
Abstract
Glutamate dysfunction has been implicated in a number of substance of abuse studies, including cocaine and methamphetamine. Moreover, in attention-deficit/hyperactivity disorder (ADHD), it has been discovered that when the initiation of stimulant treatment occurs during adolescence, there is an increased risk of developing a substance use disorder later in life. The spontaneously hypertensive rat (SHR) serves as a phenotype for ADHD and studies have found increased cocaine self-administration in adult SHRs when treated with the stimulant methylphenidate (MPH) during adolescence. For this reason, we wanted to examine glutamate signaling in the pre-limbic frontal cortex, a region implicated in ADHD and drug addiction, in the SHR and its progenitor control strain, the Wistar Kyoto (WKY). We chronically implanted glutamate-selective microelectrode arrays (MEAs) into 8-week-old animals and treated with MPH (2 mg/kg, s.c.) for 11 days while measuring tonic and phasic extracellular glutamate concentrations. We observed that intermediate treatment with a clinically relevant dose of MPH increased tonic glutamate levels in the SHR but not the WKY compared to vehicle controls. After chronic treatment, both the SHR and WKY exhibited increased tonic glutamate levels; however, only the SHR was found to have decreased amplitudes of phasic glutamate signaling following chronic MPH administration. The findings from this study suggest that the MPH effects on extracellular glutamate levels in the SHR may potentiate the response for drug abuse later in life. Additionally, these data illuminate a pathway for investigating novel therapies for the treatment of ADHD and suggest that possibly targeting the group II metabotropic glutamate receptors may be a useful therapeutic avenue for adolescents diagnosed with ADHD.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is estimated to affect 6% of children worldwide and over 50% of those diagnosed will continue to suffer into adulthood [1,2,3]. Adolescents and adults diagnosed with ADHD are more likely to suffer from mood and anxiety disorders and to develop drug addiction [4]. Methylphenidate (MPH), a dopamine reuptake inhibitor, is one of the most commonly prescribed treatments for ADHD [5]. Animal studies have established the reinforcing effects of MPH [6] and MPH has also been found to serve as a reinforcer for children diagnosed with ADHD [7]. Debate has been ongoing whether stimulant treatment for ADHD makes one more susceptible to drug abuse later in life. A meta-analysis of the literature concluded that when stimulant treatment for ADHD is initiated during childhood, there is a decreased risk for developing a substance use disorder during adulthood [8]. Conversely, when the initiation of stimulant treatment for ADHD occurs during adolescence, there is an increased risk of developing a substance use disorder [9, 10]. In rodents, exposure to chronic administration of a clinically relevant dose of MPH during adolescence caused the animals to self-administer cocaine more quickly as adults [11]. Furthermore, MPH is not always successful in treating ADHD and occasionally needs to be stopped due to negative side effects [12]. Together, these results suggest that adolescents and adults with ADHD could benefit from novel medications for the treatment of ADHD.
Glutamate dysfunction has been implicated in ADHD in a number of studies, including both preclinical and clinical work. Our laboratory has previously shown that the spontaneously hypertensive rat (SHR), a rodent model of ADHD, has aberrant glutamate signaling [13,14,15] in the frontal cortex compared to its progenitor strain, the Wistar Kyoto (WKY) [16]. Better understanding the role of glutamate in ADHD and discovering drugs that can modulate it properly without direct involvement of the catecholamine pathways could reveal novel treatment options for ADHD. The purpose of this study was to examine the role of tonic and phasic glutamate signaling in the pre-limbic region of the frontal cortex within the freely moving SHR and WKY control rats during an open-field behavior task to measure hyperactivity, a key symptom of ADHD. Additionally, the effects of MPH vs. saline on both tonic and phasic glutamate release were examined in an effort to discover any exertion of the catecholamine sympathomimetic on the glutamate system in order to better characterize novel pharmacotherapies for the treatment of ADHD.
Materials and Methods
Animals
Male, 7 week old spontaneously hypertensive rats (SHR) were obtained from Charles River Laboratories (NCrl, Wilmington, MA) and male, 7 week old Wistar Kyoto (WKY) rats were obtained from Harlan Laboratories (NHsd, Indianapolis, IN). Animals were given access to food and water ad libitum and housed in a 12 h light/dark cycle. All animals remained in a quarantine period for 1 week before experimental procedures to ensure no travel-related stress confounds were possible. During this time, each animal was handled daily to eliminate handling stress during the experiments. Protocols for animal use were approved by the Institutional Animal Care and Use Committee, which is accredited by the Association for Assessment and Accreditation of Laboratory Animal Care International. All procedures were carried out in accordance with the National Institutes of Health Guide for Care and Use of Laboratory Animals.
Microelectrode Array Preparation for Glutamate Measurements
Glutamate-oxidase (GluOx) coated microelectrode arrays (MEAs) consisting of 4 Pt sites measuring 15 × 333 µm arranged vertically in dual pairs (S2 conformation) were used as previously described [16, 17]. After the S2 MEAs were made sensitive for glutamate using 1% bovine serum albumin (BSA; Sigma-Aldrich, St. Louis, MO), 0.125% glutaraldehyde (Glut; Sigma-Aldrich), and 1% GluOx (US biological, Salem, MA), they were built into an implantable head-cap. Both ends of a piece of 1 inch long 30 gauge varnished copper wire (RadioShack, Fort Worth, TX) were scraped (~ 0.25 cm) and fluxed (#186 Rosin flux type RMA, Kester). One end of the copper wire was soldered using a low heat soldering iron (200 °C) to a gold plated-socket (Ginder Scientific, Nepean, ON). The other end of the copper wire was soldered to holes within the stubbed paddle portion of the MEA. The 4 gold pins (one for each Pt recording site) were inserted into a 9 pin ABS plug (Ginder Scientific, Nepean, ON) and the copper wires were wrapped around the body of the ABS plug. A Ag/AgCl reference electrode consisting of a 1 inch Teflon-coated silver wire (200 µm bare, 275 µm coated; A-M Systems, Carlsberg, WA) was scraped similar to the copper wires, soldered into a gold plated-socket and then placed into the ABS plug. The silver wire was electroplated with AgCl in an acidic solution of KCl prior to use as a pseudo reference. Once this Ag/AgCl wire is implanted in contact with brain tissue it becomes a Ag/AgCl reference electrode.The entire assembly was then finished with a heavy layer of water resistant-quality epoxy (Loctite Quick Set Epoxy, Home Depot, Atlanta, GA) and allowed to cure for at least 24 h to ensure a water product [18, 19]. Finally, at least 2 days before the MEAs were surgically implanted, 1,3–phenylenediamine (mPD, Acros, Fisher Scientific, Waltham, MA), a molecular size exclusion layer, was electroplated onto both the GluOx and sentinel sites to eliminate interferent molecules such as ascorbic acid and dopamine from reaching the Pt sites [20].
In Vitro Calibration
High-speed amperometric recordings, displayed at a frequency of 10 Hz, were performed using the FAST16mkIII electrochemical recording system (Fast Analytical Sensing Technology, Quanteon, LLC, Nicholasville, KY). Immediately before in vivo implantation, an in vitro calibration, as described previously [10], was used to determine selectivity (glutamate vs. ascorbic acid), limit of detection (in µM, S/N = 3), and sensitivity (slope, pA/µM). The mean slope, limit of detection and selectivity for electrodes used are presented in Table 1. In addition, the average T90 rise time of the MEAs for glutamate is 0.17 ± 0.07 s (n = 6), which allows for the rapid recordings of both tonic and phasic glutamate. No significant differences in the performance of the MEAs used between strains were observed.
Implantation Surgery
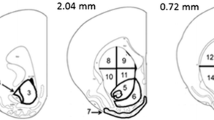
After calibration and selection of MEAs, animals were prepared for aseptic surgery. Immediately before surgery, rats were given injections of carprofen (Rimadyl®, Pfizer, Inc., New York City, NY; 10 mg/kg, s.c.) and 1 ml of 0.9% NaCl (s.c.). Isoflurane (Isothesia, Butler Schein, Dublin, OH) was used as the anesthetic for all survival surgeries. Initial anesthesia was induced with 4% isoflurane, and once the rat was secured in the stereotaxic frame (David Kopf Instruments, Tujunga, California), the isoflurane level was adjusted during surgery (1–3%) dependent on the breathing rate of the animal. Artificial tears (Rugby Laboratories, Inc., Duluth, GA) were applied to the eyes. The head was shaved, and three applications each of Povidone scrub (The Butler Co., Columbus, OH) and ethanol (70%) were used to disinfect the surgery site. A craniotomy was performed, and five holes were drilled: 1 for the MEA, 1 for the reference electrode, and three for anchoring skull screws (Small Parts, part #B00FN0K02). After the skull screws were inserted, dura was reflected and the MEA was stereotaxically placed in the pre-limbic frontal cortex (from bregma: AP + 3.2 mm and ML − 0.8 mm; from the surface of the brain: DV − 3.5 mm) [21]. The reference electrode was then positioned into its placement hole contralateral to the MEA placement, sliding along the underside of the skull. Multiple applications of dental cement (Ortho Jet Powder and Jet Acrylic Liquid, Lang Dental Manufacturing Co., Wheeling, IL) were used to secure the MEA assembly to the skull. The animal was then monitored for the next 2 days and given daily injections of 10 mg/kg carprofen and 1 ml 0.9% NaCl (both administered s.c.). On the third day post-surgery, behavior and glutamate recordings started.
Recording Apparatus
The recording apparatus consisted of a 24″ × 24″ × 24″ wooden box with a 16″ × 16″ open-field activity monitor (Omnitech Electronics Inc., Columbus, OH) inside and was used for all behavioral measures. The 4-channel electrochemical recording head-stage consisted of a miniature ABS socket connector (Ginder Scientific, Nepean ON) with 5 connector pins (1 connecting each of the 4 channels and 1 connecting the reference electrode). The recording assembly hung from the top center of the box from an 18 lead low-torque commutator (Plastics1, Roanoke, VA). This allowed the animal to freely move to all areas of the box [19].
Methylphenidate Administration
Methylphenidate (MPH) HCl [threo-methyl-α-phenyl-α-(2-piperidyl)acetate hydrochloride; M2892; Sigma-Aldrich, St. Louis, MO] was dissolved in 0.9% saline (2 mg/ml solution). Clinically, stimulants are administered orally and exert therapeutic actions at low doses that result in peak plasma concentrations within the range of 8–40 ng/ml [22]. Although MPH is administered orally for the treatment of ADHD, the majority of studies that have examined the behavioral, neurochemical, and electrophysiological actions of stimulants in rodents have used intraperitoneal (i.p.) or subcutaneous (s.c.) administration [23]. Moreover, s.c. administration was used in this study because it has more rapid pharmacokinetics compared to oral administration [24]. Most importantly, this method of administration was easiest to administer while the animal was tethered and in the open-field behavior box.
Behavior and Electrochemical Measures of Extracellular Glutamate
Behavior and glutamate recordings began on the third day post-MEA implant. Recordings occurred during the animal’s light cycle to reduce any effects of foraging [25]. The majority of studies focused on SHR behavior have been completed during the light cycle [26, 27] and studies have shown that MPH administration during the dark cycle failed to produce sensitization [28]. The animal was removed from the home cage, tethered to the commutator for glutamate recordings, and placed into the behavior box. The total distance traveled was measured in 1 min time bins over the course of the session using Oasis software. In one group of SHR and WKY rodents, a saline injection (s.c.) was administered at an hour after the start of the experiment. MPH was given (2 mg/kg, s.c.) 1 h later. The animal was then left in the behavior box for another 3 h for behavior and glutamate recordings (Fig. 1a). In a second group of SHR and WKY rodents, a saline injection (s.c.) was administered at an hour after the start of the experiment. Saline was given again (2 mg/kg, s.c.) 1 h later. The animal was then left in the behavior box for another 3 h for behavior and glutamate recordings. During the final 10 min, the voltage applied was changed to + 0.2 V vs. the Ag/AgCl reference electrode, which removed the oxidation of H2O2 on the MEA Pt recording sites and thereby further confirming peroxide-mediated measurements and the detection of glutamate recorded by the MEAs. The animal was then removed from the recording apparatus and returned to its home cage. On the second day, the same process, minus tethering to the commutator, was performed. Previous experiments from our laboratory have shown that this process reduces the stress on the area around the head-cap and ensures 2 weeks of possible experimentation (pilot data, unpublished). Alternate days of tethering then continued for a total of 11 days (Fig. 1b). After each recording session, the recording chamber was cleaned with Roccal disinfectant (Pfizer, Inc., New York City, NY). Additionally, the experimenter occasionally entered the room to monitor the animal and check to ensure that the tether was not tangled.

Experiment timeline. a Each day started with the animal being placed into the behavior box to allow for an hour of baseline activity. A saline injection (s.c.) was used to determine any injection effects on behavior and glutamate signaling. Glutamate levels were assessed roughly 30 min post-saline administration. Next, either saline or MPH was given (s.c.) and three glutamate time-points were sampled. The experiment ended 3 h after the 2nd injection. b The S2 MEA was implanted on day 0 and the animal was allowed 2 days to recover from surgery. On day 3, glutamate and behavior recordings began. Behavior was completed each day in the open-field box, whereas glutamate recordings were performed on alternate days. (Color figure online)
Histology
Following completion of the 2 week drug administration, the animals were euthanized and brains were removed and processed (frozen) for histological evaluation of microelectrode recording tracks.
Data Analyses
Collected glutamate data were analyzed using a custom Matlab®-based analysis package. Fig. 1a explains the experiment timeline and how the large amount of data was analyzed. Data for each animal was organized into 3 blocks to examine drug effects: (1) acute, day 1 or day 3; (2) intermediate, day 5 or day 7; and (3) chronic, day 9 or day 11. Next, a boxcar filter, or moving average, of 20 points was applied to the raw glutamate data file. The data file was then separated into 4 separate 10 min files per animal per block: (1) saline (90 min after the start of experiment), (2) treatment 1 (30 min post-treatment or 150 min after the start of experiment), (3) treatment 2 (80 min post-treatment or 200 min after the start of experiment), and (4) treatment 3 (130 min post-treatment or 250 min after start of experiment). This created 12 separate data files for each animal. For phasic events, the parameters were as follows: S/N > 2, positive peak area and peak amplitude, and a phasic rise time of ≥ 250 ms. Tonic glutamate measurements were sampled during the first positive phasic peak baseline from each data file. Using the above criteria, 8 out of 30 total animals were excluded from intermediate treatment tonic glutamate levels. 10 out of 30 animals were excluded from chronic treatment tonic glutamate levels. All data were analyzed using two-way repeated measures ANOVAs followed by Bonferroni corrections for multiple comparisons (GraphPad Prism 6.0). For all data, significance was set to p < 0.05.
Results
Acute, Intermediate, and Chronic Effects of a Clinically Relevant Dose of Methylphenidate on Total Distance Traveled in the Open-Field Behavior Task
For acute drug effects on behavior, a significant interaction between strain/treatment (WKY saline, WKY MPH, SHR saline, SHR MPH) and time (300 one min bins) (F897,5083 = 1.717, p < 0.0001) as well as significant effects of strain/treatment (F3,17 = 23.57, p < 0.0001) and time (F299,5083 = 4.471, p < 0.0001) were found. Baseline activity during the first day of behavioral recordings was similar between the SHR and WKY, consistent with previous reports that the hyperactive behaviors of the SHR model of ADHD are absent in a novel environment [29, 30]. Administration of saline (s.c.) also did not produce any significant differences between strains. The difference in activity started 30 min following treatment. The SHR treated with MPH had significantly higher total distance traveled than the SHR treated with saline. Additionally, the SHR MPH group had greater activity than the WKY MPH group. These differences lasted for about 90 min before the groups again displayed similar activity (Fig. 2a). These results are consistent with previous studies reporting that a low, clinically relevant dose of MPH increased activity in the SHR [31, 32].

Total distance traveled: effects of methylphenidate. Baseline activity of the SHR and WKY strains was similar, as was the activity following saline (s.c.) administration (orange arrow) for acute and intermediate recordings. a Beginning 30 min after treatment (green arrow, 2 mg/kg s.c.), the SHR treated with MPH for the first time (pink circles) was found to have significantly increased total distance traveled compared to the SHR saline group (open black circles, *p < 0.05) as well as the WKY treated with MPH group (blue triangles, xp < 0.05). This effect lasted roughly 90 min. b Beginning 30 min after intermediate treatment with MPH (green arrow, 2 mg/kg s.c.), the SHR treated with MPH (pink circles) was found to have significantly increased total distance traveled compared to the SHR saline group (open black circles, *p < 0.05) as well as the WKY treated with MPH group (blue triangles, xp < 0.05). This effect lasted roughly 120 min. c The SHR: MPH (pink) and SHR: saline (black) groups were found to have increased activity during the first 5 min of baseline compared to both WKY groups (xp < 0.05 vs. WKY: MPH; •p < 0.05 vs. WKY: saline). The activity following saline (s.c.) administration (orange arrow) was similar between all groups. Beginning 30 min after treatment (green arrow, 2 mg/kg s.c.), the SHR chronically treated with MPH (pink circles) was found to have significantly increased total distance traveled compared to the SHR saline group (open black circles, *p < 0.05). The SHR: MPH group was also found to have increased activity compared to the WKY treated with MPH group (blue triangles, xp<0.05), beginning 90 min post-MPH and this effect only lasted for about 30 min. 1 min bins. Mean ± SEM. (Color figure online)
For intermediate drug effects on behavior, a significant interaction between strain/treatment and time (F897,5083 = 3.110, p < 0.0001) as well as significant effects of strain/treatment (F3,17 = 9.153, p = 0.0008) and time (F299,5083 = 4.628, p < 0.0001) were found. Baseline activity was found to be similar between the SHR and WKY and saline (s.c.) did not produce any significant differences between strains. The difference in activity started 30 min after treatment, similar to the acute recording. The SHR treated with MPH had significantly higher total distance traveled than the SHR treated with saline. Additionally, the SHR: MPH group displayed increased activity compared to the WKY: MPH group (Fig. 2b). These differences lasted longer than they did for the acute recordings. It took nearly 120 min before the groups again displayed similar activity.
For chronic drug effects on behavior, a significant interaction between strain/treatment and time (F897,5083 = 1.805, p < 0.0001) as well as significant effects of strain/treatment (F3,17 = 7.293, p = 0.003) and time (F299,5083 = 3.637, p < 0.0001) were found. The SHR, regardless of treatment, displayed increased activity during the first 5 min of the experiment compared to both groups of the WKY, consistent with reports that the hyperactive behaviors of the SHR model of ADHD become evident after multiple exposures to an environment [30, 33, 34]. Administration of saline (s.c.) did not produce any significant differences between strains. The difference in activity started 30 min after treatment, when the SHR treated with MPH had significantly more total distance traveled than the SHR treated with saline (Fig. 2c). These differences lasted for 120 min before the groups again displayed similar activity. The SHR MPH group also had increased activity than the WKY treated with MPH group, beginning 90 min post-MPH and this effect only lasted for approximately 30 min.
Examination of Tonic and Phasic Extracellular Glutamate Signaling
Fig. 3 shows an example of tonic and phasic glutamate signaling over the course of the 5 h experiment in one animal. Three major types of phasic signaling are apparent: (1) fast single peaks (5–10 s long), (2) fast multi-peaks (5–10 s long), and (3) slower phasic signaling (1–3 min long), which consisted of many fast multi- and single-peaks (see Fig. 6 and data, below). Figure 3 shows the differences in tonic and phasic glutamate between strains and treatments. Additionally, Figure 3 shows the change in applied potential from + 0.7 to + 0.2 V vs. Ag/AgCl reference electrode, which is below the H2O2 oxidation potential and used to further confirm the detection of glutamate by the MEAs.

Strain differences in tonic and phasic glutamate levels. Post-baseline of the S2 MEA, strain differences were observed in tonic and phasic glutamate levels. Only the raw, subtracted glutamate signal is represented here for all study groups. Black, WKY saline. Blue, WKY MPH. Grey, SHR saline. Pink, SHR MPH. Orange arrow, saline (s.c.). Green arrow, methylphenidate (2 mg/kg, s.c.). Purple arrow marks when the applied voltage changed from + 0.7 to + 0.2 V vs. Ag/AgCl reference electrode, to test for the detection of glutamate. (Color figure online)
Intermediate Methylphenidate Treatment Increases Tonic Glutamate Levels in the SHR But Not the WKY
A significant effect of time (30 min after saline, and 30, 80, and 130 min after treatment) (F3,36 = 2.866, p < 0.05) and an effect of strain/treatment (WKY saline, WKY MPH, SHR saline, and SHR MPH) (F3,12 = 3.710, p < 0.05) after intermediate treatment with MPH/saline were found and seen in Fig. 4a, though no interaction between the two existed. This data demonstrates that the SHR treated with MPH (6.2 ± 1.4 µM) for 1 week has higher tonic levels than the SHR treated with saline alone (1.3 ± 1.4 µM). Additionally, the WKY saline group (6.4 ± 1.4 µM) had higher tonic glutamate than the SHR saline group. The WKY MPH group (5.0 ± 1.3 µM) was not significantly different than the other groups (Fig. 4a).

Intermediate and chronic effects of MPH. (2 mg/kg) administration on tonic glutamate levels. a The SHR MPH group (pink circles) had higher tonic glutamate levels than the SHR saline (open circles) and suggests that MPH brings tonic levels of the SHR up to that of the WKY control (blue triangles), which had similar tonic levels when treated with MPH or saline (black triangles). Additionally, the WKY saline group had higher tonic glutamate than SHR saline. b Following chronic treatment, both the SHR model of ADHD and the WKY control were observed to have increased tonic glutamate compared to animals treated with saline only. *p < 0.05. Mean ± SEM. (Color figure online)
Chronic Methylphenidate Treatment Increases Tonic Glutamate Levels in Both the SHR and WKY
Following chronic treatment, a significant interaction between time and strain/treatment (F9,39 = 2.433, p < 0.05) and an effect of strain/treatment (F3,13 = 4.009, p < 0.05) on tonic glutamate were found and seen in Fig. 4b. These data demonstrate that in both the SHR model of ADHD and the WKY control, chronic MPH treatment with a clinically relevant dose (SHR MPH 9.9 ± 2.1 µM, WKY MPH 10 ± 1.9 µM) increases tonic levels of glutamate compared to animals treated with saline alone (SHR saline 3.2 ± 2.1 µM, WKY saline 3.3 ± 2.1 µM) (Fig. 4b).
Chronic, But Not Intermediate, Methylphenidate Treatment Reduces Phasic Glutamate Signaling in the SHR
Figure 5a, b reveal that the number of phasic events per 10 min sample did not differ between strain, treatment, nor time. After intermediate drug treatment, no differences in the amplitude of phasic glutamate signals were found. Average (± SEM) phasic amplitudes during intermediate treatment were as follows: WKY saline 0.40 ± 0.033 µM, WKY MPH 0.21 ± 0.018 µM, SHR saline 0.13 ± 0.016 µM, SHR MPH 0.22 ± 0.044 µM (Fig. 5c).

Intermediate and chronic effects of MPH (2 mg/kg) administration on phasic glutamate signaling frequency. a, b The number of phasic events per 10 min sample did not differ between strain, treatment, nor time. c The phasic glutamate amplitude did not differ by group following intermediate treatment. d Following chronic administration of MPH, the SHR displayed lower phasic glutamate amplitude compared to the SHR saline group at all time points. *p < 0.05. Mean ± SEM. (Color figure online)
Following chronic treatment, a significant effect of strain/treatment (WKY saline, WKY MPH, SHR saline, SHR MPH) on phasic glutamate amplitudes (F3,22 = 3.316, p < 0.05) was observed. Also, there was a trend towards an effect of time (F3,66 = 2.413, p = 0.07). These data demonstrate that in the SHR, a significant difference existed between the MPH (SHR MPH 0.11 ± 0.0056 µM) and saline treated animals (SHR saline 0.53 ± 0.0072 µM). No effects of chronic MPH treatment on phasic glutamate amplitude were found in the WKY groups (WKY saline 0.13 ± 0.011 µM, WKY MPH 0.22 ± 0.011 µM) (Fig. 5d).
Types of Phasic Signaling Changes with Methylphenidate Treatment
Following intermediate treatment, (30 min after treatment), a significant interaction between strain/treatment (WKY saline, WKY MPH, SHR saline, SHR MPH) and type of event (rapid single, rapid multi, slow) was discovered (F6,52 = 7.311, p < 0.0001). Significant effects of strain/treatment (F3,26 = 10.55, p = 0.001) and type of event (F2,52 = 46.71, p < 0.0001) were also found to exist. The WKY saline group had less of the rapid single peaks compared to the WKY MPH and SHR saline groups. The SHR MPH had significantly more of the rapid multi peaks compared to the WKY MPH and significantly more rapid multi and slow phasic events compared to the SHR saline group (Fig. 6a).

Differences in phasic signal types. a Following intermediate treatment, during the first 10 min sample period (30 min post-treatment), it was observed that the WKY saline group had less rapid single peaks than the WKY MPH and SHR saline groups. The SHR MPH had more rapid multi peaks compared to the WKY MPH and more rapid multi and slow phasic events than the SHR saline group. b Following chronic treatment, during the first 10 min sample period (30 min post-treatment), the SHR saline group had more rapid single peaks than the WKY saline and the SHR MPH groups. The SHR MPH had more slow phasic events than the SHR saline group. Raw single races representing the three major types of phasic signaling are shown: c fast single peaks, d fast multi-peaks, and e slow phasic signaling. *p < 0.05. Mean ± SEM. (Color figure online)
Following chronic treatment (30 min after treatment), a significant interaction between strain/treatment and type of event was found (F6,52 = 8.120, p < 0.0001). A significant effect of type of event (F2,52 = 97.79, p < 0.0001) was also found. The SHR saline group was observed to have more of the rapid single peaks compared to the WKY saline and the SHR MPH groups. The SHR MPH had more slow phasic events than the SHR saline group (Fig. 6b). An example of the three major types of phasic signaling are represented in Fig. 6c–e.
Discussion
The results from this study demonstrate that tonic glutamate levels in the SHR model of ADHD were higher in the methylphenidate (MPH) treated group than the saline treated group. The links between alterations in glutamate neurotransmission and substances of abuse have been well established in such drugs as cocaine [35,36,37], amphetamine [35], and methamphetamine [37]. Given the role of glutamate on the addictive properties of these drugs, we sought to investigate the role of glutamate signaling following chronic MPH administration. Because the SHR model of ADHD self-administers cocaine more readily than the progenitor control strain, the WKY [11], the presently observed increases of tonic glutamate levels following MPH administration in the SHR may suggest a predisposition for drug abuse later in life. Supporting this theory, the SHR was discovered to be more likely to self-administer cocaine as an adult than saline-treated SHRs following chronic treatment with a clinically relevant dose of MPH (administered p.o.) at a young age [11]. Interestingly, SHRs chronically administered the non-stimulant atomoxetine as adolescents were no more likely to self-administer cocaine in adulthood [38], demonstrating that non-stimulant medications may represent an important alternative for the treatment of ADHD. Future studies should examine if increases in glutamate are observed following chronic treatment with atomoxetine within the SHR.
In addition to increased tonic glutamate following MPH treatment in the SHR, we found that chronic exposure to MPH decreased the amplitude of phasic glutamate signaling in the SHR but not the WKY control. The high tonic glutamate in the SHR model of ADHD following chronic MPH treatment does not cause an increase in the phasic release of glutamate, but instead decreases the phasic signaling amplitude without changing the frequency. It is possible that the rise of tonic glutamate levels following MPH treatment causes activation of metabotropic glutamate auto-receptors (e.g. mGluR2/3), attempting to compensate for the higher synaptic and extra-synaptic glutamate concentrations [39,40,41]. Interestingly, research has been focused on group II and III inhibitory metabotropic glutamate auto-receptors, linking them as possible therapeutic targets for anxiety [42, 43], schizophrenia [44], depression [45], alcoholism [46], and cocaine addiction [47]. The results from this study suggest that ADHD should now be included as a disorder that could benefit from targeting these auto-receptors. A recent study examining attention deficits caused by nicotine exposure during adolescence found reduced inhibitory group II mGluRs in the PFC. An mGluR2 agonist, allowing for over-stimulation of the mGluR2, was found to restore attention in these animals as adults [48]. These results suggest that targeting the inhibitory auto-receptors to restore basal glutamate signaling could therapeutically benefit individuals with ADHD. Future research should examine the effects of mGluR group II and III agonists, such as LY354740 and related compounds, on glutamate signaling, as well as the effects of these compounds on the ADHD-like behaviors of the SHR [49,50,51].
Methylphenidate (MPH) administration has been found to increase dopamine levels by blocking the dopamine transporter (DAT) [26, 52,53,54,55,56,57], as well as the norepinephrine transporter (NET) in the frontal cortex [58]. The increase in dopamine is thought to be responsible for increased motor activity [59]. Studies of signaling interactions between the dopaminergic and glutamatergic systems demonstrate that stimulation of D2 dopamine receptors is involved in the inhibition of the NMDA receptor, weakening the excitatory response to those neurons [60]. Likewise, activation of D4 receptors decrease AMPA receptors at the synapse [61]. The behavioral effects of a clinically relevant dose of MPH treatment are predictable and have been well established in the spontaneously hypertensive rat (SHR) model of ADHD [62,63,64,65]. We observed that total distance traveled increased in the SHR acutely and chronically following MPH. This increase in activity is consistent with behavioral sensitization in response to chronic MPH treatment [66], though the WKY control failed to reach sensitization levels. No challenge dose was used in this study, as has been done in previous work exploring MPH sensitization [66,67,68] and studies have shown that chronic administration alone isn’t enough to produce behavioral sensitization following low-dose MPH treatment [69] and explains the lack of increased behavior in the control WKY strain following 11 treatment days with MPH. However, the increase in activity of the hyperactive SHR assured that the low, clinically relevant dose of MPH used was appropriate to cause significant behavior effects in the ADHD model but not the control. Future directions should include a less characterized but still relevant to ADHD behavior task, such as delayed discounting, while exploring changes in glutamate and the effects of pharmacology.
Along with the discovery that chronic MPH treatment reduced the amplitude of phasic glutamate signals in the SHR model of ADHD, different types of phasic signaling were observed and found to be changed following treatment with MPH. The rapid temporal response times of the MEA biosensors for glutamate allows for the measures of both tonic and phasic changes in glutamate. To our knowledge, this is the first time that phasic glutamate signaling has been able to be quantified as having different characteristics, though this is not the first time that phasic signaling has been observed in awake, freely-moving animals using the MEA technology [19, 70]. The SHR had more rapid single peaks, lasting about 10 s before returning to baseline, than the WKY control after both intermediate and chronic saline (or vehicle) alone administration, suggesting that the SHR model of ADHD has higher activity of phasic glutamate events. In the SHR, intermediate MPH treatment was found to increase the rapid multi-peaks compared to the SHR saline group, whereas chronic MPH actually decreased these fast multi-peak phasic events in the SHR. The phasic glutamate events, both single and multi-peak are likely a consequence of “bursting activity” of glutamate neurons [71]. Additionally, after chronic treatment with MPH, the SHR had more of the slow phasic type signals, which could take as long as 3 min before returning to a stable baseline, likely representing increased tonic neuronal activity of glutamate projections. These signals seem to contribute more towards the changes in tonic glutamate than the other phasic signals and may explain why the SHR had increased tonic levels following MPH treatment. These data all suggest that targeting tonic and phasic glutamate signaling may be a useful approach for novel ADHD treatments. In addition, our data support that additional electrophysiological recordings in freely moving rats may be needed to better understand the circuitry affected with chronic MPH administration.
Overall, freely-moving glutamate measurements in the SHR model of ADHD were characterized in the pre-limbic region of the frontal cortex following chronic stimulant treatment in the SHR rat model of ADHD and its control, the WKY. Although there is no perfect animal model of ADHD, the results from these experiments demonstrate that the SHR model of ADHD is a great resource for studying dysfunction of ADHD-like behaviors such as hyperactivity. In this study, the stimulant medication MPH increased locomotion in the SHR and differences were also observed on the glutamate system. These findings illustrate a potential avenue for investigating novel therapies for the treatment of ADHD targeting glutamate. Future studies should examine the effects of current FDA-approved pharmacotherapies that are known to target the glutamatergic system, such as memantine and ceftriaxone, on the glutamate and dopamine systems of the SHR. Additionally, these results suggest that targeting the metabotropic mGluRII/III glutamate receptors may be a useful therapeutic avenue for ADHD.
References
Kessler RC, Adler L, Barkley R, Biederman J, Conners CK, Demler O, Faraone SV, Greenhill LL, Howes MJ, Secnik K, Spencer T, Ustun TB, Walters EE, Zaslavsky AM (2006) The prevalence and correlates of adult ADHD in the United States: results from the National Comorbidity Survey Replication. Am J Psychiatry 163(4):716–723
Polanczyk G, de Lima MS, Horta BL, Biederman J, Rohde LA (2007) The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psychiatry 164(6):942–948
Biederman J, Petty CR, Clarke A, Lomedico A, Faraone SV (2011) Predictors of persistent ADHD: an 11-year follow-up study. J Psychiatr Res 45(2):150–155
Biederman J, Petty CR, Evans M, Small J, Faraone SV (2010) How persistent is ADHD? A controlled 10-year follow-up study of boys with ADHD. Psychiatry Res 177(3):299–304
De Sousa A, Kalra G (2012) Drug therapy of attention deficit hyperactivity disorder: current trends. Mens Sana Monogr 10(1):45–69
Collins RJ, Weeks JR, Cooper MM, Good PI, Russell RR (1984) Prediction of abuse liability of drugs using IV self-administration by rats. Psychopharmacology 82(1–2):6–13
Fredericks EM, Kollins SH (2004) Assessing methylphenidate preference in ADHD patients using a choice procedure. Psychopharmacology 175(4):391–398
Wilens TE, Faraone SV, Biederman J, Gunawardene S (2003) Does stimulant therapy of attention-deficit/hyperactivity disorder beget later substance abuse? A meta-analytic review of the literature. Pediatrics 111(1):179–185
Kollins SH, MacDonald EK, Rush CR (2001) Assessing the abuse potential of methylphenidate in nonhuman and human subjects: a review. Pharmacol Biochem Behav 68(3):611–627
Kollins SH (2008) A qualitative review of issues arising in the use of psycho-stimulant medications in patients with ADHD and co-morbid substance use disorders. Curr Med Res Opin 24(5):1345–1357
Harvey RC, Sen S, Deaciuc A, Dwoskin LP, Kantak KM (2011) Methylphenidate treatment in adolescent rats with an attention deficit/hyperactivity disorder phenotype: cocaine addiction vulnerability and dopamine transporter function. Neuropsychopharmacology 36(4):837–847
Cascade E, Kalali AH, Wigal SB (2010) Real-world data on: attention deficit hyperactivity disorder medication side effects. Psychiatry 7(4):13–15
Russell VA (2001) Increased AMPA receptor function in slices containing the prefrontal cortex of spontaneously hypertensive rats. Metab Brain Dis 16(3–4):143–149
Lehohla M, Kellaway L, Russell VA (2004) NMDA receptor function in the prefrontal cortex of a rat model for attention-deficit hyperactivity disorder. Metab Brain Dis 19(1–2):35–42
Warton FL, Howells FM, Russell VA (2009) Increased glutamate-stimulated release of dopamine in substantia nigra of a rat model for attention-deficit/hyperactivity disorder-lack of effect of methylphenidate. Metab Brain Dis 24(4):599–613
Miller EM, Pomerleau F, Huettl P, Gerhardt GA, Glaser PE (2014). Aberrant glutamate signaling in the prefrontal cortex and striatum of the spontaneously hypertensive rat model of attention-deficit/hyperactivity disorder. Psychopharmacology 231(15):3019–3029
Burmeister JJ, Davis VA, Quintero JE, Pomerleau F, Huettl P, Gerhardt GA (2013) Glutaraldehyde cross-linked glutamate oxidase coated microelectrode arrays: selectivity and resting levels of glutamate in the CNS. ACS Chem Neurosci 4(5):721–728
Rutherford EC, Pomerleau F, Huettl P, Stromberg I, Gerhardt GA (2007) Chronic second-by-second measures of L-glutamate in the central nervous system of freely moving rats. J Neurochem 102(3):712–722
Hascup KN, Hascup ER, Stephens ML, Glaser PE, Yoshitake T, Mathe AA, Gerhardt GA, Kehr J (2011) Resting glutamate levels and rapid glutamate transients in the prefrontal cortex of the flinders sensitive line rat: a genetic rodent model of depression. Neuropsychopharmacology 36(8):1769–1777
Hinzman JM, Thomas TC, Burmeister JJ, Quintero JE, Huettl P, Pomerleau F, Gerhardt GA, Lifshitz J (2010) Diffuse brain injury elevates tonic glutamate levels and potassium-evoked glutamate release in discrete brain regions at two days post-injury: an enzyme-based microelectrode array study. J Neurotrauma 27(5):889–899
Paxinos G, Watson C (2009). The rat brain in stereotaxic coordinates. Academic Press/Elsevier, Amsterdam
Swanson JM, Volkow ND (2002) Pharmacokinetic and pharmacodynamic properties of stimulants: implications for the design of new treatments for ADHD. Behav Brain Res 130(1–2):73–78
Kuczenski R, Segal DS (2005) Stimulant actions in rodents: implications for attention-deficit/hyperactivity disorder treatment and potential substance abuse. Biol Psychiatry 57(11):1391–1396
Wargin W, Patrick K, Kilts C, Gualtieri CT, Ellington K, Mueller RA, Kraemer G, Breese GR (1983) Pharmacokinetics of methylphenidate in man, rat and monkey. J Pharmacol Exp Ther 226(2):382–386
Jensen GB, Collier GH, Medvin MB (1983) A cost-benefit analysis of nocturnal feeding in the rat. Physiol Behav 31(4):555–559
Kuczenski R, Segal DS (2001) Locomotor effects of acute and repeated threshold doses of amphetamine and methylphenidate: relative roles of dopamine and norepinephrine. J Pharmacol Exp Ther 296(3):876–883
Mc Fie S, Sterley TL, Howells FM, Russell VA (2012) Clozapine decreases exploratory activity and increases anxiety-like behaviour in the Wistar-Kyoto rat but not the spontaneously hypertensive rat model of attention-deficit/hyperactivity disorder. Brain Res 1467:91–103
Kuczenski R, Segal DS (2002) Exposure of adolescent rats to oral methylphenidate: preferential effects on extracellular norepinephrine and absence of sensitization and cross-sensitization to methamphetamine. J Neurosci 22(16):7264–7271
Johansen EB, Sagvolden T, Kvande G (2005) Effects of delayed reinforcers on the behavior of an animal model of attention-deficit/hyperactivity disorder (ADHD). Behav Brain Res 162(1):47–61
Howells FM, Bindewald L, Russell VA (2009) Cross-fostering does not alter the neurochemistry or behavior of spontaneously hypertensive rats. Behav Brain Funct 5:24
Yang PB, Amini B, Swann AC, Dafny N (2003) Strain differences in the behavioral responses of male rats to chronically administered methylphenidate. Brain Res 971(2):139–152
Amini B, Yang PB, Swann AC, Dafny N (2004) Differential locomotor responses in male rats from three strains to acute methylphenidate. Int J Neurosci 114(9):1063–1084
Knardahl S, Sagvolden T (1981) Regarding hyperactivity of the SHR in the open-field test. Behav Neural Biol 32(2):274–275
Sagvolden T, Pettersen MB, Larsen MC (1993) Spontaneously hypertensive rats (SHR) as a putative animal model of childhood hyperkinesis: SHR behavior compared to four other rat strains. Physiol Behav 54(6):1047–1055
Pulvirenti L, Swerdlow NR, Koob GF (1989) Microinjection of a glutamate antagonist into the nucleus accumbens reduces psychostimulant locomotion in rats. Neurosci Lett 103(2):213–218
Pulvirenti L, Swerdlow NR, Koob GF (1991) Nucleus accumbens NMDA antagonist decreases locomotor activity produced by cocaine, heroin or accumbens dopamine, but not caffeine. Pharmacol Biochem Behav 40(4):841–845
Witkin JM (1993) Blockade of the locomotor stimulant effects of cocaine and methamphetamine by glutamate antagonists. Life Sci 53(24):PL405-410
Somkuwar SS, Jordan CJ, Kantak KM, Dwoskin LP (2013) Adolescent atomoxetine treatment in a rodent model of ADHD: effects on cocaine self-administration and dopamine transporters in frontostriatal regions. Neuropsychopharmacology 38(13):2588–2597
Lin HC, Wang SJ, Luo MZ, Gean PW (2000) Activation of group II metabotropic glutamate receptors induces long-term depression of synaptic transmission in the rat amygdala. J Neurosci 20(24):9017–9024
Johnson KA, Niswender CM, Conn PJ, Xiang Z (2011) Activation of group II metabotropic glutamate receptors induces long-term depression of excitatory synaptic transmission in the substantia nigra pars reticulata. Neurosci Lett 504(2):102–106
Tang ZQ, Liu YW, Shi W, Dinh EH, Hamlet WR, Curry RJ, Lu Y (2013) Activation of synaptic group II metabotropic glutamate receptors induces long-term depression at GABAergic synapses in CNS neurons. J Neurosci 33(40):15964–15977
Swanson CJ, Bures M, Johnson MP, Linden AM, Monn JA, Schoepp DD (2005) Metabotropic glutamate receptors as novel targets for anxiety and stress disorders. Nat Rev Drug Discov 4(2):131–144
Riaza Bermudo-Soriano C, Perez-Rodriguez MM, Vaquero-Lorenzo C, Baca-Garcia E (2012) New perspectives in glutamate and anxiety. Pharmacol Biochem Behav 100(4):752–774
Hashimoto K, Malchow B, Falkai P, Schmitt A (2013) Glutamate modulators as potential therapeutic drugs in schizophrenia and affective disorders. Eur Arch Psychiatry Clin Neurosci 263(5):367–377
Chaki S, Ago Y, Palucha-Paniewiera A, Matrisciano F, Pilc A (2013) mGlu2/3 and mGlu5 receptors: potential targets for novel antidepressants. Neuropharmacology 66:40–52
Holmes A, Spanagel R, Krystal JH (2013) Glutamatergic targets for new alcohol medications. Psychopharmacology 229(3):539–554
Li X, Xi ZX, Markou A (2013) Metabotropic glutamate 7 (mGlu7) receptor: a target for medication development for the treatment of cocaine dependence. Neuropharmacology 66:12–23
Counotte DS, Goriounova NA, Li KW, Loos M, van der Schors RC, Schetters D, Schoffelmeer AN, Smit AB, Mansvelder HD, Pattij T, Spijker S (2011) Lasting synaptic changes underlie attention deficits caused by nicotine exposure during adolescence. Nat Neurosci 14(4):417–419
Hascup ER, Hascup KN, Pomerleau F, Huettl P, Hajos-Korcsok E, Kehr J, Gerhardt GA (2012) An allosteric modulator of metabotropic glutamate receptors (mGluR(2)), (+)-TFMPIP, inhibits restraint stress-induced phasic glutamate release in rat prefrontal cortex. J Neurochem 122(3):619–627
Koltunowska D, Gibula-Bruzda E, Kotlinska JH (2013) The influence of ionotropic and metabotropic glutamate receptor ligands on anxiety-like effect of amphetamine withdrawal in rats. Prog Neuropsychopharmacol Biol Psychiatry 45:242–249
Wang MJ, Li YC, Snyder MA, Wang H, Li F, Gao WJ (2013) Group II metabotropic glutamate receptor agonist LY379268 regulates AMPA receptor trafficking in prefrontal cortical neurons. PLoS ONE 8(4):e61787
Kuczenski R, Segal DS (1997) Effects of methylphenidate on extracellular dopamine, serotonin, and norepinephrine: comparison with amphetamine. J Neurochem 68(5):2032–2037
Gerasimov MR, Franceschi M, Volkow ND, Gifford A, Gatley SJ, Marsteller D, Molina PE, Dewey SL (2000) Comparison between intraperitoneal and oral methylphenidate administration: a microdialysis and locomotor activity study. J Pharmacol Exp Ther 295(1):51–57
Gerasimov MR, Franceschi M, Volkow ND, Rice O, Schiffer WK, Dewey SL (2000) Synergistic interactions between nicotine and cocaine or methylphenidate depend on the dose of dopamine transporter inhibitor. Synapse 38(4):432–437
Volkow ND, Wang G, Fowler JS, Logan J, Gerasimov M, Maynard L, Ding Y, Gatley SJ, Gifford A, Franceschi D (2001) Therapeutic doses of oral methylphenidate significantly increase extracellular dopamine in the human brain. J Neurosci 21(2):RC121
Huff JK, Davies MI (2002) Microdialysis monitoring of methylphenidate in blood and brain correlated with changes in dopamine and rat activity. J Pharm Biomed Anal 29(5):767–777
Marsteller DA, Gerasimov MR, Schiffer WK, Geiger JM, Barnett CR, Schaich Borg J, Scott S, Ceccarelli J, Volkow ND, Molina PE, Alexoff DL, Dewey SL (2002) Acute handling stress modulates methylphenidate-induced catecholamine overflow in the medial prefrontal cortex. Neuropsychopharmacology 27(2):163–170
Gatley SJ, Pan D, Chen R, Chaturvedi G, Ding YS (1996) Affinities of methylphenidate derivatives for dopamine, norepinephrine and serotonin transporters. Life Sci 58(12):231–239
Rebec GV (2006) Behavioral electrophysiology of psychostimulants. Neuropsychopharmacology 31(11):2341–2348
Kotecha SA, Oak JN, Jackson MF, Perez Y, Orser BA, Van Tol HH, MacDonald JF (2002) A D2 class dopamine receptor transactivates a receptor tyrosine kinase to inhibit NMDA receptor transmission. Neuron 35(6):1111–1122
Yuen EY, Liu W, Kafri T, van Praag H, Yan Z (2010) Regulation of AMPA receptor channels and synaptic plasticity by cofilin phosphatase Slingshot in cortical neurons. J Physiol 588(Pt 13):2361–2371
Wultz B, Sagvolden T, Moser EI, Moser MB (1990) The spontaneously hypertensive rat as an animal model of attention-deficit hyperactivity disorder: effects of methylphenidate on exploratory behavior. Behav Neural Biol 53(1):88–102
Sagvolden T, Metzger MA, Schiorbeck HK, Rugland AL, Spinnangr I, Sagvolden G (1992) The spontaneously hypertensive rat (SHR) as an animal model of childhood hyperactivity (ADHD): changed reactivity to reinforcers and to psychomotor stimulants. Behav Neural Biol 58(2):103–112
van den Bergh FS, Bloemarts E, Chan JS, Groenink L, Olivier B, Oosting RS (2006) Spontaneously hypertensive rats do not predict symptoms of attention-deficit hyperactivity disorder. Pharmacol Biochem Behav 83(3):380–390
Barron E, Yang PB, Swann AC, Dafny N (2009) Adolescent and adult male spontaneous hyperactive rats (SHR) respond differently to acute and chronic methylphenidate (Ritalin). Int J Neurosci 119(1):40–58
Crawford CA, McDougall SA, Meier TL, Collins RL, Watson JB (1998) Repeated methylphenidate treatment induces behavioral sensitization and decreases protein kinase A and dopamine-stimulated adenylyl cyclase activity in the dorsal striatum. Psychopharmacology 136(1):34–43
Gaytan O, al-Rahim S, Swann A, Dafny N (1997) Sensitization to locomotor effects of methylphenidate in the rat. Life Sci 61(8):PL101–PL107
McDougall SA, Collins RL, Karper PE, Watson JB, Crawford CA (1999) Effects of repeated methylphenidate treatment in the young rat: sensitization of both locomotor activity and stereotyped sniffing. Exp Clin Psychopharmacol 7(3):208–218
Suzuki T, Shindo K, Miyatake M, Kurokawa K, Higashiyama K, Suzuki M, Narita M (2007) Lack of development of behavioral sensitization to methylphenidate in mice: correlation with reversible astrocytic activation. Eur J Pharmacol 574(1):39–48
Wassum KM, Tolosa VM, Tseng TC, Balleine BW, Monbouquette HG, Maidment NT (2012) Transient extracellular glutamate events in the basolateral amygdala track reward-seeking actions. J Neurosci 32(8):2734–2746
Shepard GM (2003) The synaptic organization of the brain, 3rd edn. Oxford University Press, New York
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Miller, E.M., Quintero, J.E., Pomerleau, F. et al. Chronic Methylphenidate Alters Tonic and Phasic Glutamate Signaling in the Frontal Cortex of a Freely-Moving Rat Model of ADHD. Neurochem Res 44, 89–101 (2019). https://doi.org/10.1007/s11064-018-2483-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11064-018-2483-1