductive Health Knowledge Amongst Patients with Cystic Fibrosis. Sex Disabil 37, 15–23 (2019). https://doi.org/10.1007/s11195-019-09558-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11195-019-09558-7