
Abstract
Purpose
To explore country-specific influences on the determinants of two forms of subjective well-being (life satisfaction and quality of life) among older adults in England and the USA.
Methods
Harmonised data from two nationally representative panel studies of individuals aged 50 and over, the English Longitudinal Study of Ageing (ELSA) and the Health and Retirement Study (HRS), are used. Linear regression models are fitted separately for life satisfaction and quality of life scales using cross-sectional samples in 2004. The ELSA sample was 6,733, and the HRS sample was 2,300. Standardised coefficients are reported to determine the country-specific importance of explanatory variables, and predicted values are shown to highlight the relative importance of statistically significant country-level interaction effects.
Results
Having a disability, been diagnosed with a chronic conditions or having low household wealth are strongly associated with poorer life satisfaction and quality of life. These statistical effects are consistent in England and the USA. The association of years spent in education, however, varied between the two countries: educational inequalities have a greater adverse effect on subjective well-being in the USA compared with England.
Conclusion
Interventions are required to counterbalance health and socioeconomic inequalities that restrict sections of the population from enjoying satisfying and meaningful lives in older age. The differential association between education and well-being in England and the USA suggests that the provision of welfare benefits and state-funded public services in England may go some way to protect against the subsequent adverse effect of lower socioeconomic status on subjective well-being.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
This paper examines two dimensions of subjective well-being (SWB) (life satisfaction and quality of life) among older adults using data from two nationally representative surveys in England and the USA. The paper has two main aims. First, to explore the relative importance of broad determinants in two conceptually different measures of SWB in England and the USA to see whether key influences predict different dimensions of well-being consistently. Second, to explore whether the importance of particular determinants varies across the USA and England to see whether there is a differential country-level effect on SWB. Multiple measures and cross-country comparisons of SWB determinants are an underdeveloped area of study because of the requirement of comparative samples and data [1].
Strategies relating to public health in England and the USA are predicated on the possibility that society benefits when everyone has the opportunity to live long, healthy and productive lives [2]. The policy agenda in both countries has sought to reduce inequalities in health and well-being through interventions targeted at those people most at risk of poor health and well-being. The success of these policies can be assessed by comparing the determinants across the two countries. In doing so, we can identify those determinants that are universal and those that are a result of national context, allowing public policy to be focused [1]. Focusing on inequalities in later life is important because they can be most visible at this stage of the life course [3], and there remains the possibility that interventions in later life will make a difference even if they cannot repair all of the negative effects of disadvantages that have accumulated during the life course.
The paper is structured as follows. The next subsection provides a review of the existing literature on the determinants of SWB with particular reference to later life. Section two explains the data and methods used. Section three describes the results. The final section draws together the findings and previous literature.
Review of subjective well-being determinants
This subsection will discuss the key factors that relate to well-being among older adults. The empirical evidence on the key determinants of subjective well-being provides inconsistent findings, perhaps because of the many different ways, SWB has been theorised and operationalised [4]. In its simplest form, SWB is often measured by asking people how happy or satisfied they are with their life. However, such measurement pays little attention to the theoretical basis of SWB and the empirical development of SWB measures [5, 6]. Subjective well-being is, rather, a multidimensional social construct that comprises more than an absence of poor health and can be split into two broad theoretical strands: hedonic and eudemonic well-being [7, 8].
Hedonic well-being, or psychological well-being, refers to the idea of pleasure maximisation and is measured through cognitive scales of life satisfaction and by the presence of positive effect and absence of negative effect. Positive and negative effects are emotional mood experiences, which are often highly correlated for the same individuals; however, high levels of each are not mutually exclusive. Eudemonic well-being is seen as more than pleasure or happiness and involves a sense of realising one’s worth in life and the control that a person has over their life [9]. Eudemonic theories of well-being are often contrasted against the hedonic tradition since they were developed as a critique of the lack of theoretical grounding in life satisfaction scales and are referred to as a more social subjective concept [8]. Nonetheless, and despite their conceptual distinctiveness, both concepts of well-being are complementary as shown by their high correlation when operationalised.
In later life, age has been shown to relate to hedonic well-being, typically operationalised as life satisfaction, in a different way to eudemonic well-being, which is often operationalised using measures of quality of life. When controlling for other known associates, quality of life declines at the oldest age having increased from middle age [10, 11], whereas life satisfaction remains more stable. It has been shown that once declines in health and changes in marital status are taken into account people in the oldest old (aged 75 and over) have higher life satisfaction compared with the young old (aged 60-74) [12]. It is unclear whether the latter finding is a result of generational differences or survivor effects [13] or whether omitted variables related to age drive this association.
The relationship between gender and both strands of SWB is unclear. Cheung and Ngan [14] find that women in Hong Kong are more satisfied with life than men; however, Meggiolaro [15] finds that men in Italy have higher life satisfaction than women. Previous studies have shown small but insignificant gender effects on quality of life in England [10, 11]. A number of authors have suggested that, because of different sources of life satisfaction and quality of life, effects will interact differently with gender [16, 17]. The literature suggests stronger socioeconomic status effects for men and greater social integration and functional ability effects for women. Nonetheless, most studies of adults in later age find no effect of gender on SWB and few gendered differences in other effects, especially once controlling for health conditions [18].
A more important determinant of SWB that differentiates the older age population is the effect of living in a couple, which is considered to provide social support as well as an accumulation of resources that can directly and indirectly affect SWB, especially in later life [14]. Numerous studies have found that people who are married have higher levels of life satisfaction than those that are single, separated, divorced or widowed [1, 19, 20]. Those who are separated are often shown to have the worst life satisfaction, perhaps as a result of an adjustment phase to a life event that is generally perceived to be negative.
There is considerable debate as to how socioeconomic status affects SWB. Higher socioeconomic status can directly, through access to financial resources, and indirectly, through being able to draw on a range of cultural social resources, impact upon SWB. Netuveli et al. [10] find that in older age, quality of life is greater with higher income and for those who are retired and lower for those who are unemployed and in poor financial circumstances. The findings are replicated in many other cross-sectional studies of SWB. Cooper et al. [19] and Meggiorlaro [15] find that higher levels of education are associated with better life satisfaction among people in later life. These cross-sectional study designs make it difficult to rule out reverse causality or other endogenous effects. However, Webb et al. [21] investigate the effect of changes in socioeconomic status on SWB and find that worsening financial position contributes to declining quality of life over time.
Health, which is highly related to socioeconomic status in later life, is consistently shown to be associated with life satisfaction and quality of life [22]. This is especially the case in older age samples where poorer levels of health (measured by physical functioning and chronic conditions) appear to explain lower levels of well-being [12]. Helliwell [1] suggests that the effect of health on SWB is a long-term, rather than short-term, adjustment, which itself is determined by cumulative disadvantages. Nonetheless, short-term changes in health have been shown to have small effects on SWB in later life [12].
We restrict analysis in this paper to exploring influences on life satisfaction and quality of life and hypothesise that the importance of several of the key socioeconomic determinants for each outcome will be similar. However, based on existing literature, we hypothesise that marital status will be a more important independent predictor of life satisfaction than quality of life, whereas we expect the opposite to be the case for health status. Our second hypothesis is that some of these associations will be stronger in the USA compared with England. For example, we assume that the effect of poor health and socioeconomic status will be felt more harshly in the USA because of the higher level of inequality and less generous safety nets to protect the least well off through welfare benefits and public services, particularly during working age when socioeconomic inequalities widen. We suppose that all other effects (age, gender and marital status) will operate consistently in the USA and England given the cultural similarities between the two countries. We use broad measures of socioeconomic status, which can be deemed comparable in the USA and England, and avoid specific determinants that may be difficult to operationalise comparably in the two countries. The cross-sectional nature of the data used to test these hypotheses means that these effects should not be considered causal, but associations that require further theoretical and empirical investigation.
Methods
Data
We use cross-sectional data from two nationally representative panel surveys in England and the USA that collect observational data from respondents aged 50 and over. The American Health and Retirement Study (HRS) began in the early 1990s as two separate biennial studies that were fully integrated by 1998 [23]. Later waves of HRS include refreshment sample members that have been added to ensure the sample remains representative of the population aged over 50. The English Longitudinal Study of Ageing (ELSA), which has been developed, in part, to provide comparative data to HRS, has sampled the same respondents every 2 years since 2002. ELSA respondents were drawn from people who previously participated in the Health Survey for England and include refreshment members in later waves to ensure the sample remains cross-sectionally representative [24]. We use data from the 2004 wave in both surveys and select people aged 55 and over to ensure a comparable cross-sectional sample. Longitudinal analysis of the SWB measures used in this study was not possible at the time of analysis, because they were not collected at multiple waves for the same individuals in both ELSA and HRS.
Outcome measures
Two outcome measures of SWB are used in this study, reflecting the hedonic and eudemonic dimensions of well-being. Both measures are asked in the self-completion questionnaires given to those who are interviewed face to face in HRS (30 % of the sample with a 68 % response rate, including non-response to the interview) and ELSA (all of the sample with an 83 % response rate, including non-response to the interview). Non-response is adjusted using a weighting factor that takes account of respondent characteristics that predict attrition up to the 2004 waves of HRS and ELSA. The response rate of ELSA eligible members drawn from the HSE sample frame was 52 % in the 2004 wave [25].
Hedonic well-being is measured using the Satisfaction With Life Scale (SWLS) developed by Diener et al. [26]. This scale, which consists of five evaluative items about overall life satisfaction, is a widely used measure of subjective well-being in academic research [27]. A higher SWLS score indicates better life satisfaction. Eudemonic well-being is measured using a revised CASP-19 scale developed by Wiggins et al. [28]. CASP-19 was specifically designed to measure quality of life in later age covering four domains: control, autonomy, self-realisation and pleasure. In the original scale, three domains had five items with the control domain having four [29]. In a revised 15-item scale suggested by Vanhoutte [7], which we use here, four items are removed that either have low factor loadings to the substantive domain (i.e. shortage of money and family responsibility) or have moderate loadings across multiple substantive domains (i.e. my age prevents me from doing things and my health stops me from doing things). A higher CASP-15 score indicates better quality of life.
Explanatory variables
Demographic—Age is categorised into five groups allowing us to examine nonlinear associations: 55–59, 60–64, 64–69, 70–74 and 75 and over. Marital status is measured using a four-group categorisation based on individuals’ current and previous relationships: single and never been married nor in a civil partnership; married, in a civil partnership or cohabiting; separated or divorced; and widowed.
Socioeconomic—Wealth is measured by grouping individuals into country-specific household wealth quintiles based on non-pension family wealth. The measure includes the net value of a primary residence. Education is measured by the number of years spent in school. Individuals are grouped into four categories: those that left before the compulsory school/high school leaving age (referred to as ‘no qualifications’), those leaving at compulsory school leaving age or a high school graduate (referred to as ‘secondary school’), those leaving after school age or with some college (referred to as ‘post-secondary’) and those leaving after aged 19 or after college (referred to as ‘degree’).
Health—The number of limitations in Activities of Daily Living (ADL) and Instrumental Activities of Daily Living (IADL) reported by the respondent provide an indication of disability. ADLs comprise dressing, walking, bathing, eating, getting out of bed and using the toilet. IADLs comprise preparing a hot meal, shopping for groceries, making telephone calls, taking medication, doing work around the house and managing money. Chronic conditions are measured by the number of the following health problems a respondent reports having ever been diagnosed with: heart disease (angina, a heart attack, congestive heart, heart murmurs, abnormal heart rhythm or other heart problem), a stroke, diabetes, cancer, lung disease or arthritis.
Statistical analysis
Life satisfaction and quality of life SWB measures are first modelled separately in HRS and ELSA as a function of the explanatory variables using ordinary least squares (OLS) regression. We report standardised beta coefficients to show the relative importance of factors associated with each SWB outcome and separately in HRS and ELSA. We then pool data from HRS and ELSA and fit OLS regression models for each SWB outcome, including a dummy variable for country, and interact this effect with all other explanatory variables to determine which, if any, have a differential association across the two countries. The interaction terms were added sequentially to ensure the sample size was large enough to test each effect. The stability in the effects meant we have only reported the full model. We report predicted values for SWLS and CASP-15 for those interactions that are significant at the 95 % level in each model. All models are adjusted using weights that take account of the sample design and non-response. The statistical analysis is carried out using STATA software version 12.
Results
The characteristics of the nationally representative samples from ELSA and HRS are described elsewhere [23, 24]. Table 1 shows that average life satisfaction in older age is at a similar level in England and the USA, while quality of life is shown to be higher in the USA compared with England. In both countries, life satisfaction is highest at older ages, whereas quality of life remains constant across age groups, except for lower levels at the very oldest age. Males have marginally higher life satisfaction than women and, in the USA, lower quality of life. People in a couple have the highest life satisfaction and quality of life, and those separated or divorced have the lowest level of any marital status group. There is a clear wealth gradient to life satisfaction and quality of life, those with higher household wealth report higher levels of both SWB measures. This effect is insensitive to the exclusion of the value of housing from the wealth measure and the inclusion of a measure income (not shown here). Older adults with no educational qualifications report lower life satisfaction and quality of life than those with qualifications. The differences across education groups are greater in the USA compared with England. Those with no limitations in activities of daily living have considerably higher life satisfaction and quality of life in the USA and England. Older adults with more chronic conditions report poorer SWB on both measures and in both countries.
The results of the fitted regression models for life satisfaction and quality of life are shown in the ‘Appendix’ and are presented graphically in Figs. 1, 2 and 3. Figure 1 illustrates the relative importance of determinants in England on life satisfaction and quality of life. The strongest determinant of poor SWB in both models is whether someone has multiple disabilities, measured by three or more limitations in activities in daily living. Having more chronic health conditions is also negatively associated with life satisfaction and quality of life. Lower household wealth has a strong association with life satisfaction and quality of life. Being separated from a partner has a significant negative association on both SWB outcomes; however, the relationship is stronger relative to other variables in the life satisfaction model than in the quality of life model. There is also a consistent, but small, association with both outcomes for gender, with men having poorer life satisfaction and quality of life relative to women. Those with no qualifications or school-level qualifications only, have the lowest levels of quality of life when controlling for other effects. However, there is no significant association between education and life satisfaction in England. Age has a diverging effect on life satisfaction and quality of life. The oldest old (aged 75 and over) have higher life satisfaction, but lower levels of quality of life compared with those aged 60–74.

Standardised beta coefficients: quality of life and life satisfaction, England (ELSA). Note insignificant parameters at 95 % level set to zero. Grey shades indicate separate variables. Beta coefficient represents how many standard deviations SWB will change, per standardised deviation increase in predictor variables

Standardised beta coefficients: quality of life and life satisfaction, USA (HRS). Note insignificant parameters at 95 % level set to zero. Grey shades indicate separate variables. Beta coefficient represents how many standard deviations SWB will change, per standardised deviation increase in predictor variables

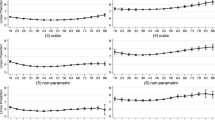
Cross-country predicted effects of marital status and education on quality of life and life satisfaction. (Color figure online)
Figure 2 illustrates the relative importance of determinants in the USA for life satisfaction and quality of life. The associations are fairly consistent across the two SWB outcomes in the USA. Having three or more limitations in activities of daily living is an important determinant of poorer life satisfaction and quality of life. Chronic conditions, household wealth and time spent in education are significantly associated with both SWB outcomes in the expected direction and have a stronger negative association with life satisfaction than disability. Older age is significantly associated with higher levels of life satisfaction, but not quality of life. Men have lower levels of quality of life relative to women, but there is no significant independent relationship between gender and life satisfaction. Being separated from a partner compared with being in a couple has a significant association with life satisfaction, but not with quality of life.
Figure 3 shows differences across the USA and England in the association between SWB and potential determinants. Predicted values of life satisfaction and quality of life are shown for determinants that have a statistically significant interaction term with a country dummy in a model of pooled data from ELSA and HRS, indicating that they have a differential effect across England and the USA.
There is a differential association between education and life satisfaction and quality of life across the two countries. People with a degree are predicted to have higher SWB on both outcomes in the USA compared with England and the opposite is the case for no qualifications. For example, people with a degree have predicted life satisfaction scores 3 % lower in England than in the USA, whereas people with no qualifications have predicted life satisfaction scores 6 % higher in England than in the USA. In Fig 3, a more diagonal line for the USA compared with the UK indicates that SWB inequalities associated with education are greater in the USA. There is a differential association between life satisfaction, but not quality of life, and marital status in the USA and UK, which is strongest for those who are single and never married, and separated or divorced. Both groups report lower life satisfaction in England as compared with the USA, which is not the case for the married or cohabiting and widowed groups. A summary of the pooled model from ELSA and HRS is provided in the ‘Appendix’.
Discussion
The academic literature suggests that it is important to separate out the measurement of the conceptually different dimensions of hedonic well-being and eudemonic well-being [4–7]. This is because there are determinants that are specific to each dimension and therefore require different policy interventions to ensure equality in subjective well-being. This paper uses data from two samples of older adults in England and the USA and finds key determinants that are associated with variation in both hedonic life satisfaction and eudemonic quality of life. The paper also points to the SWB dimension-specific determinants and how the relative importance of the determinants differs between England and the USA. These are important findings to help evaluate effective country-specific policy responses.
The most consistent predictors of SWB in older age are health and wealth status. This finding brings together the evidence that supports the importance of health and wealth on both dimensions of SWB [10, 12, 15, 19, 22] and other studies that suggest changes in health and socioeconomic circumstances, linked to SWB [21]. Specifically, we find that those in poorer health, measured by physical functioning or diagnosed chronic conditions, are shown to have lower levels of life satisfaction and quality of life in both England and the USA. The same is true for those living in the poorest households as measured by household financial wealth. The causal pathways through which these effects operate are likely to have been built up during the life course as a result of reciprocal and multidimensional disadvantages, which manifest in health and wealth inequalities. The later life changes in health and socioeconomic circumstances that have been shown to predict declines in SWB [21] are likely themselves to be interrelated with cumulative disadvantages. This means that the policy interventions required to ensure everyone is able to live long, enjoyable and meaningful lives need to be substantial to counteract disparities in later life. More research is required to unpack these associations to help formulation of effective policy interventions and to determine whether changes in later life circumstances affect SWB.
Despite confirming the consistent effect of health and wealth, we find that the association with health status is strongest for quality of life in England and the USA. This suggests it is more difficult to find meaning and have control in one’s life when in poorer health than it is to enjoy and be satisfied with one’s life. It has been suggested previously that poor objective health may not have such an adverse effect on life satisfaction [12]. This is because people may evaluate the enjoyment and success in their life relative to their health status, and therefore, the presence of physical health conditions may not always mean people cannot be happy or satisfied with their life. Nonetheless, the evidence presented here indicates that functional limitations and chronic health conditions do have an effect, independent of other characteristics, on life satisfaction in England and the USA.
The effect of marital status is a more important determinant of life satisfaction than quality of life. Older adults who are separated or divorced have considerably lower levels of life satisfaction than those in a couple. Partnerships may provide the support to feel more positively about life, while being in a state of separation makes this more difficult even when taking into account health and wealth circumstances [19]. This suggests that those separated or divorced could benefit from formal and informal support to cope with what could be a traumatic event with a potentially long-term effect.
We provide some evidence to confirm our hypothesis that socioeconomic inequalities are more important in the USA as compared with England. The effect of years spent in education has a stronger effect in the USA where having a degree has a greater protective effect and having no qualifications has a more negative effect on both life satisfaction and quality of life. This suggests that efforts to counterbalance inequality in England (e.g. welfare benefits and free at the point of use public services) might help to ensure that educational inequalities are not felt so harshly.
Marital status has a differential association with life satisfaction across England and the USA. Older adults, who are single and never married, or separated or divorced, are shown to have lower life satisfaction in England compared with those in the USA. This may reflect a greater acceptance from family, peers and wider society of being voluntarily single in later life in the USA than in England. This does not mean there is no effect of being separated or divorced in the USA, because people in these groups are nevertheless more likely to report lower life satisfaction than those in a couple. It could be the case that older adults who are separated or divorced are not provided with the same level of support from their family and friends, which means they do not reflect as positively on their life and take enjoyment from it. Separated and divorced older adults might find it hard to draw on assistance from their children and other family because marriage dissolution is often perceived as a failure.
There are a number of limitations of this paper, which need to be set against the findings. The cross-sectional sample used means it is not possible to draw causal inference in the determinants that are found to be statistically significant. These effects are likely to be interrelated with more specific characteristics that we have not observed. We are limited by the availability of SWB measures in the internationally comparative datasets. As more data becomes available in ELSA and HRS, it will be possible to make longitudinal comparisons of SWB measures in England and the USA. We are also limited to comparable explanatory variables that are available in ELSA and HRS. We have used objective measures of demographic, socioeconomic and health status that are comparable in the two surveys rather than subjective measures, which have been found by Smith et al. [4] to explain more of the variance in SWB outcomes. Another limitation is the attrition of panel respondents who were sampled at baseline but did not respond to the wave in HRS and ELSA from which the SWB measures were collected. Sample weights were used to correct for non-response bias. A final limitation is that the determinants of SWB are likely to vary to a greater extent in countries that differ across cultural, political and economical domains than do England and the USA.
This paper makes two important contributions. First, it shows that there are consistent objective determinants of SWB across conceptually different outcomes in later life, including independent effects of health and wealth status. Policies are therefore most likely to be effective if they counterbalance these multiple disadvantages. The paper also shows that there are certain determinants that are more important for hedonic well-being measures, as indexed by life satisfaction, including being separated or divorced, and others are more important for eudemonic well-being, as indexed by a quality of life measure, including health. Second, the paper shows there are certain determinants whose importance varies across the USA and England, including education and marital status. This raises the potential for a more complete understanding of how national context and policy can influence subjective well-being outcomes and therefore how best to intervene to ensure these disparities are reduced.
References
Helliwell, J. F. (2003). How’s life? Combining individual and national variables to explain subjective well-being. Economic Modelling, 20(2), 331–360. doi:10.1016/S0264-9993(02)00057-3.
Shields, M., & Price, S. W. (2005). Exploring the economic and social determinants of psychological well-being and perceived social support in England. Journal of the Royal Statistical Society: Series A (Statistics in Society), 168(3), 513–537. doi:10.1111/j.1467-985X.2005.00361.x.
Chandola, T., Ferrie, J., Sacker, A., & Marmot, M. (2007). Social inequalities in self reported health in early old age: Follow-up of prospective cohort study. BMJ, 334(7601), 990. doi:10.1136/bmj.39167.439792.55.
Smith, A. E., Sim, J., Scharf, T., & Phillipson, C. (2004). Determinants of quality of life amongst older people in deprived neighbourhoods. Ageing and Society, 24(5), 793–814. doi:10.1017/S0144686X04002569.
Stanley, M., & Cheek, J. (2003). Well-Being and older People: A review of the literature. Canadian Journal of Occupational Therapy, 70(1), 51–59. doi:10.1177/000841740307000107.
Van Praag, B. M., Frijters, P., & Ferrer-i-Carbonell, A. (2003). The anatomy of subjective well-being. Journal of Economic Behavior & Organization, 51(1), 29–49. doi:10.1016/S0167-2681(02)00140-3.
Vanhoutte, B. (2014). The multidimensional structure of subjective well-being in later life. Journal of Population Ageing, 7(1), 1–20. doi:10.1007/s12062-014-9092-9.
Keyes, C. L. M., Shmotkin, D., & Ryff, C. D. (2002). Optimizing well-being: The empirical encounter of two traditions. Journal of Personality and Social Psychology. Keyes, Corey L. M.: Emory U, Dept of Sociology, Tarbutton Hall, Atlanta, GA, US, 30322, ckeyes@emory.edu: American Psychological Association. doi:10.1037/0022-3514.82.6.1007.
Ryff, C. D. (1989). Happiness is everything, or is it? Explorations on the meaning of psychological well-being. Journal of Personality and Social Psychology, 57(6), 1069.
Netuveli, G., Wiggins, R. D., Hildon, Z., Montgomery, S. M., & Blane, D. (2006). Quality of life at older ages: evidence from the English longitudinal study of aging (wave 1). Journal of Epidemiology and Community Health, 60(4), 357–363. doi:10.1136/jech.2005.040071.
Wiggins, R. D., Higgs, P. F. D., Hyde, M., & Blane, D. B. (2004). Quality of life in the third age: Key predictors of the CASP-19 measure. Ageing and Society, 24(5), 693–708. doi:10.1017/S0144686X04002284.
Jivraj, S., Nazroo, J., Vanhoutte, B., & Chandola, T. (2014). Aging and subjective well-being in later life. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences. doi:10.1093/geronb/gbu006.
Baird, B. M., Lucas, R. E., & Donnellan, M. B. (2010). Life satisfaction across the lifespan: Findings from two nationally representative panel studies. Social Indicators Research, 99(2), 183–203. doi:10.1007/s11205-010-9584-9.
Cheung, C., & Ngan, R. M. (2011). Filtered life satisfaction and its socioeconomic determinants in Hong Kong. Social Indicators Research, 109(2), 223–242. doi:10.1007/s11205-011-9897-3.
Meggiolaro, S. (2013). Life satisfaction among the elderly in Italy in a gender approach. Working Paper Series, N.6. Department of Statistical Science, University of Padua, Italy.
Degutis, M., & Urbonavicius, S. (2013). Determinants of subjective wellbeing in Lithuania. Inzinerine Ekonomika, 24(1), 111–118.
Vanhoutte, B., & Nazroo, J. (forthcoming). Cognitive, affective and eudemonic well-being in later life: Measurement equivalence over gender and life stage. Sociological Research Online.
Dolan, P., Peasgood, T., & White, M. (2008). Do we really know what makes us happy? A review of the economic literature on the factors associated with subjective well-being. Journal of Economic Psychology, 29(1), 94–122. doi:10.1016/j.joep.2007.09.001.
Cooper, C., Bebbington, P., King, M., Jenkins, R., Farrell, M., Brugha, T., et al. (2011). Happiness across age groups: results from the 2007 National Psychiatric Morbidity Survey. International Journal of Geriatric Psychiatry, 26(6), 608–614. doi:10.1002/gps.2570.
Helliwell, J. F. (2006). Well-being, social capital and public policy: What’s new? The Economic Journal, 116(510), C34–C45. doi:10.1111/j.1468-0297.2006.01074.x.
Webb, E., Blane, D., McMunn, A., & Netuveli, G. (2011). Proximal predictors of change in quality of life at older ages. Journal of Epidemiology and Community Health, 65(6), 542–547. doi:10.1136/jech.2009.101758.
Martinez-Martin, P., Prieto-Flores, M.-E., Forjaz, M. J., Fernandez-Mayoralas, G., Rojo-Perez, F., Rojo, J.-M., et al. (2012). Components and determinants of quality of life in community-dwelling older adults. European Journal of Ageing, 9(3), 255–263. doi:10.1007/s10433-012-0232-x.
National Institute on Aging. (2007). Growing Old in America: The Heath and Retirement Study (HRS Databook). Bethesda: National Institute on Aging.
Steptoe, A., Breeze, E., Banks, J., & Nazroo, J. (2012). Cohort Profile: The English Longitudinal Study of Ageing (ELSA). International Journal of Epidemiology. doi:10.1093/ije/dys168.
Cheshire, H., Cox, K., Lessof, C., & Taylor, R. (2006). Methodology. In J. Banks, E. Breeze, C. Lessof, & J. Nazroo (Eds.), Retirement, health and relationships of the older population in England: The 2004 English Longitudinal Study of Ageing (Wave 2) (pp. 367–383). London: Institute for Fiscal Studies.
Diener, E., Emmons, R., Larsen, R., & Griffin, S. (1985). The Satisfaction with Life Scale. Journal of Personality Assessment, 49(4), 71–75.
Pavot, W., & Diener, E. (2008). The Satisfaction with Life Scale and the emerging construct of life satisfaction. The Journal of Positive Psychology, 3(2), 137–152. doi:10.1080/17439760701756946.
Wiggins, R. D., Netuveli, G., Hyde, M., Higgs, P., & Blane, D. (2007). The evaluation of a self-enumerated scale of quality of life (CASP-19) in the context of research on ageing: A combination of exploratory and confirmatory approaches. Social Indicators Research, 89(1), 61–77. doi:10.1007/s11205-007-9220-5.
Higgs, P., Hyde, M., Wiggins, R., & Blane, D. (2003). Researching quality of life in early Old age: The importance of the sociological dimension. Social Policy & Administration, 37(3), 239–252. doi:10.1111/1467-9515.00336.
Acknowledgments
This research was supported by funding for the English Longitudinal Study of Ageing, which is provided by the National Institute of Aging (grants 2RO1AG7664-01A1 and 2RO1AG017644) and a consortium of UK government departments coordinated by the Office for National Statistics.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
Rights and permissions
About this article

Cite this article
Jivraj, S., Nazroo, J. Determinants of socioeconomic inequalities in subjective well-being in later life: a cross-country comparison in England and the USA. Qual Life Res 23, 2545–2558 (2014). https://doi.org/10.1007/s11136-014-0694-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-014-0694-8