
Abstract
We investigated effects of breast cancer subtype on overall survival (OS), local and distant control, and time from initial diagnosis to brain metastases (BM). We also investigated advances in graded prognostic assessment (GPA) scores. A cohort of 72 patients treated for BM from breast cancer with Gamma Knife stereotactic radiosurgery at our institution from 2000 to 2014 had subtyping available and were used for this study. Median follow up for OS was 12 months and for control was 6 months. OS for luminal, HER2, and triple negative subtypes were 26, 20, and 22 months. OS when stratified by Sperduto et al. (J Clin Oncol 30(4):419–425, 2012) and Subbiah et al. (J Clin Oncol 33(20):2239–2245, 2015) GPAs were similar (p = 0.087 and p = 0.063). KPS and treatment modality were significant for OS (p = 0.002; p = 0.034). On univariate analysis, triple negative subtype and >3 BM were trending and significant for decreased OS (p = 0.084; p = 0.047). On multivariable analysis HER2, triple negative, and >3 BM were significant for OS (p = 0.022; p = 0.040; p = 0.009). Subtype was significant for response on a per lesion basis (p = 0.007). Subtype was trending towards significance when analyzing time from initial diagnosis to BM treatment (p = 0.064). Breast cancer subtype is an important prognostic factor when stratifying breast cancer patients with BM. The addition of number of BM to the GPA is a useful addition and should be further investigated. Subtype has an effect on lesion response, and also on rate of development BM after initial diagnosis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Breast cancer is responsible for 14.0 % of all new cancer diagnoses and 6.8 % of cancer deaths in the US. For those with distant metastases, the 5-year survival rate is 6 % [1]. Breast cancer is the second leading cause of brain metastases (BM), and patients who develop BM have a particularly poor prognosis [2–5]. Estimates of the rate of BM in breast cancer range from 10 to 15 % in all cases to 30 % in those patients with stage IV disease. Patients with the human epidermal growth factor receptor 2 (HER2) or triple negative subtypes have been shown to be especially susceptible to the development of BM [5–13]. In recent studies, the role of breast cancer subtype on survival in brain metastases has begun to be examined and included in prognostic assessments [3, 4].
The original work in development of prognostic indexes for patients with BM dates back to 1997, with the development of Recursive Partitioning Analysis (RPA) from the Radiation Therapy Oncology group [14]. In current clinical practice, there are graded prognostic assessments (GPA) for each type of cancer. The most commonly used for BM from breast cancer was published by Sperduto et al. in 2011, and updated by the same group in 2012 [3, 15]. Both of these scoring systems included breast cancer subtype as a prognostic factor for survival. The most recent update for breast cancer specific BM, published by Subbiah et al., included the number of brain metastases in the GPA [4].
The purpose of this study was to determine if breast cancer subtype affects OS, local control, or distant brain control in breast cancer patients treated with Gamma Knife stereotactic radiosurgery (SRS) at our institution. Furthermore, we sought to evaluate the advance of the breast cancer-specific GPA and its effectiveness at predicting outcomes in our patients [3, 4].
Methods
From November 2000 to May 2014, we evaluated all of the patients with brain metastases from breast cancer treated with Gamma Knife stereotactic radiosurgery at Columbia University Medical Center. 72 patients had enough information available to be included. Subtype, age, number of metastases, KPS, and survival data were all required. The following variables were collected from medical records due to their potential prognostic significance: subtype (HER2 type, triple-negative, Luminal A, or Luminal B), age at SRS treatment, age at original breast cancer diagnosis, time between breast diagnosis and first BM treatment, clinical stage at primary diagnosis, Karnofsky Performance Status (KPS), chemotherapy history, number of brain metastases, presence of extracranial metastases, status of primary tumor (controlled or uncontrolled), and treatment modality (SRS only, SRS and surgery, SRS and whole brain radiotherapy [WBRT], or SRS, WBRT, and surgery). Patients received 20 Gy if tumor was 2 cm or less, 18 Gy if 2–3 cm, and 16 Gy 3–4 cm [16]. Local and distant brain failures were assessed by reviewing follow up brain imaging. For those patients where follow up imaging was not available, information on local and distant failures was taken from radiology reports. For patients where follow up brain imaging was available, response was classified according to the Response Evaluation Criteria in Solid Tumors (RECIST) [17]. In-field local tumor failure was defined as an increase of >20 % in tumor volume. Distant brain failure was defined as any new lesion appearing on follow up MRI that had not been previously diagnosed or seen on SRS planning MRIs. For response to treatment, complete response for a lesion was defined as no residual tumor appearing on follow up MRIs, partial response was a decrease in tumor size >30 %, progression was an increase in tumor volume >20 %, and stable was all other tumors [18]. We calculated two Graded Prognostic Assessment scores (0–4) for each patient by totaling the scores for the individual prognostic indicators. The first based on Sperduto et al. included KPS (≤50—0 points, 60—0.5 points, 70–80—1 point, or 90–100—1.5 points), subtype (triple-negative—0 points, Luminal A—1 point, HER2—1.5 points, or Luminal B—2 points), and age (≥60—0 points or <60—0.5 points) [3]. The second based on Subbiah et al. included KPS (≤50—0 points, 60—0.5 points, 70–80—1 point, or 90–100—1.5 points), subtype (triple-negative—0 points, Luminal A—0.5 points, Luminal B—1 point, and HER2—1.5 points), age (>50—0 points or ≤50—0.5 points), and number of brain metastases (1–3—0.5 points, or >3—0 points) [4]. Patients were also stratified into 3 groups based on subtype alone: triple-negative, HER2 type, and Luminal types (combining Luminal A and Luminal B). Overall survival (OS) was calculated from the first treatment for BM. Patients were excluded if there was incomplete information on dates of treatments, death, follow up, or subtyping. The study was approved by the institutional review board of Columbia University Medical Center.
Statistical analysis
For baseline characteristics, summary statistics were calculated using frequencies and proportions for categorical data. A Chi square test was used to determine significance between baseline characteristics. Column proportions were compared and the p-values were adjusted at the 0.05 level using the Bonferonni method. Survival curves were calculated using the Kaplan–Meier method. Hazard ratios (HR) and 95 % confidence intervals were determined using the Cox proportional hazards model and log-rank tests were used to assess significant differences between groups. Patients lost to follow-up were censored for survival at the time of last visit. To identify baseline variables associated with OS time, multivariable analysis was performed with the Cox proportional hazards model, including those variables on univariate analysis with a p value ≤0.1. All statistical analysis was performed using IBM SPSS version 23.
Results
Patient attributes
72 patients were included in this study for analysis. The median age was 54 years with a range of 30–83. Median follow up time was 12 months for overall survival. 48 patients with 150 individual lesions were included in the control analysis, with a median follow-up time of 6 months. On baseline characteristics stratified by subtype, KPS and treatment modality had significant differences. Luminal patients were more likely to have a higher KPS [n = 47 (98 %)] when compared with HER2 type and triple negative patients [n = 8 (67 %) and n = 11 (92 %) respectively]. 27 patients (37 %) received only SRS, 15 (21 %) received SRS and surgery, and 30 (42 %) received either SRS and WBRT or all 3 treatment modalities. Luminal patients were most likely to get SRS alone [n = 21 (44 %)] when compared with HER2 and triple-negative patients [n = 2 (17 %) and n = 4 (33 %) respectively]. Luminal patients were also more likely to get SRS and surgery alone [n = 13 (27 %)] when compared with HER2 and triple-negative patients [n = 1 (8.3 %) for both]. HER2 and triple-negative patients were most likely to get some combination of treatments including WBRT [n = 9 (75 %) and n = 7 (58 %)] when compared with luminal patients [n = 14 (29 %)] (Table 1). Histology from initial breast surgery was available for 58 patients. 46 (79 %) patients had invasive ductal carcinoma, with 3 (5.2 %), 7 (12 %), and 2 (3.4 %) having lobular ductal carcinoma, mixed IDC/LDC, and other or unidentifiable respectively. GPA scores of 0.0–2.0, 2.5–3.0, or 3.5–4.0 were calculated for all 72 patients based upon both Sperduto et al. and Subbiah et al. [3, 4].
Control
48 patients with 150 individual lesions had follow up brain imaging or radiology reports available for determination of local and distant brain failures. 35 (73 %) patients were luminal subtype, 6 (13 %) were HER2, and 7 (15 %) were triple negative. Of the 150 lesions, 121 (81 %) were luminal, 12 (8.0 %) were HER2, and 17 (11 %) were triple negative. There was a significant difference in response to treatment by lesion based on subtype (p = 0.01). There were no significant differences in local failure by patient, local failure by lesion, or distant failure by patient between the different subtypes (p = 0.96; p = 0.69; p = 0.64 respectively). Luminal subtype lesions were more likely to have a complete response [n = 58 (48 %)] when compared with HER2 and triple negative lesions [n = 0 (0.0 %) and n = 6 (35 %)] (Table 2).
Survival
On univariate analysis, having more than 3 BM was a significant predictor of lower OS (HR 1.985; 95 % CI 1.008–3.907; p = 0.05). Triple negative subtype also showed a trend towards worse OS (HR 1.992; 95 % CI 0.911–4.354; p = 0.08). Age at initial breast cancer diagnosis, age at SRS treatment, time between breast cancer diagnosis and BM, KPS, type of BM, chemotherapy, extracranial metastases, primary control, and treatment modality were not significant predictors of OS (Table 3). Based on univariate results, number of brain metastases and breast cancer subtype were included in multivariable analysis. On multivariable analysis, having more than 3 BM was still a significant predictor of decreased OS (HR 2.668; 95 % CI 1.276–5.578; p = 0.01). Triple-negative and HER2 subtypes became significant predictors of decreased OS (HR 2.355; 95 % CI 1.040–5.332; p = 0.04 and HR 2.638; 95 % CI 1.154–6.034; p = 0.02) (Table 4).
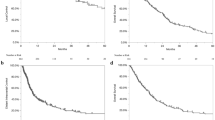
On Kaplan–Meier analysis for OS from first BM treatment, neither subtype nor either GPA showed a significant difference between groups. Median OS for the entire cohort was 25 months. Median OS for luminal, HER2, and triple-negative subtypes was 26, 20, and 22 months respectively (p = 0.11). For the Sperduto et al. GPA, median OS was 25, 22, and 36 for scores of 1.0–2.0, 2.5–3.0, and 3.5–4.0 respectively (p = 0.09) [3]. For the Subbiah et al. GPA, median OS for scores of 0.5–2.0, 2.5–3.0, and 3.5–4.0 was 25, 20, and 25 (p = 0.06) (Online Resource 1) (Fig. 1) [4].

Kaplan-Meier method for determining OS: a survival outcomes stratified by subtype (p = .11); b survival outcomes stratified by GPA (Sperduto et al.; p = .09); c survival outcomes stratified by GPA (Subbiah et al.; p = .06)
In addition to OS from first BM treatment, Kaplan–Meier analysis was performed to determine time from initial breast diagnosis to first treatment for BM, and to analyze overall survival from initial breast cancer diagnosis stratified by subtype. Median time from initial breast cancer diagnosis to first BM treatment was 6, 2, and 3 years, for luminal, HER2, and triple negative patients respectively (p = 0.06) (Table 5) (Online Resource 2) (Online Resource 3). There was a significant difference between subtypes with median overall survivals of 53, 90, and 159 months for HER2, triple-negative, and luminal subtypes respectively (p = 0.00) (Online Resource 4).
Discussion
BM are the most common malignant type of intracranial tumors in adults, with breast cancer being the second leading cause behind only NSCLC [2, 5, 19, 20]. Breast cancer subtype is a powerful predictor of prognosis in the localized setting and was incorporated into the diagnosis-specific GPA for breast cancer in 2011 [10, 15, 21, 22]. We sought to investigate whether these subtypes were predictive of OS, local and distant brain failures, and to assess the updates to the breast cancer-specific GPA by analyzing patients treated with SRS at our institution.
On baseline characteristics, we found significant differences between KPS and treatment modalities between the subtypes (p = 0.00 and p = 0.03 respectively). The HER2 and triple negative patients were more likely to present with a KPS < 70 than luminal patients, and were also more likely to receive WBRT as part of their treatment modality. These results are not entirely surprising, as common clinical practice indicates that BM patients with poor KPS are more likely to receive WBRT.
When analyzing local and distant control, we found a significant difference in the response to treatment on a per lesion basis when stratified by subtype (p = 0.01). Almost half of the luminal lesions (48 %) showed a complete response at an average follow up time of 6 months, compared with none of the HER2 lesions (0.0 %) and fewer of the triple-negative lesions (35 %). When looking at the lesions that progressed, the luminal (23 %), HER2 (18 %), and triple-negative (24 %) subtypes have similar results. This can partially be explained by the longer median OS time for luminal patients. It is possible that the longer median OS allows for longer follow up, and therefore an increased likelihood of lesion progression. We found no difference in local or distant control on a per patient basis.
On univariate analysis we found that having greater than 3 BM was significant for decreased OS (p = 0.05). In addition, triple-negative and HER2 patients had a trend towards worse OS (p = 0.08 and p = 0.12 respectively). On multivariable analysis, greater than 3 BM, triple-negative, and HER2 types were all significant for decreased OS (p = 0.01; p = 0.04; p = 0.02). This decrease in OS of triple-negative patients concurs with the previous GPA studies in the literature [3, 4, 15]. On Kaplan–Meier analysis, the difference in OS between the subtypes did not reach significance (p = 0.12), but showed a trend for worse survival in the HER2 type and triple negative patients when compared with the luminal patients. As has been shown in the literature, adding other prognostic factors to subtype, such as in the GPA, can improve predictive value [3].
When compared to the Sperduto et al. GPA, median OS in our patients was longer, but the overall predictive value in stratification of patients via this method was confirmed. Sperduto et al. reported median OS of 3.4, 7.7, 15.1, and 25.3 months for GPA scores of 0.0–1.0, 1.5–2.0, 2.5–3.0, and 3.5–4.0 respectively. The median OS for the entire cohort was 13.8 months (95 % CI 11.53–15.87). In our cohort, median OS was 25.1, 21.7, and 36.3 months for GPA values of 1.0–2.0, 2.5–3.0, and 3.5–4.0 respectively (p = 0.09; no patients in our study had GPA values of 0.0 or 0.5). Upon univariate cox regression, these findings were confirmed. GPA scores of 1.0–2.0 and 2.5–3.0 were both found to have decreased OS (HR 2.047; 95 % CI 1.099–5.271; p = 0.03 and HR 2.181; 95 % CI 0.960–4.956; p = 0.06 respectively) when compared with the 3.4–4.0 reference group. The differences in median OS is most likely exaggerated by the difference in patient selection. Firstly, this study includes only patients who had SRS as part of their treatment modalities, while Sperduto et al. included all treatment modalities. Secondly, Sperduto et al. used a large database with patients dating from 1985 to 2007. The changes in treatment of BM between 1985 and the start of this study are numerous, and could result in a substantial effect on the median OS times [3]. Additionally, the systemic therapy options available to these patients have drastically changed and improvement in extracranial metastases control may have contributed to increase OS.
Subbiah et al. sought to improve the existing breast cancer specific GPA by adding an additional factor: number of BM. This was appropriate for our study as an increased number of BM was shown to have decreased OS on both univariate and multivariable analysis. This modified GPA trended towards being a better stratification method for predicting patient outcomes in our cohort. While not statistically significant from the Sperduto et al. GPA, the addition of number of BM did improve the prognostic stratification of our patients. The lack of significance is possibly attributable to the difference in patient selection in this study. Subbiah et al. reported median OS of 3.1, 6.3, 15.5, and 26 months for GPA scores of 0.0–1.0, 1.5–2.0, 2.5–3.0, and 3.5–4.0 respectively. The median OS (months) for the entire patient population was 9.4 months. When stratifying patients by this method, we found median OS to be 25.1, 20.0, and 25.1 months for GPA scores of 0.5–2.0, 2.5–3.0, and 3.5–4.0 respectively (p = 0.06; no patients in our study had a GPA value of 0.0). This was confirmed via univariate cox regression with scores of 0.5–2.0 and 2.5–3.0 showing decreased OS (HR 2.342; 95 % CI 1.037–5.288; p = 0.04 and HR 2.160; 95 % CI 0.945–4.939; p = 0.07 respectively) when compared with the 3.5–4.0 reference group. The differences in OS and stratification can again be partially explained by differences in patient selection. Like Sperduto et al., Subbiah et al. includes patients who received any treatment modality, not just those receiving SRS. Improvement in overall quality of care over time is also a factor, but less so than in the Sperduto et al. comparison as Subbiah et al. included patients dating from 1996 to 2013 [4].
Kaplan–Meier analysis was also performed to determine if there was a difference in the time from initial breast cancer diagnosis to the first treatment for BM. The median overall times were 6, 2, and 3 years, for luminal, HER2 and triple negative cancers (p = 0.06). Previous studies have indicated that HER2 positive and triple-negative cancers may have an increased risk of brain metastases [5–13]. The time it takes for these metastases to occur has not been well studied. These results indicate that subtype is a potential factor not only in predicting risk for likelihood of BM, but in rate of occurrence after initial diagnosis as well. The Kaplan–Meier regressions analyzing OS by subtype from initial diagnosis showed median OS of 53, 90, and 159 months for HER2, triple-negative, and luminal subtypes respectively (Online Resource 4). This is consistent with the results analyzing OS from first CNS treatment, with luminal patients having longer OS and HER2 and triple negative patients having a worse prognosis.
This study has several limitations. Notably, it is retrospective and therefore lends itself to unforeseen variables and the chance of selection bias. Another is that while many patients underwent surgical resection of their BM, many others did not. For those that underwent resection and pathology was available, we were able to confirm the subtype. For those that did not undergo resection there is the potential for differing subtypes between primary tumor and BM. Loss to follow up decreased the number of patients available for control data. This cohort of patients represents the entirety of the breast cancer BM treated with SRS at our institution, and provided sufficient power to perform analysis. It should be noted that this study only includes patients that received SRS, whereas Sperduto et al. and Subbiah et al. included all treatment modalities [3, 4]. We believe that future studies on breast cancer BM should continue to look at the effect of subtype on both OS and control outcomes, and study the usefulness of including number of brain metastases as a prognostic indicator in the breast cancer specific GPA. Finally, we believe the analysis of subtype effect on time from initial diagnosis to BM could be an important clinical factor, and this should be examined in further detail.
Conclusion
For patients with BM from breast cancer treated with SRS at our institution, HER2 and triple-negative patients trended towards decreased OS. There was a significant difference in lesion response based on subtype. Both the Sperduto et al. GPA and modified GPA from Subbiah et al. proved to be useful in prognostic stratifications for our patients. The addition of number of brain metastases to the GPA was useful and should continue to be investigated. Finally, HER2 and triple-negative patients trended towards a faster rate of metastasis to the brain when compared with luminal type patients, but there was insufficient power to reach statistical significance. This is an area that should be examined in future studies.
References
Howlander N, Noone AM, Krpacho M et al (2015) SEER cancer statistics review. SEER web site
Eichler AF, Kuter I, Ryan P et al (2008) Survival in patients with brain metastases from breast cancer. Cancer 112(11):2359–2376
Sperduto PW, Kased N, Roberge D et al (2012) Summary report on the graded prognostic assessment: an accurate and facile diagnosis-specific tool to estimate survival for patients with brain metastases. J Clin Oncol 30(4):419–425
Subbiah IM, Lei X, Weinberg JS et al (2015) Validation and development of a modified breast graded prognostic assessment as a tool for survival in patients with breast cancer and brain metastases. J Clin Oncol 33(20):2239–2245
Hofer S, Pestalozzi BC (2013) Treatment of breast cancer brain metastases. Eur J Pharmacol 717(1–3):84–87
Freedman RA, Anders CK (2012) Treatment of Breast Cancer in Brain Metastases. Curr Breast Cancer Rep 4(1):1–9
Tsukada Y, Fouad A, Pickren JW (1983) Central nervous system metastasis from breast carcinoma. Autopsy study. Cancer 52:1249–1254
Gori S, Rimondini S, De Angelis V (2007) Central nevous system metastases in HER-2 postive metastatic breast cancer patients treated with trastuzumab: incidence, survival, and risk factors. Oncologist 12:766–773
Tomasello G, Bedard P, De Azambuja E (2010) Brain metastases in HER2-positive breast cancer: the evolving role of lapatinib. Crit REv Oncol/Hematol 75:110–121
Kennecke H, Yerushalmi R, Woods R et al (2010) Metastatic behavior of breast cancer subtypes. J Clin Oncol 28(20):3271–3277
Clayton AJ, Danson S, Jolly S et al (2004) Incidence of cerebral metastases in patients treated with trastuzumab for metastatic breast cancer. Br J Cancer 91:639–643
Niwinska A, Murawksa M, Pogoda K (2010) Breast cancer brain metastases: differences in survial depending of biological subtype, RPA RTOG prognostic class and systemic treatment after whole-brain radiotherapy (WBRT). Ann Oncol 21(5):942–948
Nam BH, Kim SY, Han HS et al (2008) Breast cancer subtypes and survival in patients with brain metastases. Breast Cancer Res 10(1):R20
Gaspar LE, Scott C, Rotman M et al (1997) Recursive partitioning analysis (RPA) of prognostic factors in three Radiation Therapy Group (RTOG) brain metastases trials. Int J Radiat Oncol Biol Phys 37:745–751
Sperduto PWKN, Roberge D et al (2011) The effect of tumor subtype on survival and the Graded Prognostic Assessment (GPA) for patients with breast cancer and brain metastases. Int J Radiat Oncol Biol Phys 82:2111
Shaw E, Charles Scott, Souhami L et al (1999) single dose radiosurgical treatment of recurrent previously irradiated primary brain tumors and brain metastases: final report of RTOG protocol 90-05. Int J Radiat Oncol Biol Phys 47(2):291–298
Therasse P, Arbuck SG, Eisenhauer EA et al (2000) New guidelines to evaluate the response to treatment in solid tumors. J Nat Cancer Inst 92(3):205–216
Jani A, Rozenblat T, Yaeh A et al (2015) the energy index does not affect local control of brain metastases treated by gamma knife stereotactic radiosurgery. Neurosurgery 77(1):119–125
Nayak L, Lee EQ, Wen PY (2012) Epidemiology of brain metastases. Curr Oncol Rep 14(1):48–54
Wang TJC, Saad S, Qureshi YH et al (2015) Does lung cancer mutation status and targeted therapy predict outcomes and local control in the setting of brain metastases treated with radiation? Nero-Oncology 17(7):1022–1028
Nguyen PL, Taghian AG, Katz MS et al (2008) Breast cancer subtype approximated by estrogen receptor, progesterone receptor, and HER-2 is associated with local and distant recurrence after breast-conserving therapy. J Clin Oncol 26(14):2373–2378
Parker JS, Mullins M, Cheang MCU et al (2009) Supervised risk predictor of breast cancer based on intrinsic subtypes. J Clin Oncol 27(8):1160–1167
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Grubb, C.S., Jani, A., Wu, CC. et al. Breast cancer subtype as a predictor for outcomes and control in the setting of brain metastases treated with stereotactic radiosurgery. J Neurooncol 127, 103–110 (2016). https://doi.org/10.1007/s11060-015-2014-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11060-015-2014-8