
Abstract
Children who exhibit early-starting conduct problems are more likely than their peers to initiate sexual activity and substance use at an early age, experience pregnancy, and contract a sexually-transmitted disease [STD], placing them at risk for HIV/AIDS. Hence, understanding the development of multi-problem profiles among youth with early-starting conduct problems may benefit the design of prevention programs. In this study, 1,199 kindergarten children (51 % African American; 47 % European American; 69 % boys) over-sampled for high rates of aggressive-disruptive behavior problems were followed through age 18. Latent class analyses (LCA) were used to define developmental profiles associated with the timing of initiation of sexual activity, tobacco and alcohol/drug use and indicators of risky adolescent sex (e.g. pregnancy and STD). Half of the high-risk children were randomized to a multi-component preventive intervention (Fast Track). The intervention did not significantly reduce membership in the classes characterized by risky sex practices. However, additional analyses examined predictors of poor outcomes, which may inform future prevention efforts.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Children who show “early starting” conduct problems at school entry (age 5–6) typically exhibit a diverse range of externalizing problems, concurrent attention and learning problems, and are at elevated risk for developing “life-course persistent” patterns of criminal activity (Dishion and Patterson 2006). Early-starting aggressive children are more likely than their peers to initiate other socially-censured behaviors at a young age, including cigarette smoking (Joun et al. 2002) and alcohol use (Capaldi et al. 1996). In addition, childhood conduct problems predict the early initiation of sexual intercourse, elevated rates of adolescent sexual activity, and risky sexual behaviors, such as multiple sex partners, unintended pregnancy, and sexually transmitted diseases [STDs], which confer risk for HIV/AIDS (Ramrakha et al. 2007). Ramrakha et al. (2007) found that childhood conduct problems doubled the odds of early sexual debut and risky adolescent sex.
Several studies suggest that childhood conduct problems initiate a developmental cascade that promotes tri-morbid risk in adolescence (antisocial behavior, substance use, risky sexual activity) (Capaldi et al. 1996; Dishion and Patterson 2006). Given this developmental progression, researchers interested in reducing risky sexual activity have suggested that prevention efforts to reduce childhood conduct problems might also reduce risky sexual activity and its consequences, such as unintended pregnancy, STDs, and HIV/AIDS. Focused on this broad question, the present study had three aims: 1) to examine the developmental co-occurrence of aggressive behavior, tobacco and alcohol/drug use, and risky sexual activity within a sample of children with early-starting conduct problems, 2) to examine the degree to which different adolescent problem profiles (and corresponding risk for early pregnancy and STDs) were predicted by early childhood characteristics and associated with proximal preadolescent characteristics, and 3) to determine whether a prevention program that had a positive impact reducing the early aggressive-disruptive behaviors of these children (Fast Track) also reduced their risk for emerging tri-morbid problem profiles and risky sexual activity. The overall goal was to extend understanding of developmental factors associated with early sexual activity and its consequences in a diverse and vulnerable population of children with elevated conduct problems, in order to inform and strengthen future prevention programming targeting sexual risk.
Developmental Mechanisms and the Predictive Significance of “Starting Early”
Initiating sexual intercourse early (by age 13–14) increases risk for STDs, unintended pregnancies, and HIV/AIDS (Meshke et al. 2000). Early sexual debut is often accompanied by the early initiation of tobacco and alcohol/drug use, which compounds youth risk (Kotchick et al. 2001). For example, youth who initiate cigarette smoking early (by age 11) are at elevated risk for carrying weapons in adolescence, and for sustained and heavy smoking in adulthood (DuRant et al. 1999; Tucker et al. 2002).
Problem behavior theory suggests that early-starting aggressive behaviors reflect both an alienated stance toward adult authority and poor self-regulation skills. When youth enter adolescence and achieve greater autonomy, these tendencies support the initiation of a range of rule-breaking behaviors, promoting tri-morbid risks of antisocial behavior, substance use, and risky sexual activity (Brendgen et al. 2007; Hipwell et al. 2010; Zweig et al. 2001). Indeed, longitudinal research has documented that, along with childhood aggression, childhood impulsivity and self-regulation deficits predict risky sexual activity in adolescence, including early sexual debut, multiple partners, and sex without condoms (Crockett et al. 2006; Zimmer-Gembeck et al. 2004). Early child risk characteristics (impulsivity, aggression, inattention) appear most problematic in contexts in which positive socialization supports are compromised, particularly in the adverse contexts faced by socio-economically distressed families (Rose et al. 2005), and when parents are emotionally detached or uninvolved (Hipwell et al. 2010; Raffaelli and Crockett 2003).
In addition to their direct effects on child functioning, early aggression and self-regulatory deficits may undermine adaptive socialization in later childhood, fostering peer rejection, conflicts with teachers, and school disengagement, thereby increasing risk for multi-problem behavioral profiles at the transition into adolescence (Kotchick et al. 2001). Consistent with this model, prior analyses of youth in the Fast Track control group found that aggression and inattention at school entry increased risk for school maladjustment, antisocial activity, and substance use in middle school which, in turn, mediated the early initiation of sexual activity (Schofield et al. 2008). Specific risk factors linked with early sexual activity may include association with peers who exhibit deviant and risk-taking behavior (Capaldi et al. 1996; Raffaelli and Crockett 2003), depressed mood (DiClemente et al. 2001; Hipwell et al. 2010), and school problems (Schofield et al. 2008). In addition, the timing of puberty has been implicated as a risk factor for early sexual debut in some studies (Gowen et al. 2004).
Prevention Program Design
Given the developmental links between early-starting aggression, substance use, and risky sexual activity, prevention programs that reduce aggression and promote self-regulation skills in elementary school years might also reduce risk for the development of multi-problem profiles in adolescence and the associated risks of unintended pregnancies and STDs. The multi-component Fast Track preventive intervention targeted children who entered elementary school with high rates of aggressive-disruptive behaviors, and addressed the primary risk factors for antisocial behavior (e.g., poor parenting practices, poor peer relations and social competence deficits, weak reading readiness, and poor home-school relations) (Bierman et al. 1996; McMahon et al. 1996). Recognizing the importance of addressing both school and home contexts, the intervention included parents and teachers and was organized developmentally to provide intensive intervention at school entry (beginning in 1st grade) with ongoing monitoring and intervention support through the transition into high school (through 10th grade). The intensive intervention in grades 1–3 produced positive effects, reducing aggressive behaviors among children (by parent and teacher report), promoting positive peer interactions (by observer ratings) and higher social preference (by peer nominations) (CPPRG 2002). These effects waned during the middle school years (grades 6–8), when no intervention effects were apparent (CPPRG 2010a). However, later analyses showed positive intervention effects on adolescent outcomes, including delays in onset and reductions in the rate of juvenile arrests (CPPRG 2010b) and reduced rates of externalizing disorder for the highest-risk youth (CPPRG 2011). This study examines the possibility that the Fast Track intervention also had effects on risky sexual outcomes in adolescence.
Person-Centered Approaches
Although aggressive-disruptive behaviors at school entry signal increased risk for the early initiation of sexual activity, tobacco, and alcohol/drug use, not all aggressive children go on to develop these problems in early adolescence. Given the potential for synergistic risk, developmental research designed to understand heterogeneity in the risk profiles that emerge among children with early-starting conduct problems is needed. This kind of research requires a person-centered framework in which youth are classified into groups based on the presence of problem behaviors (Lanza et al. 2007).
In addition, it is important to note that the base rates of behavior problems associated with early sexual activity vary as a function of gender, location, and race. For example, girls are less likely than boys to show overt aggression, African American girls are likely to initiate sexual activity at a younger age than European-American girls, and youth who live in violent, urban areas have increased opportunities for deviant peer involvement relative to rural youths (Doljanac and Zimmerman 1998; Zweig et al. 2001). Hence, examining gender, race, and urban/rural differences in the predictability of early sexual activity is warranted.
The Present Study
Significant concerns exist about youth who initiate sexual behavior at young ages: their numbers are increasing in the U.S., they disproportionately include children of color from families living in poverty, and they are not served by current prevention programs that target teenagers (Albert et al. 2003). Their risks for STDs and HIV/AIDS are dramatically higher than their more advantaged peers who initiate sexual activity at later ages, and yet very little is known about nature of their early risks or the concurrent preadolescent risk behaviors that may complicate prevention program design and moderate intervention effectiveness. The present study offered a unique opportunity to inform future prevention program design by examining the early childhood antecedents and preadolescent correlates of early sexual debut in a large, diverse, multi-site sample of vulnerable children at-risk due to elevated rates of childhood conduct problems and family adversity. The large sample size and study design made it possible to go beyond the variable-centered linear predictions provided by prior longitudinal studies, and to explore variations in individual risk profiles using person-oriented analyses. In addition, the present study offered the opportunity to evaluate the impact of the Fast Track prevention program on early sexual activity, to determine whether a program effective at reducing early aggression and improving the gradeschool social and academic adjustment of children with early-starting conduct problems might also confer benefits in terms of reducing sexual risk. First, we applied a person-oriented approach (LCA) to better understand the patterns of co-occurring precocious tobacco use, alcohol/drug use, and risky sexual activity in this sample of vulnerable children oversampled for early-starting conduct problems. Second, we explored early childhood behaviors (e.g., externalizing behaviors, attention problems, academic difficulties) and family features (low SES, low parental warmth) as predictors of the development of tri-morbid problem profiles and risky sexual outcomes. We also examined associations between more proximal risks evident in late childhood and preadolescence (e.g., pubertal timing, depressed mood, deviant peer affiliation, and school adjustment) and profiles of tri-morbid risk. Finally, we tested for intervention effects on risky sexual activity and outcomes and evaluated whether the preventive intervention affected profile classification and reduced the probability that children would be part of a high-risk profile class.
Method
Participants
Behaviorally disruptive target children (N = 891) were identified using a multi-stage screening procedure. Over three successive years, kindergarten teachers at 55 schools at four sites (Durham, NC; Nashville, TN; Seattle, WA; and rural central Pennsylvania) completed the Authority Acceptance scale of the TOCA-R (Werthamer-Larsson et al. 1991) on all kindergarteners (N = 9,594). Parents of children scoring in the top 40 % within cohort and site were contacted, and 91 % (N = 3,274) completed a 24- item scale describing child aggressive-disruptive behaviors at home. Children were selected into the high-risk sample by starting with the highest combined teacher-parent screen score and moving downward until cells were filled within sites, cohorts, and conditions. Participating schools were divided into several matched sets at each site, based on school size and student demographics, and then randomly assigned to intervention (N = 445) or control (N = 446) conditions. In addition, a stratified normative sample of children (N = 308 additional children) was identified from control schools for a total original sample of 1,199.
At the time of the first assessment in kindergarten, the mean age of the children was 6.5 years (SD = 0.48). Across all sites, the sample was 69 % boys, 51 % African American, 47 % European American, and 2 % of other ethnicity. Families had elevated risk characteristics: 58 % were single-parent families, 29 % of the parents had not finished high school, and 40 % were in the lowest socioeconomic class, representing unskilled workers (Hollingshead 1979).
Twelve years after recruitment, at the final assessment point for this study, only partial data was available for 29 % of the sample, but LCA uses full information likelihood to estimate missing data for these cases. However, 9 % of the sample had insufficient data for inclusion.
Intervention Procedures
Elementary School Phase (Grades 1–5)
During the elementary phase of the intervention (grades 1–5), the Fast Track adaptation of the Promoting Alternative Thinking Strategies (PATHS) Curriculum was implemented by teachers in grades 1–5 at the intervention schools (see Bierman et al. 1996 for more details). In addition, parents and children in the high-risk intervention condition were invited to "enrichment programs" held at local schools. These programs offered social skills training for children (focused on emotion regulation, prosocial behaviors, self-control and social problem-solving skills), parenting management skills training for parents (focused on providing warm support, communication skills, limit-setting, and supporting school success), and parent–child sharing sessions designed to promote positive parent–child relationships (see McMahon et al. 1996 for details). Group interventions were intensive in grades 1–2 (35 sessions total), and included monthly "boosters" in grades 3–5. Children and families were offered a standard level of services in grade 1; in subsequent years, criterion-referenced assessments were used to adjust individualized services including peer pairing and academic tutoring for children and home visits for parents.
Middle School Phase and Transition To High School (Grades 6–10)
A middle school transition program included 6 child sessions on organization and study skills, visits to the middle school, and parent sessions focused on developing positive connections with counselors and teachers. Four family group meetings addressed substance use and sexual activity, parental monitoring and communication, and youth resistance, refusal, and decision-making skills. Following grade 7, all intervention was individualized, in order to avoid iatrogenic processes that might occur in group intervention. Case managers completed criterion-referenced ratings at three times each year and based on these ratings, offered family visits, youth mentoring meetings, and/or academic support.
All intervention components were guided by detailed manuals, and annual cross-site trainings and weekly supervisory meetings served to standardize intervention approaches across site. Multiple strategies were used to increase parental involvement (e.g., transportation, child-care, refreshments, nominal payment ($15) for each group session attended). Only a few families (6 % of the sample) declined to initiate participation in the intervention. Of the 94 % participating, 79 % of the parents and 90 % of the children attended at least 50 % of the sessions offered. Intervention participation decreased gradually across the years, and by grade 6, 10 % of the families had moved outside of the service delivery area. During the middle school years, approximately 15 % of the youth were rated as low risk, but a majority continued to receive some services through tenth grade. On average, 63 % of the parents and 78 % of the youth attended group sessions held in middle school (parent mean of 3.8 meetings attended; youth mean of 6.4 meetings attended). Individualized services were provided to 80 % of the parents and 78 % of the youth during grades 8–10.
Procedures
All procedures followed APA guidelines for the ethical conduct of research and were approved by the institutional review boards at each of the four sites. Each summer, two research interviewers visited each home; one interviewed the primary caregiver and the other interviewed the youth. The interviewer read through all questionnaires and recorded the caregiver’s response. Computer-assisted interviews were conducted with the youth, who wore headphones and listened to items being read to them on a laptop computer, answering directly. Each spring, rating forms were delivered and explained to teachers, who then completed them and returned them to the project. Parents, youth, and teachers were all compensated financially for their participation. Data collection staff were naïve concerning the normative, intervention, or control status of the families and youth they interviewed. Data were processed at a central data center that served all four sites.
Measures
Problem Behaviors Included in Profiles
Questions drawn from the National Longitudinal Study of Adolescent Health (Add Health, Resnick et al. 1997) were administered to youth every year between 7th and 11th grades to assess the initiation of problem behaviors. Youth were asked if they had ever had sexual intercourse (“When I say sexual intercourse, I mean when a male inserts his penis into a female’s vagina”), if they had smoked cigarettes, cigars, or used chewing tobacco or snuff, and if they had used alcohol (beer, wine, wine coolers and liquor) or illegal drugs (marijuana, cocaine, crack, inhalants, heroin, LSD, PCP, ecstasy, mushrooms, speed and other pills not prescribed by a physician). These responses were used to stratify the sample into three groups reflecting the timing of first initiation of each behavior, as follows. Very early initiation involved first intercourse, tobacco use, or substance use by grade 8, age 14. Early initiation involved first intercourse, tobacco use, or substance use by grade 10–11, age 16–17. Later (or non-) initiation included all other youth. Pregnancy and STDs were scored dichotomously, “1” indicating that a girl had a pregnancy or a boy reported causing a pregnancy, and “1” indicating an STD diagnosis reported at any interview during adolescence.
Kindergarten Predictors
Aggressive-disruptive behaviors were assessed by kindergarten teachers on the externalizing scale of the Teacher Report Form of the Child Behavior Checklist (TRF, Achenbach 1991), with 33 items (e.g., argues, fights, disobedient) rated on a 3-point scale (α = 0.94 in this sample). Attention problems were assessed using the 20-item attention problem scale of the TRF (example: “Can’t concentrate, can’t pay attention for long”) rated on a 3-point scale (α = 0.94 in this sample). Cognitive ability was assessed with the block design and vocabulary subtests of the Wechsler Intelligence Scale for Children—IV, and reading skills were assessed with the letter-word identification subtest from the Woodcock-Johnson Psycho-Educational Battery—Revised. Age-corrected standard scores were used. More complete measure descriptions can be found at: www.fasttrackproject.org.
In addition to these child characteristics, family socioeconomic status (SES; Hollingshead 1979) was assessed by caretakers’ reports of their education level and occupation and categorized using the Hollingshead (1979) system. Parental warmth was rated by observers using 6-items describing the mother’s sensitivity and responsiveness to her child’s cues on the Interaction Rating Scale (IRS; Crnic and Greenberg 1987) after observing parent–child interactions on play and teaching tasks during the home visit (α = 0.88; κ = 0.71).
Preadolescent Characteristics
Measures collected at the end of seventh grade were examined as possible correlates of risk status. Youth provided self-reports of their pubertal development using the Pubertal Development Scale (Petersen et al. 1988), rating their physical development (for boys, voice changes, facial hair; for girls, breast development, onset of menstruation). A total score was used (α = 0.75 for boys, α = 0.61 for girls). To assess depression, youth completed the Reynolds Adolescent Depression Scale (RADS) (Reynolds & Mazza, 1998), rating 30 items describing depressive symptoms on a 4-point rating scale (α = 0.90 in this sample). Assessing deviant peer affiliation, youth rated 5 items describing gang involvement (e.g., gang membership, length of affiliation), and parents rated 10 items describing the child’s close friends (e.g., disapproval of the friends, concerns about negative influence), with the total score reflecting deviant friends (α = 0.87). Youth rated their school adjustment on 8 items describing academic and disciplinary difficulties during the prior school year using a 5-point scale (“I stayed out trouble at school”, “School work was really hard” – reverse scored, “I did not do well in academics” – reverse scored) (α = 0.75).
Results
Descriptive Analyses
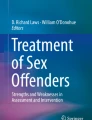
Table 1 shows the proportion of girls and boys in the sample (normative and high risk children combined) who initiated sexual activity, tobacco use, and alcohol/drug use at the various time points (very early, early, or later) and who had (or caused) a pregnancy or contracted a sexually-transmitted disease. Rates are shown separately for girls and boys in the three demographic groups studied (e.g., urban African American, urban European American, and rural European American). Consistent with prior research, urban African American youth had earlier sexual activity and higher rates of pregnancy and STDs than the other groups, but there were few demographic differences for the timing of tobacco and alcohol/drug initiation.
When examined separately, rates were generally higher in the high-risk sample than the normative control group; for example across the demographic groups, 58–75 % reported very early initiation of tobacco use (compared to 39–63 % in the normative sample), 46–62 % reported the very early initiation of alcohol or drug use (compared to 32–49 % in the normative sample), and 18—54 % reported the very early initiation of sexual activity (compared to 2–31 % in the normative sample.) Consistent with prior research, these findings show that children with early-starting conduct problems are at elevated risk for the precocious initiation of illicit substance use and sexual activities. Unprotected sexual activity was common, with one-third of the girls in the high-risk sample reporting a pregnancy and one-fifth reporting an STD by eleventh grade (age 17 for most). Correlations among risk behaviors are shown in Table 2. As anticipated, the timing of first sexual intercourse was correlated with the timing of first tobacco and alcohol/drug use.
Latent Class Analyses—Identifying Risk Classes
Latent class models were estimated using PROC LCA (Lanza et al. 2007). Full-information maximum-likelihood was used to account for missing data on the latent class indicators. The software to conduct LCA is available at http://methodology.psu.edu.
A model with four risk classes was selected on the basis of the BIC, AIC and model interpretation using data for the entire sample (high-risk and normative samples, combined). However, the classes were not invariant across sex, based upon likelihood ratio tests comparing models which restricted item parameters to be equal and models which allowed item parameters to vary by sex (p < .001). Therefore, data from boys and girls were analyzed separately. The number of latent classes was reassessed separately for each sex, and four latent class models remained the best model for each sex based on the same criteria. When each of the three demographic groups within each sex was analyzed separately (e.g., urban African American, urban European American, rural European American), four latent class models were still preferred in all cases and the interpretations remained the same within sex. This finding suggested that it would be reasonable to combine all locality-race groups into a single measurement model separately for each sex, but allow the proportion of children in each class to vary among the locality-race groups.
LCA Profiles for Boys
Table 3 shows the prevalence of the four risk classes that emerged for boys. Risk class 1 was most prevalent class, representing about 35 % of the boys in the sample. The item-response probabilities, shown in Table 3, are similar conceptually to factor loadings, but here they represent the probability that youths in the latent class exhibit each risky behavior. For example, boys in risk class 1 were likely to be very early sexual initiators (0.88), very early tobacco initiators (0.95), and very early alcohol users (0.86). Relative to the other classes, boys in this class also showed an elevated probability of causing a pregnancy (0.39) and experiencing an STD (0.20). Urban African American boys had a higher probability of being in this class (0.45) than urban or rural European American boys (0.31 and 0.18, respectively), as did youth in the high-risk sample (0.85). We labeled this class “preadolescent multi-problem” as it was defined by preadolescent initiation of sexual activity, tobacco use, and alcohol/drug use. The second risk class represented 14 % of the sample. Boys in this class had a high probability of being early (but not very early) sexual initiators (1.00), early (but not very early) tobacco initiators (0.70), and early (but not very early) alcohol users (0.64). Relative to the other classes, these boys also had a somewhat elevated probability of causing pregnancy (0.35) but were not likely to contract a STD (0.03). Urban African American boys had an elevated probability of being in this class (0.27) relative to urban or rural European American boys (0.00 and 0.02, respectively), as did youth in the high-risk sample (0.86). We labeled this class “adolescent multi-problem” to reflect the initiation of tri-morbid problems during mid-adolescence (grades 9–10). Boys in class 3 (approximately 30 % of the sample) had a high probability of very early tobacco initiation (0.87) and very early alcohol initiation (0.59), but were likely to delay sexual initiation (0.54), with a corresponding low probability of causing pregnancy or contracting a STD (0.06–0.01, respectively). Urban and rural European American boys were more likely to be in this class (0.46 and 0.48, respectively) than urban African American boys (0.13). We labeled this class “preadolescent substance users”. Boys in risk class 4 (21 % of the sample) were characterized by low probabilities on each risky behavior, and were labeled “low risk.”
LCA Profiles for Girls
Table 4 shows the prevalence of the four risk classes that emerged for girls. Risk class 1 represented about 28 % of the girls in the sample. Girls in this class were likely to be very early sexual initiators (0.54), very early tobacco initiators (0.92), and very early alcohol users (0.89), with an elevated probability of pregnancy (0.55) and STD (0.44). We labeled this class “preadolescent multi-problem”. Relative risk for membership in this class was 0.36 for urban African American girls compared with 0.28 and 0.23 for urban and rural European American girls, respectively, and girls from the high-risk sample were relatively likely to be in this class (0.73). Girls in Class 2 (10 % of the sample) had an elevated probability of initiating early (but not very early) sex (0.93) and very early or early tobacco use (0.57–0.80, respectively) and also showed a very elevated probability of pregnancy (0.72). The probability of experiencing an STD was low (0.26) but higher than the probability experienced by girls in class 3 or 4. Interestingly, this group had an extremely low probability of alcohol or drug use. Urban African American girls were more likely to be in this class (0.21) than were urban or rural European American girls (0.04 and 0.05, respectively). We labeled this class “adolescent dual problem” reflecting the association with mid-adolescent initiation of sexual activity and tobacco use, but no early alcohol/drug use. Girls from the high-risk sample had an elevated probability of membership in this class (0.65). Girls in risk class 3 (27 % of the sample) showed an elevated probability of very early tobacco use (0.89), and very early alcohol-drug use (0.57) but were unlikely to initiate very early or early sexual activity (0.00–0.34, respectively). Urban European American girls were more likely to be in this class (0.44) than either urban African American (0.19) or rural European American girls (0.32). We labeled this class “preadolescent substance users” because they initiated both tobacco and alcohol/drug use in preadolescence, but did not initiate concurrent sexual activity. Girls in risk class 4 (35 % of the sample) had low probabilities on each of the risky behaviors and were labeled “low risk.”
Child and Family Predictors and Correlates of Risky Sexual Outcomes and Profiles
The next set of analyses examined associations between childhood and preadolescent characteristics and risky sexual outcomes using two approaches: 1) examining linear associations between child characteristics and the timing of risk behavior initiation and risky sexual outcomes, and 2) examining group differences to determine which characteristics significantly differentiated youth who developed different profiles of adolescent risk. The top part of Table 5 (indicated with T1 for time 1 measurements), shows simple correlations linking kindergarten child characteristics (externalizing behavior, attention problems, reading skills, cognitive ability) and family features (family SES, parental warmth) to the timing of initiation of risky adolescent behaviors (sexual activity, tobacco use, and alcohol/drug use) and occurrence of pregnancy or STD. For both boys and girls, higher rates of kindergarten externalizing behaviors and inattention and lower levels of cognitive ability predicted greater sexual risk (early sexual initiation, adolescent pregnancy and, for girls, STDs). In addition, poor reading skills predicted earlier sexual activity among boys. Lower family SES and lower levels of parental warmth in kindergarten were also significant predictors of early sexual activity, pregnancy, and (for family SES only) elevated STDs for both boys and girls.
The bottom part of Table 5 (indicated with T2 for eighth grade measures), shows simple correlations linking child characteristics at the end of eighth grade (age 14) to the timing of sex, tobacco, and substance use initiation. For both boys and girls, pubertal development, depressive symptoms, gang involvement, deviant friends, and school maladjustment were significantly associated with earlier timing of sexual activity, tobacco, and alcohol/drug use. Depressive symptomatology (for girls), gang involvement (for boys), deviant friends and school maladjustment (for girls and boys) were also associated with elevated rates of pregnancy and, in some cases, STDs.
Next, we examined the degree to which each of these kindergarten characteristics were associated with the risk classes. Youth were assigned to their most likely LCA class using posterior probabilities, and ANOVAs with post-hoc (Bonferonni) comparisons were used to identify significant group differences. As shown in Table 6, all of the kindergarten characteristics and eighth grade characteristics studied here (with the exception of kindergarten reading skills for girls) significantly differentiated girls and boys in the preadolescent multi-problem class from youth in the low-risk class. Youth in class 2 (who also had elevated rates of pregnancy and STDs) differed significantly from the low-risk class on all of the kindergarten child and family characteristics (for boys) and in early inattention, lower family SES and lower parental warmth (for girls). Interestingly, however, this group did not differ from the low-risk group on 8th grade measures of pubertal development, depressive symptoms, gang involvement, or deviant friends (for boys), although they had lower rates of school adjustment. Interestingly, youth in Class 3, who engaged in early tobacco and substance use but did not have elevated risk for pregnancy or STDs, did not differ significantly from youth in the low risk group on any of the kindergarten characteristics (except for inattention for boys), but showed higher levels than the low risk group on all of the eighth grade measures (except for deviant friends for boys).
Examination of Prevention Program Effects
Finally, we examined prevention program effects on risky outcomes. Logistic regressions were computed to determine whether assignment to intervention condition (compared with control) was associated with differences in the timing of the initiation of tobacco use, drug/alcohol use, or sexual intercourse, or associated with pregnancy or STDs that are used in the LCA analyses. No significant effects emerged (all p s > .10). We were also interested in determining whether intervention affected youth’s problem profiles, represented by the latent classes. In particular, we wanted to determine whether intervention reduced the risk that high-risk youth would be classified into classes 1 or 2 (where risk for pregnancy and STDs was concentrated) compared with class 4 (the low-risk class). Intervention-control group assignment was incorporated in the latent class model to predict latent class membership probabilities. However, none of these comparisons indicated a significant impact of intervention status on profile membership for boys or girls (all ps > .10). When youth were assigned to their most likely class membership using posterior probabilities, the proportion of youth assigned to each class was similar for the intervention and control groups: 1) preadolescent multi-problem, 36 % intervention, 37 % control; 2) adolescent multi-problem (boys) or adolescent dual-problem (girls), 16 % intervention, 16 % control; 3) preadolescent substance use, 30 % intervention, 28 % control; and 4) low risk, 17 % intervention, 18 % control.
Discussion
To improve the effectiveness of prevention programs targeting youth at highest risk for early and risky sexual behavior, it is critical to understand the developmental precursors of risk and to incorporate a developmental perspective into prevention program design (Hipwell et al. 2010). Current prevention programs that target middle-school students may be too little, too late to change the trajectories of the highest-risk early starters -- those who initiate sexual activity by age 13. Given its increasing prevalence in the U.S. and its association with socioeconomic disadvantage, early-starting sexual activity represents an important source of health disparities, particularly in the area of STDs and HIV/AIDs risk (Albert et al. 2003; Brendgen et al. 2007). This study provides important insights into the early childhood and preadolescent characteristics of youth who are at high risk for early sexual activity and the associated negative consequences of unintended pregnancy and STD. Although the Fast Track prevention program was effective in reducing antisocial behavior, no “spillover” effects reducing the early initiation of sexual risk and accompanying early initiation of substance use were detected. This study focused on the timing of initiation and hence these findings do not preclude the possibility of intervention effects on other aspects of sexual activity or substance use. However, the failure to delay initiation, as well as the developmental findings from the study, have implications for future research and indicate the challenges associated with developing effective prevention programming to reduce sexual risk among children with early-starting conduct problems.
Profiles of Multi-Problem Risk
For some time, it has been known that children who show high rates of aggressive conduct problems at school entry are at elevated risk for developing “life-course persistent” patterns of criminal activity and maladjustment (Dishion and Patterson 2006). A number of studies also suggest that they are likely to precociously initiate cigarette smoking (Joun et al. 2002), alcohol use (Capaldi et al. 1996), and risky sexual activity, experiencing heightened risk for adolescent pregnancy, STDs, and HIV/AIDS (Capaldi et al. 1996; Ramrakha et al. 2007). The present study extended this research by applying recently-developed LCA techniques to better understand variation in the risk profiles of children growing up with the vulnerabilities conferred by early conduct problems and socio-economic disadvantage. This person-oriented approach enabled an exploration of heterogeneity in profiles of emerging adolescent risk among aggressive youth.
The importance of a person-oriented approach was highlighted by the different profiles of problem co-occurrence that emerged in this study. Four distinct profiles emerged for girls and boys, based on the timing of initiation of three risk behaviors (sexual intercourse, tobacco use, alcohol/drug use) and indicators of risky sex (adolescent pregnancy, STD). Three of the classes were distinguished by risky behaviors (and included more early-starting aggressive youth than normative peers), but only two of these classes showed elevated sexual risk. Specifically, the “preadolescent multi-problem” class, characterized by the very early initiation (by 8th grade, age 13–14) of all three risky behaviors (sexual intercourse, tobacco use, and alcohol/drug use) was at high risk for teen pregnancy (0.39 for boys, 0.55 for girls) and STDs (0.20 for boys, 0.44 for girls). The “adolescent multi-problem” profile (for boys) characterized by the mid-adolescent initiation of sexual activity, tobacco use and alcohol use, and “adolescent dual problem” profile (for girls, characterized by the mid-adolescent initiation of sexual activity and tobacco use also conferred risk for teen pregnancy (0.35 for boys; 0.72 for girls) and STDs for girls (0.26). In contrast, youth in the third risk profile initiated tobacco and substance use in preadolescence, but delayed sexual activity thereby rarely experiencing teen pregnancy or STD.
Demographic Variation
The LCA analyses revealed that profiles of adolescent risk varied for boys and girls, and required separate models. Although similarities emerged across gender in the number and characteristics of several classes, differences also emerged, reflecting the importance of considering gender in modeling developmental processes of risk. In addition, prior studies have documented earlier ages of initiation of sexual activity among African American youth compared with European-American youth (Doljanac and Zimmerman 1998). In the present study, a large majority of the African American youth in the sample were assigned to risk class 1 or 2, which conveyed the highest risk for pregnancy and STD (72 % of the African American boys; 57 % of the African American girls). The dramatic differences in sexual risk associated with ethnicity/race that are evident here suggest that more focused efforts are needed to understand the factors that contribute to early and risky sexual activity among urban African American youth. As an important limitation, it should be noted that in this sample, the urban African American youth experienced a higher level of adversity than the urban European American youth on a number of dimensions, including higher rates of family and community poverty, greater exposure to neighborhood violence and disadvantaged schools. Hence, in this context, race may be a proxy for a host of contextual factors that increase risk and reduce opportunities for resilience.
Childhood Predictors and Preadolescent Characteristics Associated with Risk Profiles
The predominant model guiding our understanding of developmental mechanisms contributing to the co-occurrence of adolescent antisocial behavior, substance use, and risky sexual activity is problem behavior theory (Udry et al. 1995). In this model, high levels of aggressive-disruptive behavior in childhood are viewed as a common risk factor for all three adolescent problems, as they reflect a rebellious orientation toward authority and lack of social control. As youth move into the early adolescent years and transition into middle school, their opportunities for rule-breaking behaviors are enhanced by reduced adult monitoring, increased mobility, and increased opportunity to affiliate with other deviant peers who provide exposure, access to, and encouragement for a range of acting-out behaviors, including sexual activity, tobacco, and alcohol/drug use (Ellickson et al. 2001).
The current findings are consistent with the developmental model posited by problem behavior theory, in the sense that a significant proportion of children with early aggressive-disruptive behaviors exhibited one of two patterns of adolescent problem behaviors that included heightened risk for negative sexual outcomes (pregnancy, STDs). However, these two patterns differed significantly, with one involving the very early initiation of the tri-morbid array of risky behaviors (tobacco, alcohol/drug use, and risky sexual activity) and the other representing a pattern of delayed risk that involved the initiation of problem behaviors in mid-adolescence (without associated alcohol/drug use among the girls). Relative to the low-risk class, the two classes with heightened risk for negative sexual outcomes (classes 1 or 2) shared a set of early childhood risks. Common kindergarten characteristics included elevated inattention, low family SES, and low parental warmth relative to the low-risk class. In addition, all except the girls in the adolescent dual-problem class also had higher levels of aggression, lower cognitive ability, and (among boys) reading difficulties at kindergarten entry relative to youth who emerged in the low-risk class. These are descriptive associations, and hence causality cannot be inferred. These two groups differed in the area of preadolescent risk. Whereas those in class 1 (preadolescent multi-problem) were elevated on the preadolescent risk factors, youth in class 2 (adolescent dual- or multi-problem) were elevated only on preadolescent school maladjustment. These findings suggest that childhood experiences require closer attention as precursors to early sexual risk, as children with early inattention and low levels of family support may be especially at-risk for cascading school maladjustment and the initiation of sexual activity – even when youth do not experience preadolescent risks or the early initiation of substance use.
In contrast, another risk group was characterized by a pattern of preadolescent substance use initiation without co-occurring risky sexual activity or risk for STDs or unintended pregnancy. Youth in this class did not show elevated risks in early childhood, with the exception of inattention and reading problems among boys, but relative to the low-risk children they showed elevations on all (or, for boys, almost all) of the preadolescent risk variables studied (early puberty, deviant peer affiliation, school maladjustment). Again, these findings are descriptive and not causal, and need to be replicated in future research. However, they also suggest that early childhood characteristics and family experiences are associated with vulnerability for early sexual activity in ways that are distinct from the effects of preadolescent rebellion. Future research is needed to replicate and extend these findings, and to explore the developmental mechanisms associated with diverging trajectories among the aggressive children. Such research may foster more nuanced developmental models to guide prevention programming. In addition, future research may examine additional risk factors.
Prevention Program Results and Implications
Although the Fast Track intervention successfully reduced the aggression levels of youth in elementary school (CPPRG 2002) and also reduced juvenile arrests and conduct disorder (among the highest risk youth) (CPPRG 2010b, 2011), the present study found no evidence that it delayed the timing of sexual debut, significantly reduced pregnancy or STDs through age 17, or moved youth from higher-risk to lower-risk profiles of tri-morbidity. It is valuable to speculate about the possible reasons for the lack of significant intervention effects. The expectation that Fast Track might reduce risky sexual activity was based upon a developmental model in which child aggression at school entry contributes to a negative cascade, fueling interpersonal conflict (with teachers, peers, and parents) and learning failures that undermine social control and school engagement. By the end of elementary school, alienated and disengaged aggressive youth are vulnerable to the attractions of a deviant life-style that offers easy social affiliation and gratification (e.g., substance use, sexual activity) and allows them to escape from restrictive (often punitive) school demands and behavioral controls (Capaldi et al. 1996; Schofield et al. 2008). Despite Fast Track’s significant intervention impact on the reduction of aggression and promotion of academic skills in elementary school, it appears that the intervention did not substantially change youth vulnerability to the attractions of early adolescent substance use and sexual activity, and hence did not delay the timing of sexual or substance use debut. It is possible that the lack of intervention impact on the timing of early adolescent risk behaviors and risky sex outcomes occurred because the impact on early aggression and learning competencies was too weak to protect youth against the opportunities for deviant peer affiliation in middle school and thereby prevent the negative cascade in adjustment at the transition into middle school. Fast Track effects, while statistically significant, were small to moderate in size, and did not move most youth into “normative” levels of aggression. Alternatively, the negative cascade model, while descriptive, may not be causal. That is, although early aggression may indicate risk for precocious substance use and sexual activity, additional factors may contribute to both aggression and the other outcomes. For example, theorists have also speculated that poor self-regulation and related deficits in key areas of neuropsychological functioning contribute both to over-reactive aggressive responding and also to learning difficulties and impulsive decision-making, including decisions regarding substance use and sexual activity (Crockett et al. 2006; Zimmer-Gembeck et al. 2004). In the present study, kindergarten cognitive skills, including elevated inattention and lower levels of cognitive ability, significantly predicted the earlier initiation of sexual activity and adolescent pregnancy involvement for boys and girls. A critical question for future prevention design is the degree to which these early cognitive skills are malleable in psychosocial interventions and, if so, whether improvements reduce risk for early and unprotected sexual activity.
One additional possibility is that the transition into middle school and its accompanying reduction in adult monitoring and increase in youth affiliation with deviant peers opened new opportunities and support for substance use and sexual activity that were not reduced effectively with the youth-focused case management that Fast Track provided during the middle school years. Interestingly, although child kindergarten characteristics significantly predicted the timing of sexual debut and pregnancy, they were not associated with the timing of tobacco or alcohol/drug use initiation. These concurrent risks appear more heavily associated with peer-group norms and opportunities, and hence require attention to the peer context to reduce risk. Certainly, additional research examining the Fast Track intervention, as well as future research examining alternative intervention approaches is critically needed to better understand causal pathways and mechanisms associated with effective prevention targeting the tri-morbidity of antisocial behavior, substance use, and risky sexual activity among youth with early-starting conduct problems. Given the present findings, an expanded and differentiated prevention model may be needed to address alternative risk/protective mechanisms and diverging developmental trajectories characterizing youth at different developmental periods in varying ecological contexts, particularly over the transition into middle school when the contextual supports and peer-group risks change dramatically.
Limitations
It should be noted that several limitations in the study design may have contributed to the lack of intervention findings. This study examined the timing of onset of problem behaviors and risky sex outcomes through age 17. In addition, the assessment of risky sexual activity was somewhat limited in the Fast Track data through age 17, as youth were not asked to report on multiple partners or other aspects of sexual activity until age 18. Preliminary analyses of follow-up data collected during early adulthood suggest that intervention effects may emerge in some areas of risky sexual activity associated with HIV/AIDS, including multiple partners and condom use. If so, such findings would be consistent with other patterns observed in the Fast Track data in which intervention effects that were evident in elementary school diminished during the middle school years (CPPRG 2010a) but re-emerged in later high school and early adulthood (CPPRG 2010b; 2012). In addition, extended analyses that move beyond these “intent to treat” outcome analyses may be useful, in terms of identifying subgroups for whom the Fast Track prevention program was more effective, and thereby generating ideas for strengthening future prevention program designs that could be tested in future trials.
References
Achenbach, T. M. (1991). Manual for the teacher’s report form and 1991 profile. Burlington: University of Vermont Department of Psychiatry.
Albert, B., Brown, S., & Flanigan, C. (Eds.). (2003). 14 and younger: The sexual behavior of young adolescents. Washington: National Campaign to Prevent Teen Pregnancy.
Bierman, K., Greenberg, M., & CPPRG. (1996). Social skills training in the Fast Track program. In R. Peters & R. McMahon (Eds.), Preventing childhood disorders, substance abuse, and delinquency (pp. 65–89). Thousand Oaks: Sage.
Brendgen, M., Wanner, B., & Vitaro, F. (2007). Peer and teacher effects on the early onset of sexual intercourse. American Journal of Public Health, 97, 2070–2075.
Capaldi, D. M., Crosby, L., & Stoolmiller, M. (1996). Predicting the timing of first sexual intercourse for at-risk adolescent males. Child Development, 67, 344–359.
CPPRG. (2002). Evaluation of the first 3 years of the Fast Track Prevention Trial with children at high risk for adolescent conduct problems. Journal of Abnormal Child Psychology, 30, 19–35.
CPPRG. (2010a). The difficulty of maintaining positive intervention effects: A look at disruptive behavior, deviant peer relations, and social skills during the middle school years. The Journal of Early Adolescence, 30, 593–624.
CPPRG. (2010b). Fast Track intervention effects on youth arrests and delinquency. Journal of Experimental Criminology, 6, 131–157.
CPPRG. (2011). The effects of the Fast Track preventive intervention on the development of conduct disorder across childhood. Child Development, 82, 331–345.
CPPRG. (2012). Impact of early intervention on externalizing psychopathology at age 25. Unpublished manuscript.
Crnic, K., & Greenberg, M. T. (1987). Transactional relationships between perceived family style, risk status, and mother-child interactions in 2 year olds. Journal of Pediatric Psychology, 12, 343–362.
Crockett, L. J., Raffaelli, M., & Shen, Y. (2006). Linking self-regulation and risk proneness to risky sexual behavior: Pathways through peer pressure and early substance use. Journal of Research on Adolescence, 16, 503–525.
DiClemente, R., Wingood, G., Crosby, R., Sionean, C., Brown, L., Rothbaum, B.,…Davies, S. (2001). A prospective study of psychological distress and sexual risk behavior among Black adolescent females. Pediatrics, 108, 85–90.
Dishion, T. J., & Patterson, G. R. (2006). The development and ecology of antisocial behavior. In D. Cicchetti & D. J. Cohen (Eds.), Developmental psychopathology. Vol. 3: Risk, disorder, and adaptation. New York: Wiley.
Doljanac, R. F., & Zimmerman, M. A. (1998). Psychosocial factors and high-risk sexual behavior: Race differences among urban adolescents. Journal of Behavioral Medicine, 21, 451–467.
DuRant, R. H., Smith, J. A., Kreiter, S. R., et al. (1999). The relationship between early age of onset of initial substance use and engaging in multiple health risk behaviors among young adolescents. Archives of Pediatric and Adolescent Medicine, 153, 286–291.
Ellickson, P. L., Tucker, J. S., & Klein, D. J. (2001). High-risk behaviors associated with early smoking: Results from a 5-year follow-up. Journal of Adolescent Health, 28, 465–473.
Gowen, L., Feldman, S., & Diaz, R. (2004). A comparison of the sexual behaviors and attitudes of adolescent girls with older versus similar-aged boyfriends. Journal of Youth and Adolescence, 33, 167–175.
Hipwell, A. E., Keenan, K., Loeber, R., & Battista, D. (2010). Early predictors of sexually intimate behaviors in an urban sample of young girls. Developmental Psychology, 46, 366–378.
Hollingshead, A. A. (1979). Four-factor index of social status. New Haven: Yale University.
Joun, H., Ensminger, M. E., & Sydnor, K. D. (2002). A longitudinal study of developmental trajec-tories to young adult cigarette smoking. Drug and Alcohol Dependency, 66, 303–314.
Kotchick, B. A., Shaffer, A., Forehand, R., & Miller, K. S. (2001). Adolescent sexual risk behavior: A multi-system perspective. Clinical Psychology Review, 21, 493–519.
Lanza, S. T., Collins, L. M., Lemmon, D. R., & Schafer, J. L. (2007). PROC LCA: A SAS procedure for latent class analysis. Structural Equation Modeling, 14, 671–694.
McMahon, R., Slough, N., & CPPRG. (1996). Family-based intervention in the Fast Track Program. In R. Peters & R. McMahon (Eds.), Preventing childhood disorders, substance abuse, and delinquency (pp. 90–110). Thousand Oaks: Sage.
Meshke, L. L., Zweig, J. M., Barber, B. L., & Eccles, J. S. (2000). Demographic, biological, psychological, and social predictors of the timing of first intercourse. Journal of Research on Adolescence, 10, 315–338.
Petersen, A. D., Crockett, L., Richards, M., & Boyer, A. (1988). Self-report measure of pubertal status: Reliability, validity, initial norms. Journal of Youth and Adolescence, 17, 117–133.
Raffaelli, M., & Crockett, L. (2003). Sexual risk taking in adolescence: The role of self-regulation and attraction to risk. Developmental Psychology, 39, 1036–1046.
Ramrakha, S., Bell, M. L., Paul, C., Dickson, N., Moffitt, T. E., & Caspi, M. (2007). Childhood behavior problems linked to sexual risk taking in young adulthood: A birth cohort study. Journal of the American Academy of Child and Adolescent Psychiatry, 46, 1272–1279.
Resnick, M., Bearman, P., Blum, R., Bauman, K., Harris, K., Jones, J., et al. (1997). Protecting adolescents from harm. Findings from the National Longitudinal Study on Adolescent Health. The Journal of the American Medical Association, 278.
Reynolds, W. M., & Mazza, J. J. (1998). Reliability and validity of the Reynolds Adolescent Depression Scale with young adolescents. Journal of School Psychology, 36, 353–376.
Rose, A., Koo, H., Bhaskar, B., Anderson, K., White, G., & Jenkens, R. (2005). The influence of primary caregivers on the sexual behavior of early adolescents. Journal of Adolescent Health, 37, 135–144.
Schofield, H. T., Bierman, K. L., Heinrichs, B., Nix, R. L., & CPPRG. (2008). Predicting early sexual activity with behavior problems exhibited at school entry and in early adolescence. Journal of Abnormal Child Psychology, 36, 1175–1188.
Tucker, J. S., Ellickson, P. L., & Klein, D. J. (2002). Five-year prospective study of risk factors for daily smoking in adolescence among early nonsmokers and experimenters. Journal of Applied Social Psychology, 32, 1588–1603.
Udry, J. R., Kovenock, J., Morris, N. M., & van den Berg, B. J. (1995). Childhood precursors of age at first intercourse for females. Archives of Sexual Behavior, 24, 329–337.
Werthamer-Larsson, L., Kellam, S. G., & Wheeler, L. (1991). Effect of first grade classroom environment on shy behavior, aggressive behavior, and concentration problems. American Journal of Community Psychology, 19, 585–602.
Zimmer-Gembeck, M. J., Siebenbruner, J., & Collins, W. A. (2004). A prospective study of intraindividual and peer influences on adolescents’ heterosexual romantic and sexual behavior. Archives of Sexual Behavior, 33, 381–394.
Zweig, J. M., Lindberg, L. D., & McGinley, K. A. (2001). Adolescent health risk profiles: The co-occurrence of health risks among females and males. Journal of Youth and Adolescence, 30, 707–728.
Acknowledgements
This work was supported by National Institute of Mental Health (NIMH) grants R18 MH48043, R18 MH50951, R18 MH50952, and R18 MH50953. The Center for Substance Abuse Prevention and the National Institute on Drug Abuse also provided support for Fast Track through a memorandum of agreement with the NIMH. This work was also supported in part by Department of Education grant S184U30002, NIMH grants K05MH00797 and K05MH01027, and NIDA grants DA16903, DA017589, and DA015226.
We are grateful for the close collaboration of the Durham Public Schools, the Metropolitan Nashville Public Schools, the Bellefonte Area Schools, the Tyrone Area Schools, the Mifflin County Schools, the Highline Public Schools, and the Seattle Public Schools. We greatly appreciate the hard work and dedication of the many staff members who implemented the project, collected the evaluation data, and assisted with data management and analyses. We particularly express appreciation to Brenda Heinrichs for her work on data analyses for this paper.
Disclosure
Drs. Bierman, Coie, Dodge, Greenberg, Lochman, and McMahon are the developers of the Fast Track curriculum and have a publishing agreement with Oxford University Press. Dr. Greenberg is an author on the PATHS curriculum and has a royalty agreement with Channing-Bete, Inc. Dr. Greenberg is a principal in PATHS Training, LLC. Dr. McMahon is a coauthor of Helping the Noncompliant Child and has a royalty agreement with Guilford Publications, Inc.; he is also a member of the Treatments That Work Scientific Advisory Board with Oxford University Press. The other authors have no financial relationships to disclose.
Author information
Authors and Affiliations
Consortia
Additional information
Members of the Conduct Problems Prevention Research are, in alphabetical order, Karen L. Bierman (Pennsylvania State University), John D. Coie (Duke University), Kenneth A. Dodge (Duke University), Mark Greenberg (Pennsylvania State University), John E. Lochman (University of Alabama), Robert J. McMahon (Simon Fraser University and the Child & Family Research Institute), and Ellen E. Pinderhughes (Tufts University).
Members of the Conduct Problems Prevention Research are, in alphabetical order, Karen L. Bierman (Pennsylvania State University), John D. Coie (Duke University), Kenneth A. Dodge (Duke University), Mark Greenberg (Pennsylvania State University), John E. Lochman (University of Alabama), Robert J. McMahon (Simon Fraser University and the Child & Family Research Institute), and Ellen E. Pinderhughes (Tufts University).
Rights and permissions
About this article
Cite this article
Conduct Problems Prevention Research Group. Trajectories of Risk for Early Sexual Activity and Early Substance Use in the Fast Track Prevention Program. Prev Sci 15 (Suppl 1), 33–46 (2014). https://doi.org/10.1007/s11121-012-0328-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11121-012-0328-8