
Abstract
This study investigated the lifetime prevalence of suicide attempts (SA) and independent demographic and clinical correlates in stabilized schizophrenia inpatients. A cross-sectional study was conducted in three psychiatric hospitals in Anhui province, an agricultural province located in east China. Psychopathology and depressive symptoms were assessed using the Positive and Negative Syndrome Scale (PANSS) and Hamilton Depression Rating Scale (HAMD), respectively. A total of 315 stable schizophrenia inpatients were interviewed prior to discharge. The lifetime prevalence of SA was 22.2%. Multiple logistic regression analysis revealed that female gender (P < 0.001, OR = 3.4, 95%CI: 1.9–6.0), being married (P = 0.02, OR = 2.2, 95%CI: 1.1–4.4) and having more severe depressive symptoms (P = 0.014, OR = 1.2, 95%CI: 1.01–1.3) were independently and significantly associated with higher risk of SA. Lifetime SA is common among hospitalized schizophrenia patients living in agricultural areas of China. For suicide prevention, regular assessments, appropriate interventions and clinical management should be integrated into a community-based psychiatric service model for this population.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Schizophrenia is a severe psychiatric disorder, with a high risk of suicidality [1, 2] and an approximate 10–20 years expected reduction in life expectancy [3,4,5]. Up to 40% [6] of premature mortality in schizophrenia could be attributed to suicide and other unnatural deaths. A meta-analysis found a suicide rate of 4.9% in people with schizophrenia [1]. A recent meta-analysis [7] reported that some factors contributing to suicidality in schizophrenia include male gender, being white, younger age, shorter illness length, poor adherence to treatment, high premorbid IQ, depressive symptoms, substance abuse and having a previous suicide attempt.
Suicidality is a multistage continuum that ranges from suicidal ideation (SI), as a key initial step, suicide attempts (SA), to final suicide [8]. SI refers to thoughts or wishes to die, and SA is defined as a self-destructive act that occurred at least once but did not result in death [9]. SI is a precursor of SA, and SA is a major predictor of later suicide; therefore, examining the pattern and correlates of SA is important in suicide prevention [10,11,12,13]. To date, most studies on SA in schizophrenia have been conducted in Western countries. With a different sociocultural and economic context, the risk factors for SA in Asian countries may be different and it is therefore important to conduct epidemiological studies of SA in different settings [14].
In China approximately 7.16 million people suffer from schizophrenia [15, 16] and SA is common in this population, with a range of prevalence estimates across studies [17,18,19,20,21,22]. For example, Zhang et al. [20] found the SA rate was 9.2% among hospitalized schizophrenia patients in Beijing. Another study [23] reported a 19.8% SA prevalence among schizophrenia inpatients in Sichuan province. A meta-analysis found that the pooled lifetime prevalence of SI and SA were 25.8% and 14.6% respectively in Chinese patients with schizophrenia [24]. However, most of these studies were conducted in big cities or economically developed areas, with scant data for agricultural areas.
Unlike in most developed countries, in China the de-hospitalization campaign never occurred. Hospital-based care has been and remains to be the mainstream mental health service. In order to help patients with severe mental illness re-enter the community, community-based mental care has started gaining attention. One important step was the initiation of a national community-based psychiatric service delivery model (the “686” project) in 2004. This service has integrated the resources of psychiatric hospitals and existing community health systems and provided individual service plans [25]. Approximately 4 million patients with schizophrenia have been registered in 31 provinces, municipalities and autonomous regions and of them, 88.7% received regular services by 2015 [26]. The current community-based psychiatric service model mainly focuses on the prevention of aggressive behaviours. However, the pattern and risk factors for suicidality, particularly SA, are not clear, although these are important in suicide prevention.
In this research project, we set out to examine the prevalence of SA and its demographic and clinical correlates in stabilized schizophrenia inpatients.
Methods
Patients and Study Sites
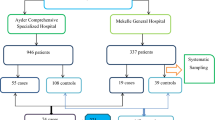
This was a multi-center, cross-sectional study conducted in three psychiatric hospitals between May and December, 2018 in Anhui province, an agricultural province located in east China with around 70.6 million population. Hospitalized patients in the participating hospitals were consecutively recruited prior to discharge if the following inclusion criteria were met: 1) aged 18 years or above; 2) a diagnosis of schizophrenia according to the ICD-10 [27] for at least 5 years; 3) clinically stable for at least one month; 4) able to provide informed consent and complete the assessment. Patients with major medical conditions were usually not admitted to psychiatric hospitals or departments, therefore any such patients were excluded from this study. The study protocol was approved in the Ethics Committee of Chaohu Hospital of Anhui Medical University. All patients provided written informed consent.
Data Collection
Basic demographic and clinical data were collected by a review of the medical records. The Positive and Negative Syndrome Scale (PANSS) [28] was used to measure psychotic symptoms, including “positive” (items P1, P3, P5, G9), “negative” (items N1, N2, N3, N4, N6 and G7), “cognitive” (items P2, N5, G11), “depression” (items G2, G3, G6) and “excitement” (items P4, P7, G8 and G14) factors [29, 30]. Depressive symptoms was assessed by the 17-item Hamilton Depression Rating Scale (HAMD) [31]. Four psychiatrists conducted the interview and the intra-class correlation coefficients of the above instruments across raters were > 0.8. Following other studies [19, 20], lifetime SA was inquired about by a standardized question: “did you ever attempt suicide?”. SA was also confirmed with family members. In addition, lifetime and current SIs were evaluated using the Chinese version of the 19-items Beck Suicide Ideation Scale (BSI-CV) [32].
Statistical Analysis
Analyses were performed using SPSS version 24.0 (SPSS Inc., Chicago, IL, USA). The normality of distribution of continuous variables was tested by the one-sample Kolmogorov-Smirnov test. Basic demographic and clinical characteristics between patients with and without SA were compared using either a t-test or the Mann–Whitney U test for continuous variables, and a χ2 test for categorical variables. Demographic and clinical correlates of SA were entered in a multiple logistic regression model. The independent variables for logistic regression were selected based on preliminary bivariate tests that distinguished patients with and without SA. All statistical tests were two-sided and a significance level of 0.05 was chosen.
Results
Altogether, 333 patients were invited to participate in the study; of them, 315 met the study criteria and completed the assessment, giving a participation rate of 94.6%. The lifetime prevalence of SA was 22.2% (95%CI: 17.6–26.8%) (70/315). Among patients with SA, 61.4% (43/70) attempted once, 24.3% (17/70) attempted twice, and 14.3% (10/70) attempted three times or more. The lifetime and current prevalence of SI in the whole sample was 36.8% (95%CI: 31.5–42.2%) and 6.4% (95%CI: 3.6–9.1%), respectively.
As shown in Table 1, patients with SA were more likely to be women, married and have more severe depressive symptoms. Multivariate analyses revealed that women (P < 0.001, OR = 3.4, 95%CI: 1.9–6.0), married status (P = 0.02, OR = 2.2, 95%CI: 1.1–4.4) and having more severe depressive symptoms (P = 0.014, OR = 1.2, 95%CI: 1.01–1.3) were significantly and independently associated with higher risk of SA (Table 2).
Discussion
To the best of our knowledge, this was the first multi-center study to examine the prevalence and independent demographic and clinical correlates of SA in clinically stable schizophrenia inpatients in China. We found that 22.2% (95%CI: 17.6–26.8%) of patients in the whole sample had lifetime SA, which is in the range of 18–55% reported previously [33,34,35], but was higher than the fig. (17.6%; 95%CI: 9.0–31.7%) reported in a recent meta-analysis in Chinese schizophrenia patients [24]. This lifetime prevalence of SI was 36.8% (95%CI: 31.5–42.2%), which is also higher than that in Dong et al’s meta-analysis (18.5%; 95%CI: 8.1–37.0%) [24]. There are several possible reasons for the higher SA in this study. First, the relatively underdeveloped economy in agricultural areas of China, such as Anhui province, may be associated with a higher risk for suicidality including SA [36]. Second, discrimination and stigma may be more pronounced in agricultural areas, which would make schizophrenia patients less likely to seek help, making them more isolated and depressed and at higher risk for suicidality [37].
Gender is usually associated with suicidality. We found that the risk for SA was 3.3 times higher in women than in men, which is consistent with findings in the Chinese general population [14]. Some studies found that men are more likely to die from suicide, whereas SAs not resulting in death and suicidal ideation are more common in women [38,39,40,41]. However, other studies have also reported higher suicide deaths among women in China compared to men [42, 43] but a systematic review reported that the gender difference in suicide deaths has disappeared since 2000 [44]. Certain sociocultural factors associated with female patients, such as lower economic and social status, more severe discrimination and stigma, and frequent family conflicts [45, 46], may account for the higher risk of suicidality. Women usually undertake housework at home in Chinese society, particularly in agricultural areas. Due to the impact of psychiatric symptoms and drug-induced side effects, their ability to perform housework may be impaired, which could lead to family conflicts and then increase the risk of suicidality. Women’s responsibility for housework has also been cited as a reason for shorter hospitalizations among women who require inpatient mental healthcare compared to men [47]. This may result in sub-optimal treatment outcomes, thereby increasing suicide risk.
In this study married patients were more likely to have SA, which is consistent with previous findings in community-dwelling patients with schizophrenia in China [19]. Being married is usually an indicator of better social functioning in Western societies due to family support [48, 49]. This may not be true in China where it was reported that unmarried females received greater social support than married counterparts because of their contact with teachers or supervisors and colleagues [50]. It may also be the case that initially well-connected and highly functioning people tend to develop a sense of hopelessness after getting mentally ill, possibly because of “losing face” or shame [19, 51, 52]. As expected, more severe depressive symptoms were associated with more frequent SA [18,19,20, 53].
The strengths of this study include the multicenter design and the inclusion of patients prior to discharge in agricultural areas of China. However, several limitations needed to be addressed. First, given the cross-sectional design, no causal relationship between SA and demographic and clinical variables can be inferred. Second, only psychiatric hospitals in Anhui were involved; therefore, the findings cannot be generalized to other agricultural areas of China. Finally, due to the stigma related to psychiatric disorders [54], SAs might be concealed by some patients and families, which could underestimate SA rate.
In conclusion, this study found that SA was common in stable schizophrenia inpatients in agricultural areas of China, particularly in female patients, married people, and those who had more severe depressive symptoms. In order to reduce the risk of suicide, regular assessment and appropriate interventions and management approaches on suicide prevention should be integrated into the community-based psychiatric service model for this population.
References
Palmer BA, Pankratz VS, Bostwick JM. The lifetime risk of suicide in schizophrenia: a reexamination. Arch Gen Psychiatry. 2005;62(3):247–53.
Fialko L, Freeman D, Bebbington PE, Kuipers E, Garety PA, Dunn G, et al. Understanding suicidal ideation in psychosis: findings from the psychological prevention of relapse in psychosis (PRP) trial. Acta Psychiatr Scand. 2006;114(3):177–86. https://doi.org/10.1111/j.1600-0447.2006.00849.x.
Chesney E, Goodwin GM, Fazel S. Risks of all-cause and suicide mortality in mental disorders: a meta-review. World Psychiatry. 2014;13(2):153–60. https://doi.org/10.1002/wps.20128.
Nordentoft M, Mortensen PB, Pedersen CB. Absolute risk of suicide after first hospital contact in mental disorder. Arch Gen Psychiatry. 2011;68(10):1058–64. https://doi.org/10.1001/archgenpsychiatry.2011.113.
Tiihonen J, Lonnqvist J, Wahlbeck K, Klaukka T, Niskanen L, Tanskanen A, et al. 11-year follow-up of mortality in patients with schizophrenia: a population-based cohort study (FIN11 study). Lancet. 2009;374(9690):620–7. https://doi.org/10.1016/S0140-6736(09)60742-X.
Bushe CJ, Taylor M, Haukka J. Mortality in schizophrenia: a measurable clinical endpoint. J Psychopharmacol. 2010;24(4 Suppl):17–25. https://doi.org/10.1177/1359786810382468.
Cassidy RM, Yang F, Kapczinski F, Passos IC. Risk factors for Suicidality in patients with schizophrenia: a systematic review, meta-analysis, and meta-regression of 96 studies. Schizophr Bull. 2018;44(4):787–97. https://doi.org/10.1093/schbul/sbx131.
Kessler RC, Borges G, Walters EE. Prevalence of and risk factors for lifetime suicide attempts in the National Comorbidity Survey. Arch Gen Psychiatry. 1999;56(7):617–26.
Kasckow J, Felmet K, Zisook S. Managing suicide risk in patients with schizophrenia. CNS Drugs. 2011;25(2):129–43. https://doi.org/10.2165/11586450-000000000-00000.
De Leo D, Cerin E, Spathonis K, Burgis S. Lifetime risk of suicide ideation and attempts in an Australian community: prevalence, suicidal process, and help-seeking behaviour. J Affect Disord. 2005;86(2–3):215–24.
Drake RE, Gates C, Whitaker A, Cotton PG. Suicide among schizophrenics: a review. Compr Psychiatry. 1985;26(1):90–100.
Harkavy-Friedman JM, Restifo K, Malaspina D, Kaufmann CA, Amador XF, Yale SA, et al. Suicidal behavior in schizophrenia: characteristics of individuals who had and had not attempted suicide. A. J Psychiatry. 1999;156(8):1276–8.
Kessler RC, Berglund P, Borges G, Nock M, Wang PS. Trends in suicide ideation, plans, gestures, and attempts in the United States, 1990-1992 to 2001-2003. JAMA. 2005;293(20):2487–95.
Cao X-L, Zhong B-L, Xiang Y-T, Ungvari GS, Lai KY, Chiu HF, et al. Prevalence of suicidal ideation and suicide attempts in the general population of China: a meta-analysis. Int. J. Psychiatry Med. 2015;49(4):296–308.
Phillips MR, Zhang J, Shi Q, Song Z, Ding Z, Pang S, et al. Prevalence, treatment, and associated disability of mental disorders in four provinces in China during 2001-05: an epidemiological survey. Lancet. 2009;373(9680):2041–53.
Chan KY, Zhao FF, Meng S, Demaio AR, Reed C, Theodoratou E, et al. Prevalence of schizophrenia in China between 1990 and 2010. J Glob Health. 2015;5(1):010410. https://doi.org/10.7189/jogh.05.010410.
Zoghbi AW, Al Jurdi RK, Deshmukh PR, Chen DC, Xiu MH, Tan YL, et al. Cognitive function and suicide risk in Han Chinese inpatients with schizophrenia. Psychiatry Res. 2014;220(1–2):188–92. https://doi.org/10.1016/j.psychres.2014.07.046.
Xiang YT, Weng YZ, Leung CM, Tang WK, Ungvari GS. Socio-demographic and clinical correlates of lifetime suicide attempts and their impact on quality of life in Chinese schizophrenia patients. J Psychiatr Res. 2008;42(6):495–502.
Yan F, Xiang YT, Hou YZ, Ungvari GS, Dixon LB, Chan SS, et al. Suicide attempt and suicidal ideation and their associations with demographic and clinical correlates and quality of life in Chinese schizophrenia patients. Soc Psychiatry Psychiatr Epidemiol. 2013;48(3):447–54. https://doi.org/10.1007/s00127-012-0555-0.
Zhang XY, Al Jurdi RK, Zoghbi AW, Chen DC, Xiu MH, Tan YL, et al. Prevalence, demographic and clinical correlates of suicide attempts in Chinese medicated chronic inpatients with schizophrenia. J Psychiatr Res. 2013;47(10):1370–5. https://doi.org/10.1016/j.jpsychires.2013.05.024.
Ran MS, Xiang MZ, Mao WJ, Hou ZJ, Tang MN, Chen EY, et al. Characteristics of suicide attempters and nonattempters with schizophrenia in a rural community. Suicide Life Threat Behav. 2005;35(6):694–701.
Gao Q, Fan H, Di F, Xia X, Long H, Zhu H. Suicide behaviors in adult inpatients with mental disorders in Beijing, China. Int J Environ Res Public Health. 2017;14(3). https://doi.org/10.3390/ijerph14030259.
Yang KJ, Xiao SY, Li XW, Liao CP, Lai J. Comparative study of schizophrenic patients who committed suicide or self-injurious behaviours during hospitalization. Sichuan Mental Health. 2015;28(05):430–5.
Dong M, Wang SB, Wang F, Zhang L, Ungvari GS, Ng CH, et al. Suicide-related behaviours in schizophrenia in China: a comprehensive meta-analysis. Epidemiol Psychiatr Sci. 2017:1–10. https://doi.org/10.1017/S2045796017000476.
Xiang YT, Yu X, Sartorius N, Ungvari GS, Chiu HF. Mental health in China: challenges and progress. Lancet. 2012;380(9855):1715–6. https://doi.org/10.1016/S0140-6736(11)60893-3.
Xiang YT, Ng CH, Yu X, Wang G. Rethinking progress and challenges of mental health care in China. World Psychiatry. 2018;17(2):231–2. https://doi.org/10.1002/wps.20500.
World Health Organisation. ICD-10 Classifications of Mental and Behavioural Disorder: Clinical Descriptions and Diagnostic Guidelines. Geneva 1992.
Kay SR, Opler LA, Lindenmayer JP. Reliability and validity of the positive and negative syndrome scale for schizophrenics. Psychiatry Res. 1988;23(1):99–110.
Wallwork RS, Fortgang R, Hashimoto R, Weinberger DR, Dickinson D. Searching for a consensus five-factor model of the positive and negative syndrome scale for schizophrenia. Schizophr Res. 2012;137(1–3):246–50. https://doi.org/10.1016/j.schres.2012.01.031.
Rodriguez-Jimenez R, Bagney A, Mezquita L, Martinez-Gras I, Sanchez-Morla EM, Mesa N, et al. Cognition and the five-factor model of the positive and negative syndrome scale in schizophrenia. Schizophr Res. 2013;143(1):77–83. https://doi.org/10.1016/j.schres.2012.10.020.
Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960;23:56–62.
Beck AT, Kovacs M, Weissman A. Assessment of suicidal intention: the scale for suicide ideation. J Consult Clin Psychol. 1979;47(2):343–52.
Fenton WS, McGlashan TH, Victor BJ, Blyler CR. Symptoms, subtype, and suicidality in patients with schizophrenia spectrum disorders. A J Psychiatry. 1997;154(2):199–204.
Sorenson SB, Knight K. Suicide in schizophrenia. J Clin Psychiatry. 1986;47(11):570–1.
Bolton C, Gooding P, Kapur N, Barrowclough C, Tarrier N. Developing psychological perspectives of suicidal behaviour and risk in people with a diagnosis of schizophrenia: we know they kill themselves but do we understand why? Clin Psychol Rev. 2007;27(4):511–36. https://doi.org/10.1016/j.cpr.2006.12.001.
Iemmi V, Bantjes J, Coast E, Channer K, Leone T, McDaid D, et al. Suicide and poverty in low-income and middle-income countries: a systematic review. Lancet Psychiatry. 2016;3(8):774–83. https://doi.org/10.1016/S2215-0366(16)30066-9.
Rusch N, Zlati A, Black G, Thornicroft G. Does the stigma of mental illness contribute to suicidality? Br J Psychiatry. 2014;205(4):257–9. https://doi.org/10.1192/bjp.bp.114.145755.
Canetto SS. Meanings of gender and suicidal behavior during adolescence. Suicide Life Threat Behav. 1997;27(4):339–51.
Weissman MM, Bland RC, Canino GJ, Greenwald S, Hwu HG, Joyce PR, et al. Prevalence of suicide ideation and suicide attempts in nine countries. Psychol Med. 1999;29(1):9–17.
Nock MK, Borges G, Bromet EJ, Alonso J, Angermeyer M, Beautrais A, et al. Cross-national prevalence and risk factors for suicidal ideation, plans and attempts. Br J Psychiatry. 2008;192(2):98–105. https://doi.org/10.1192/bjp.bp.107.040113.
Canetto SS, Sakinofsky I. The gender paradox in suicide. Suicide Life Threat Behav. 1998;28(1):1–23.
Phillips MR, Li X, Zhang Y. Suicide rates in China, 1995-99. Lancet. 2002;359(9309):835–40.
Yip PS, Liu KY. The ecological fallacy and the gender ratio of suicide in China. Br J Psychiatry. 2006;189:465–6. https://doi.org/10.1192/bjp.bp.106.021816.
Li Y, Li Y, Cao J. Factors associated with suicidal behaviors in mainland China: a meta-analysis. BMC Public Health. 2012;12:524. https://doi.org/10.1186/1471-2458-12-524.
Law S, Liu P. Suicide in China: unique demographic patterns and relationship to depressive disorder. Curr Psychiatry Rep. 2008;10(1):80–6.
Phillips MR, Yang G, Li S, Li Y. Suicide and the unique prevalence pattern of schizophrenia in mainland China: a retrospective observational study. Lancet. 2004;364(9439):1062–8.
Weiyuan C. Women and suicide in rural China. Bull World Health Organ. 2009;87(12):888–9. https://doi.org/10.2471/BLT.09.011209.
Isaac M, Chand P, Murthy P. Schizophrenia outcome measures in the wider international community. Br J Psychiatry Suppl. 2007;50:s71–7.
Ran MS, Wong YI, Yang SY, Ho PS, Mao WJ, Li J, et al. Marriage and outcomes of people with schizophrenia in rural China: 14-year follow-up study. Schizophr Res. 2017;182:49–54. https://doi.org/10.1016/j.schres.2016.10.034.
Zhang J. Marriage and suicide among Chinese rural young women. Soc Forces. 2010;89(1):311–26. https://doi.org/10.1353/sof.2010.0065.
Black DW, Winokur G. Age, mortality and chronic schizophrenia. Schizophr Res. 1988;1(4):267–72.
Warnes H. Suicide in schizophrenics. Dis Nerv Syst. 1968;29(5):Suppl):35–40.
Altamura AC, Bassetti R, Bignotti S, Pioli R, Mundo E. Clinical variables related to suicide attempts in schizophrenic patients: a retrospective study. Schizophr Res. 2003;60(1):47–55.
Yang LH, Kleinman A. 'Face' and the embodiment of stigma in China: the cases of schizophrenia and AIDS. Soc Sci Med. 2008;67(3):398–408. https://doi.org/10.1016/j.socscimed.2008.03.011.
Acknowledgements
The study was supported by the National Natural Science Foundation of China (No. 81771449), the Anhui Province Key Scientific and Technological Projects (1804 h08020263).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of Interest
The authors have no conflicts of interest concerning this article.
Human and Animal Rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
NA.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Zhong, Y., Xia, L., Zhao, TT. et al. The Prevalence of Suicide Attempts and Independent Demographic and Clinical Correlates among Chronic Schizophrenia Patients in Agricultural Areas of China. Psychiatr Q 90, 683–691 (2019). https://doi.org/10.1007/s11126-019-09644-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11126-019-09644-1