
Objectives: Longitudinal studies of maternal depression in the postpartum period have demonstrated that a chronic state of depressive symptoms is not rare. In spite of this, however, the characteristics of chronically depressed mothers have rarely been studied. This study examines the demographic and socioenvironmental characteristics across time of childrearing women with chronic depressive symptoms. Methods: A cohort of 476 childrearing lower-income mothers was interviewed from the first trimester of pregnancy through the tenth year postpartum. The Center for Epidemiologic Studies-Depression Scale (CES-D; Radloff, L. (1977) Appl Psychol Meas 1:385–401) was used to define depressive symptomatology. Four groups were defined based on the CES-D scores at 18 months, 3, 6 and 10 years: never-depressed (CES-D < 16), depressed only at one phase (CES-D ≥ 16), chronically mildly depressed (CES-D > 16 and ≤24 at three or more phases), and chronically severely depressed (CES-D ≥ 25 at three or more times). Demographic and socioenvironmental characteristics of the groups were evaluated across time. Results: Chronically depressed women compared to never-depressed women were less likely to be married, had less education, had lower family income, and were more likely to use substances. They reported more frequent arguments with close family members or friends, separation/divorce with partners, financial problems, less social support, and more financial strain. Conclusions: Women who continue to be depressed across the 10 postpartum years have less optimal outcomes compared to women who are not depressed and those who are only intermittently depressed. Pregnancy and delivery and subsequent pediatric visits are important times to identify women who are depressed.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
INTRODUCTION
During the childbearing years, depression can have an important effect on the well-being of both the mother and her offspring. Depressed mothers express more negative and hostile feelings toward their children than do non-depressed mothers, and family and marital problems can result from the effects of the negative feelings and low energy of the depressed mothers (1).
Depression in the childrearing years is common, and is often chronic or recurrent. A study of mothers from the seventh prenatal month to 82 months postpartum found that 70% were depressed at one or more of the six assessments, and most of the mothers who were depressed at 82 months had also been depressed at previous phases (2). Women with depression often have either a pattern of recurrence or they develop a chronic depressive state (3–9). Indeed, about half of the women who had a depressive episode after delivery had depressive episodes before delivery as well (10).
Chronic depression in mothers has a negative effect on the offspring. Chronically depressed mothers interact with their infants in a less positive way and with less sensitivity, and children of chronically depressed mothers are less securely attached than those whose mothers are not chronically depressed (11–14). In addition, the children of chronically depressed mothers have more behavioral problems (8).
Using a self-report measure of depressive symptoms 5 times over a period of 1–36 months postpartum, the NICHD Early Child Care Research Network noted that chronically depressed mothers differed in educational attainment, income-to-needs ratios, percent living with a partner, and perceived social support. The authors suggested that there was an association between these measures of psychosocial risk and the development of chronic depression (14).
The risk factors for depressive symptoms among childrearing mothers include lower socioeconomic status (2, 15–19), marital difficulties (2, 16, 19, 20), single parenting (21), having young children (22), poor living accommodations (2), stressors (16, 23), low social support (2, 16, 24), negative life events (16, 25, 26), experiences of childhood abuse, and partner abuse (26). However, in many of these studies, a small number of variables were examined and confounding factors such as income and number of children in the household were not controlled in the analyses. In addition, most studies of maternal depression have not considered the relations between substance use and depression, although substance use is known to be related to depression (27).
These findings suggest the importance of identifying the characteristics of depressed mothers. In this analysis, we use data from a longitudinal study of low-income mothers. These mothers have been followed from the first trimester of pregnancy through 10 years postpartum. First, we describe the prevalence and course of depressive symptoms in the childrearing years and examine the differences in maternal characteristics among groups that are defined by the chronicity and severity of depressive symptoms. Next, we will examine the demographic and socioenvironmental characteristics of chronically depressed women at delivery and across the subsequent childrearing years.
METHODS
Study Design
The Maternal Health Practices and Child Development (MHPCD) Project is a longitudinal investigation of the effects of prenatal alcohol and marijuana exposure on the growth, behavior, and cognitive development of the offspring. Women aged 18 years or older, who attended a prenatal clinic located in an obstetrical hospital, were recruited in 1982 and 1983 for the study. They were in their fourth or fifth month of pregnancy. This study was approved by the University of Pittsburgh Institutional Review Board and the Human Experimentation Committee of the Magee-Womens Hospital. Written informed consent was obtained from the participants. Detailed information on this cohort has been published (28).
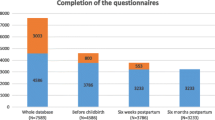
Participants in the study were interviewed 8 times from the fourth month of pregnancy to 10 years postpartum. At delivery, 763 mothers and their live born singleton infants were evaluated. By the 10-year phase, the sample size was reduced to 636 due to child deaths, maternal refusals, and those who were lost to follow-up. Of the remaining sample, 106 of the children were not in the custody of the biological mother for at least one interview; these cases were not included in the analysis. Among the 530 remaining mothers with consistent custody, 476 participated in all of the four interviews at 18 months, 3, 6, and 10 years postpartum. These women constitute the analysis cohort. Race, parity, gravidity, education, marital status, family income, and depression scores at delivery, 18 months, 3, 6, and 10 years were not significantly different between the group of 476 mothers who were interviewed at all phases and the 54 mothers who missed one or more interviews.
Sample Description
At recruitment, the mean age of the 476 women was 23.2 years (SD 4.1) (range: 18–42 years). The mothers were of lower socioeconomic status. Their mean education was 11.8 years (SD 1.3) (range: 8–18 years) and the average family income was $360/month. Thirty-six percent of the women were married, 47% were Caucasian, and 53% were African-American. The average parity was 0.86 (range: 0–9) at the initial interview, and 43.5% were primigravidous.
Measurements
Depressive Symptoms
The Center for Epidemiologic Studies-Depression Scale (CES-D) (29) was used at each phase to assess depressive symptoms. The CES-D is a 20-item questionnaire that was developed for and has been used widely to measure symptoms in the general population and psychiatric populations. The scale does not make a diagnosis of depression, rather, it is a measure of symptoms (30, 31). This scale correlates well with other established measures of depression, the Zung (r = .90) and the Beck (r = .81), establishing its validity (30). A cut-point of 16 has been defined as indicating a clinically significant level of depressive symptoms (32, 33). In the present study, the reliability coefficients (Cronbach's α) for the CES-D scores at 18 months, 3, 6, and 10 years were 0.89, 0.90, 0.89, and 0.91, respectively. We defined a CES-D score of 25 as an indication of a very high level of depressive symptoms. That value was selected because it is one standard deviation above the average score among recovered depression patients reported by Weissman et al. (33). The women were asked about symptoms since the previous interview.
Characteristics of the Environment
At each interview, participants were asked about their family structure, the number of people in the household, whether they lived with a husband, boyfriend, another adult, or no adult, the number of siblings of the index child, and the number of years between children.
Maternal Substance Use
At each study phase, maternal substance use, including tobacco, alcohol, cocaine, and marijuana, and other illicit drug use, was ascertained. Heavy polysubstance use was defined as use of two or more substances at or above the defined levels: two or more drinks per day, or one or more joints of marijuana per day, or any other illicit drug.
Life Events
At delivery, women were asked about life events during pregnancy. At all subsequent interviews, life events were assessed since the time of the previous interview.
Social Support
At delivery, 18 months, 3, 6, and 10-year assessments, the mothers were asked: how often they could turn to relatives (5-point scale from never to all the time); and how satisfied they were with the support from relatives (4-point scale from 1—very unsatisfactory to 4—very satisfactory support). No support was coded as 0. The average of these two questions was used as a measure of support from relatives. Support from friends was defined in the same way. At 18 months, 3, 6, and 10 years, women were asked whether they were satisfied with the support they received in their role as a mother. This was coded on a 5-point scale from never to all the time.
Chronic Stress
During the delivery interview, the mother was asked to report how often she worried about not having enough money for herself and the baby (rated on a 5-point scale from never to all the time). In later study phases, three questions on financial strain were asked on a 5-point scale ranging from never to all of the time, 1) short on money every month, 2) unable to buy essential things for the child, and 3) unable to buy extra things for the child. The mean of the three answers was used to represent financial strain. At delivery, the availability of childcare was ascertained, At all postpartum interviews, the actual amount of childcare help was evaluated on a 5-point scale from never to all the time. The answers were reverse coded and used as the variable named “lack of help with child care.’
Statistical Analysis
Definition of Groups
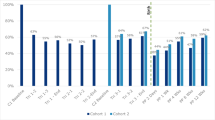
In these analyses, CES-D scores between 0 and 15 were defined as not depressed, scores between 16 and 24 were defined as mildly depressed, and scores above 24 as severely depressed. This allowed us to evaluate whether the correlates of chronic depression differed by the severity of the symptoms. Four groups were defined to examine the chronicity and severity of depressive symptoms: 1) mothers who scored below 16 at all phases were defined as not-depressed (NO); 2) mothers who scored 16 or above only once were defined as once-depressed (ONE); 3) mothers who scored 3 or 4 times between 16 and 24 were defined as chronically mildly depressed (CM). Mothers who scored 25 or more all the time, or who scored from 16 to 24 once and 25 or higher 3 times were defined as chronically severely depressed (CS). There were 80, 73, 98, and 85 women in the NO, ONE, CM, and CS groups, respectively. Of the 476 mothers, 336 belonged to one of these typologies. The remaining 140 women scored 16 or more at least twice, but did not meet the definition of CM or CS.
Group Comparisons
Post hoc group comparisons were done on demographic characteristics, characteristics of the environment, life events, maternal substance use, social support variables, and chronic stressors across and between groups. The Kruskal-Wallis non-parametric test was used for analyses because the variables were not normally distributed. A p-value of less than 0.05 was defined as a significant difference.
Correlates of Chronic Severe Depression
To examine the correlates of chronic depression, stepwise multivariate logistic regression analysis was performed at each phase. In these analyses, the NO group was used as the control group and contrasted to the CS group.
RESULTS
The average CES-D scores of the 476 mothers who completed all four interviews from 18 months to 10 years were 19.01 (SD 8.89) at 18 months postpartum, 18.59 (SD 9.31) at 3 years, 17.49 (SD 9.51) at 6 years, and 18.10 (SD 9.47) at the 10-year interview. At each phase, the sample mean was at or above the clinical threshold. At 18 months, 3, 6, and 10 years, 64.3, 62.4, 56.9, and 60.1% of the women, respectively, scored at or above the cut-point of 16. Only 16.8% of the women scored below 16 at all phases, and an additional 15.3% scored above 16 only once. The remaining 67.9% of the women reported depressive symptoms above the clinical threshold twice or more between 18 months and 10 years postpartum.
Although the depression typologies were defined from postpartum experience, the CM and the CS groups had significantly higher CES-D scores at delivery than the NO or the ONE groups. In the CS group, 71% (n = 56) of the women scored 25 or more on the CES-D at delivery, 11% (n = 9) scored in the non-depressed range at delivery. By contrast, only 5% (n = 4) of the women in the NO group scored 25 or more on the CES-D at delivery, while 67% (n = 51) of them scored 15 or less.
The demographic characteristics of the groups are presented in Table I. Maternal age and race did not differ across the groups. The level of education was significantly lower for the CS group compared to the other groups. The percent of women who were employed increased across time in all of the groups. At 10 years, however, the CS group was significantly lower than the NO and ONE groups. Family income also did not differ across the groups at delivery. At all subsequent phases, however, the average incomes of the women in both the CS and CM groups were significantly lower than the NO and ONE groups.
There were significant group differences at each phase in the proportion of women who were married. The CS group consistently had the lowest proportion of women and the NO group consistently had the highest proportion of married women. Over time, while the percent of women in the other three groups who were married increased, the proportion married in the CS group remained low. Women in the CS group had the highest average daily cigarette use. There were no differences in alcohol or marijuana use (data not presented). There were significant differences in the rate of other illicit drug use, the use of illicit drugs other than marijuana. The rate of use was higher among the CS group.
The average number of the life events, separation/divorce, financial problems, and serious arguments did not differ across groups at delivery, but in the postpartum, the rates were consistently higher in the CS group in contrast to the other groups (Table II). The CS group was notable in that, at 10 years postpartum, 37% had experienced a major financial problem compared to 11.5% among the NO group. The average number of arguments, as well, was significantly different across groups, with those in the CS group demonstrating the largest number. There were no significant differences among groups on bereavement, having a baby, or current pregnancy at any assessment phase (data not presented).
Social support was measured as support from relatives and friends and support for the woman's role as a mother. Perceptions of support as a mother were consistently and significantly lower in the CS women in contrast to the other three groups (Table III). The women in the CS group also reported significantly less general support from their relatives compared to the other groups. Women in the CM category also were more likely to report less support as a mother and less satisfactory support from their relatives, particularly at 10 years postpartum.
Chronic stress was defined as financial strain and less help with childcare. The women in the CS group reported the highest level of financial strain at all phases (Table III). In addition, the women in the CM group were also significantly higher than the NO and ONE groups in the frequency of this stressor. The CS and CM mothers also reported more problems obtaining help with childcare than the mothers in the other groups.
A logistic regression analysis was used to evaluate the independent effects of the variables that were significant in the above analyses. Only women in the NO and the CS group were included (Table IV). The results were quite consistent across time. Financial strain (more), marital status (not married), social support (less), and the life event, serious arguments (more) significantly predicted membership in the CS group. Use of multiple substances at delivery, childcare problems at 18 months, tobacco use at 3 years, and work status (unemployed) at 10 years, significantly differentiated those in the CS group from those in the NO group. There were no significant interactions between covariates.
DISCUSSION
The average rate of depression was high in this sample. Approximately 70% of the women reported symptoms of depression above the clinical threshold at two or more of the four phases, while only 17% scored below the clinical threshold across all phases of the analysis. The rates of depression in our study are higher than other studies of low-income child-rearing mothers (4, 16, 34, 35).
This higher rate could be due to two factors: the demographic characteristics of the sample, and characteristics of the instrument. The subjects in this study were attending a hospital-based prenatal clinic in an urban area. The women were lower income, few were married, and the average education level at delivery was less than a high school diploma. These demographic characteristics are associated with an increased prevalence of depressive symptoms and depression (2, 15–19, 36).
At the same time, it is possible that the instrument that we used, the CES-D, could have lead to over-reporting symptom levels. In a general population study, 21% scored at or above a cut-point of 16 (29, 32). In psychiatric populations, 99% of the acute depressed patients had CES-D scores of 16 or higher (33). To adjust for the high rates in the study cohort, we defined two groups: those with chronic and mild symptoms of depressions, and those with chronic and severe symptoms. As we demonstrated, it was the latter group that was consistently and significantly different from the women who were not depressed. Therefore, although the rates may be higher than expected, the CS group would be defined as problematic regardless of the base rate of depression in the population.
In the descriptive analyses, there were few differences across the groups at delivery. However, the status of the CS group became more problematic with time compared with those who were not depressed or had only a few occasions of depressive symptoms above the standard cut-off. Given the similarity of the groups at delivery, it may be possible to change the trajectory of symptoms of these severely depressed women if intervention is provided early, during pregnancy or in the immediate postpartum.
In the postpartum, women in the CS group had a lower rate of employment, lower income, and more financial stress. They were less likely to be married, reported less satisfaction with the social support they received from friends and relatives, and experienced more life events. The CS women smoked more cigarettes and used more illicit drugs. When all of the individually significant results were combined in a logistic regression, five factors consistently differentiated the CS group from the NO group: financial stress, marital status, social support, and life events, particularly involvement in a serious argument. It is not possible to tell whether these factors play a role in the development of depression, or in the maintenance of a high level of depressive symptoms, or whether they might be consequences of the depressive symptomatology. They are, however, characteristics that can be evaluated, and that identify women who are at risk of chronic and severe depressive symptoms.
During pregnancy or at delivery, it is important to screen for depression, financial hardship, marital status, substance use, and social support. Identifying women who have multiple risk factors is an important first step toward intervention. Moreover, in the postpartum, mothers are seen by their obstetrician/gynecologist, visit pediatricians with their children, and take their children to nursery or preschool programs. Each of these sites could be utilized to screen for risk factors for chronic and severe depression. If maternal psychological distress, reduced social support, and difficulties with financial resources are evaluated at these various visits, those most at risk for continued depression could be identified, and appropriate interventions instituted.
This study has several limitations. Since the assessments were not done frequently, the patterns of depressive symptoms between interviews may not have been consistent. Assessment of the male partners was not done, and the marital rate does not necessarily represent stability of partners. Maternal history of depression prior to the index pregnancy, the timing of the onset of depressive symptoms, and family history of depression were also not assessed. Finally, the typologies identified the characteristics of chronically depressed mothers, other courses of depression were not studied.
In summary, this study has identified financial strain, low social support, and life events as important correlates of chronic and severe depressive symptoms. The present study has also demonstrated the consistent financial and social disadvantages that are experienced by chronically depressed women of childrearing age. As depression persists, subsequent social and financial disadvantage of these women worsens. Early identification of depression, social support, and financial problems could prevent the long-term pattern of chronic and severe depression across the childrearing years if appropriate intervention could be initiated.
REFERENCES
Gelfand DM, Teti DM. The effects of maternal depression on children. Clin Psychol Rev 1990;10:329–53.
Coleman EZ, Ghodsian M, Wolkind SN. Depression in mothers 6 years after the birth of a first child. Soc Psychiatry 1986;21:76–82.
Philipps LHC, O'Hara MW. Prospective study of postpartum depression: 4 1/2-Year follow-up of women and children. J Abnorm Psychol 1991;100(2):151–5.
Alpern L, Lyons-Ruth K. Preschool children at social risk: Chronicity and timing of maternal depressive symptoms and child behavior problems at school and at home. Dev Psychopathol 1993;5:371–87.
Cooper P, Murray L. Course and recurrence of postnatal depression. Br J Psychiatry 1995;166:191–5.
Campbell SB, Cohn JF. The timing and chronicity of postpartum depression: Implications for infant development. In: Murray L, Cooper PJ, editors. Postpartum depression and child development. New York: Guilford Press, 1997:165– 97.
Najman JM, Anderson MJ, Bor W, O'Callaghan MJ, Williams GM. Postnatal depression – myth and reality: Maternal depression before and after the birth of a child. Soc Psychiatry Psychiatr Epidemiol 2000;35:19–27.
Brennan PA, Hammen C, Andersen MJ, Bor W, Najman JM, Williams GM. Chronicity, severity, and timing of maternal depressive symptoms: Relationships with child outcomes at age 5. Dev Psychol 2000;36(6):759–66.
McLennan JD, Kotelchuck M, Cho H. Prevalence, persistence, and correlates of depressive symptoms in a national sample of mothers of toddlers. J Am Acad Child Adolesc Psychiatry 2001;40(11):1316–23.
Bromet EJ, Solomon ZH, Dunn LO, Nicklas NN. Affective disorder in mothers of young children. Br J Psychiatry 1982;140:30–6.
Campbell SB, Cohn JF, Myers TA. Depression in first-time mothers: Mother infant interaction and depression chronicity. Dev Psychol 1995;31:349–57.
Teti DM, Gelfand DM, Messinger DS, Isabella R. Maternal depression and the quality of early attachment: An examination of infants, preschoolers, and their mothers. Dev Psychol 1995;31:364–76.
Frankel KA, Harmon RJ. Depressed mothers: They don't always look as bad as they feel. J Am Acad Child Adolesc Psychiatry 1996;35:289–98.
NICHD, Early Child, Care Research, Network. Chronicity of maternal depressive symptoms, maternal sensitivity, and child functioning at 36 months. Dev Psychol 1999;35(5):1297–1310.
Brown GW, Bhrolchain MN, Harris T. Social class and psychiatric disturbance among women in an urban population. Sociology 1975;9:225–54.
Hall LA, Williams CA, Greenberg RS. Supports, stressors, and depressive symptoms in low-income mothers of young children. Am J Public Health 1985;75(5):518–22.
Belle D. Poverty and women's health. Am Psychol 1990;45(3):385–9.
Boyce P, Harris M, Silove D, Morgan A, Wilhelm K, Hadzi-Pavlovic D. Psychological factors associated with depression: A study of socially disadvantaged women with young children. J Nerv Ment Dis 1998;186(1):3–11.
Romito P, Saurel-Cubizolles M-J, Lelong N. What makes new mothers unhappy: Psychological distress one year after birth in Italy and France. Soc Sci Med 1999;49:1651–61.
Richman N. Behavioral problems in pre-school children: Family and social factors. Br J Psychiatry 1977;131:523–7.
Lang C, Field T, Pickens J, Martinez A, Bendell D, Yando R, Routh D. Preschoolers of dysphoric mothers. J Child Psychol Psychiatry 1996;37(2):221–4.
D'Arcy C, Siddique CM. Social support and mental health among mothers of preschool and school age children. Soc Psychiatry 1984;19:155–62.
Hall LA, Farel AM. Maternal stresses and depressive symptoms: Correlates of behavior problems in young children. Nurs Res 1988;37(3):156–61.
Reis J. Correlates of depression according to maternal age. J Genet Psychol 1988;149:535–45.
Costello CG. Social factors associated with depression: A retrospective community study. Psychol Med 1982;12:329– 39.
Webster-Stratton C, Hammond M. Maternal depression and its relationship to life stress, perceptions of child behavior problems, parenting behaviors, and child conduct problems. J Abnorm Child Psychol 1988;16(3):299–315.
Schuckit MA. Drug and alcohol abuse: A clinical guide to diagnosis and treatment (4th edn.) New York: Plenum, 1995.
Day NL, Richardson GA, Geva D, Robles N. Alcohol, marijuana, and tobacco: Effects of prenatal exposure on offspring growth and morphology at age six. Alcohol Clin Exp Res 1994;18(4):786–94.
Radloff L. The CES-D Scale: A self-report depression scale for research in the general population. Appl Psychol Meas 1977;1:385–401.
Myers JK, Weissman MM. Use of a self-report symptom scale to detect depression in a community sample. Am J Psychiatry 1980;137(9):1081–4.
Breslau N. Depressive symptoms, major depression, and generalized anxiety: A comparison of self-reports on CES-D and results from diagnostic interviews. Psychiatry Res 1984;15:219–29.
Comstock GW, Helsing KJ. Symptoms of depression in two communities. Psychol Med 1976;6:551–64.
Weissman MM, Sholomskas D, Pottenger M, Prusoff BA, Locke BZ. Assessing depressive symptoms in five psychiatric populations: A validation study. Am J Epidemiol 1977;106(3):203–14.
Burns EI, Doremus PC, Potter MB. Value of health, incidence of depression, and level of self-esteem in low-income mothers of pre-school children. Issues Compr Pediatr Nurs 1990; 13(2):141–53.
Burdette HL, Whitaker RC, Harvey-Berino J, Kahn RS. Depressive symptoms in low-income mothers and emotional and social functioning in their preschool children. Ambul Pediatr 2003;3(6):288–294.
Murphy JM, Olivier DC, Monson RR, Sobol AM, Federman EB, Leighton AH. Depression and anxiety in relation to social status. Arc Gen Psychiatry 1991;48:223–9.
ACKNOWLEDGMENT
The authors wish to thank Young Jhon for her assistance with data analyses.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Seto, M., Cornelius, M.D., Goldschmidt, L. et al. Long-Term Effects of Chronic Depressive Symptoms Among Low-Income Childrearing Mothers. Matern Child Health J 9, 263–271 (2005). https://doi.org/10.1007/s10995-005-0002-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10995-005-0002-x