
Abstract
Evidence of the effectiveness of programs to change gendered social norms related to intimate partner violence (IPV) is growing, but their potential to significantly impact actual occurrence of IPV at population level is lacking. We study whether modest changes in gendered social norms related to wife-beating can result in significant changes in the incidence of emotional, physical, and sexual IPV among ever married women in Uganda. We employ an imputation-based causal inference approach, based on nationally representative Demographic Health Survey data. The steps are (1) model the association between adjusted neighborhood norms and experiences of IPV using a random effects logistic regression model, (2) impute unobserved counterfactual probabilities of experiencing IPV for each woman while manipulating her neighborhood norms by setting it to different values, (3) average the probabilities across the population, and (4) bootstrap confidence intervals. Results show that statistically significant inverse associations between more prohibitive neighborhood IPV norms and women’s experiences of different forms of IPV at the population level exist. The effect is however small, that even if an entire community disapproves of wife-beating, incidence of IPV falls by about 10 percentage points to 48.5% (95% CI 46.0%–50.9%) from the observed value of 57.6% (95% CI 55.2%–59.9%). Furthermore, changes in neighborhood social norms are found to have no statistical significant effect on the incidence of sexual violence. In conclusion, changing gendered social norms related to wife-beating will not result in significant reductions in different forms for IPV at the population level.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Intimate partner violence (IPV), which includes the threats or actual infliction of physical, sexual, or emotional/psychological abuse, has negative consequences for public health globally, with pervasive societal and clinical implications for women, children, and men from all backgrounds. In particular, IPV is associated with adverse health outcomes among affected women (Campbell 2002; Ellberg et al. 2008; Pallitto et al. 2005; Tsai 2013). As such, women who experience any of the forms of IPV during pregnancy have increased chances of sexually transmitted infections, vaginal bleeding, miscarriage, and premature rupture of membranes and are more likely to deliver infants who are low birth weight or preterm (Biswas et al. 2015; Johri et al. 2011; Sharps et al. 2007; Tsai et al. 2016). Women who experience sexual IPV, which includes being forced to have sexual intercourse or perform any sexual acts against their will, may have limited ability to protect themselves from sexually transmitted infections or unwanted pregnancies. Children who witness IPV within their homes or neighborhoods have been reported to have increased odds of experiencing or perpetrating physical, emotional, and sexual violence within their formative years (Chan 2015; Devries et al. 2017; Widom et al. 2014).
Yet IPV remains unacceptably prevalent. Globally, an estimated 30% of women report to have ever experienced physical and/or sexual violence by an intimate partner in their lifetime and this is the highest among women in the WHO African, Eastern Mediterranean, and Southeast Asia regions at 37% (Devries et al. 2013; WHO 2013). In Uganda, despite a favorable policy environment to protect women with the introduction of the Domestic Violence Act of 2010, IPV prevalence remains very high; 60% of ever married women aged 15–49 years report having ever experienced physical, emotional, or sexual violence by an intimate partner during their lifetime and 45% experienced at least one of these three forms of IPV in the 12 months preceding the survey (UBOS and ICF International 2012). Notably, there has been a stable and unacceptably high prevalence of lifetime sexual IPV among ever married Ugandan women in the past decade with its prevalence estimated at 24.8% in 2006, 28% in 2011, and most recently at 22% in 2016 (UBOS and ICF International 2012, 2017; UBOS and Macro International 2007).
Strong evidence exists that neighborhood social norms about the roles and behavior of men and women contribute to an increased level of IPV in various settings (Devries et al. 2013; Jewkes 2002; Linos and Kawachi 2012; Shakya et al. 2016; Tsai et al. 2017). Given the importance of social norms, such as male masculinity and female subordination in shaping acceptable behavior within communities, several programs aimed at shifting norms and behavior around IPV have been implemented across Africa, Asia, Central America, and the Middle East (Heise 2011). In Uganda, for example, the SASA! Project, a community mobilization project designed to transform gender relations and power dynamics, reduced social acceptability of IPV (Abramsky et al. 2014; Kyegombe et al. 2014; Raising Voices, LSHTM,, and CEDOVIP 2015), and consequently, it has been replicated in over 15 other countries. The general strategy of the SASA! Project and several of its variants is to bring about changes in social norms through local activism, media, use of communication materials and community-based edutainment/theater and advocacy in order to reduce the social acceptability of IPV (Heise 2011; Niolon et al. 2017).
Although evidence for the effectiveness of programs like SASA! to shift gendered norms, attitudes, and beliefs related to IPV is growing, their potential to significantly impact the actual occurrence of IPV in a general population still requires rigorous evaluation for several reasons. Firstly, findings from these IPV prevention trials/programs primarily rely on self-reported changes in gendered social beliefs and norms among members of neighborhoods where the programs are being implemented. This measure can be strongly influenced by social desirability bias. Secondly, if changes in social norms indeed influence behavior, it is unknown whether these changes differentially affect the three forms of IPV: physical, emotional, and sexual. Thirdly, rates of justifying wife-beating have been used as indicators for prevalence of IPV at the community level. However, changes in this measure at a community level do not inform to what extent it translates to a reduction of IPV at the population level. This is important to inform national policy and development partners about whether it is worthwhile to invest in programs to change gendered social norms and whether such changes can translate to actual reductions in IPV.
In the present paper, we use a simulation study based on data from a nationally representative population-based household survey, the 2011 Uganda Demographic Health Survey (UDHS), in which different levels of interventions to change gendered norms related to wife-beating are hypothesized. We apply causal inference methods to evaluate the potential effects of modest changes in the level of social acceptance of wife-beating within neighborhoods on the prevalence of sexual, emotional, and physical IPV—among ever married women. In particular, we determine the population average causal effect which is the difference in the prevalence of IPV that would be observed in the population if there had been an intervention to change gendered social norms related to wife-beating at the neighborhood level, as opposed to if there was no programmatic intervention. Studies that assess how a potential intervention on an exposure at the individual-level or neighborhood-level might change disease burden across the population are well-documented (Ahern et al. 2009; Rockhill 2005; Rose 2001). This approach to our research question enables us to understand whether modest changes in gendered social norms related to wife-beating within neighborhoods could result in significant changes in the prevalence of different forms of IPV at the population level. Results from this study will also help us understand whether community-based programs/interventions to change social norms are worthwhile investments.
Data and Methods
Data Source and Structure
We analyzed data from a nationally representative population-based household survey, the 2011 UDHS. The survey utilized a two-stage stratified sample design. Stratification was achieved by separating each of the 10 statistical regions into urban and rural areas. The first stage involved selecting 405 enumeration areas or clusters from the census-sampling frame—119 in urban areas and 286 in rural areas. The second stage of selection involved the systematic sampling of 30 households per cluster from a list of households in each cluster. A total of 12,150 households (3570 in urban areas and 8580 are in rural areas) were selected to participate in the entire survey. However, the domestic violence module was implemented only in a subsample of these households resulting in a total of 2056 (1705 ever married) women aged 15–49 years and 1730 (1211 ever married) men aged 15–54 years who completed the domestic violence module. To maintain confidentiality, only one consenting woman or man per household was administered the questions on gender violence. Data collection was carried out from May through December 2011.The detailed sampling criteria is described elsewhere (UBOS and ICF International 2012).
Sample and Study Variables
The primary geographic unit at the second stage of sample—the cluster—was used as neighborhood unit of analysis in the present study. We retained neighborhoods in which at least 5 households completed the domestic violence module and which have a representation of both males and females as responders to the domestic violence module. For the present study, the final dataset consisted of 392 neighborhoods (i.e., 96.8% of total 2011 UDHS cluster size) with a median of 10 and a maximum of 15 households per neighborhood. The remaining number of respondents, that is, 3731 (2017 females and 1714 males) constituted the final sample size for computation of IPV acceptability in the neighborhood.
The neighborhood measure of IPV acceptability, the exposure variable of interest, was computed as the proportion of both male and female respondents in each neighborhood who believed that there was no justification for a woman to be beaten by her husband under any of the circumstances provided. Specifically, respondents were asked whether or not beating one’s wife was justified under these five circumstances:
-
1.
Wife goes out without telling husband.
-
2.
Wife neglects the children.
-
3.
Wife argues with husband.
-
4.
Wife refuses to have sex with husband.
-
5.
Wife burns the food.
A respondent who responded with “no” to each of the five items was considered not to justify IPV under any circumstance and was assigned a score of “1”. If a respondent answered “yes” or “do not know” to at least one of the five items, a score of “0” was assigned. The proportion of respondents who did not justify IPV under any circumstance was computed in three ways: for both males and females combined, for females only, and for males only. These are hereafter referred to as prohibitive neighborhood IPV norms.
To estimate the prevalence of IPV, the primary outcome, information was obtained from each ever married female respondent of the domestic violence module, on her experiences of violence committed by current and former spouses using a scale of items under the themes of physical, sexual, and emotional violence. A respondent who answered “yes” to any of the provided questions was considered to have an experience of a specific form of IPV. Women’s experiences of physical, emotional, sexual, or any one of these from of IPV was each studied separately. For a detailed description of these items, see UDHS report, p.240 (UBOS and ICF International 2012).
We also extracted women-level background characteristics to be included in the statistical analyses as covariates, namely, women’s residence (urban or rural), age at time of survey (15–49 years), number of living children (none, 1–2, 3–4, 5+), religion (Catholic, Protestant, Pentecostal, Seventh-day Adventist, Muslim/other), wealth index quintiles (poorer, poor, middle, richer, richest), level of education (none, primary, secondary+), and marital status (whether presently or formerly in union).
Statistical Analysis Approach
The major objective of the present paper is to examine how the distribution of the three forms of IPV would be different in the population if we were able to change gendered social norms related to wife-beating within neighborhoods (e.g., due to a hypothetical intervention). However, we are missing counterfactual observations, because each woman’s outcome can only be recorded under one exposure state. One solution to this problem is to use an imputation-based causal inference method called the “g-computation algorithm”, an approach that has been thoroughly discussed in statistical and social epidemiological literature (Ahern et al. 2009; Gutman and Rubin 2013; Lanza et al. 2013; Westreich et al. 2015).
To answer this question, we adopted an imputation-based causal inference approach following the same step-by-step approach by Ahern et al. (2009) to impute unobserved counterfactual probabilities of experiencing IPV by assuming that neighborhood norms related to wife-beating have a direct causal effect on IPV at the population level. Here, imputation is used to fill in “missing” counterfactual observations of women’s experiences of IPV, as observed in only one exposure state of neighborhood norms, in order to estimate changes in the prevalence of different forms of IPV, in consideration of some potential interventions to change neighborhood norms. These probabilities are estimated by “setting” or fixing the neighborhood norms to different levels that correspond to the range of observed data. The unobserved counterfactual probability of experiencing a specific form of IPV given a neighborhood social norm level that a particular woman did not experience can be thought of as missing data. As such, we can impute each woman’s probability of experiencing a specific form of IPV if she had experienced a social norm value that she did not experience to estimate the missing counterfactuals. For a more detailed description of the analytic approach, we refer to Ahern et al. (2009).
In the first step, we estimated the association between the exposure variable (i.e., prohibitive neighborhood IPV norms computed as the proportion of respondents who did not justify IPV against women under any of the given 5 circumstances) and the outcomes of interest—that is, women’s experiences of physical, emotional, sexual, or any of the three forms of IPV. For this step, we fitted a random effects logistic regression model to the 2011 UDHS dataset, adjusting for women’s background characteristics with neighborhoods (clusters) as random intercepts. That is, if Y = yni is an observed binary indicator of woman i experiencing IPV in neighborhood n, then the corresponding estimated probability is given by a random effects logistic regression model as
where β0, β1, and βq are unknown regression coefficients respectively for the intercept, prohibitive neighborhood IPV norms, and the observed background characteristic wq of woman i; for q = 1, … . , Q; β1q is the unknown regression coefficient for the interaction term between neighborhood IPV norms and a woman characteristic wq; and β0n is the random intercept for neighborhood n from a normal distribution with \( {\beta}_{0n}\sim N\left(0,{\sigma}_0^2\right) \).
In the second step, we used the model from step 1 to impute the probabilities of experiencing the three forms of IPV for each woman in the dataset under a range of counterfactual levels of prohibitive neighborhood IPV norms. These probabilities were imputed by setting prohibitive neighborhood IPV norm values across the entire range of observed proportions 0 (everyone in the neighborhood believes IPV is justifiable) to 100% (no one in the neighborhood believes IPV is justifiable) in 5 percentage interval points. Each woman’s unobserved probability of experiencing IPV under these counterfactual scenarios was imputed based on her individual background characteristics (W = wi) and a “set” IPV norms’ value in the neighborhood (A = an) in which that woman belongs. This unobserved counterfactual probability of experiencing IPV was imputed by assuming that prohibitive neighborhood IPV norms at \( \mathcal{A} \) “set” levels may have a causal effect on IPV at population level, adjusted for women’s background characteristics W. The model is then given as:
where \( \mathcal{A} \) is a “set” of prohibitive neighborhood norms, W are observed background women characteristics, and Ya are counterfactuals of IPV, which would have been observed at “set” prohibitive neighborhood IPV norm levels \( {a}_n\in \mathcal{A}=\left(0,1\right) \). The imputed probability of experiencing IPV by each woman i in the neighborhood n when its proportion of prohibitive norms is “set” at an is then computed as
where Lni = (β0 + β0n) + β1(an − a0) + β2 + … + βQ is the corresponding imputed log odds of experiencing IPV and an − a0 is difference between the set neighborhood IPV proportion an for which a probability of experiencing IPV is to be imputed and the average proportion of all neighborhood norms at population level a0.
In the third step, we averaged imputed probabilities of each form of IPV for each individual across the whole population, in order to obtain the population-level predicted effect of changing IPV norm levels on the prevalence of IPV in the whole population. Lastly, in the fourth step, we computed 95% confidence intervals around the estimate of the population-level prevalence of IPV using bootstrapping techniques. In the present study, each imputed probability for each set level of neighborhood norms was resampled from the study population with replacement 200 times (a moderate number due to computational time needed by random effects models) in order to capture a sampling distribution from which we calculated a corresponding standard error. A more detailed step-by-step approach of this causal inference methodology is described elsewhere (Ahern et al. 2009). Data manipulation and exploration were implemented in STATA 15 (StataCorp LLC 2017) while model fitting, imputation, and bootstrap steps were done R 3.4.1 (R Core Team 2017).
Results
Table 1 shows the percentage of ever married women who experienced various forms of IPV by their current or former spouse/partner over the course of their intimate relationship. Overall, 57.5% of women reported to have experienced at least one form of IPV; 41% experienced both physical and emotional while 27% had ever experienced sexual forms of IPV. These figures indicate that different forms of violence are not mutually exclusive and show that women were likely to report having experienced multiple forms of IPV. Specifically, women who were older, formerly in union, residing in rural areas, with many living children, with no formal education, and in lower quintiles of wealth index reported higher prevalence of either physical, emotional, sexual, or any one of these forms of IPV.
We hypothesized an interaction between neighborhood IPV norms and women characteristics of marital status, place of residence, and number of living children. However, we found no statistically significant associations between prevalence of different forms of IPV and these interaction terms and were therefore not included in the final model. Table 2 shows adjusted log odds estimates from random effects logistic regression models of the association between neighborhood IPV norms (coded in three ways: both men and women, women only, and men only) and the prevalence of different forms of IPV (physical, emotional, sexual, or any form of IPV), obtained in step 1 of the four-step analysis approach. We found an inverse association between more prohibitive neighborhood IPV norms and women’s experiences of physical, emotional, sexual, or any forms of IPV. Notably, this association was statistically significant if prohibitive neighborhood IPV norms were among both men and women combined. Similar inverse associations were observed between prohibitive neighborhood IPV norms among women only and women’s experiences of physical, emotional, sexual, or any form of IPV.
However, more prohibitive neighborhood IPV norms among men alone were not significantly associated with women’s experiences of all forms of IPV. Specifically, whereas results revealed a nonsignificant inverse relationship between prohibitive neighborhood IPV norms among males and women’s experiences of physical, emotional, or any form of IPV; this was not the case for experiences of sexual violence where the effect was positive and significant (β = 0.89; 95% CI 0.08, 1.71).
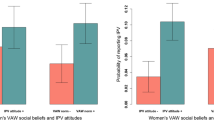
We then assessed the effect of a potential intervention to change prohibitive neighborhood IPV norms on the prevalence of the different forms of IPV at the population level. Results from steps 2, 3, and 4 in the “Data and Methods” section are given in Table 3 and Fig. 1. Table 3 shows the imputed prevalence of different forms of IPV when prohibitive neighborhood norms for both males and females were set at 0%, 25%, 50%, 75%, and 100%. When prohibitive neighborhood IPV norms for both men and women were set at their highest level (no one justifies of violence against women) in all neighborhoods, the imputed prevalence of any form of IPV experienced by women in the whole population was reduced to 48.5% (95% CI 46.0%–50.9%) from the observed prevalence of 57.6% (95% CI 55.2%–59.9%). When prohibitive IPV norms were set at their lowest level (everyone justifies violence against women) in all neighborhoods, the imputed prevalence of IPV in the whole population increased to 70%. Similar trends were observed for all three forms of IPV. Figure 1 presents the bootstrapped 95% confidence intervals for the imputed IPV prevalence for all possible “set” proportions of prohibitive neighborhood IPV norms among both men and women.

Predicted prevalence of different forms of IPV corresponding to set levels of prohibitive neighborhood IPV norms for both men and women
Discussion and Conclusion
In the present paper, we study whether modest changes in gendered social norms related to justification or acceptance of wife-beating within neighborhoods would result in significant changes in the prevalence of different forms of intimate partner violence (IPV) at the population level in Uganda. Using a casual inference approach, we examined what levels of experiencing sexual, emotional, physical, or any of these forms of IPV would be, by manipulating social norms related to justification or acceptance of wife-beating in neighborhoods, on the assumption that these norms have a direct causal effect on experiences of IPV at population level. Our goal was to understand whether programs that aim to change social norms within neighborhoods influence IPV behavior, and if so, whether that association is strong enough to significantly change women’s experience of IPV.
Obtained results showed statistically significant inverse associations between more prohibitive neighborhood IPV norms for men and women combined or only among women and women’s experiences of different forms of IPV under study. Furthermore, although our analysis shows that more prohibitive neighborhood IPV social norms related to wife-beating result in statistically significant reductions in incidence of IPV at the population level, the effect is rather small. Simulation results show that even in extreme hypothetical situations where everyone on the community disapproves of wife-beating as a social norm, the incidence of any form of IPV will only fall by about 10 percentage points. This finding is not in isolation. In a recent analysis of IPV data from 30 Sub-Saharan African countries by Cools and Kotsadam (2017), it was reported that incidence of IPV and the acceptance of wife-beating vary synchronously across both time and space. They show that communities and/or time periods with record lower levels of acceptance of wife-beating (i.e. more prohibitive IPV norms) have lower levels of IPV incidence and vice versa, but these effects are not substantially different between different communities.
From a policy and programming perspective, the implication of these findings is that community-based interventions such as SASA! designed to change gendered social norms may not cause significant reductions in different forms for IPV at the population level. In fact, it has been explained that IPV is a function of social ecology including individuals’ life histories, traumatic scars, and day-to-day contextual factors, as well as norms that friends, family members, and social institutions reinforce as appropriate behavior among men and women (Abramsky et al. 2014; Heise 2011; Kyegombe et al. 2014). Therefore, it is important for strategies for reducing gendered social norms related IPV to incorporate a wider range of individual, household, community, institutional, and societal factors that view violence in the family as unacceptable and that can be acted on in order to contribute to generational efforts to eliminate IPV. Scientifically proven interventions such as SASA! could be repackaged with a combination structured legal platforms for perpetrators, as well as intensive programs to educate and empower women.
Furthermore, although we observed significant inverse associations between more prohibitive neighborhood IPV norms and experiences of physical and emotional IPV among women, but the effect on experiences of sexual violence was not statistically significantly different from 0. Reasons for this result are not straightforward to delineate, but similar findings have been reported in randomized controlled trials that evaluate the role of supportive counseling and women empowerment to prevent and respond to incidence of IPV (Van Parys et al. 2017; Van Parys et al. 2014). More specifically, Tiwari et al. (2010) showed that an intervention consisting of women empowerment and additional components to change gendered attitudes related to IPV among Chinese women, significantly resulted in less emotional and physical violence (except for sexual IPV). Similarly, Kiely et al. (2010) reported that their comprehensive cognitive behavioral intervention only reduced recurrent episodes of physical and emotional IPV significantly, except for sexual IPV. This calls for more integrated and robust approaches for deconstructing hierarchical gender norms. In the area of IPV prevention, this may require constructing new concepts of masculinity and femininity as well as renegotiating power and patriarchal nuances in relationships, in order to shift programming towards multilayered programming that engages both women and men (Heise 2011) and to sequentially address different forms of IPV.
Interestingly, for the present study, however, reductions in incidence of IPV among women was not observed if more prohibitive neighborhood IPV social norms related to wife-beating were examined only among men. The implication of this result is that interventions to change gendered social norms such as justification of wife-beating only among men are unlikely to be effective in reducing actual experiences of IPV at the population level. Yet both women and men are equally important in the fight against IPV. For instance, in a 2011 national study of gender differences in risks for IPV among South African adults, it was observed that rates of perpetrating IPV are generally similar for women and men at about 25% (Gass et al. 2011). In a 2011 national survey in Uganda, ever married men age 15–49 years were reported to be about 6 times more likely to have initiated physical violence against their wives at 41% compared with 7% of ever married women who reported that they had ever initiated physical violence against their husbands (UBOS and ICF International 2012). These observations reinforce calls for projects aimed at changing gendered social norms and beliefs to move towards more simultaneous or sequential gender-synchronized approaches that address both sexes under the same programmatic umbrella (Gass et al. 2011; Greene and Levack 2010; Heise 2011; Stern et al. 2017). Moreover, the lack of significant effect of prohibitive IPV among men on the incidence of IPV among women was not unexpected because questions used to estimate gendered social norms related to wifebeating and posed to men, only focused on attitudes, but never explored whether responding men have actually ever perpetrated IPV towards their loved ones. This leaves us with unanswered questions of the potential impact of changing men’s attitudes and beliefs towards wife-beating on one hand and actual perpetration of IPV on the other hand.
A number of limitations for the considered illustrative example exist. Firstly, we focused on experiences of IPV among women only. That is why the measure for social norms adopted in the present study is limited because only questions related to justification of wife-beating were used to compute prohibitive neighborhood norms. However, it has been shown that men whether in heterosexual or same-sex intimate relationships who experience IPV report equally suffer from mental health outcomes and increased rates of sexually transmitted infections (Abrahams et al. 2006; Reid et al. 2008; Siemieniuk et al. 2013). In Uganda, though at a relatively lower scale compared to women, about 43% of ever married Ugandan men reported experiencing IPV by their intimate partners both in 2006 and 2011 (UBOS and ICF International 2012; UBOS and Macro International 2007). This limitation of the present paper is a call for demographic health surveys to include situations for which men and women believe that IPV against men is justifiable in order to inform policy and programming.
A second limitation of using any experiences of IPV with a present or former intimate partner as the main outcome of interest is temporality. This is because the norms of a community where a woman lives now may be different from those of the community where she experienced violence. The implication of this limitation is that the temporal ordering assumption, a requirement for causal interpretation (Buehner 2014; Rothman and Greenland 2005), such that neighborhood IPV social norms (i.e., exposure) precede the onset of any of the forms of IPV (i.e., outcomes), could be considered not being met by the structure of the data. Moreover, some of the women’s background characteristics corrected for in the statistical model such as parity and age are not constant and were measured, possibly after their experiences of IPV. However, most of the covariates in the current analysis, were considered to be fixed or that they are static over long time periods (such as race, sex, marital status, education), and we therefore consider that it is plausible to assume that they came before the exposure. In order to have an appropriate temporal ordering, we assumed that it is the neighborhood norms that change in advance of any woman experiencing a form of IPV. Although this is a reasonable assumption, the reverse may also be true; the implication of which would be that we are inferring the wrong causal direction for the estimated parameter.
A third limitation is the consideration of one exposure state—the neighborhood IPV social norms—an aggregate of the norms of survey respondents in a neighborhood instead of individual-level norms. However, our illustration provides a basis for the estimation of potential effects of an intervention on neighborhoods, subgroups of individuals, and/or individuals of interest. In this way, one can be able to estimate what would happen to the prevalence of a form of IPV if it was possible to change the exposure (i.e., IPV social norms) for any subgroups of individuals of interest. Moreover, Ahern et al. (2009) argued that “this is not a question that makes much sense from the perspective of intervention, because one would likely not intend to modify individual-level social norms while leaving the norms of a subgroup unchanged.” The current estimation approach and the considered illustrative example assume ignorability of nonlinearity of group-level processes and/or cross-level interactions, for instance, when familial-level or partner-level norms are reinforced by neighborhood-level norms. The assumption of ignorability and unmeasured confounders is common in epidemiological research of social exposures (VanderWeele 2008). The assumption here is that of an effective randomization of the exposure reflecting the absence of confounders for the exposure–outcome relation being studied, but this is not always correct. Sensitivity analyses to estimate the potential impact of ignored causal relations such as nonlinearity of group-level processes and absence of unmeasured confounders may be important in understanding how these uncertainties affect the current estimation method (Groenwold et al. 2010).
Lastly, we have assumed that absence of interference such that experiencing IPV by one woman is independent of the exposure and outcomes (or counterfactuals) of other women. This is called the stability assumption in neighborhood effects research (VanderWeele 2008). For the current illustration, we have assumed that IPV is a behavior that is likely not to have an element of contagion; that the experiences of IPV by an individual woman is likely not to affect the experiences of IPV by other women. However, it is plausible to assume that dynamic processes are likely to take place at the neighborhood level that can affect community-level norms and consequently change IPV prevalence. Therefore, estimation models that take these dynamic processes into account may be interesting for future research to anticipate the effects of any potential interventions (Ahern et al. 2009).
For the adopted analytical approach, these assumptions need to be met to be able to interpret the predicted values of the hypothesized cause-effect relationship. A detailed discussion of the implications of failure to meet these assumptions is available elsewhere (Ahern et al. 2009). Although the adopted analytical approach and the considered example do not necessarily meet all of the above assumptions, we submit that these limitations are likely to not substantially affect conclusions from the present analysis.
References
Abrahams, N., Jewkes, R., Laubscher, R., & Hoffman, M. (2006). Intimate partner violence: Prevalence and risk factors for men in Cape Town, South Africa. Violence and Victims, 21, 247–264.
Abramsky, T., Devries, K. M., Kiss, L., Nakuti, J., Kyegombe, N., Starmann, E., … Watts, C. (2014). Findings from the SASA! Study: A cluster randomized controlled trial to assess the impact of a community mobilization intervention to prevent violence against women and reduce HIV risk in Kampala, Uganda. BMC Medicine, 12(1). doi https://doi.org/10.1186/s12916-014-0122-5
Ahern, J., Hubbard, A., & Galea, S. (2009). Estimating the effects of potential public health interventions on population disease burden: A step-by-step illustration of causal inference methods. American Journal of Epidemiology, 169, 1140–1147. https://doi.org/10.1093/aje/kwp015.
Biswas, A., Dalal, K., Rahman, F., & Deave, T. (2015). Intimate partner violence during pregnancy and victim’s perception on miscarriage. International Journal of Public Health Research, 3, 58.
Buehner, M. J. (2014). Time and causality: Editorial. Frontiers in Psychology, 5. doi https://doi.org/10.3389/fpsyg.2014.00228
Campbell, J. C. (2002). Health consequences of intimate partner violence. The Lancet, 359, 1331–1336. https://doi.org/10.1016/S0140-6736(02)08336-8.
Chan, K. L. (2015). Association between intimate partner violence and child maltreatment in a representative student sample in Hong Kong. Violence Against Women, 21, 500–515. https://doi.org/10.1177/1077801215569080.
Cools, S., & Kotsadam, A. (2017). Resources and intimate partner violence in Sub-Saharan Africa. World Development, 95, 211–230. https://doi.org/10.1016/j.worlddev.2017.02.027.
Devries, K. M., Mak, J. Y. T., Garcia-Moreno, C., Petzold, M., Child, J. C., Falder, G., … Watts, C. H. (2013). The global prevalence of intimate partner violence against women. Science, 340(6140), 1527–1528. doi https://doi.org/10.1126/science.1240937
Devries, K. M., Knight, L., Child, J. C., Kyegombe, N., Hossain, M., Lees, S., … Naker, D. (2017). Witnessing intimate partner violence and child maltreatment in Ugandan children: A cross-sectional survey. BMJ Open, 7(2), e013583. doi:https://doi.org/10.1136/bmjopen-2016-013583
Ellberg, L., Högberg, U., Lundman, B., Källén, K., Håkansson, S., & Lindh, V. (2008). Maternity care options influence readmission of newborns. Acta Paediatrica, 97, 579–583. https://doi.org/10.1111/j.1651-2227.2008.00714.x.
Gass, J. D., Stein, D. J., Williams, D. R., & Seedat, S. (2011). Gender differences in risk for intimate partner violence among South African adults. Journal of Interpersonal Violence, 26, 2764–2789. https://doi.org/10.1177/0886260510390960.
Greene, M. E., & Levack, A. (2010). Synchronizing gender strategies: A cooperative model for improving reproductive health and transforming gender relations.. (Interagency Gender Working Group (IGWG)) Washington, DC: Population Reference Bureau. Retrieved from http://www.prb.org/igwg_media/synchronizing-gender-strategies.pdf. Accessed 5 Dec 2017.
Groenwold, R. H. H., Nelson, D. B., Nichol, K. L., Hoes, A. W., & Hak, E. (2010). Sensitivity analyses to estimate the potential impact of unmeasured confounding in causal research. International Journal of Epidemiology, 39, 107–117. https://doi.org/10.1093/ije/dyp332.
Gutman, R., & Rubin, D. B. (2013). Robust estimation of causal effects of binary treatments in unconfounded studies with dichotomous outcomes. Statistics in Medicine, 32, 1795–1814. https://doi.org/10.1002/sim.5627.
Heise, L. (2011). What works to prevent partner violence? An evidence overview(Monograph) London School of Hygiene and Tropical Medicine. Retrieved from http://strive.lshtm.ac.uk/resources/what-works-prevent-partner-violence-evidence-overview. Accessed 2 Nov 2017.
Jewkes, R. (2002). Intimate partner violence: Causes and prevention. The Lancet, 359, 1423–1429. https://doi.org/10.1016/S0140-6736(02)08357-5.
Johri, M., Morales, R. E., Boivin, J.-F., Samayoa, B. E., Hoch, J. S., Grazioso, C. F., … Arathoon, E. G. (2011). Increased risk of miscarriage among women experiencing physical or sexual intimate partner violence during pregnancy in Guatemala City, Guatemala: Cross-sectional study. BMC Pregnancy and Childbirth, 11(1). doi:https://doi.org/10.1186/1471-2393-11-49.
Kiely, M., El-Mohandes, A. A. E., El-Khorazaty, M. N., & Gantz, M. G. (2010). An integrated intervention to reduce intimate partner violence in pregnancy: A randomized controlled trial. Obstetrics & Gynecology, 115, 273–283. https://doi.org/10.1097/AOG.0b013e3181cbd482.
Kyegombe, N., Starmann, E., Devries, K. M., Michau, L., Nakuti, J., Musuya, T., et al. (2014). “SASA! is the medicine that treats violence”. Qualitative findings on how a community mobilisation intervention to prevent violence against women created change in Kampala, Uganda. Global Health Action, 7, 25082.
Lanza, S. T., Coffman, D. L., & Xu, S. (2013). Causal inference in latent class analysis. Structural Equation Modeling: A Multidisciplinary Journal, 20, 361–383. https://doi.org/10.1080/10705511.2013.797816.
Linos, N., & Kawachi, I. (2012). Community social norms as social determinants of violence against women. American Journal of Public Health, 102, 199–200. https://doi.org/10.2105/AJPH.2011.300410.
Niolon, P. H., Kearns, M. C., Dills, J., Rambo, K., Irving, S. M., Armstead, T. L., & Gilbert, L. K. (2017). Preventing intimate partner violence across the lifespan: A technical package of programs, policies, and practices. Atlanta, GA: National Center for Injury Prevention and Control, Centers for Disease Control and Prevention.
Pallitto, C. C., Campbell, J. C., & O’Campo, P. (2005). Is intimate partner violence associated with unintended pregnancy? A review of the literature. Trauma, Violence, & Abuse, 6, 217–235. https://doi.org/10.1177/1524838005277441.
R Core Team. (2017). R: A language and environment for statistical computing (Version 3.4.1). Vienna, Austria: R Foundation for Statistical Computing. Retrieved from https://www.R-project.org.
Raising Voices, LSHTM, & CEDOVIP. (2015). Is violence against women preventable? Findings from the SASA! study summarized for general audiences. Kampala. Kampala, Uganda. Retrieved from http://raisingvoices.org/wp-content/uploads/2016/01/SASApopularReport.FINAL_.jan2016.pdf. Accessed 10 Nov 2017.
Reid, R. J., Bonomi, A. E., Rivara, F. P., Anderson, M. L., Fishman, P. A., Carrell, D. S., & Thompson, R. S. (2008). Intimate partner violence among men. American Journal of Preventive Medicine, 34, 478–485. https://doi.org/10.1016/j.amepre.2008.01.029.
Rockhill, B. (2005). Theorizing about causes at the individual level while estimating effects at the population level: Implications for prevention. Epidemiology, 16, 124–129. https://doi.org/10.1097/01.ede.0000147111.46244.41.
Rose, G. (2001). Sick individuals and sick populations. International Journal of Epidemiology, 30, 427–432. https://doi.org/10.1093/ije/30.3.427.
Rothman, K. J., & Greenland, S. (2005). Causation and causal inference in epidemiology. American Journal of Public Health, 95, S144–S150. https://doi.org/10.2105/AJPH.2004.059204.
Shakya, H. B., Hughes, D. A., Stafford, D., Christakis, N. A., Fowler, J. H., & Silverman, J. G. (2016). Intimate partner violence norms cluster within households: An observational social network study in rural Honduras. BMC Public Health, 16(1). doi https://doi.org/10.1186/s12889-016-2893-4.
Sharps, P. W., Laughon, K., & Giangrande, S. K. (2007). Intimate partner violence and the childbearing year: Maternal and infant health consequences. Trauma, Violence, & Abuse, 8, 105–116. https://doi.org/10.1177/1524838007302594.
Siemieniuk, R., Miller, P., Woodman, K., Ko, K., Krentz, H., & Gill, M. (2013). Prevalence, clinical associations, and impact of intimate partner violence among HIV-infected gay and bisexual men: A population-based study: Partner violence among gay/bisexual men. HIV Medicine, 14, 293–302. https://doi.org/10.1111/hiv.12005.
StataCorp LLC (2017). Stata data analysis and statistical Software: Release 15. College Station, TX: StataCorp LP. Retrieved from https://www.stata.com.
Stern, E., Heise, L., & McLean, L. (2017). The doing and undoing of male household decision-making and economic authority in Rwanda and its implications for gender transformative programming. Culture, Health & Sexuality, 1–16. https://doi.org/10.1080/13691058.2017.1404642
Tiwari, A. F. Y., Salili, F., Chan, R. Y. P., Chan, E. K. L., & Tang, D. (2010). Effectiveness of an empowerment intervention in abused Chinese women. Hong Kong Medical Journal, 16, 25–28.
Tsai, A. C. (2013). Intimate partner violence and population mental health: Why poverty and gender inequities matter. PLoS Medicine, 10, e1001440. https://doi.org/10.1371/journal.pmed.1001440.
Tsai, A. C., Tomlinson, M., Comulada, W. S., & Rotheram-Borus, M. J. (2016). Intimate partner violence and depression symptom severity among South African women during pregnancy and postpartum: Population-based prospective cohort study. PLoS Medicine, 13, e1001943. https://doi.org/10.1371/journal.pmed.1001943.
Tsai, A. C., Kakuhikire, B., Perkins, J. M., Vořechovská, D., McDonough, A. Q., Ogburn, E. L., et al. (2017). Measuring personal beliefs and perceived norms about intimate partner violence: Population-based survey experiment in rural Uganda. PLoS Medicine, 14, e1002303. https://doi.org/10.1371/journal.pmed.1002303.
Uganda Bureau of Statistics [UBOS], & ICF International. (2012). Uganda Demographic and Health Survey 2011. Kampala, Uganda: UBOS and ICF International. Retrieved from http://dhsprogram.com/publications/publication-fr264-dhs-final-reports.cfm. Accessed 3 Sept 2017.
Uganda Bureau of Statistics [UBOS], & ICF International. (2017). Uganda Demographic Health Survey 2016: Key Indicators Report. Kampala, Uganda: UBOS, and Rockville, Maryland, USA: UBOS and ICF International. Retrieved from http://dhsprogram.com/publications/publication-PR80-Preliminary-Reports-Key-Indicators-Reports.cfm.
Uganda Bureau of Statistics [UBOS], & Macro International. (2007). Uganda Demographic and Health Survey 2006. Calverton, Maryland, USA: UBOS and Macro International. Retrieved from http://dhsprogram.com/pubs/pdf/FR194/FR194.pdf. Accessed 20 March 2018.
Van Parys, A.-S., Verhamme, A., Temmerman, M., & Verstraelen, H. (2014). Intimate partner violence and pregnancy: A systematic review of interventions. PLoS One, 9, e85084. https://doi.org/10.1371/journal.pone.0085084.
Van Parys, A.-S., Deschepper, E., Roelens, K., Temmerman, M., & Verstraelen, H. (2017). The impact of a referral card-based intervention on intimate partner violence, psychosocial health, help-seeking and safety behaviour during pregnancy and postpartum: A randomized controlled trial. BMC Pregnancy and Childbirth, 17. https://doi.org/10.1186/s12884-017-1519-x.
VanderWeele, T. J. (2008). Ignorability and stability assumptions in neighborhood effects research. Statistics in Medicine, 27, 1934–1943. https://doi.org/10.1002/sim.3139.
Westreich, D., Edwards, J. K., Cole, S. R., Platt, R. W., Mumford, S. L., & Schisterman, E. F. (2015). Imputation approaches for potential outcomes in causal inference. International Journal of Epidemiology, 44, 1731–1737. https://doi.org/10.1093/ije/dyv135.
Widom, C. S., Czaja, S., & Dutton, M. A. (2014). Child abuse and neglect and intimate partner violence victimization and perpetration: A prospective investigation. Child Abuse & Neglect, 38, 650–663. https://doi.org/10.1016/j.chiabu.2013.11.004.
World Health Organisation [WHO] (Ed.). (2013). Global and regional estimates of violence against women: Prevalence and health effects of intimate partner violence and non-partner sexual violence. Geneva: World Health Organization, Department of Reproductive Health and Research.
Acknowledgments
We wish to acknowledge the Ministry of Health of Uganda and Demographic Health Survey program, who granted us access to use the DHS data. Furthermore, we are grateful to the East Africa Social Science Translation Collaborative under the Center of Effective Global Action, University of California, Berkeley (EASST/CEGA), for having awarded the lead author the Fall 2017 EASST/CEGA Impact Evaluation Fellowship, during which manuscript preparation and statistical data analysis were carried out.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
This is not applicable in this study. The paper utilized secondary data of the Demographic Health Survey program, and permission to use these publically available data was obtained from http://www.dhsprogram.com before data download and subsequent statistical analysis. As such, no ethical reviews and approvals were required before or during preparation of the present manuscript.
Informed Consent
This is not applicable in this study. This is a simulation-based manuscript based on secondary data of the Demographic Health Survey program. There was no interaction with human subjects during preparation of this manuscript.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 16 kb)
Rights and permissions
About this article

Cite this article
Kadengye, D.T., Iddi, S., Hunter, L. et al. Effectiveness of Potential Interventions to Change Gendered Social Norms on Prevalence of Intimate Partner Violence in Uganda: a Causal Inference Approach. Prev Sci 20, 1043–1053 (2019). https://doi.org/10.1007/s11121-019-01010-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11121-019-01010-8