
Abstract
The application of olive oil is one of the traditional practices used in umbilical cord care in Turkey. The study was conducted experimentally, so as to compare microbiologically the efficacy of olive oil use and keeping the stump dry. Data were obtained using a personal information form and an omphalitis follow-up form, as well as from cultures taken from the infants’ umbilical cords. Cultures were taken from the neonates’ umbilical cords at three different times. The Pearson chi-square test, student t test, percentages, and averages were used for statistical data analysis. The average time for separation is 9.46 days. For the control group, this period is 9.8 days, while for the study group, it is 9.1, lacking a statistically significant difference between the two groups (P > 0.05). However, when the cut-off point for umbilical cord detachment is set at 10 days, the cords of 71.6% of the neonates in the study group, compared with 55.6% of the control group, are observed to have separated before 10 days, representing a significant difference between the groups (P < 0.05). In all of the cultures collected, growth was noted in 35.9% of the study group and 33.3% of the control group. The correlation between the method used for the care of the cord and the total culture results was not statistically significant (P > 0.05). Olive oil can be used in the umbilical cord care of neonates under appropriate conditions; we recommended that this investigation be repeated on expanded sample groups.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Every year, on average, 4 million neonatal deaths occur worldwide. More than 99% of these mortalities take place in developing countries, with almost half of infants dying from infection. Umbilical cord infections are among the leading causes of neonatal mortality. The World Health Organization (WHO) reports that 460,000 neonatal deaths associated with umbilical cord infections occur annually in developing countries [1–5]. Umbilical cord infections, which rank high among the leading causes of neonatal death, especially in developing countries, were also a primary cause of neonatal fatalities in developed countries in the 1940s [6].
Pathogenic micro-organisms, such as staphylococci and coli-form bacilli, as well as gram-negative staphylococci and nonpathogenic micro-organisms, are present on the skin of the newborn following normal vaginal birth [7]. The umbilical cord provides a favorable medium for bacterial colonization because it contains necrotic tissue [8]. The umbilical cord, therefore, carries a potentially high risk of infection development and associated death in neonates [6, 8]. Under normal conditions, before separation, the umbilical cord dries out, turns a brownish color, and usually detaches within the 5–15 days following birth [7]. In cases where an umbilical cord infection develops, however, the periphery of the cord reddens, swells, and when infected by anaerobic microorganisms, a purulent discharge is present. On the other hand, sepsis may develop in the infant even in the absence of these signs and symptoms. Sepsis presents with high fever, lethargy, and malnutrition [7]. Umbilical cord infection is, therefore, very dangerous, and can be fatal, among neonatal infections.
Washing hands, and attention to hygiene, are foremost in preventing umbilical cord infections. Topical antibiotics and antiseptics are used in umbilical cord care. However, it has been reported that topical antiseptics may have toxic and carcinogenic effects [9]. Studies of animals have found that, although triple dye (brilliant green, proflavine hemisulphate, and crystal violet in an aqueous solution), has been determined to be very effective against Staph. aureus, it may have toxic and carcinogenic effects. Keeping the umbilical cord clean and dry is another method of care [6, 8, 10–12] and a variety of traditional practices exist for the care of the umbilical cord in different cultures. These include application of coal, various spices, cow dung, ash, machine oil, turmeric, mustard oil, dried banana, breast milk, and olive oil to the cord [7, 12, 13]. While olive oil and similar substances are not harmful to the baby, and in fact may even be beneficial, the use of substances such as coal, cow dung, and ash carry serious risks of bacterial infection and neonatal tetanus development [7, 12].
The application of olive oil is one of the traditional practices used in umbilical cord care in Turkey. According to the literature, the fruit and fiber of the olive tree are known to have an antimicrobial effect [14]. The linoleic acid present in olive oil is seen to act as an antifungal agent by preventing the oxygenation of fungi [15]. Another characteristic of olive oil is its basal moisturizing action. Olive oil is reported to reduce the skin’s vulnerability to trauma and accelerates the healing process [16]. Studies have shown that pheloic, found in olive oil, promotes endothelium growth, causing local vasodilation and reducing inflammation [10, 15, 17]. A study demonstrated that local administration of olive oil cured approximately two-thirds of fungal infections [18]. Additionally, olive oil has been reported to contain vitamin E, which is a natural antioxidant often used to treat minor skin lesions [19]. The literature also indicates that olive oil is effective in preventing nipple cracks and reducing soreness in the mother, while preventing mouth sores in the infant [15].
Despite traditional practice, however, no studies have examined the use of olive oil in caring for the umbilical cord. Since it is not possible to eradicate traditional practices in any society completely, it is important to ensure correct usage of practices of a benign nature. This study was intended to determine the heretofore unexplored effect of olive oil, which is known to have many benefits for maternal and infant health, in umbilical cord care.
Methods
Study Design
The study was conducted experimentally, so as to compare microbiologically the efficacy of olive oil use and keeping the stump dry. Olive oil was used for the umbilical cord care of the newborns in the study group, whereas in the control group, umbilical cord care consisted solely of keeping the cord clean and dry.
Sample and Data Collection
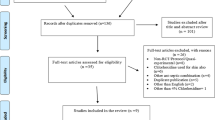
The study was conducted at the postpartum clinic of a university hospital in Ankara, Turkey, and at the mothers’ homes. The sample consisted of 150 women, prescribed by the WHO as 75 in the study group, and 75 in the control group, based on the frequency of omphalitis (0.1%) [1]. However, for various reasons, one loss occurred in the study group, and three in the control group during the first culture; two losses occurred in the study group and eight in the control group during the second culture; and there were 14 losses in the study group and 10 in the control group during the third culture. Mothers aged 20–35 years, with at least an elementary school education, who had not experienced any infection during pregnancy and who had no chronic diseases, and with term babies with no anomalies and a birth weight of over 2,500 g, were included in the sample. The study and control groups were paired to avoid statistical differentials (P > 0.05) in variables that might influence the study outcome (mother’s education, age, number of births, baby’s birth weight) (Table 1).
Measurement
Data were obtained using a personal information form developed by the investigators by reviewing relevant literature to record data related to the mother and the neonate, and an omphalitis follow-up form, as well as from cultures taken from the infants’ umbilical cords.
Implementation of the study began at the maternity clinic of the hospital and continued at the mothers’ homes through to the detachment of the babies’ umbilical cords. Cultures were taken from the neonates’ umbilical cords at three different times. The first culture was taken immediately after birth, before the initial umbilical care took place; the second was at 72 h following birth; and the third was following separation of the cord. The investigators collected the first and second cultures, usually at postpartum clinics. The mothers, who had been taught by the investigators how to obtain a sample, took the third culture at home after the separation of the cord, and informed the investigators. The investigators picked up these cultures from the mothers’ homes. The cultures were cultivated in a laboratory by two researchers who specialized in microbiology.
The investigators provided the olive oil to be used for the umbilical cord care of the neonates in sterilized, photo-protective glass dropper bottles. Olive oil was applied to the umbilical cords of the neonates in the study group twice a day, in doses of five drops each in the morning and evening, totaling 10 drops per day. Administration of olive oil to the study group infants began immediately after birth and continued for 2 days following separation of the umbilical cord. The investigators visited the mothers in their hospital rooms following delivery, and gave them information about umbilical cord care. In addition, the investigators demonstrated to the mothers in the study group how to apply olive oil to their newborns’ umbilical cord. Each mother in the study group was also given an illustrated brochure developed by the investigators, which explained the stages of the olive oil treatment, important points in umbilical cord care, and the warning signs and symptoms of omphalitis, in both writing and pictures. The brochure also included contact information of the investigators to enable the mothers to establish communication when they needed and when the cord was detached. Similarly, the mothers in the control group were also given an illustrated brochure with information on the rules of keeping the cord dry and the warning signs of omphalitis. This brochure also listed the investigators’ contact information.
Permission was obtained from Gazi University’s Medical, Surgical, and Pharmaceutical Practices Local Ethical Council to conduct the study. The investigators explained the study to expectant mothers before childbirth. Mothers who agreed to participate in the study, both orally and in writing, and who fitted the study criteria, were included in the sample. The women were aware of their free choice to leave the study at any stage.
Data Analysis
Data were analyzed in a single-blind. Investigators who cultivated and analyzed the cultures did so without knowledge of the groups to which the samples belonged. The Pearson chi-square test, student t test, percentages, and averages were used for statistical data analysis.
Limitations
Although olive oil is being used in umbilical cord care as a traditional practice, especially in rural areas in Turkey, it has taken a long time to reach the sample group because the study was conducted in an urban area. There have been losses in the sample group and, consequently, some babies have been hospitalized for various reasons and some families have left town. It has taken a long time to reach the sample group because of the many sample selection criteria and cases have been paired into study and control groups one by one.
Results
Of the mothers participating in the study, 62.7% were university graduates, 62.7% were primiparous, and had an average age of 30.09 years. The average birth weight of the neonates was 3,258.19 g, 53.3% of whom were female.
Table 2 shows the interval of umbilical cord separation by method used. The average time for separation is 9.46 days. For the control group, this period is 9.8 days, while for the study group, it is 9.1, lacking a statistically significant difference between the two groups (P > 0.05). However, when the cutoff point for umbilical cord detachment is set at 10 days, the cords of 71.6% of the neonates in the study group, compared with 56.0% of the control group, are observed to have separated before 10 days, representing a significant difference between the groups (P < 0.05).
Although not included in the table, Staph. epidermidis (first culture: 0.7%; second culture: 34.5%; third culture: 27.8%), Staph. aureus (first culture: 1.4%; second culture: 16.2%; third culture: 17.5%), Klebs. pneumoniae (first culture: 0.7%; second culture: 4%; third culture: 4%) and E. coli (first culture: 0.0%; second culture: 4.7%; third culture: 1.3%) were the micro-organisms that proliferated the most in the cultures obtained, while none of the neonates developed omphalitis. In all of the cultures collected from the neonates, growth was noted in 35.9% of the study group and 33.3% of the control group. The correlation between the method used for the care of the cord and the total culture results was not statistically significant (P > 0.05).
Table 3 shows the distribution of the microorganisms with the highest colonization rate, according to the method of umbilical cord care. Staph. epidermidis grew in the cultures taken from 53.3% of the neonates in the study group, and in 44% in the control group. The difference in Staph. epidermidis growth in the neonatal groups was not found to be statistically significant (P > 0.05). Staph. aureus growth occurred in the cultures of 22.7% of the study group and 33.3% of the control group, and the difference lacked statistical significance (P > 0.05). Klebs. pneumoniae was present in 6.7% of the study group and 10.7% of the controls, and the difference between the groups lacked statistical significance (P > 0.05). Finally, E. coli growth occurred in the cultures of 8.2% of the study group and 4% of the control group neonates, with no statistical significance in the difference between the groups (P > 0.05).
Discussion
Use of olive oil is one of the traditional methods of umbilical cord care in Turkey. Although some traditional approaches are harmful to human health, others have benefits. Our study has determined that the average time of umbilical cord detachment of the neonates according to the method used was very close (S: 9.1 days, C: 9.8 days). A meaningful differential between the groups in terms of cord detachment time averages was lacking (P > 0.05). However, with a 10 day cutoff point for umbilical cord detachment, it was found that the umbilical cords of three-quarters of the neonates in the study group, compared with slightly more than half of those in the control group, had detached in less than 10 days. The difference between the groups in terms of cord detachment before and after 10 days was statistically significant, with the cords of the neonates in the study group separating before 10 days (P < 0.05). Results obtained from studies investigating the time of cord separation according to the method of care vary. Mullany et al. determined the mean separation time was shorter in dry cord care (4.24 days) and soap/water (4.25 days) clusters than in chlorhexidine clusters (5.32 days). Dore et al., meanwhile, determined the mean separation time in alcohol group to be 9.8 days and in natural drying group 8.16 days, and in the study by Vural and Kisa, cord separation occurred at a mean of 9.9 days in the povidone-iodine group, and in the dry care and topical human milk groups, cord separation occurred at a mean of 7.7 and 7 days respectively. Ekici et al. determined the mean separation time in alcohol group as 8.1 ± 2.3 days, in povidone-iodine and alcohol group as 8.7 ± 2.8 days and in natural drying group as 6.1 ± 2.1 days [3, 5, 12, 20]. According to the WHO, the longer the umbilical cord retention, the higher the risk of omphalitis development [1]. Detachment of the umbilical cords of the neonates in our study group before the 10 day period suggests that use of olive oil in cord care may reduce the risk of omphalitis.
The neonate lacks normal protective flora at birth, which begins to form within 24 h following birth. Normal skin flora of a neonate develops with the micro-organisms transferred from the mother’s vagina, skin, and hands [1]. The micro-organisms that most frequently pass through this route are Staph. epidermidis and Staph. aureus. In our study, the micro-organisms that grew in largest quantities in the cultures from the umbilical cords of neonates were, respectively, Staph. epidermidis, Staph. aureus, and E. coli, with none of the babies developing omphalitis. According to the literature, multiple micro-organisms feature in the development of omphalitis. These are, usually, Staph. aureus, Group-A streptococci, E. coli, Klebs. pneumoniae, and Proteus mirabilis [21]. Performing the birth outside of the hospital in unfavorable conditions, and not observing hygienic rules in umbilical care and using some traditional practices in umbilical care, increase the risk of neonatal infection. In developing countries especially, many traditional practices, such as animal manure, turmeric, mustard oil, dried herbs and coal dust, have been used in the umbilical care and, as a result, neonatal deaths have been increasing due to ompholithis [13, 22]. In recent years, births have been performed mostly in hospitals as hygienic conditions in Turkey have improved and neonatal mortality has decreased significantly [23]. Besides this, some traditional practices continue to be performed in Turkey. Olive oil is one of these traditional practices applied in the umbilical cord care of newborn. In laboratory studies, it was determined that the olive oil has antimicrobial effects. Medina et al. determined that the content of dialdehydic due decarboxymethyl oleuropein of extra virgin olive oil has a strong and broad spectrum of anti-microbial effects and Tripoli et al. stated that olive oil can be used in the treatment of some infectious diseases because of its antimicrobial effects [24, 25]. Kiechl-Kohlendorfer et al. [26] applied water-based skin creams and olive oil with softening creams in the umbilical cord of premature newborns, and found that dermatitis was seen less in newborn infants when olive oil was used in the umbilical cord care.
The findings of our study can be said to be in keeping with the literature. Based on the conclusion of our study that S. epidermidis, S. aureus, K. pneumoniae, and E. coli were the micro-organisms with the highest rates of proliferation, and that no significant statistical difference existed between the groups in terms of micro-organism growth, it is believed that the use of olive oil in the care of the umbilical cords of neonates, which is a traditional practice in the country, carries no health risk.
Umbilical cord separation time of the neonates in the study group was determined as 9.8 days, compared with 9.1 days for the control group, and no meaningful difference was observed in the cord separation time averages of the two groups. A statistically significant correlation was also lacking between the method used and the overall culture results. The micro-organisms that reproduced the most in the cultures collected were Staph. epidermidis, Staph. aureus, Klebs. pneumoniae, and E. Coli, and omphalitis did not develop in any of the neonates. The difference between the study and control groups, in terms of proliferating micro-organisms, was not statistically meaningful.
Our study concludes that olive oil can be used in the umbilical cord care of neonates under appropriate conditions, and recommends that the investigation be repeated on expanded sample groups.
References
World Health Organization (1998). Care of the umbilical cord: A review of the evidence. Geneva.
Darmstadt, G. L., & Dinulos, J. G. (2000). Newborn skin care. Pediatric Clinics of North America, 47(4), 757–782.
Dore, S., Buchan, D., Couls, S., Hamber, L., Stewart, M., Cowan, D., et al. (1998). Alcohol versus natural drying for newborn cord care. Journal of Obstetric, Gynecologic, and Neonatal Nursing, 27(6), 621–627.
Gladstone, I. M., Clapper, L., Thorp, J. W., & Wright, D. I. (1988). Randomized study of six umbilical cord care regimens. Comparing length of attachment, microbial control, and satisfaction. Clinical Pediatrics, 27(3), 127–129.
Mullany, L. C., Darmstadt, G. L., Khatry, S. K., LeClerg, S. C., Katz, J., & Tielsch, J. M. (2006). Impact of umbilical cord cleansing with 4.0% chlorhexidine on time to cord separation among newborns in southern Nepal: A cluster-randomized, community- based trial. Pediatrics, 118(5), 1864–1871.
Pezzati, M., Biagioli, E. C., Martelli, E., Gambi, B., Biagiotti, R., & Rubaltelli, F. F. (2002). Umbilical cord care: The effect of eight different cord-care regimens on cord separation time and other outcomes. Biology of the Neonate, 81(1), 38–44.
Zupan, J., Garner, P., & Omari, A.A. (2004). Topical umbilical cord care at birth. Cochrane Database of Systematic Reviews, Issue 3. Art. No.: CD001057. DOI: 10.1002/14651858.CD001057.pub2.
Kul, M., Gürsel, O., Gülgün, M., Kesik, V., Sarıcı, S. Ü., & Alpay, F. (2005). Sağlıklı term yenidoğanlarda farklı göbek bakımı uygulamalarının göbek düşme zamanı ve diğer klinik sonuçlar üzerine etkilerinin değerlendirilmesi. Türk Pediatri Arşivi, 40(3), 227–231.
Siegfried, E., & Shah, P. (1999). Skin care practices in the neonatal nursery: a clinical survey. Journal of Perinatology, 19(1), 31–39.
Janssen, P., Selwood, B. L., Dobson, S. R., Peacock, D., & Thiessen, P. N. (2003). To dye or not to dye: A randomized, clinical trial of a triple dye/alcohol regime versus dry cord care. Pediatrics, 111(1), 15–20.
Panyavudhikrai, S., Danchaivijitr, S., Vantanasiri, C., Trakulsomboon, S., Kolatat, T., Dhiraputra, C., et al. (2002). Antiseptics for preventing omphalitis. Journal of the Medical Association of Thailand, 85(2), 229–234.
Vural, G., & Kisa, S. (2006). Umbilical cord care: a pilot study comparing topical human milk, povidone-iodine, and dry care. Journal of Obstetric, Gynecologic, and Neonatal Nursing, 35(1), 123–128.
Mullany, L. C., Faillace, S., Tielsch, J. M., Stoltzfus, R. J., Nygaard, K. E., Kavle, J. A., et al. (2009). Incidence and risk factors for newborn umbilical cord infections on Pemba Island, Zanzibar, Tanzania. The Pediatric Infectious Disease Journal, 28(6), 503–509.
Kubo, A., Lunde, C. S., & Kubo, I. (1995). Antimicrobial activity of the olive oil flavor compounds. Journal of Agricultural and Food Chemistry, 43(6), 1629–1633.
Hafner-Eaton, C. (1997). Breast yeast. Midwifery Today and Childbirth Education, 42(3), 37.
Krampf, L. (1996). Baby your baby’s skin. Delicious! Your Magazine of Natural Living, 12(9), 66–68.
Brent, N., Rudy, S. J., Redd, B., Rudy, T. E., & Roth, L. A. (1998). Sore nipples in breastfeeding women: A clinical trial of wound dressings vs. conventional care. Archives of Pediatric Adolescent Medicine, 152(11), 1077–1082.
Al-Waili, N. S., Saloom, K. S., Al-Waili, T. N., & Al-Waili, A. N. (2006). The safety and efficacy of a mixture of honey, olive oil, and beeswax for the management of hemorrhoids and anal fissure: a pilot study. The Scientific World Journal, 2(6), 1998–2005.
Stoukides, C. (1993). The galactopharmacopedia: Topical medications and breastfeeding. Journal of Human Lactation, 9(3), 185–187.
Ekici, B., Ergin, A. B., & Şahiner, P. (2007). Yenidoğanların göbek bakiminda kullanilan yöntemlerin etkinliğinin karşilaştırılması. Çalışma Çocuk Dergisi, 7(3), 191–196.
Brook, I. (1998). Microbiology of necrotizing fasciitis associated with ompholitis in the newborn infant. Journal of Perinatology, 18(1), 28–30.
Mullany, L. C., Darmstadt, G. L., Katz, J., Khatry, S. K., LeClerq, S. C., Adhikari, R. K., et al. (2009). Risk of mortality subsequent to umbilical cord infection among newborns of southern nepal: Cord infection and mortality. The Pediatric Infectious Disease Journal, 28(1), 17–20.
Hacettepe University Institute of Population Studies. (2003). Turkey demographic and health survey 2003. Turkey: Ankara.
Medina, E., de Castro, A., Romero, C., & Brenes, M. (2006). Comparison of the concentrations of phenolic compounds in olive oils and other plant oils: Correlation with antimicrobial activity. Journal of Agricultural and Food Chemistry, 54, 4954–4961.
Tripoli, E., Giammanco, M., Tabacchi, G., Di Majo, D., Giammanco, S., & La Guardia, M. (2005). The phenolic compounds of olive oil: Structure, biological activity and beneficial effects on human health. Nutrition Research Reviews, 18, 98–112.
Kiechl-Kohlendorfer, U., Berger, C., & Inzinger, R. (2008). The effect of daily treatment with an olive oil/lanolin emollient on skin integrity in preterm infants: A randomized controlled trial. Pediatric Dermatology, 25(2), 174–178.
Acknowledgments
The study has supported by The Unit of Academic Studies Projects of Gazi University.
Conflict of interest statement
This study has supported as financial by The Unit of Academic Studies Projects of Gazi University. By this financial support; materials of culture and umblical cord care have brought and investigators cost of transports have been met.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Şentürk Erenel, A., Vural, G., Yaman Efe, Ş. et al. Comparison of Olive Oil and Dry-Clean Keeping Methods in Umbilical Cord Care as Microbiological. Matern Child Health J 14, 999–1004 (2010). https://doi.org/10.1007/s10995-009-0536-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10995-009-0536-4