
Abstract
Purpose
The cancer anorexia–cachexia syndrome (CACS) is highly prevalent in lung cancer (LC) patients (57–61%), and represents the direct cause of death in 20% of cases. Accurately quantifying CACS has been a challenging issue; consequently, this study presents the clinical validation of the Spanish version of the Functional Assessment of Anorexia–Cachexia Therapy (FAACT) scale in LC patients from Latin America.
Methods
The Spanish version of the FAACT and the Mexican-Spanish version of the EORTC-QLQ-C30 instruments were applied to a cohort of patients with LC at the National Cancer Institute of Mexico. Reliability and validity tests were performed to assess the psychometric properties of the scales, and clinical validation was assessed considering the association of scales with subjective and objective clinical data.
Results
Two hundred patients were included. Questionnaire compliance rates were high (100%) and the instrument was well accepted in all cases; internal consistency tests demonstrated good convergent and divergent validity of the scale structure. Cronbach’s α coefficient for three out of five basic multi-item scales was > 0.7 (0.55–0.86). FAACT scales presented significant associations with clinical parameters, including biochemical and nutritional variables (i.e., energy intake, p = 0.002), as well as strongly correlated with the appetite loss subscale of the QLQ-C30 questionnaire (r = − 0.624). Physical well-being (p < 0.0009), functional well-being (p = 0.004), anorexia/cachexia scale (p = 0.029), and FAACT total scores (p = 0.0009) were strongly associated to overall survival.
Conclusion
The Spanish version of the FAACT questionnaire is reliable and valid for the assessment of health-related quality of life and CACS in LC patients and can be used in clinical trials.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Lung cancer (LC) remains the leading cause of cancer-related deaths and is considered a significant health care issue worldwide [1, 2]. Malnutrition is present in 45–50% of patients with advanced LC at the time of diagnosis and it usually increases as the disease progresses [3]. Malnutrition contributes to worsen treatment-related toxicity [4], affects the health-related quality of life (HRQL), and prognosis [5], while weight loss is an independent predictor of shorter overall survival (OS) [6]. Cancer-related anorexia is defined as reduced food intake, while cachexia is edged as the physiologic state of muscle and fat catabolism with a concomitant weight loss; together, these factors constitute the cancer anorexia–cachexia syndrome (CACS) [7, 8]. CACS is present in 57–61% of patients with LC [9], and some reports lead to think this number might increase in the last 2 weeks of life [10]. Almost half of patients lose ≥ 10% of their original body weight throughout the course of the disease [11], and death usually occurs once weight loss has reached 30% of the patient’s historic stable body weight, with CACS being directly attributable for 20% of cancer deaths [12, 13].
Recently, novel chemotherapeutic agents and new combinations have been described in LC with encouraging results in terms of traditional outcomes measures such as response rate, progression-free survival, and OS [14, 15]. However, as new clinical trials emerge, it is important to take into consideration the effect of these therapeutic strategies in patients’ HRQL [16].
The evaluation of HRQL and CACS is essential and should be assessed in all LC-related clinical trials. Therefore, well-designed instruments are needed and their clinical validity must be demonstrated, particularly for non-English speakers, for whom validated instruments are scarce. This is particularly relevant in the current clinical research scenario, which values multicentric trials, and in turn, patients who are not native English speakers are constantly included [17].
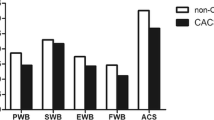
The Functional Assessment of Anorexia–Cachexia Therapy (FAACT) instrument is constructed from the Functional Assessment of Cancer Therapy-General (FACT-G), which includes several subscales developed and validated to measure HRQL, specifically among cancer patients (physical well-being [PWB], emotional well-being [EWB], functional well-being [FWB], and social well-being [SWB]). In addition to these four subscales, the 12-item anorexia/cachexia scale (AC/S) can be added, therefore comprising the FAACT instrument. In addition to FACT-G, other scales that can be calculated using different combinations of the subscales include the FACT-TOI (Trial Outcome Index), which is calculated based on the PWB, FWB, and AC/S [18].
Originally FAACT was developed as an English-language assessment tool, and although it has been validated in English and in other languages, such as Chinese, the scale has not been previously validated in Spanish. Therefore, the aim of this study was to present a psychometric and clinical validation of the Spanish version of the FAACT instrument in a cohort of patients with LC from Latin America.
Methods
Patients and data collection
Consecutive patients attending the Thoracic Oncology Unit at the National Cancer Institute of Mexico (INCan) from July 2014 to July 2015 were prospectively included in this study. All patients who had histologically confirmed diagnosis of LC were invited to participate; including any age (> 18 years of age) or sex, regardless of the histopathology subtype of the neoplasm. Clinical history and physical examination were registered, including blood cell count, albumin levels, nutrients intake, and nutritional status. Clinical staging of patients was defined according to the Seventh Edition of the Tumor, Node, Metastases (TNM) Staging System of the American Joint Committee on Cancer (AJCC) [19].
Exclusion criteria included refusal to participate, inability to understand or complete the questionnaires, or a critical illness besides cancer. Most participants were under treatment undergoing their first, second, third, or further line of chemotherapy, although surveillance patients were also included.
All patients were requested to read and sign a written consent form. Study purpose and data protection policy were detailed in a printed form accompanying the questionnaires. The Institutional Review Board and the Ethics Committee approved the research protocol (014/021/ICI) (CEI/923/14).
Measurements
The FAACT instrument in the Spanish version was supplied by FACIT (FACIT.org) after the appropriate registration for academic purposes and obtaining a license agreement to use the questionnaire. The FAACT instrument included the four subscales of FACT-G: PWB, EWB, FWB, SWB, and the additional anorexia cachexia subscale (AC/S), assigning a value of 0–4 for each item [20, 21]. All questionnaire evaluations were performed according to the specific instructions provided by the Functional Assessment of Chronic Illness Therapy (FACIT) Measurement System. Briefly all subscale items are summed to a total, which is the subscale score, and finally, a total score summarizes the five subscales (0–156). For all FAACT subscales and symptom indices, a higher score indicates a better HRQL [22].
Regarding the AC/S score, a previous consensus by the European Society for Clinical Nutrition and Metabolism (ESPEN) established that a score of ≤ 24 in the AC/S scale would be enough to establish a diagnosis of anorexia [23].
The FAACT questionnaire was correlated with the European organization for research and treatment of cancer (EORTC) Quality of Life Questionnaire (QLQ-C30, version 3.0), which assesses five functioning subscales (physical, role, emotional, cognitive, and social performance), nine symptom subscales (fatigue, nausea and vomiting, pain, dyspnea, Insomnia, appetite loss, constipation, diarrhea, financial difficulties), and a Global health/quality of life scale. The validated Mexican-Spanish version of the QLQ-C30 instrument was used [24], along with the translated Spanish version of the FAACT questionnaire. Scores for multi-item functional or symptom subscales and for single items of QLQ-C30 were calculated based on the guidelines established by the EORTC, briefly we performed a linear transformation of raw scores into a 0–100 score, with 100 representing best global health, functional status, and worst symptoms [25]. Both questionnaires were used with permission of Functional Assessment of Chronic Illness Therapy (FACIT) and EORTC Quality of Life Study Group, respectively.
Subjective Global Assessment (SGA) was performed to classify patients as having severe or moderate malnourishment (B or C), or being well nourished (A) [26]. Macro and micronutrient intake was measured with a food frequency questionnaire (SNUT) validated for Mexican population by the National Institute of Public Health of Mexico [22].
Data analysis
Based on the proposal of Tabachnik and Fidell, which considers that in order to obtain reliable estimates through multivariate analysis, the number of observations estimated was five patients per item [27], considering that the FAACT instrument has 39 items and the sample size was 195 patients.
Sample characteristics were analyzed with descriptive statistics. The assessment of bivariate correlation of items was performed using the Spearman Correlation Coefficient (CC) for convergent and divergent validity, and Cronbach’s α was used for multi-item correlation for assessing internal consistency. In addition, we divided patients into subgroups according to variables of clinical interest, including body mass index (BMI), Karnofsky performance status (KPS), lines of therapy, stage, weight loss > 10%, neutrophils/lymphocytes ratio (NLR), platelets/lymphocytes ratio (PLR), serum albumin, hemoglobin, SGA, energy intake, and different nutrients intake (protein, carbohydrate, fat, iron, vitamin B6, and B12). We hypothesized that patients with indicators of a better clinical condition (i.e., IMC > 18 kg/m2, KPS > 80, serum albumin > 3.9, weight loss < 10%, SGA = A, energy intake > 1000 kcal/day), would have a higher FAACT score, better nutritional status, and would correlate with improved survival outcomes. Clinical validity was evaluated by the extent to which FAACT scores were able to discriminate among groups of patients who differed according to these clinical variables; the Kruskal–Wallis test was used to analyze differences between groups. Finally, FAACT and QLQ-C30 subscales were correlated with Spearman test to evaluate similarity. A survival analysis was also performed as a secondary goal according to the different subscales of the FAACT instrument [PWB (0–14 vs. 15–23 vs. 24–28), FWB (0–19 vs. 20–25), AC/S (0–23 vs. 24–48)] and the total FAACT score (0–98 vs. 99–119 vs. 120–156). The aim of this additional analysis was to determine if the scores from the FAACT instrument could serve as a prognostic determinant in our LC patient population. OS was defined as the time from study enrollment until last follow-up or death. Only stage IV patients were included in this analysis as to avoid a survival bias from earlier stage patients, who are known to have longer survival. OS was analyzed using the Kaplan–Meier method, comparisons among median values were performed using the Log-rank test. Probability values of 0.05 or less were considered significant, and two-tailed statistics were taken into account in all cases. SPSS for MAC version 20 was employed to perform all computations (IBM, Corp., Armonk, NY, USA).
Results
Patients
A total of two hundred patients (116 female and 84 male) with a median age of 61.8 (± 13.2) years were included in this study. The most frequent histological type was adenocarcinoma in 67%, followed by squamous cell carcinoma in 14% of the patients. In 78% of patients, the clinical stage was IV, in 13% stage III, and 3% stage I or II. Median BMI was 24.1 (12.1–41.7), while the SGA score showed that 58.5% of patients had a moderate or severe malnourishment (B or C). Median score for the FAACT instrument was 107.5 (89–122).
Reliability and validity
Descriptive statistics of data obtained from FAACT are shown in Table 1. The floor represents the minimum value answered and the ceiling represents the maximum. The first five subscales of FAACT presented measurements across the range of each scale.
Table 2 describes a summary of multi-trait scaling analyses for the five FAACT subscales presented. We assessed that convergent and divergent validity existed from the bivariate correlation of the different subscales of the FACT-G instrument. Items from their own-scale showed high correlation scores, while items from other scales showed lower correlation. Although some overlapping was found in convergent (“Item own-scale correlations”) and divergent (“Item other-scale correlations”) scales, this was due to the fact that some of the subscales present items related among them, for example, PWB is related to FWB, likewise PWB is related to AC/S. For internal consistency, PWB, SWB, and FWB subscales show multivariate correlations Cronbach’s α coefficients > 0.70 (0.55–0.86).
Clinical validation
The FAACT total score and its subscales presented a strong association with several clinical variables. Lower BMI (< 18.5 kg/m2) was associated with lowers PWB, FWB, AC/S, and total FAACT score. A bad performance status (KPS ≤ 80) was associated with lower PWB, SWB, EWB, FWB, and AC/S subscales scores. Weight loss ≥ 10% in 6 months was associated with lower PWB, FWB, and AC/S subscales scores. High rates of neutrophils lymphocytes index (NLI) were associated with worse PWB and AC/S, while a high rate of platelets lymphocytes index (PLI) was associated with worst PWB, FWB, and AC/S subscales scores. Serum albumin ≤ 3.9 and hemoglobin ≤ 12.8 were associated with lower PWB, FWB, and AC/S scores. Clinical and biochemical variables are shown in Table 3.
A risk or a state of malnutrition (SGA B or C) was associated with worst PWB, FWB, AC/S, and TOTAL SCORE. Energy intake ≤ 1000 kcal was associated with worst PWB, FWB, AC/S, FACT-TOI, FACT-G, and FACT TOTAL score (Table 4).
Correlations between instruments
FAACT total score had better correlations with global health status (0.618), physical functioning (0.606), emotional functioning (0.642), and appetite loss (− 0.624) subscales from QLQ-C30; the scores scatters are shown in Fig. 1.

Correlation of the Total FAACT score with QLQ-C30 subscales scores. a Correlation of Global health status from Quality Life Questionnaire C-30 (QLQ-C30) with Functional Assessment of Anorexia Cachexia Therapy (FAACT) total score. b Correlation of emotional functioning from QLQ-C30 with FAACT total score. c Correlation of physical functioning from QLQ-C30 with FAACT total score. d Correlation of appetite loss from QLQ-C30 with FAACT total score
Survival
Survival was calculated from the day the questionnaire was performed until last visit, loss of follow-up, or death. Only stage IV patients receiving treatment were included in the analysis leaving a total of 146 patients, of which 30.8% died over a period of 2 years. The median post-questionnaire survival was 10.7 months. Moreover, FAACT and subscales scores were divided into quartiles, survival according to these groups is shown in Fig. 2. Higher scores predicted longer survival in the PWB (p < 0.001), FWB (p = 0.004), AC/S (p = 0.029), and FAACT total (p = 0.002).

Survival according to scores from FAACT and subscales. a Physical well-being results were divided in three groups according to scores (subscale range 0–28). b Functional well-being results were divided in two groups according to scores (subscale range 0–28). c Anorexia/cachexia results were divided in two groups according to scores (subscale range 0–48). d FAACT total results were divided in three groups according to scores (subscale range 0–156)
Discussion
As novel LC therapies emerge, it is important to consider how these interventions will impact patient HRQL, in addition to their potential efficacy. The EORTC is one of the most used instruments in clinical trials to measure HRQL in cancer patients, it includes the Quality of Life Questionnaire (QLQ-C30), which evaluates global, functional, and symptomatic items [16]. Also, most studies in cancer patients assess adverse effects of treatment with the Common Terminology Criteria for Adverse events (CTCAE) instrument; which has the purpose of recording 790 adverse events, while 78 symptoms are appropriate for self-reporting. Whereas these instruments are an approximation to evaluating changes in quality of life of cancer patients, including those with anorexia, there are specific instruments for evaluating quality of life in anorexia/cachexia cancer patients and their changes throughout their treatments. The FAACT instrument represents a more appropriate tool for evaluating HRQL in patients with CACS at diagnosis and throughout their follow-up. This study brings a valid and reliable Spanish version of the FAACT instrument proving internal consistency, convergent and divergent validity, and clinical validation in Spanish-speaking LC patients.
Cronbach’s α coefficients are very similar to those found in advanced non-small cell LC patients in the English version from 2015; particularly in PWB, SWB, FWB with differences ranging from 0.04 to 0.24 [18]. Systemic inflammatory response (SIR) may contribute to the deterioration of nutritional and functional status in LC patients [28], and such parameters were discriminated significantly with the FAACT scores. Other highly discriminated parameters include KPS, NLR, PLR, serum albumin, and hemoglobin.
Likewise, parameters that are related with anthropometric characteristic and CACS include weight loss of more than 10% in the last 6 months, SGA, and energy intake, all of which were also well discriminated by the FAACT scores. However, no differences were found in the FAACT scores between above or below means in macro or micronutrients. This is likely explained by the fact that a more specific instrument is needed, than a food frequency questionnaire, to quantify micronutrients, for example, a 24-h recall. Nevertheless, this is a challenging parameter to evaluate, due to the fact that patients usually undergo biochemical studies 1 day before their questionnaire evaluation, and they are required to go on a fast, therefore the previous day intake rarely represents their usual diet. Furthermore, when correlating the QLQ-C30 questionnaires with the FAACT instrument, the highest correlation was observed between the appetite loss item (QLQ-C30) and the AC/S score (FAACT). This allows the FAACT instrument to be considered a more objective instrument to evaluate HRQL in cancer patients with anorexia and/or cachexia.
As previously mentioned, HRQL is an important aspect which must be systematically evaluated in all LC patients, particularly those who are being subjected to novel therapeutic agents and/or combination therapy. Through this study, we are able to establish a highly reliable questionnaire, which can identify patients who are at risk or already undergoing a deterioration of their HRQL, and as such these patients can be channeled to specialists who can aid in the process. Another important aspect is the possibility of diagnosing anorexia using specifically the AC/S, which is a widely available tool, with a high degree of acceptance by patients. The AC/S item of FAACT can diagnose anorexia using the consensus cut-off point of ≤ 24 in cancer patients [23], which identifies subjects with severe anorexia, or also apply a cut-off point of ≤ 32, which has been seen to identify LC patients with mild–moderate anorexia [in progress]. This would inherently open the possibility to better assess patients who are candidates for appetite stimulants, with the aim of improving nutritional status, HRQL, and survival outcomes.
The present study has several strengths, we included a large cohort of Mexican patients with LC treated in a single cancer center, undergoing similar treatments and protocols, as well as clinical chemistry assessments. Also, we prospectively followed the patients and included an OS analysis. This study additionally suggests an association between the FAACT subscales and survival in LC patients. Moreover, data from this study support that we can reliably measure HRQL in LC patients who are at risk or diagnosed with CACS using an easy, quick, and freely available instrument in Spanish version, which allows for a systematic patient follow-up. It is important to note that the association found between CACS and OS proposes that the FAACT questionnaire could be used as a prognostic factor for establishing a personalized management; however, this implication requires further validation using a larger sample and longer follow-up. Limitations of this study include the fact that some baseline characteristics were slightly unbalanced, such as a higher percentage of females compared to males (58% vs. 42%). Another limitation which can be taken into consideration for future studies is the fact that these patients are likely to have an altered body composition, and it would be interesting to assess body fat and fat-free mass, which was not an objective in this study.
In conclusion, in a Mexican population of LC patients the Spanish version of the FAACT instrument is reliable and valid for the assessment of HRQL and CACS. FAACT demonstrated internal consistency, convergent and divergent validity, and clinical validation. The Spanish version of the FAAACT can be used in clinical trials involving Mexican patients with LC.
References
Torre, L. A., Bray, F., Siegel, R. L., Ferlay, J., Lortet-Tieulent, J., & Jemal, A. (2015). Global cancer statistics, 2012. Cancer Journal For Clinicians, 65(2), 87–108. https://doi.org/10.3322/caac.21262.
Salsman, J. M., Beaumont, J. L., Wortman, K., Yan, Y., Friend, J., & Cella, D. (2015). Brief versions of the FACIT-fatigue and FAACT subscales for patients with non-small cell lung cancer cachexia. Supportive Care in Cancer, 23(5), 1355–1364. https://doi.org/10.1007/s00520-014-2484-9.
Sanchez-Lara, K., Turcott, J. G., Juarez-Hernandez, E., Nunez-Valencia, C., Villanueva, G., Guevara, P., et al. (2014). Effects of an oral nutritional supplement containing eicosapentaenoic acid on nutritional and clinical outcomes in patients with advanced non-small cell lung cancer: Randomised trial. Clinical Nutrition, 33(6), 1017–1023. https://doi.org/10.1016/j.clnu.2014.03.006.
Arrieta, O., Michel Ortega, R. M., Villanueva-Rodriguez, G., Serna-Thome, M. G., Flores-Estrada, D., Diaz-Romero, C., et al. (2010). Association of nutritional status and serum albumin levels with development of toxicity in patients with advanced non-small cell lung cancer treated with paclitaxel-cisplatin chemotherapy: A prospective study. BMC Cancer, 10, 50. https://doi.org/10.1186/1471-2407-10-50.
Sanchez-Lara, P. A., Zhao, H., Bajpai, R., Abdelhamid, A. I., & Warburton, D. (2012). Impact of stem cells in craniofacial regenerative medicine. Frontiers in Physiology, 3, 188. https://doi.org/10.3389/fphys.2012.00188.
Kovarik, M., Hronek, M., & Zadak, Z. (2014). Clinically relevant determinants of body composition, function and nutritional status as mortality predictors in lung cancer patients. Lung Cancer, 84(1), 1–6. https://doi.org/10.1016/j.lungcan.2014.01.020.
Fearon, K., Strasser, F., Anker, S. D., Bosaeus, I., Bruera, E., Fainsinger, R. L., et al. (2011). Definition and classification of cancer cachexia: An international consensus. The Lancet Oncology, 12(5), 489–495. https://doi.org/10.1016/S1470-2045(10)70218-7.
Blum, D., Stene, G. B., Solheim, T. S., Fayers, P., Hjermstad, M. J., Baracos, V. E., et al. (2014). Validation of the consensus-definition for cancer cachexia and evaluation of a classification model: A study based on data from an international multicentre project (EPCRC-CSA). Annals of Oncology, 25(8), 1635–1642. https://doi.org/10.1093/annonc/mdu086.
Del Ferraro, C., Grant, M., Koczywas, M., & Dorr-Uyemura, L. A. (2012) Management of anorexia–cachexia in late stage lung cancer patients. Journal of Hospice and Palliative Nursing. https://doi.org/10.1097/NJH.0b013e31825f3470.
Teunissen, S. C., Wesker, W., Kruitwagen, C., de Haes, H. C., Voest, E. E., & de Graeff, A. (2007). Symptom prevalence in patients with incurable cancer: A systematic review. Journal of Pain and Symptom management, 34(1), 94–104. https://doi.org/10.1016/j.jpainsymman.2006.10.015.
Argiles, J. M. (2005) Cancer-associated malnutrition. European Journal of Oncology Nursing, 9(Suppl 2), S39–S50. https://doi.org/10.1016/j.ejon.2005.09.006.
Tisdale, M. J. (2002). Cachexia in cancer patients. Nature Reviews Cancer, 2(11), 862–871. https://doi.org/10.1038/nrc927.
Skipworth, R. J., Stewart, G. D., Dejong, C. H., Preston, T., & Fearon, K. C. (2007). Pathophysiology of cancer cachexia: Much more than host–tumour interaction? Clinical Nutrition, 26(6), 667–676. https://doi.org/10.1016/j.clnu.2007.03.011.
Pilkington, G., Boland, A., Brown, T., Oyee, J., Bagust, A., & Dickson, R. (2015). A systematic review of the clinical effectiveness of first-line chemotherapy for adult patients with locally advanced or metastatic non-small cell lung cancer. Thorax, 70(4), 359–367. https://doi.org/10.1136/thoraxjnl-2014-205914.
Therasse, P., Arbuck, S. G., Eisenhauer, E. A., Wanders, J., Kaplan, R. S., Rubinstein, L., et al. (2000). New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. Journal of the National Cancer Institute, 92(3), 205–216.
Basch, E., Geoghegan, C., Coons, S. J., Gnanasakthy, A., Slagle, A. F., Papadopoulos, E. J., et al. (2015). Patient-reported outcomes in cancer drug development and US Regulatory Review: Perspectives from industry, the food and drug administration, and the patient. JAMA Oncology, 1(3), 375–379. https://doi.org/10.1001/jamaoncol.2015.0530.
Wheelwright, S., Darlington, A. S., Hopkinson, J. B., Fitzsimmons, D., White, A., & Johnson, C. D. (2013). A systematic review of health-related quality of life instruments in patients with cancer cachexia. Supportive Care in Cancer, 21(9), 2625–2636. https://doi.org/10.1007/s00520-013-1881-9.
LeBlanc, T. W., Samsa, G. P., Wolf, S. P., Locke, S. C., Cella, D. F., & Abernethy, A. P. (2015) Validation and real-world assessment of the Functional Assessment of Anorexia–Cachexia Therapy (FAACT) scale in patients with advanced non-small cell lung cancer and the cancer anorexia–cachexia syndrome (CACS). Supportive Care in Cancer 23(8), 2341–2347. https://doi.org/10.1007/s00520-015-2606-z.
Edge, S. B., & Compton, C. C. (2010). The American Joint Committee on Cancer: The 7th edition of the AJCC cancer staging manual and the future of TNM. Annals of Surgical Oncology, 17(6), 1471–1474. https://doi.org/10.1245/s10434-010-0985-4.
Chang, V. T., Xia, Q., & Kasimis, B. (2005). The Functional Assessment of Anorexia/Cachexia Therapy (FAACT) appetite scale in veteran cancer patients. The Journal of Supportive Oncology, 3(5), 377–382.
Ribaudo, J. M., Cella, D., Hahn, E. A., Lloyd, S. R., Tchekmedyian, N. S., Von Roenn, J., et al. (2000). Re-validation and shortening of the Functional Assessment of Anorexia/Cachexia Therapy (FAACT) questionnaire. Quality of life research. Care and Rehabilitation, 9(10), 1137–1146.
Hernandez-Avila, M., Romieu, I., Parra, S., Hernandez-Avila, J., Madrigal, H., & Willett, W. (1998). Validity and reproducibility of a food frequency questionnaire to assess dietary intake of women living in Mexico City. Salud publica de Mexico, 40(2), 133–140.
Muscaritoli, M., Anker, S. D., Argiles, J., Aversa, Z., Bauer, J. M., et al. (2010). Consensus definition of sarcopenia, cachexia and pre-cachexia: Joint document elaborated by Special Interest Groups (SIG) “cachexia-anorexia in chronic wasting diseases” and “nutrition in geriatrics”. Clinical Nutrition, 29(2), 154–159. https://doi.org/10.1016/j.clnu.2009.12.004.
Arrieta, O., Nunez-Valencia, C., Reynoso-Erazo, L., Alvarado, S., Flores-Estrada, D., Angulo, L. P., et al. (2012). Health-related quality of life in patients with lung cancer: Validation of the Mexican-Spanish version and association with prognosis of the EORTC QLQ-LC13 questionnaire. Lung Cancer, 77(1), 205–211. https://doi.org/10.1016/j.lungcan.2012.02.005.
Fayers, P. M. M. D. (2000). Quality of life: Assessment, analysis and interpretation. Chichester: Wiley.
Bauer, J., Capra, S., & Ferguson, M. (2002). Use of the scored Patient-Generated Subjective Global Assessment (PG-SGA) as a nutrition assessment tool in patients with cancer. European Journal of Clinical Nutrition, 56(8), 779–785. https://doi.org/10.1038/sj.ejcn.1601412.
Tabachnick, B. G., & Fidell, L. S. (2014). Using multivariate statistics (6th edn.). Jarlow: Pearson.
Sanchez-Lara, K., Turcott, J. G., Juarez, E., Guevara, P., Nunez-Valencia, C., Onate-Ocana, L. F., et al. (2012). Association of nutrition parameters including bioelectrical impedance and systemic inflammatory response with quality of life and prognosis in patients with advanced non-small-cell lung cancer: A prospective study. Nutrition and Cancer, 64(4), 526–534. https://doi.org/10.1080/01635581.2012.668744.
Acknowledgements
The authors certify that they comply with the ethical guidelines for authorship and publishing of the Journal of Supportive Care in Cancer.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Oscar Arrieta has received payment for lectures from Pfizer, AstraZeneca, Boehringer-Ingelheim, and Roche. Julissa Luvian-Morales declares no conflict of interest. Jenny G. Turcott declares no conflict of interest. Luis F. Oñate-Ocaña declares no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Arrieta, O., Luvián-Morales, J., Turcott, J.G. et al. Quality of life and anorexia/cachexia in lung cancer: validation of the Spanish version of the FAACT instrument. Qual Life Res 27, 2709–2718 (2018). https://doi.org/10.1007/s11136-018-1930-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-018-1930-4