
Abstract
Purpose
To review the literature on health-related quality of life (HRQoL) outcomes for exercise-based cardiac rehabilitation (EBCR) in contemporary acute coronary syndrome (ACS) patients.
Methods
Electronic databases (CENTRAL, MEDLINE, Embase, and CINAHL) were searched from January 2000 to March 2019 for randomised controlled trials (RCTs) comparing EBCR to a no-exercise control in ACS patients recruited after year 2000, follow-up of at least 6 months, and HRQoL as outcome. Potential papers were independently screened by two reviewers. Risks of bias were assessed using the Cochrane Tool. Data analyses were performed using RevMan v5.3, random effects model.
Results
Fourteen RCTs (1739 participants) were included, with eight studies suitable for meta-analyses. EBCR resulted in statistically significant and clinically important improvements in physical performance (mean difference [MD] 7.09, 95% CI 0.08, 14.11) and general health (MD 5.08, 95% CI 1.03, 9.13) (SF-36) at 6 months, and in physical functioning (MD 9.82, 95% CI 1.46, 18.19) at 12 months. Statistically significant and sustained improvements were also found in social and physical functioning. Meta-analysis of two studies using the MacNew Heart Disease HRQoL instrument did not show any significant benefits. Of the six studies unsuitable for meta-analyses, five reported significant changes in overall HRQoL, general physical activity levels and functional capacity, or quality-adjusted life-years (QALYs).
Conclusions
In an era where adherence to clinical practice guidelines has improved survival, EBCR still achieves clinically meaningful improvements in physical performance, general health, and physical functioning in the short and long term in contemporary ACS patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Acute coronary syndrome (ACS) is the leading contributor to overall cardiovascular disease (CVD) burden globally [1], resulting in 18 million deaths in 2016 [1, 2] and projected to exceed 23 million by 2030 [3, 4]. Disease reoccurrence is also extremely common as 40% of ACS survivors are readmitted to hospital within 30 days of discharge [5] and 20% experience a repeat cardiac event within the first year [6]. Although there have been reductions in mortality from CVD in recent decades due to the availability and accessibility of life-saving cardiac interventions and guideline-based medications, this rate of decline is slowing, thus many more people live with CVD and related disability.
Lower health-related quality of life (HRQoL) is often experienced post cardiac event [7]. Persistent symptoms, both physical (e.g. pain and fatigue) and psychological (e.g. depression and anxiety), decrease patients’ perceived level of personal competence and their ability to perform usual activities [8,9,10]. When compared to the general population, ACS survivors are shown to be 2.7 times more likely to report fair/poor general health and 1.5 times more likely to state limitations to daily activities [11]. Therefore, more comprehensive interventions aimed at improving patients’ physical functioning, reducing physical limitations, and regaining previous abilities are needed.
Cardiac rehabilitation (CR) aims to improve multiple aspects of a patient’s life and includes several interventions such as supervised exercise, smoking cessation counselling, medication education, and stress reduction strategies. CR is defined by the World Health Organization (WHO) as “the sum of activities required to ensure them [patients] the best possible physical, mental and social conditions, so that they may, by their own efforts, resume and maintain as normal a place as possible in the community” [12]. Exercise-based cardiac rehabilitation (EBCR) is the most widely recognised CR strategy [13] because of known dose–response benefit for mortality from all causes including CVD [14, 15], and a strong potential to improve HRQoL [16]. EBCR is consistently and strongly recommended in international clinical practice guidelines, particularly for ACS [17,18,19,20,21].
Previous reviews evaluating the effectiveness of EBCR [22,23,24] including the latest Cochrane review [24] focused on clinical endpoints such as mortality, morbidity, and hospital readmission. The most recent of these reviews, which examined only contemporary trials (since 2000) reported a lack of benefits for mortality and hospital readmissions [22]. These reviews referred to improvements in HRQoL but failed to conduct the meta-analyses needed to form robust conclusions. One review conducted a thematic analysis on HRQoL outcomes reported that HRQoL improvements have a bidirectional relationship with increased physical activity [25]. Another recently published meta-analysis of HRQoL outcomes [26] concluded that CR results in modest benefits with greater improvements from non-exercise-based and psychological interventions, which seems counterintuitive. These findings contradict the results of two recently updated Cochrane reviews, which found no consistent evidence of superior HRQoL following patient education [27] and considerable uncertainty around the effects of psychological interventions [28]. One criticism of this meta-analysis is that older trials were included, which may not reflect the impact of contemporary therapies for ACS. Therefore, the impact of EBCR on patient-reported outcome measures (PROMs) such as HRQoL considering medical progress in this evolving patient group remains poorly understood.
Clinicians and policymakers need to be guided by robust evidence to decide on appropriate patient interventions with reference to endpoints that matter to patients with ACS. PROMs provide more individualised perspectives on patient-valued outcomes [29] and offer opportunities to measure health benefits of interventions beyond survival, disease, and physiological markers [30, 31]. Therefore, this review aimed to synthesise available evidence and evaluate the HRQoL benefits of EBCR in ACS patients who were treated based on latest guideline recommendations and were recruited from year 2000.
Methods
This systematic review and meta-analysis was performed following a protocol registered in PROSPERO (ID: CRD42018109816). All reporting is in accordance with the Cochrane collaboration [32] and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [33].
Data sources and searches
We used Boolean search methods combining keywords (cardiac rehabilitation AND exercise) AND quality of life AND ‘acute coronary syndrome’ OR ‘myocardial infarction’ OR ‘angina’ AND ‘trial’. To identify relevant papers, one author (DC) searched four electronic databases including Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, and Embase via OvidSP and CINAHL via EBSCO (Supplementary Table).
Two reviewers (DC and RG) independently screened titles and abstracts. Full-text publications of potentially relevant papers were assessed for eligibility based on prespecified criteria. Any differences in decisions were resolved by other reviewers (SR, LL). We also examined the reference lists of included papers, publications with the first or last authors, and sought full-text articles that may have come out from conference abstracts, and consulted previous systematic reviews with similar aims to this review [22, 24, 25, 34] to ensure a comprehensive search.
Study selection
We included published randomised controlled trials (RCTs) comparing EBCR to a no-exercise control with HRQoL as outcome assessed using a validated instrument, and a follow-up of at least 6 months. Studies that compared traditional EBCR to alternative exercise CR modalities such as yoga, tai chi, and other similar routines were excluded. Only those trials reported in English were included, unless a translated version was readily available.
Interventions
EBCR is delivered supervised or unsupervised, either in isolation or as part of a comprehensive program that may include some form of educational and/or psychosocial support [12, 24]. Standard care is defined in this review as usual medical care and follow-up mainly focused on pharmacologic therapy and may include advice or informal education on exercise, psychosocial support, and diet, but does not involve a structured exercise component.
Participants
To ensure representation of a population that would have received contemporary treatments, we included adult participants who have had ACS (where ≥ 80% of total study population had acute myocardial infarction [AMI] with or without revascularisation such as PCI or CABG), angina pectoris, or CAD confirmed by angiography; on optimum secondary preventative medical therapy according to the recommendations of the Sixth Joint Task Force [21]; and recruited after the year 2000 (following the methods of a recently published systematic review) [22].
Risk of bias assessment
We utilised the Cochrane Risk of Bias Assessment Tool [35] (Supplementary Table), specifically designed for RCTs, which assesses selection, performance, detection, attrition, and reporting biases. Three further quality characteristics were included in the assessment (groups balanced at baseline, intention-to-treat analysis, and groups that received comparable treatment except for the intervention) in accordance with the 2016 Cochrane review [24]. One reviewer (DC) critically appraised the risks of bias of included studies and a second reviewer (RG) independently reviewed all assessments. Any inconsistencies were resolved by discussion or by consensus meeting (SR, LL).
Data extraction
Data from included studies were extracted and entered into an electronic spreadsheet. There was substantial variation in the quality of data reporting in studies included in the meta-analyses. We contacted the original authors [36,37,38,39,40,41] for data not reported in the papers. However, necessary statistical information such as standard deviations (SDs) that could not be supplied by the original researchers were imputed for meta-analysis with the guidance of a statistician. Methods employed to estimate missing SDs [42, 43] were (a) using the Cochrane SD spreadsheet, (b) manual computation for SD using the upper and lower limits of the confidence intervals (CIs), and (c) using the t test table. Where data on individual domains were not reported at all [41] or when SDs were too impracticable to be statistically estimated robustly [40, 44], the specific HRQoL domains of these studies were excluded from the meta-analyses.
Data synthesis and analysis
Where meta-analysis was possible, data were combined for statistical analyses using Review Manager v5.3, random effects model. Statistical heterogeneity of included studies was assessed using the χ2 test and the I2 statistic. Data were presented as mean differences (MD) with 95% confidence interval (CI) and statistical significance at p value ≤ 0.05. Furthermore, data were interpreted using the published minimal clinically important differences (CID) standards in health status for patients with heart disease [45]. These standards were developed using state changes, which represent the smallest amount that an individual’s score can shift by moving up or down one response choice [45]. CID values for the Short Form-36 Health Survey (SF-36) vary according to domain (5 for physical functioning, general health, and mental health; 6.25 for physical performance and vitality; 8.33 for emotional performance; 10 for bodily pain; and 12.5 for social functioning) [45]. For the MacNew Questionnaire (MacNew), the published CID value is 0.5 [46]. A sensitivity analysis was also conducted to examine the robustness of the study findings (difference MD ranged from − 1.53 to 2.74 for each domain). Potential for publication bias was assessed using Egger’s test and funnel plots were constructed to visualise possible asymmetry [47] (Supplementary Figure). Where meta-analysis was not appropriate, the results have been analysed and reported descriptively.
Results
Study selection and characteristics
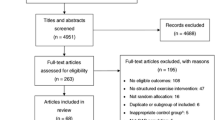
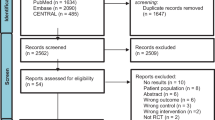
Initial electronic search yielded 2442 references, of which 1288 were screened after duplicate removal and 55 full-text articles were assessed for eligibility based on the prespecified criteria. Ultimately, 14 RCTs (Table 1) were included in the systematic review (1739 participants) and eight of these were suitable for meta-analyses (Fig. 1). Five studies were included in the meta-analysis for the SF-36 at 6-month follow-up [36, 37, 40, 44, 48], two for SF-36 at 12 months [44, 49], and two for the MacNew at 6 months [50, 51]. One study was included in meta-analyses for SF-36 for both 6 and 12 months [44].

Preferred reporting items for systematic reviews and meta-analyses flow diagram
The mean age of participants in individual studies ranged from 56 to 77 years, 81.1% were males, with two studies including males exclusively [40, 41]. Included studies were conducted in Europe (n = 6) [38, 39, 49, 50, 52, 53], Canada (n = 2) [51, 54], and one each in Australia [44], China [48], Hong Kong [37], Japan [40], New Zealand [36], and Saudi Arabia [41].
HRQoL assessment instruments
All HRQoL instruments used in the included trials were validated for the ACS patient population. The most commonly used generic HRQoL instrument was the SF-36 or its condensed version, SF-12 (n = 8) [36,37,38, 40, 41, 44, 48, 49], followed by EQ-5D (n = 3) [36, 39, 52], and 15D (n = 1) [53]. Cardiac disease-specific instruments were also used such as the MacNew (n = 2) [50, 51], Myocardial Infarction Dimensional Assessment Scale (MIDAS) [48], and the Quality of Life Index (QOLI)—cardiac version III [54]. Two studies used multiple HRQoL instruments [36, 48].
Interventions
Centre-based with supervised exercise sessions was the most common mode of EBCR delivery (n = 6) [37, 39, 40, 44, 49, 52], followed by home-based with telephone or face-to-face follow-up (n = 3) [38, 48, 54], home-based with technology- or web-based intervention (n = 3) [36, 50, 51], and a blended centre- and home-based model (n = 2) [41, 53]. EBCR was typically offered with education and psychosocial group sessions including behavioural and lifestyle modification. While there was variation in CR programs, the most common structure was a 6- to 12-week program, with 60 min of supervised exercise, delivered three times a week. Telephone or email support was also available for those involving technological interventions.
Effect on HRQoL
The meta-analysis of five studies [36, 37, 40, 44, 48] that used SF-36 at 6-month follow-up (Fig. 2) showed that EBCR significantly increased physical performance (n = 555, MD 7.09, 95% CI 0.08, 14.11), general health (n = 702, MD 5.08, 95% CI 1.03, 9.13), social functioning (n = 664, MD 4.42, 95% CI 0.35, 8.50), physical functioning (n = 664, MD 4.29, 95% CI 0.98, 7.59), and mental health (n = 702, MD 3.04, 95% CI 0.17, 5.92), with physical performance and general health improvements both statistically significant and clinically important. Statistical heterogeneity across these studies was high (I2 = 4 to 84%).

SF-36 domains at 6 months
In the two studies [44, 49] that used SF-36 at 12 months (Fig. 3), EBCR showed both statistically significant and clinically important improvements in physical functioning (MD 9.82, 95% CI 1.46, 18.19) and statistically significant benefits in bodily pain (MD 8.54, 95% CI 01.34, 15.75) and social functioning (MD 7.07, 95% CI 0.35, 13.79). There was moderate evidence of statistical heterogeneity between these studies (I2 = 0 to 71%).

SF-36 domains at 12 months
Two studies [50, 51] that used MacNew at 6 months (n = 216) also qualified for a meta-analysis (Supplementary Figure) but showed no statistically significant nor clinically important difference between groups was observed across the four HRQoL domains. There was low statistical heterogeneity between these studies (I2 = 0 to 33%).
Six studies were unsuitable to be included in the meta-analyses because there was no consistent instrument used [39, 52,53,54] or necessary statistics such as SDs for individual domains were not available [38, 41]. Of these, five studies individually showed statistically significant improvements from EBCR, either in overall HRQoL (p < 0.05) [41, 52, 54], general physical activity levels and functional capacity (p < 0.05) [39, 52, 54], or quality-adjusted-life-years (QALYs) (average change + 0.013) [53].
Risk of bias assessment
The overall risk of bias of the included studies was low based on the Cochrane Risk of Bias Assessment Tool (Fig. 4). Studies that failed to report enough detail to be accurately assessed were given an unclear score. All studies showed balanced baseline characteristics. However, three studies [37, 40, 51] had interventions other than EBCR delivered unequally across intervention and control groups. The risk for reporting bias was low for all of the studies except one [38], which did not report exercise capacity outcomes at other follow-up periods. Four studies [37, 41, 51, 54] had high potential for attrition bias, while three studies [37, 40, 41] did not conduct intention-to-treat analysis. Detection bias was judged as unclear for six studies [37, 38, 40, 41, 53, 54] and high for four [44, 48,49,50]. For selection bias, eight studies [37, 40, 41, 48, 49, 52,53,54] had unclear score for allocation concealment and six [37, 40, 41, 49, 52, 53] for random sequence allocation. There was also low evidence of publication bias as shown in the funnel plots (Supplementary Table).

Risk of bias assessment
Discussion
In this systematic review and meta-analysis, we report that in the context of current optimal medical therapy, clinically important improvements from EBCR are still achieved in physical performance and general health, as well as physical functioning in the long term. Significant and sustained benefits are also observed in physical and social functioning, with the addition of short-term gains for mental health and long-term reductions in bodily pain. These findings support and complement previous reviews without meta-analyses that showed overall HRQoL benefits from EBCR [22, 24, 25] and, particularly, improvements in physical activity [25]. However, contrary to the only meta-analysis that showed minimal improvements from exercise [26], our meta-analyses found not only statistically significant but also clinically meaningful differences between groups in physical performance and general health, as well as physical functioning—the domains that are known to be impacted most by ACS diagnosis [11]. Combining RCTs that used the same instruments in assessing HRQoL made it possible to pool data into a meta-analysis and quantify the differences between groups.
EBCR is a complex intervention and health benefits may be occurring as a result of the combined effect or interplay of different components. However, the main intervention used in EBCR is exercise due to the well-acknowledged health benefits in the literature such as decreased mortality and risk factors associated with most chronic diseases, including CVD [55]. Participation in exercise activities improves physical function and exercise tolerance, especially if the exercises were tailored to individual needs and capacity [55, 56]. These improvements in physical function are also more likely translated to increased performance of daily activities that are easily recognised and felt by patients. It is therefore not surprising to observe improvements in physical performance as well as general health from EBCR. In addition, effects of exercise in physical functioning are not simply sustained but also found to be more meaningful in the long term. It is further suggested that health benefits from exercise may not only be explained by way of increased physical activity, but also possibly by cellular or molecular mechanisms [57].
Social functioning benefits from EBCR proved substantial and were sustained over time. These improvements are potentially associated with physical gains, which enable patients to be more confident participating in social activities [58]. The inherent presence of social contact in EBCR from both staff and other participants in CR programs may also have been beneficial not just in social functioning but also in mental health. Regular social support from CR staff that kept patients socially engaged was identified as a contributor to the effectiveness of CR that extends to the post-discharge period [59]. Furthermore, peer support through multiple modes of interaction between people experiencing the same challenges from a life-changing event such as ACS have been shown to positively affect psychosocial health outcomes [60].
The meta-analyses in this review included both a generic (SF-36) and a cardiac disease-specific HRQoL questionnaire (MacNew), reflecting the recommendation of the American Heart Association (AHA) [61]. However, when cardiac-specific data for the MacNew was pooled, no difference in any domain was detected between groups, despite individual studies [50, 51] reporting improvements in some domains. This result is contrary to a previous meta-analysis that included a wide range of interventions [26], which showed statistical improvement in all MacNew domains. Failure to detect significant change with the MacNew in our study could be a consequence of ceiling effect [62] as both studies had samples with high scores at baseline and the distribution of statistical power when combining data [63].
Limitations
While we have run a systematic and thorough database search and examined the reference lists of previews reviews and included papers, as well as papers published by the first and last authors for comprehensiveness, one limitation of this review is the possibility that some studies that used terms other than health-related quality of life but were still relevant and utilised a validated instrument may have been missed. Another limitation is the small number of eligible studies for meta-analysis due to the differences in instruments used. Excluding papers reported in languages other than English may also have narrowed the scope of this review. There was substantial contextual variability between studies in terms of income level of countries where the studies were conducted. While differences in the quality of data reporting was mitigated by contacting the authors for information needed and by estimating data using available statistical techniques, some studies were still excluded from meta-analyses due to incomplete data reporting. Meta-regression analysis was also not conducted due to the inconsistent reporting of variables within individual studies.
Conclusions and recommendation
We report that EBCR imparts clinically important differences to HRQoL, particularly physical performance and general health (short term) and physical functioning (long term) in patients with ACS even in the current era of optimised cardiac care. This review reinforces the importance of evaluating CR benefits beyond mortality and morbidity to consider patient-valued outcomes, such as HRQoL. Understanding the effects of EBCR in patient-reported outcomes offers guidance for clinicians and program coordinators to provide care and evaluate interventions using more person-centred approaches. We recommend that PROMs be given due recognition as a valuable endpoint, with the specific inclusion of HRQoL as one PROM in routine assessments in ACS patients attending CR.
References
Roth, G. A., Johnson, C., Abajobir, A., Abd-Allah, F., Abera, S. F., Abyu, G., et al. (2017). Global, regional, and national burden of cardiovascular diseases for 10 causes, 1990 to 2015. Journal of the American College of Cardiology,70(1), 1–25. https://doi.org/10.1016/j.jacc.2017.04.052.
Murray, C. J. L. (2017). Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: A systematic analysis for the Global Burden of Disease Study 2016. The Lancet,390, 1151–1210. https://doi.org/10.1016/S0140-6736(17)32152-9.
Laslett, L. J., Alagona, P., Jr., Clark, B. A. I., Drozda, J. P., Jr., Saldivar, F., Wilson, S. R., et al. (2012). The worldwide environment of cardiovascular disease: Prevalence, diagnosis, therapy, and policy issues: A report from the American College of Cardiology. Journal of the American College of Cardiology,60(25 Suppl), S1–S49. https://doi.org/10.1016/j.jacc.2012.11.002.
World Health Organization. (2017). Cardiovascular diseases (CVDs) Fact Sheet.
Sangu, P. V., Ranasinghe, I., Aliprandi Costa, B., Devlin, G., Elliot, J., Lefkovitz, J., et al. (2012). Trends and predictors of rehospitalisation following an acute coronary syndrome: Report from the Australian and New Zealand population of the Global Registry of Acute Coronary Events (GRACE). Heart,98(23), 1728–1731. https://doi.org/10.1136/heartjnl-2012-302532.
Jernberg, T., Hasvold, P., Henriksson, M., Hjelm, H., Thuresson, M., & Janzon, M. (2015). Cardiovascular risk in post-myocardial infarction patients: Nationwide real world data demonstrate the importance of a long-term perspective. European Heart Journal,36(19), 1163–1170. https://doi.org/10.1093/eurheartj/ehu505.
Foxwell, R., Morley, C., & Frizelle, D. (2013). Illness perceptions, mood and quality of life: A systematic review of coronary heart disease patients. Journal of Psychosomatic Research,75(3), 211–222. https://doi.org/10.1016/j.jpsychores.2013.05.003.
Waltz, M., & Badura, B. (1988). Subjective health, intimacy, and perceived self-efficacy after heart attack: Predicting life quality five years afterwards. Social Indicators Research,20, 303–332.
Kawecka-Jaszcz, K., Klocek, M., Tobiasz-Adamczyk, B., & Bulpitt, C. J. (2013). Health-related quality of life in cardiovascular patients. Milan: Springer.
Dickens, C. C., McGowan, L., Percival, C., Tomenson, B., Cotter, L., Heagerty, A., et al. (2006). Contribution of depression and anxiety to impaired health-related quality of life following first myocardial infarction. British Journal of Psychiatry,189, 367–372. https://doi.org/10.1192/bjp.bp.105.018234.
Mollon, L., & Bhattacharjee, S. (2017). Health related quality of life among myocardial infarction survivors in the United States: A propensity score matched analysis. Health and Quality of Life Outcomes,15(1), 235. https://doi.org/10.1186/s12955-017-0809-3.
World Health Organization. (1993). Rehabilitation after cardiovascular diseases, with special emphasis on developing countries. In W. R. O. f. Europe (Ed.). Geneva: WHO Regional Office for Europe.
Abell, B., Glasziou, P., Briffa, T., & Hoffmann, T. (2016). Exercise training characteristics in cardiac rehabilitation programmes: A cross-sectional survey of Australian practice. Open Heart,3(1), e000374. https://doi.org/10.1136/openhrt-2015-000374.
Schuler, G., Adams, V., & Goto, Y. (2013). Role of exercise in the prevention of cardiovascular disease: Results, mechanisms, and new perspectives. European Heart Journal,34(24), 1790–1799. https://doi.org/10.1093/eurheartj/eht111.
Sattelmair, J., Pertman, J., Ding, E. L., Kohl, H. W., 3rd, Haskell, W., & Lee, I. M. (2011). Dose response between physical activity and risk of coronary heart disease: A meta-analysis. Circulation,124(7), 789–795. https://doi.org/10.1161/CIRCULATIONAHA.110.010710.
Martin, C. K., Church, T. S., Thompson, A. M., Earnest, C. P., & Blair, S. N. P. (2009). Exercise dose and quality of life: A randomized controlled trial. Archives of Internal Medicine,169(3), 269–278.
Chew, D. P., Scott, I. A., Cullen, L., French, J. K., Briffa, T. G., Tideman, P. A., et al. (2016). National Heart Foundation of Australia & Cardiac Society of Australia and New Zealand: Australian clinical guidelines for the management of Acute Coronary Syndromes 2016. Heart, Lung & Circulation,25(9), 895–951. https://doi.org/10.1016/j.hlc.2016.06.789.
Smith, S. C., Jr., Benjamin, E. J., Bonow, R. O., Braun, L. T., Creager, M. A., Franklin, B. A., et al. (2011). AHA/ACCF secondary prevention and risk reduction therapy for patients with coronary and other atherosclerotic vascular disease: 2011 update: A guideline from the American Heart Association and American College of Cardiology Foundation. Circulation,124(22), 2458–2473. https://doi.org/10.1161/CIR.0b013e318235eb4d.
Price, K. J., Gordon, B. A., Bird, S. R., & Benson, A. C. (2016). A review of guidelines for cardiac rehabilitation exercise programmes: Is there an international consensus? European Journal of Preventive Cardiology,23(16), 1715–1733. https://doi.org/10.1177/2047487316657669.
Ibanez, B., James, S., Agewall, S., Antunes, M. J., Bucciarelli-Ducci, C., Bueno, H., et al. (2018). 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). European Heart Journal,39(2), 119–177. https://doi.org/10.1093/eurheartj/ehx393.
Piepoli, M. F., Hoes, A. W., Agewall, S., Albus, C., Brotons, C., Catapano, A. L., et al. (2016). 2016 European guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts). Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). European Heart Journal,37(29), 2315–2381. https://doi.org/10.1093/eurheartj/ehw106.
Powell, R., McGregor, G., Ennis, S., Kimani, P. K., & Underwood, M. (2018). Is exercise-based cardiac rehabilitation effective? A systematic review and meta-analysis to re-examine the evidence. British Medical Journal Open,8, e019656. https://doi.org/10.1136/bmjopen-2017-019656.
van Halewijn, G., Deckers, J., Tay, H. Y., van Domburg, R., Kotseva, K., & Wood, D. (2017). Lessons from contemporary trials of cardiovascular prevention and rehabilitation: A systematic review and meta-analysis. International Journal of Cardiology,232, 294–303. https://doi.org/10.1016/j.ijcard.2016.12.125.
Anderson, L., Thompson, D. R., Oldridge, N., Zwisler, A. D., Rees, K., Martin, N., et al. (2016). Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database of Systematic Reviews,1, Cd001800. https://doi.org/10.1002/14651858.cd001800.pub3.
Shepherd, C. W., & While, A. E. (2012). Cardiac rehabilitation and quality of life: A systematic review. International Journal of Nursing Studies,49(6), 755–771. https://doi.org/10.1016/j.ijnurstu.2011.11.019.
Francis, T., Kabboul, N., Rac, V., Mitsakakis, N., Pechlivanoglou, P., Bielecki, J., et al. (2019). The effect of cardiac rehabilitation on health-related quality of life in patients with coronary artery disease: A meta-analysis. Canadian Journal of Cardiology,35(3), 352–364. https://doi.org/10.1016/j.cjca.2018.11.013.
Anderson, L., Brown, J. P. R., Clark, A. M., Dalal, H., Rossau, H. K. K., Bridges, C., et al. (2017). Patient education in the management of coronary heart disease. Cochrane Database of Systematic Reviews. https://doi.org/10.1002/14651858.CD008895.pub3.
Richards, S. H., Anderson, L., Jenkinson, C. E., Whalley, B., Rees, K., Davies, P., et al. (2017). Psychological interventions for coronary heart disease. Cochrane Database of Systematic Reviews,4, CD002902. https://doi.org/10.1002/14651858.cd002902.pub4.
Norekval, T. M., Falun, N., & Fridlund, B. (2016). Patient-reported outcomes on the agenda in cardiovascular clinical practice. European Journal of Cardiovascular Nursing,15(2), 108–111. https://doi.org/10.1177/1474515115614133.
Reeve, B. B., Wyrwich, K. W., Wu, A. W., Velikova, G., Terwee, C. B., Snyder, C. F., et al. (2013). ISOQOL recommends minimum standards for patient-reported outcome measures used in patient-centered outcomes and comparative effectiveness research. Quality of Life Research,22(8), 1889–1905. https://doi.org/10.1007/s11136-012-0344-y.
Thompson, D. R., Ski, C. F., Garside, J., & Astin, F. (2016). A review of health-related quality of life patient-reported outcome measures in cardiovascular nursing. European Journal of Cardiovascular Nursing,15(2), 114–125. https://doi.org/10.1177/1474515116637980.
Higgins, J., & Green, S. E. ([updated March 2011]). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0: The Cochrane Collaboration, 2011.
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., & Group, P. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ,339, b2535. https://doi.org/10.1136/bmj.b2535.
Long, L., Anderson, L., Dewhirst, A. M., He, J., Bridges, C., Gandhi, M., et al. (2018). Exercise-based cardiac rehabilitation for adults with stable angina. Cochrane Database of Systematic Reviews,2, CD012786. https://doi.org/10.1002/14651858.cd012786.pub2.
Higgins, J. P., Altman, D. G., Gotzsche, P. C., Juni, P., Moher, D., Oxman, A. D., et al. (2011). The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ,343, d5928. https://doi.org/10.1136/bmj.d5928.
Maddison, R., Pfaeffli, L., Whittaker, R., Stewart, R., Kerr, A., Jiang, Y., et al. (2015). A mobile phone intervention increases physical activity in people with cardiovascular disease: Results from the HEART randomized controlled trial. European Journal of Preventive Cardiology,22(6), 701–709. https://doi.org/10.1177/2047487314535076.
Yu, C., Lau, C., Chau, J., McGhee, S., Kong, S., Cheung, B. M., et al. (2004). A short course of cardiac rehabilitation program is highly cost effective in improving long-term quality of life in patients with recent myocardial infarction or percutaneous coronary intervention. Archives of Physical Medicine and Rehabilitation,85, 1915–1922. https://doi.org/10.1016/j.apmr.2004.05.010.
Oerkild, B., Frederiksen, M., Hansen, J. F., & Prescott, E. (2012). Home-based cardiac rehabilitation is an attractive alternative to no cardiac rehabilitation for elderly patients with coronary heart disease: Results from a randomised clinical trial. BMJ Open. https://doi.org/10.1136/bmjopen-2012-001820.
Santaularia, N., Caminal, J., Arnau, A., Perramon, M., Montesinos, J., Abenoza Guardiola, M., et al. (2017). The efficacy of a supervised exercise training programme on readmission rates in patients with myocardial ischemia: Results from a randomised controlled trial. European Journal of Cardiovascular Nursing,16(3), 201–212. https://doi.org/10.1177/1474515116648801.
Seki, E., Watanabe, Y., Sunayama, S., Iwama, Y., Shimada, K., Kawakami, K., et al. (2003). Effects of phase III cardiac rehabilitation programs on health-related quality of life in elderly patients with coronary artery disease: Juntendo Cardiac Rehabilitation Program (J-CARP). Circulation Journal,67, 73–77.
Mutwalli, H. A., Fallows, S. J., Arnous, A. A., & Zamzami, M. S. (2012). Randomized controlled evaluation shows the effectiveness of a home-based cardiac rehabilitation program. Saudi Medical Journal,33(2), 152–159.
Weir, C. J., Butcher, I., Assi, V., Lewis, S. C., Murray, G. D., Langhorne, P., et al. (2018). Dealing with missing standard deviation and mean values in meta-analysis of continuous outcomes: A systematic review. BMC Medical Research Methodology,18(1), 25. https://doi.org/10.1186/s12874-018-0483-0.
Ladak, L. A., Hasan, B. S., Gullick, J., & Gallagher, R. (2018). Health-related quality of life in congenital heart disease surgery in children and young adults: A systematic review and meta-analysis. Archives of Disease in Childhood. https://doi.org/10.1136/archdischild-2017-313653.
Briffa, T. G., Eckermann, S. D., Griffiths, A. D., Harris, P. J., Heath, M. R., Freedman, S. B., et al. (2005). Cost-effectiveness of rehabilitation after an acute coronary event: A randomised controlled trial. Medical Journal of Australia,183(9), 450–455.
Wyrwich, K. W., Spertus, J. A., Kroenke, K., Tierney, W. M., Babu, A. N., & Wolinsky, F. D. (2004). Clinically important differences in health status for patients with heart disease: An expert consensus panel report. American Heart Journal,147(4), 615–622. https://doi.org/10.1016/j.ahj.2003.10.039.
Dixon, T., Lim, L. L. Y., & Oldridge, N. B. (2002). The MacNew heart disease health-related quality of life instrument: Reference data for users. Quality of Life Research,11, 173–183.
Sterne, J. A., & Egger, M. (2001). Funnel plots for detecting bias in meta-analysis: Guidelines on choice of axis. Journal of Clinical Epidemiology,54, 1046–1055.
Wang, W., Chair, S. Y., Thompson, D. R., & Twinn, S. F. (2012). Effects of home-based rehabilitation on health-related quality of life and psychological status in Chinese patients recovering from acute myocardial infarction. Heart and Lung,41(1), 15–25. https://doi.org/10.1016/j.hrtlng.2011.05.005.
Bettencourt, N., Dias, C., Mateus, P., Sampaio, F., Santos, L., Adao, L., et al. (2005). Impact of cardiac rehabilitation on quality of life and depression after acute myocardial infarction. Revista Portuguesa de Cardiologia,24(5), 687–696.
Devi, R., Powell, J., & Singh, S. (2014). A web-based program improves physical activity outcomes in a primary care angina population: Randomized controlled trial. Journal of Medical Internet Research,16(9), e186. https://doi.org/10.2196/jmir.3340.
Reid, R. D., Morrin, L. I., Beaton, L. J., Papadakis, S., Kocourek, J., McDonnell, L., et al. (2012). Randomized trial of an internet-based computer-tailored expert system for physical activity in patients with heart disease. European Journal of Preventive Cardiology,19(6), 1357–1364. https://doi.org/10.1177/1741826711422988.
Sandstrom, L., & Stahle, A. (2005). Rehabilitation of elderly with coronary heart disease: Improvements in quality of life at a low cost. Advances in Physiotherapy,7, 60–66. https://doi.org/10.1080/14038190510010287.
Hautala, A. J., Kiviniemi, A. M., Makikallio, T., Koistinen, P., Ryynanen, O. P., Martikainen, J. A., et al. (2017). Economic evaluation of exercise-based cardiac rehabilitation in patients with a recent acute coronary syndrome. Scandinavian Journal of Medicine and Science in Sports,27(11), 1395–1403. https://doi.org/10.1111/sms.12738.
Houle, J., Doyon, O., Vadeboncoeur, N., Turbide, G., Diaz, A., & Poirier, P. (2012). Effectiveness of a pedometer-based program using a socio-cognitive intervention on physical activity and quality of life in a setting of cardiac rehabilitation. Canadian Journal of Cardiology,28(1), 27–32. https://doi.org/10.1016/j.cjca.2011.09.020.
Warburton, D. E. R., & Bredin, S. S. D. (2017). Health benefits of physical activity: A systematic review of current systematic reviews. Current Opinion in Cardiology,32(5), 541–556. https://doi.org/10.1097/HCO.0000000000000437.
Wise, F. M. (2010). Coronary heart disease: The benefits of execise. Australian Family Physician,39(3), 129–133.
Neufer, P. D., Bamman, M. M., Muoio, D. M., Bouchard, C., Cooper, D. M., Goodpaster, B. H., et al. (2015). Understanding the cellular and molecular mechanisms of physical activity-induced health benefits. Cell Metabolism,22(1), 4–11. https://doi.org/10.1016/j.cmet.2015.05.011.
Dedeyne, L., Deschodt, M., Verschueren, S., Tournoy, J., & Gielen, E. (2017). Effects of multi-domain interventions in (pre)frail elderly on frailty, functional, and cognitive status: A systematic review. Clinical Interventions in Aging,12, 873–896. https://doi.org/10.2147/CIA.S130794.
Gallagher, R., Randall, S., Lin, S. H. M., Smith, J., Clark, A. M., & Neubeck, L. (2018). Perspectives of cardiac rehabilitation staff on strategies used to assess, monitor and review: A descriptive qualitative study. Heart and Lung,47(5), 471–476. https://doi.org/10.1016/j.hrtlng.2018.06.001.
Colella, T. J., & King, K. M. (2004). Peer support: An under-recognized resource in cardiac recovery. European Journal of Cardiovascular Nursing,3(3), 211–217. https://doi.org/10.1016/j.ejcnurse.2004.04.001.
Rumsfeld, J. S., Alexander, K. P., Goff, D. C., Jr., Graham, M. M., Ho, P. M., Masoudi, F. A., et al. (2013). Cardiovascular health: The importance of measuring patient-reported health status: A scientific statement from the American Heart Association. Circulation,127(22), 2233–2249. https://doi.org/10.1161/CIR.0b013e3182949a2e.
Terwee, C. B., Bot, S. D., de Boer, M. R., van der Windt, D. A., Knol, D. L., Dekker, J., et al. (2007). Quality criteria were proposed for measurement properties of health status questionnaires. Journal of Clinical Epidemiology,60(1), 34–42. https://doi.org/10.1016/j.jclinepi.2006.03.012.
Turner, R. M., Bird, S. M., & Higgins, J. P. (2013). The impact of study size on meta-analyses: Examination of underpowered studies in Cochrane reviews. PLoS ONE,8(3), e59202. https://doi.org/10.1371/journal.pone.0059202.
Acknowledgements
We would like to acknowledge the valuable assistance of Judith Fethney, our resident statistician, in providing guidance on our statistical methods.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not required for conducting this review.
Informed consent
Informed consent was not required for conducting this review.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Candelaria, D., Randall, S., Ladak, L. et al. Health-related quality of life and exercise-based cardiac rehabilitation in contemporary acute coronary syndrome patients: a systematic review and meta-analysis. Qual Life Res 29, 579–592 (2020). https://doi.org/10.1007/s11136-019-02338-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-019-02338-y