
Abstract
Over the last few years, the protective role of parental monitoring on adolescent adjustment (i.e., active parental efforts aimed at setting limits and tracking adolescents’ activities and whereabouts) has been challenged. Recent research has shifted attention to the conditions under which monitoring may be more or less effective. Grounded in Self-Determination Theory, this study investigated the role of parents’ autonomy-supportive and psychologically controlling parenting in effects of parental monitoring on adolescents’ adjustment. It also considered the role of adolescents’ clinical status (i.e., clinically referred vs non-referred). Adopting a person-centered approach, we aimed to identify naturally occurring profiles of monitoring, autonomy-support, and psychological control and to examine differences between these profiles in terms of life satisfaction, positive affect, and internalizing and externalizing problems. Participants included 218 referred (Mage = 14.44, 56% girls) and 218 matched adolescents from a larger sample of 1056 community (Mage = 14.83, 52.9% girls). Multigroup Latent Profile Analyses revealed five parenting profiles which were structurally equivalent in both samples: high monitoring with either high autonomy support or high psychological control, low monitoring with either high autonomy-support or high psychological control, and an average profile. Referred youth were significantly more present in the average profile and in the profiles characterized by high levels of psychological control. As hypothesized, profiles showed a differential association with adolescents’ self-reported adjustment, with the high monitoring—high autonomy support profile yielding the most optimal and the low monitoring—high psychological control profile yielding the worst outcomes. Associations between profiles and outcomes were similar for referred and non-referred adolescents. These findings highlight the importance of considering the parenting climate (i.e., autonomy-supportive versus psychologically controlling) to understand effects of parental monitoring during adolescence.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
During the adolescent years, youth increasingly spend more time on their own or with their peers (Larson et al. 1996). As a result, parents have fewer opportunities to directly supervise their offspring and parental monitoring becomes increasingly important. Parental monitoring refers to “a set of parenting behaviors involving attention to and tracking of the child’s whereabouts, activities, and adaptations” (Dishion and McMahon 1998, p. 61). For instance, parental monitoring entails asking an adolescent about what s/he did after school, talking with other adults (e.g., teachers) about the adolescent’s behavior, or checking at what time the adolescent comes home after a party (Barber 1996).
In spite of the commonly held belief that active parental monitoring plays a protective role against engagement in antisocial behavior, drug taking, alcohol misuse, or deviant peer association, observed associations between active monitoring and problem behavior are small at best (see Racz and McMahon 2011 for a review). This observation raises the question whether active monitoring may be effective in reducing problem behaviors and fostering well-being under some conditions but not in others. The present study aims to shed light on this issue by examining whether the more general parenting climate may help to explain under which conditions monitoring relates to adolescents’ problem behavior and well-being. That is, grounded in Self-Determination Theory (Ryan and Deci 2017), this study sought to examine the role of adolescents’ perceived autonomy-supportive and psychologically controlling parenting in effects of monitoring, thereby also examining whether these styles play a (dis)similar role in referred and non-referred youth.
Active Parental Monitoring
Parental monitoring has long been regarded as a key factor in reducing adolescents’ risk for behavioral problems (e.g., Dishion and McMahon 1998; Steinberg et al. 1994). Monitoring has also been linked to lower risk for depression and anxiety (Yap et al. 2014), although these associations are less commonly studied. However, a seminal set of studies conducted by Stattin and Kerr (2000) and Kerr and Stattin (2000) caused a turning point in the monitoring literature by challenging the supposed protective role of parental monitoring. Stattin and Kerr (2000) criticized the typical assessment of parental monitoring, which was most often operationalized as the extent to which parents are knowledgeable of their child’s whereabouts, activities, and friendships (i.e., parental knowledge), instead of measuring the set of active parenting behaviors assumed to be central to parental monitoring (e.g., tracking and supervision; Dishion and McMahon 1998). This inaccurate operationalization led to misinterpretations of the association between parental monitoring and adolescents’ problem behavior. Stattin and Kerr (2000) found that the most important source of parental knowledge is not active parental monitoring as such but adolescents’ spontaneous disclosure of information. As a result, negative associations between parental knowledge and problem behaviors primarily reflect ‘child effects’ (with better adjusted adolescents disclosing more information to parents) instead of ‘socialization effects’, where parents’ active monitoring efforts would protect adolescents against problem behaviors (Laird et al. 2003).
Because measures of parental knowledge do not adequately represent the concept of parental monitoring, the question remains whether parents’ active efforts to monitor their adolescents’ behavior (i.e., the conceptualization of monitoring central in this paper) do yield any benefits. Since Stattin and Kerr’s critical analysis of the monitoring literature, research has increasingly made use of more adequate measures of monitoring that tap into active tracking and supervision of adolescents’ whereabouts. However, most studies relying on such measures found limited evidence for the protective role of active parental monitoring (e.g., Hamza and Willoughby 2011; Keijsers et al. 2010; Kerr and Stattin 2000) and some even linked it to more problematic behaviors (e.g., Kerr et al. 2010; Lansford et al. 2018). Given these inconsistent findings, research has begun to examine conditions under which active monitoring might be more or less effective in fostering adolescents’ psychosocial adjustment. For instance, studies considered the interplay of active monitoring with families’ socio-demographic background and context (e.g., SES and neighborhood safety; Bacchini et al. 2011; Rekker et al. 2017), with adolescents’ peer context (Musci et al. 2015), with adolescent characteristics such as gender (e.g., Kincaid et al. 2012; Villarreal and Nelson 2018) and personality-based or temperamental traits (e.g., Crocetti et al. 2016; Mann et al. 2015; Thompson et al. 2015), and even with genetic markers of susceptibility to environmental influences (e.g., Salvatore et al. 2015; Trucco et al. 2016).
However, few studies to date addressed the role of the more general parenting climate in which active monitoring efforts take place. This is unfortunate because the functional role of specific parenting practices (such as monitoring) may be affected by characteristics of the broader parenting climate (Darling and Steinberg 1993). Accordingly, there is a need to investigate parents’ style of interacting with their adolescent child as a critical condition to explain the effectiveness of parental monitoring. One key dimension of parenting with strong relevance in adolescence is the degree to which parents interact with their child in autonomy-supportive (versus more controlling) ways (Soenens et al. 2018).
Parental Monitoring in the Context of Autonomy-relevant Parenting
The concept of autonomy-supportive parenting is central to Self-Determination Theory (SDT; Ryan and Deci 2017), a general theory on motivation, well-being, and social adjustment. According to this theory, people have three basic psychological needs that are essential to psychological growth, mental health, and adaptive behavior, that is, the needs for autonomy, competence, and relatedness (Ryan and Deci 2017; Vansteenkiste and Ryan 2013). Autonomy refers to the need to experience psychological freedom and to enact behaviors with a sense of authenticity and volition. Relatedness concerns to the need to feel socially connected and cared by significant others. Finally, the need for competence involves the experience of effectiveness and proficiency in achieving one’s goals. Research has convincingly demonstrated that need satisfaction relates positively to adolescents’ psychosocial adjustment, as indexed by vitality, positive affect, and life satisfaction, (e.g., Costa et al. 2016; Rodríguez-Meirinhos et al. 2019; Soenens et al. 2019). However, frustration of these needs would render individuals prone to ill-being and maladjustment (Vansteenkiste and Ryan 2013). In this regard, studies have found that need frustration, which manifests in feelings of pressure and coercion (autonomy frustration), failure and inadequacy (competence frustration), and loneliness and social alienation (relatedness frustration) is associated with adolescents’ maladjustment, including externalizing problems, anxiety, and depressive symptoms (Costa et al. 2016; Inguglia et al. 2018; Rodríguez-Meirinhos et al. 2019).
During adolescence, socializing figures (including parents) play a crucial role in meeting or frustrating these critical needs (Grolnick et al. 1991; Joussemet et al. 2008), with autonomy-relevant parenting being particularly important (Soenens et al. 2018). In SDT, need-supportive and need-thwarting parent-child interactions are typically featured by two autonomy-relevant parenting dimensions, that is autonomy support and psychological control. An autonomy-supportive style facilitates psychological need satisfaction, and satisfaction of the need for autonomy in particular (Soenens et al. 2018). It allows adolescents to experience a sense of volition, for instance, through encouraging initiative, building in desired choices, validating their feelings and perspectives, providing meaningful rationales when choices are constrained, and avoiding the use of controlling language (Joussemet et al. 2008). In contrast, controlling parenting, which is pressuring and domineering in nature (Grolnick and Pomerantz 2009), is likely to actively thwarts children’s psychological needs, giving rise, in particular, to feelings of pressure and coercion (Soenens et al. 2018). One form of controlling parenting studied extensively in adolescence is psychological control (Barber 1996). Psychologically controlling parents rely on intrusive and manipulative tactics such as love withdrawal, guilt induction, disappointment, or shaming to impose their own perspective and demand obedience and conformity with their expectations (Grolnick and Pomerantz 2009; Soenens and Vansteenkiste 2010). When approached in a controlling way, adolescents have no other choice than to act, think, or feel in parent-prescribed ways.
Because of their differential associations with the basic psychological needs, autonomy-supportive and controlling parenting relate differently to adolescents’ adjustment, with autonomy-supportive parenting contributing to well-being (Joussemet et al. 2008; Soenens et al. 2018; Vasquez et al. 2016) and with controlling parenting increasing risk for problem behaviors (Grolnick and Pomerantz 2009; Pinquart 2017a, 2017b; Soenens and Vansteenkiste 2010). Moreover, these parenting styles are assumed to alter the effectiveness of other parenting practices (such as rule-setting and monitoring). While adolescents would be more inclined to accept and endorse parental practices that are conveyed in an autonomy-supportive parenting climate, they would be less likely to do so and even more likely to defensively react against parental practices within a more controlling climate (Ryan and Deci 2017). Research has indeed shown that an autonomy-supportive style when introducing rules is related to better internalization (Soenens et al. 2009), more willing compliance (Laurin and Joussemet 2017), and stronger legitimacy beliefs about parental authority (Van Petegem et al. 2017). When regulations are introduced in autonomy-supportive ways, adolescents are more likely to see the value of these guidelines, feel more volitionally inclined to comply with them, and experience greater psychological need satisfaction while doing so (Vansteenkiste et al. 2018). Conversely, setting limits in a controlling way has been found to hinder internalization and to even elicit oppositional defiance to the parents’ rules (Vansteenkiste et al. 2014).
Because autonomy-supportive and controlling parental styles play a role in the developmental outcomes associated with specific parental practices, an investigation of these styles may also help to clarify when active parental monitoring is effective and when it is not (Enzle and Anderson 1993). As such, it is important to examine combinations of active monitoring and autonomy-relevant parenting. Based on the combination of what parents do (or not do) to regulate the child´s behavior (i.e., high or low monitoring) and how parents follow up on these regulations (i.e., autonomy-supportive or controlling style), Soenens and Vansteenkiste (2010) hypothesized at least four possible combinations. That is, parents can inquire about children’s whereabouts in a more autonomy-supportive or pressuring way. When adopting an autonomy-supportive stance, parents curiously wonder about children’s whereabouts, thereby respecting children’s rhythm of disclosing information, and validating any resistance to do so. Also, they would give meaningful rationales for their monitoring efforts, for instance, by expressing their care and concern. With such an autonomy-supportive parental style, adolescents are more likely to perceive parental authority as legitimate, with this perception contributing to the effectiveness of parental monitoring (Keijsers and Laird 2014; LaFleur et al. 2016). Conversely, if parents adopt a controlling approach, they engage in more intrusive and meddlesome practices. In a Big Brother-like fashion, they would convey a sense of distrust and suspiciously intervene in issues that adolescents consider as more personal. To enforce cooperation and disclosure, they may make use of guilt-tricks, bribes, or sarcasm. With such a controlled style, parental monitoring is likely to be less effective because parental monitoring elicits resistance and even backfires (i.e., relates to increased rather than decreased problem behaviors) when adolescents feel pressured by parents (Tilton-Weaver et al. 2013). Even in the absence of active monitoring, parents may adopt an autonomy-supportive or controlling approach. In the case of low monitoring and high autonomy support, children may get the impression that they enjoy the freedom to do whatever they want. However, in the case of low monitoring with high control parents may come across as unpredictable and hostile. These parents may fail to follow up on agreements, yet, be prone to emotional outbursts where they attack the child for unclearly communicated rules and expectations.
To date, few (if any) studies have directly attempted to identify these four hypothesized profiles and to examine their differential associations with youth problematic behavior and well-being. Yet, there is indirectly relevant evidence for the assumed role of autonomy-relevant communication in effects of monitoring.
A number of studies have documented how the amount and style of regulating adolescent behavior are distinct constructs (e.g., Grolnick et al. 2014; Soenens et al. 2009) that operate in tandem to influence adolescent behavior. For instance, Caron et al. (2006) reported that setting limits, providing consequences, and monitoring the child’s behavior related to fewer behavioral problems, yet only in combination with low psychological control. Similarly, Sher-Censor et al. (2015) showed that parental communication of expectations for behavior related only to lower internalizing and externalizing problems when expectations were communicated in an autonomy-supportive fashion. Likewise, Farkas and Grolnick (2010) found that the combination of parental autonomy support with the provision of consistent expectations as well as feedback about rule-related behaviors related to greater academic engagement.
While previous research indirectly points to the potential role of autonomy-relevant parenting in effects of parental monitoring, no study to date has explicitly investigated how perceived monitoring practices co-occur with autonomy support and psychological control within families. In this regard, person-centered analyses offer a natural and elegant approach to identify parenting profiles combining the degree of monitoring with the style of parenting and to investigate whether adolescents report different levels of psychosocial adjustment depending on their parents’ perceived profile.
Monitoring in Referred and Non-referred Adolescents
Most research on effects of active parental monitoring has relied on samples of adolescents from the general population, with only few studies including adolescents at risk for psychopathology. This is an important lacuna in the literature because adolescents’ risk status may be another factor, next to parents’ autonomy-relevant parenting, that co-determines the effectiveness of active parental monitoring. Moreover, psychological problems are common in adolescence and more prevalent than in other developmental periods (Costello et al. 2011).
In this context, Dishion et al. (2003) suggested that active parental monitoring may come with greater benefits for adolescents who are at higher risk of problem behavior. However, evidence supporting this hypothesis is indirect and limited. For instance, Laird et al. (2010) found that parental solicitation related to reduced antisocial behavior among adolescents spending more unsupervised time, but not among those who spent less time unsupervised. Ahmad et al. (2015) also showed that, among boys, adolescent disclosure of information was related to lower norm-breaking behavior, but only when mothers were high on control (i.e., parental communication of rules and limit-setting), thereby concluding that parental regulation may be more effective among adolescents living in challenging contexts.
Few studies have directly investigated the role of active parental monitoring in problem behavior among adolescents exhibiting behavioral or emotional disorders. Two exceptions are the intervention studies by Tiernan et al. (2015) and Ewing et al. (2015). Both studies showed mixed results, however. While Tiernan et al. (2015) found, in a sample of adolescents exhibiting antisocial behavior, that increases in parental monitoring were associated with reduced levels of antisocial behavior, Ewing et al. (2015) found, in a sample of youth using alcohol and drugs, no significant association with marijuana use. Although evidence is somewhat inconclusive, scholars thus tend to assume that adolescents at risk for psychopathology would benefit most from being monitored more closely.
Some authors even argued that a controlling or pressuring approach would also be more beneficial for at-risk adolescents. For instance, Mason et al. (1996) argued (yet did not provide conclusive evidence) that youths with deviant behaviors benefit more from at least moderate levels of behavioral and psychological control. This argument contradicts predictions derived from SDT, according to which controlling (i.e., pressuring and domineering) parenting behaviors threatens adolescents’ psychological need for autonomy (Joussemet et al. 2008). Because autonomy is a universally important need (Ryan and Deci 2017), SDT assumes that parental autonomy support is beneficial for all adolescents, whereas psychological control increases risk for maladjustment for all adolescents (Soenens et al. 2018). A few studies, provided preliminary evidence for the notion that autonomy-relevant parenting has similar effects in at-risk and community adolescents. For instance, Van Petegem et al. (2015) reported that controlling parenting elicited defiant and rebellious reactions among both referred and non-referred adolescents. Likewise, in an experimental study, Savard et al. (2013) demonstrated that adolescent girls with behavioral or emotional problems found a tedious yet important clinical workshop more valuable and less irritating when introduced in an autonomy-supportive way. However, these studies did not include a comparative, matched control-group. Hence, it remains unclear whether effects of monitoring and autonomy-relevant parenting practices would be different in referred adolescents compared to non-referred youth. An examination of this question is critical because there are conflicting hypotheses in the literature about the degree to which adolescents’ risk status could moderate effects of parental monitoring and controlling parenting. Research on monitoring-relevant dynamics also has strong applied value for intervention programs that better inform parents about beneficial ways of monitoring their adolescent’s whereabouts.
Current Study
This study aimed to examine how active parental monitoring is related to adolescents’ psychosocial adjustment and to contextualize effects of parental monitoring by examining the interplay with perceived autonomy-supportive and controlling parenting. This study focused on adolescents’ perceptions of monitoring and autonomy-relevant parenting because these perceptions ultimately play a more important role in their well-being and behavior than parents’ actual or intended behaviors (Lamborn et al. 1991). Adopting a person-centered approach, the first aim was to identify distinct parenting profiles based on the combination of perceived monitoring, autonomy support, and psychological control using a mixed sample of clinically referred and non-referred adolescents. Specifically, it was expected that both the presence and the absence of monitoring could co-occur in combination with a more autonomy-supportive and a more controlling parenting style, thereby producing four parenting profiles (i.e., Hypothesis 1). Second, the generalizability of the identified parenting profiles across referred and non-referred adolescents was investigated. To do so, the similarity in the obtained profile solution was tested both in terms of its characterization (i.e., number of retained profiles; description of profiles) as well as in terms of the distribution of referred and non-referred individuals across the profiles. Overall, it was anticipated that the structure of the parenting profiles would be similar in the referred and non-referred youth (Hypothesis 2a). Yet, the distribution of referred and non-referred youth was expected to differ across the identified parenting profiles. Previous research suggests that parents tend to reduce their monitoring efforts (Kerr and Stattin 2003) and to engage in more controlling practices when youth display more behavioral or emotional problems (Pinquart et al. 2017a, 2017b). Confronted with an adolescent’s enduring problematic behavior (as in the case of referred youth), parents may give up on attempts to still regulate the adolescent’s behavior. When parents do intervene, their feelings of stress and anger make them prone to engage in more controlling parenting strategies (Mackler et al. 2015; Putnick et al. 2008). Thus, a greater proportion of referred adolescents in profiles characterized by low monitoring and high psychological control was expected (Hypothesis 2b). Third, it was examined whether adolescents belonging to different profiles would differ in terms of their psychosocial adjustment and whether these relations were (dis)similar for referred and non-referred adolescents. Considering the benefits associated with parental autonomy support and the costs associated with psychological control, it was hypothesized that individuals in the profiles high on autonomy support would report greater psychological wellbeing (i.e., life satisfaction and positive affect) and lower externalizing and internalizing problems. The opposite pattern of outcomes was expected in the profiles high on psychological control (Hypothesis 3a). Because the current study is among the first to formally compare effects of monitoring profiles between referred and non-referred adolescents and there are conflicting hypotheses in literature, the moderating role of adolescents’ risk status was examined in a more exploratory fashion (Research Question 3b).
Methods
Participants
This study included a mixed sample of clinically referred and non-referred adolescents. The clinical subsample comprised 218 adolescents between 12 and 17 years of age (M = 14.44, SD = 1.64, 56% girls) that were referred to Child and Adolescent Mental Health services in the Southern region of Spain. Most participants were enrolled in school (96.3%), following compulsory secondary education (80.5%), post-secondary education (9.5%), and professional training (10%). As for family structure, 70.6% lived in two-parent families, 17% were from single-parent families, or 9.6% reconstituted families, and the remaining 2.8% lived with extended relatives who assumed the parental role. Participants’ family socioeconomic status (SES) was measured by the Family Affluence Scale (FASII; Boyce et al. 2006), which indicated a representative range of low (22.5%; 0–3), middle (53.2%; 4–6), and high (24.3%; 7–9) family SES (M = 5.11, SD = 1.92, range = 0–9).
The non-referred group consisted of 1056 community adolescents from 12 to 17 years (M = 14.83, SD = 1.55, 52.9% girls). All participants were enrolled in school, following compulsory secondary education (74.3%), post-secondary education (22.5%), and professional training (3.2%). As for family structure, the majority came from two-parent families (83.6%), whereas the remaining participants lived in single-parent families (9%), in reconstituted families (5.4%), or with other relatives (1.7%). Based on the FASII, 9.1% had low, 44.2% middle, and 46.7% high family SES (M = 6.16, SD = 1.85, range = 1–9).
Participants of both groups were individually matched. Each participant in the referred group was matched with a randomly selected adolescent from the non-referred group that had the same gender, age category (12–14 or 15–17 years old), family structure, and family SES. Through this procedure, two comparable groups of 218 referred and 218 non-referred adolescents were produced. These groups did not differ in terms of gender, χ²(1) = 0.00, p > 0.05, age, t(434) = 0.89, p > 0.05, family structure, χ²(1) = 0.00, p > 0.05, or family SES, χ²(1) = 0.00, p > 0.05, indicating that the matching was successful.
Procedure
Referred adolescents were recruited via 12 Child and Adolescent Mental Health facilities of the public health system in the Southern region of Spain according to a quota sampling procedure. At the first stage, 522 potential eligible participants meeting the selection criteria (aged between 12 and 17 years, living with his/her families instead of residing in an institution, not enduring a psychotic episode or outbreak, and not being intellectually disabled) were identified. As the aim was to select a sample that represented the diversity of adolescents that attend mental health services, eligible participants were then classified into 24 mutually exclusive sub-groups according to their gender (boys and girls), age (12–14 or 15–17 years old), primary referral problem (externalizing, internalizing, or other social, attentional, and thought problems), and the higher parental educational level (basic education: primary, secondary school and medium professional training; or higher education: high-school degree, high professional training, and university). The same number of participants (n = 10) was assigned to each of the 24 subgroups (2 × gender, 2 × age, 3 × primary referral problem, and 2 × parents’ educational level). At the second stage, 287 randomly chosen parents were contacted to provide consent for the participation of their adolescent. Seven sub-groups had less than 10 eligible participants. The acceptance rate was 75.96% (57 parents and 12 adolescents turned down participation).
Non-referred adolescents were recruited from 12 high-schools located in the same areas as the Mental Health facilities. Schools were selected according to the size of the municipality (<30.000 or ≥30.000 inhabitants for small and larger municipalities, respectively), the annual average per capita income of the school area (<21.966€ for low income areas and ≥21.966€ for higher income areas), and the type of school (public or private).
Trained psychologists of the research team administered questionnaires. Referred adolescents filled them in the clinical settings while non-referred did it during school hours.
Measures
Parenting dimensions
A combination of scales and subscales was used to measure adolescents’ perceptions of the parenting behavior. Autonomy support was assessed with a 7-item version (Soenens et al. 2007) of the autonomy support scale of the Perceptions of Parent Scale (Grolnick et al. 1991; e.g., “My parents allow me to decide things for myself”). Active monitoring was measured with the 8-item Parental Monitoring of Behavior subscale from the Parental Regulation Scale—Youth Self-Report (Barber 2002; Soenens et al. 2006; e.g., “My parents ask me questions about how I am behaving outside the home”). Psychological control was tapped with the 8-item Psychological Control Scale—Youth Self-Report (Barber 1996; e.g., “My parents often interrupt me”). Items were rated on a scale from 1 (strongly disagree) to 5 (strongly agree). Cronbach’s alphas were 0.85, 0.86, and 0.90 for autonomy support, monitoring, and psychological control, respectively.
Externalizing and internalizing problems
The scales for internalizing (31 items regarding anxious-depressed, withdrawn-depressed and somatic complaints) and externalizing (32 items regarding rule-breaking behavior and aggressive behavior) problems of the Youth Self Report (Achenbach and Rescorla 2001) were administered to measure adolescents’ emotional and behavioral problems. Participants rated items on a scale from 0 (not true) to 2 (very true or often true), according to the behavior displayed over the last six months. Cronbach’s alphas were 0.90 and 0.90 for internalizing and externalizing problems, respectively.
Life satisfaction
Satisfaction with one’s life was measured with the 5-item Satisfaction with Life Scale (SWLS; Diener et al. 1985; Spanish validation by Atienza et al. 2000). Items (e.g., “I am satisfied with my life”) were rated on a scale from 1 (strongly disagree) to 7 (strongly agree). Cronbach’s alpha was 0.89.
Positive affect
The extent to which participants have felt enthusiastic, active, and alert over the past week was measured with the 10-item positive affect subscale of the Positive and Negative Affect Schedule (PANAS; Watson et al. 1988; Spanish validation by López-Gómez et al. 2015). Items, each one describing a positive emotional state (e.g., “interested”), were rated on a scale from 1 (very slightly or not at all) to 5 (extremely). Cronbach’s alpha was 0.89.
As participants were Spanish speaking, measures that were originally developed in English and had not been previously validated in this language were translated using a forward-backward translation procedure. First, measures were translated from English to Spanish by two researchers fluent in both languages. Afterwards, an independent researcher, also fluent in English and Spanish, translated the resulting items back to English to examine the accuracy of the translation. Discrepancies were discussed until an agreement on the final wording was reached.
Strategy of Analysis
Latent Profile Analysis (LPA) was conducted to identify profiles of parenting based on three manifest indicators, that is autonomy support, psychological control, and active monitoring (Hypothesis 1). Manifest indicators were calculated as mean scores of the items measuring each parenting dimension. Starting with a single solution and sequentially increasing the number of profiles, several nested LPA models (5000 initial random starts, 100 iterations, and 500 optimizations) were estimated separately for each sample. To determine the optimal number of profiles, each model was compared against the model containing one profile less using a combination of fit statistics, interpretability, distinctiveness, and size of the profiles. Fit indices included the Akaike and the Bayesian Information Criteria (AIC and BIC), the sample-sized adjusted BIC (aBIC), the entropy, and the Parametric Bootstrapped Likelihood Ratio Test (BLRT). Smaller AIC, BIC and ABIC values indicate better fit. Entropy values approaching 1 suggests better classification. The BLRT compares the model k profiles to a model with k-1 profiles, and a significant p value suggests that the addition of one more profile led to a significant improvement in model fit.
Multigroup LPA (MLPA; using the KNOWNCLASS option) was conducted to test the similarity of the identified latent parenting profiles across the referred and non-referred samples. Following Olivera-Aguilar and Rikoon (2018), to investigate equivalence in the structure of the profiles (Hypothesis 2a), a semi-constrained model (i.e., means and variances of the profile constituting indicators constrained to equality) was compared against an unconstrained model (i.e., all parameters allowed to vary). To determine whether referred and non-referred adolescents were equally distributed across the profiles (Hypothesis 2b), a fully-constrained model (i.e., the size of the profiles is added to the previous constraints) was compared against the semi-constrained model. Model comparisons were based on the BIC and the Satorra-Bentler Chi-Square Difference Test (SB-Δχ²). Lower BIC values along with a non-significant SB-Δχ² indicated that the invariance assumption held.
Finally, differences between the profiles in terms of several indicators of psychological (mal)adjustment were examined using a MANOVA and subsequent ANOVAs with Bonferroni post-hoc tests (Hypothesis 3a). To investigate whether relations between profiles and outcomes were (dis)similar for referred and non-referred adolescents, a MANOVA was conducted (Research Question 3b).
Preliminary analyses and analyses of (co)variance were conducted in SPSS25. LPA and MLPA were performed in Mplus7.4 using the robust maximum likelihood (MLR) estimator. To reduce the confounding influence of sociodemographic characteristics and to avoid the bias associated with testing invariance with unequal size samples, analyses were conducted with the matched referred (n = 218) and non-referred groups (n = 218) only. The percentage of missing values per variable was ≤0.06% and ≤2.8 for the referred and non-referred samples, respectively. As indicated by the Little’s MCAR test for the referred, χ²(8) = 5.81, p > 0.05, and non-referred, χ²(8) = 7.36, p> 0.05, samples, missings were completely at random. Thus, missing data were handled using pairwise deletion in SPSS and Full Information Maximum Likelihood (FIML) estimation in Mplus.
Results
Preliminary Analyses
Descriptive statistics and bivariate correlations for the study variables are displayed in Table 1. In both samples, perceived autonomy support and psychological control were strongly negatively correlated, and both variables were unrelated to monitoring. Further, autonomy support correlated negatively with externalizing and internalizing problems, and positively with life satisfaction and positive affect, while an opposite pattern of correlations was found for psychological control. No significant correlations were found between monitoring and any of the psychological (mal)adjustment variables in the non-referred group. However, in the referred group, monitoring was negatively correlated with internalizing problems, and positively with positive affect and life satisfaction.
Next, a MANOVA, with adolescents’ clinical status (i.e., referred versus non-referred) serving as the independent variable and the measured constructs as outcomes, showed a multivariate significant effect, Wilk’s Lambda = 0.89; F(7, 421) = 4.47, p < 0.001. Follow-up ANOVAs (see Table 1) revealed that referred adolescents perceived their parents as less autonomy-supportive and more psychologically controlling, while both groups scored equal in terms of perceived monitoring. As expected, the referred group displayed more externalizing and internalizing problems, as well as less life satisfaction and positive affect.
Primary Analyses
Hypothesis 1: Single-group Latent Profile Analysis (LPA). Fit indices for solutions with one to six latent profiles are summarized in Table 2. In the referred sample, the AIC, BIC, and aBIC favored the five-profile solution; the addition of a sixth profile only led to a marginal drop in these values. The BLRT did not provide consistent results because it was significant for each model comparison until seven profiles were compared against six profiles. However, solutions with more than five profiles only showed quantitative differences in terms of profile elevation, but not qualitatively distinct profile shapes. The five-profile solution also achieved the greatest degree of classification accuracy as indicated by the entropy.
In the non-referred sample, the solution with five profiles showed the minimum BIC. The AIC and aBIC decreased only slightly between the five and six-profile solutions. The BLRT suggested that model fit improved as the number of profiles increased but it became non-significant for the solutions with six (versus five) profiles. The entropy was equal or above 0.90 for all solutions. Thus, for the sake of parsimony and given that the added value of person-centered analysis relies on identifying groups with qualitatively distinct patterns, the solution with five profiles was retained as the best fitting and most interpretable solutionFootnote 1.
Hypothesis 2: Multi-group Latent Profile Analysis (MLPA). Next, MLPA was conducted to test whether the retained five-profile solution was equivalent in terms of structure and size of the profiles across the referred and non-referred samples. Results indicated that the semi-constrained model (i.e., means and variances of the parenting indicators defining each profile fixed to equality) led to equal fit as the unconstrained model (BIC = 3545.03 versus 3623.44 for the semi-constrained and unconstrained models, respectively; SB-Δχ²(18) = 27.35, p > 0.05). However, the fully-constrained model (i.e., proportion of individuals assigned to each profile fixed to equality) showed poorer fit than the semi-constrained model (BIC = 3561.02 versus 3545.03 for the fully-constrained and semi-constrained models, respectively; SB-Δχ²(4) = 40.29, p < 0.001). Thus, while the structure of the five-profile solution was equivalent for both groups, the distribution of referred and non-referred adolescents across the profiles was significantly different.
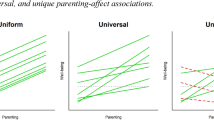
Figure 1 depicts the structure of the five-profile solution obtained in the semi-constrained model. The estimated standardized and raw scores for each parenting indicator within the profiles and the percentage of variance explained in the indicators by the profiles are reported in Table 3. Two autonomy-supportive profiles, one high and one low on parental monitoring, were found. Individuals in the first profile, labelled “High Autonomy support—High Monitoring”, reported high autonomy support, low psychological control, and high monitoring. Individuals in the second profile, labelled “High Autonomy support—Low Monitoring”, exhibited high autonomy support and low psychological control and monitoring. Both profiles were equivalent in terms of autonomy support and psychological control, but differed in the score of monitoring. The third profile, labelled “Average”, was characterized by individuals with average scores on perceived autonomy support, psychological control, and monitoring. Finally, two controlling profiles were found, one low and one high on parental monitoring. Individuals in the fourth profile, labelled “High Psychological Control—High Monitoring”, reported low autonomy support and high psychological control along with low levels of monitoring. Finally, individuals in the fifth profile, labelled “High Psychological Control—Low Monitoring”, scored low on autonomy support and high on psychological control and monitoring. Again, both controlling profiles only differed in terms of monitoring, with the means for autonomy support and psychological control being statistically similar.

Five-profile solution based on the estimated z-scores for autonomy support (AS), psychological control (PC), and monitoring (M)
The distribution of referred and non-referred individuals across the five profiles is shown in Table 3. Compared to the referred sample, a higher proportion of non-referred adolescents were classified into the autonomy-supportive profiles. In contrast, adolescents from the referred sample were comparatively more present in the “Average”, “High Psychological Control—High Monitoring”, and “High Psychological Control—Low Monitoring” profiles.
Hypothesis 3: Associations between profile membership and (mal)adjustment. Finally, it was investigated whether individuals classified into different profiles also differed in terms of psychological (mal)adjustment. As entropy was large (0.94) and most individuals (86%) were assigned with a probability higher than 90% to one of the five profiles, the maximum posterior probabilities from the semi-constrained model were used to determine the most likely profile membership for each individual.
The MANOVA, with profile membership as the independent variable and with externalizing problems, internalizing problems, life satisfaction, and positive affect as the dependent variables, revealed statistically significant multivariate profile differences, Wilks’ λ = 0.45; F(16, 1286) = 25.14, p < 0.001, η2 = 0.19. This finding indicated that participants in distinct latent profiles differed on the combined set of psychological (mal)adjustment indicators. After entering clinical status (referred versus non-referred) in a next step, Wilks’ λ = 0.97; F(4, 416) = 2.79, p = 0.026, η2 = 0.03, the multivariate effect of profile membership remained significant, Wilks’ λ = 0.49; F(16, 1271) = 20.66, p < 0.001, η2 = 0.16. The interaction between clinical status and profile membership was not significant (p > 0.05), suggesting that relations between profiles and outcomes were similar for referred and non-referred individuals.
Subsequent ANOVAs and post-hoc comparisons (see Table 4) indicated that individuals in the autonomy-supportive profiles, and in particular in the profile “High Autonomy support—High Monitoring”, reported the best indices of psychological adjustment. Individuals in these profiles were followed by those in the “Average” profile. Finally, individuals in the controlling profiles, and more specifically in the profile “High Psychological Control—Low Monitoring”, demonstrated the poorest levels of psychological adjustment. Within the autonomy-supportive profiles, individuals in the profile “High Autonomy support—High Monitoring” showed significantly greater life satisfaction and positive affect, but not more externalizing and internalizing problems than individuals in the profile “High Autonomy support—Low Monitoring”. As for the controlling profiles, individuals in the profile “High Psychological Control—High Monitoring” reported lower externalizing and internalizing problems and greater life satisfaction than individuals in the profile “High Psychological Control—Low Monitoring”. Finally, individuals in the “Average” profile showed less externalizing and internalizing problems and more life satisfaction than those in the controlling profiles. The opposite pattern was observed between the “Average” profile and the autonomy-supportive profiles. However, participants in the “Average” profile did not significantly differ from individuals in the profile “High Psychological Control—High Monitoring” in terms of internalizing problems. Participants in the “Average” profile also did not differ from those in the profiles “High Psychological Control—High Monitoring” and “High Autonomy support—Low Monitoring” in terms of positive affect.
Discussion
Since Stattin and Kerr’s (2000) reformulation of parental monitoring, research has called into question the extent to which parents’ active monitoring attempts protect against problem behavior and contribute to positive youth development. Adopting a person-centered approach, this study aimed to contribute to the debate surrounding the effectiveness of active parental monitoring by examining the interplay between perceived monitoring and autonomy-relevant parental practices. Rather than zooming in on isolated parenting dimensions, the aim was to identify naturally occurring combinations of monitoring, autonomy support, and psychological control within families and to examine associations between these profiles and adolescents’ well-being and externalizing and internalizing adjustment problems. This study also attempted to make a novel contribution by investigating the generalizability of the identified parenting profiles across referred and non-referred adolescents.
Consistent with the notion that active monitoring can be implemented with different styles (Soenens and Vansteenkiste 2010), parental monitoring was unrelated to both autonomy support and psychological control. This result provides a first indication that setting rules and tracking an adolescent’s behaviors does not by definition imply being controlling, nor that supporting autonomy is incompatible with parental monitoring. As such, these findings confirm the importance of distinguishing between control-as-structure and control-as-pressure (Grolnick and Pomerantz 2009). Parental behaviors that potentially bring structure to adolescents’ lives (including monitoring and other practices that regulate adolescent behavior) are clearly distinct from parental behaviors that pressure an adolescent into compliance (i.e., low autonomy support and high psychological control).
Profiles of Active Monitoring and Autonomy-relevant Parenting
Congruent with the observed distinctiveness between monitoring and autonomy support and control, person-centered analyses identified five profiles of parenting representing diverse combinations. These different combinations align well with the daily reality of parenting, as parents often rely on a variety of parenting dimensions simultaneously. Specifically, supporting Hypothesis 1, four profiles that matched with those hypothesized on the basis of SDT (Soenens and Vansteenkiste 2010) and one additional average profile were found. Two profiles were characterized by the simultaneous provision of a high degree of perceived autonomy support and low psychological control combined with either high or low monitoring. Adolescents in the “High Autonomy support—High Monitoring” profile view their parents as granting autonomy, yet at the same time inquiring about their whereabouts and checking that they behave according to the rules and expectations. Possibly, these parents monitor their child’s behavior by engaging in a dialogue in which they curiously ask questions, respond with genuine interest to the information disclosed, and make the adolescent feel heard and cared for. In contrast, parents in the “High Autonomy support—Low Monitoring” profile were perceived as granting autonomy but not necessarily offering clear guidelines and tracking their child’s whereabouts. Possibly, this profile is characteristic of adolescents who are naturally well-behaved such that parents do not feel a strong need to actively monitor their activities. Across time, these parents may have developed much confidence in the adolescent’s appropriate behavior, with this confidence also allowing parents to grant more autonomy.
Two other profiles were characterized by the provision of low autonomy support and high psychological control combined with either high or low monitoring. In the “High Psychological Control—High Monitoring” profile, adolescents perceived their parents as actively monitoring their behavior, yet being controlling. Possibly parents use manipulative tactics to request information about their whereabouts and to enforce rule compliance. In contrast, parents in the profile “High Psychological Control—Low Monitoring” also engaged in controlling parenting, yet without actively regulating the adolescent’s behavior. In this case, adolescents may feel pressured to act upon unknown or inconsistent regulations. Parents do not clearly communicate the rules nor attempt to stay informed about their whereabouts, yet still resort to manipulation tactics to influence adolescents’ behavior.
Finally, parents in the “Average” profile clustered around the mean of the pooled sample in terms of the provision of autonomy support, psychological control, and monitoring. These average scores may indicate that perhaps parents monitor the adolescent’s behavior in some domains (e.g., friendships, school performance, digital behavior, etc.) but not in others. Another possibility is that they show substantial daily fluctuations in their parenting behavior, with the ups and downs in parents’ daily behavior being averaged out when adolescents report about their behavior across a longer time span (Mabbe et al. 2018). While on some occasions these parents may have sufficient energy to show genuine interest in their child’s whereabouts, on other moments situational constraints (e.g., adolescents’ misconduct or parental distress) may deplete their energy such that they engage in more psychological control (Aunola et al. 2017).
Supporting Hypotheses 2a and 2b, the same parenting profiles were identified in both referred and non-referred youth, but with different prevalence rates. Overall, there were more adolescents in the autonomy-supportive than in the controlling profiles. However, non-referred adolescents were comparatively more likely to be classified into the “High Autonomy support —High Monitoring” profile, which represented half of the sample, or in the “High Autonomy support—Low Monitoring” profile. Indeed, the proportion of non-referred adolescents in the “Average” or controlling profiles was lower. In contrast, referred adolescents were distributed more evenly across the profiles. Aligned with research showing that problematic behavior elicits more controlling parenting (and vice versa) (Pinquart 2017a, 2017b), a lower proportion of referred adolescents belonged to the autonomy-supportive or “Average” profiles and a greater proportion to the controlling profiles.
Parenting Profiles and Adolescents’ (Mal)adjustment
Demonstrating the importance of distinguishing between the identified profiles, individuals classified into different parenting profiles also differed across a number of psychological (mal)adjustment indicators. According to Hypothesis 3a, adolescents in the “High Autonomy support—High Monitoring” profile displayed the most adaptive pattern of outcomes and even scored higher than adolescents in the “High Autonomy support—Low Monitoring” in terms of life satisfaction and positive affect. These findings are consistent with the notion that a combination of parental regulation and autonomy-supportive parenting, where parents acknowledge the adolescent’s perspective, provide meaningful rationales, and avoid the use of psychologically controlling tactics, is ideal to foster adolescents’ wellbeing (Soenens and Vansteenkiste 2010). Somewhat surprisingly, however, adolescents in the “High Autonomy support—High Monitoring” did not differ from adolescents in the “High Autonomy support—Low Monitoring” profile in terms of externalizing and internalizing problems. The latter finding suggests that the “High Autonomy support—Low Monitoring” profile perhaps does not reflect an overly lenient and permissive parenting profile but may instead represent a profile where parents simply trust their adolescent (because s/he displays low levels of problem behavior) and see no need for strong and active monitoring.
The benefits associated with an autonomy-supportive style of monitoring shown in this study are consistent with the assumption in SDT that the adoption of an autonomy-supportive style contributes to psychological need satisfaction and facilitates rule internalization (Laurin and Joussemet 2017; Vansteenkiste et al. 2018), with these psychological resources in turn contributing to adolescents’ mental health and appropriate behavior (Ryan and Deci 2017).When parents explain the relevance of monitoring attempts, show an interest in the adolescent’s perspective, allow choice, and avoid the use of controlling language, adolescents feel supported in their psychological needs (and in their need for autonomy in particular) and tend to personally endorse regulations (Vansteenkiste et al. 2014). With such experiences of autonomy, adolescents are more likely to experience well-being and, across time, to take responsibility and self-regulate their behavior without parents constantly checking up on them or reminding regulations.
The two profiles characterized by the presence of a controlling style were more clearly differentiated from one another. Adolescents in the “High Psychological Control—Low Monitoring” profile displayed the highest levels of internalizing and externalizing problems, as well as the lowest scores on life satisfaction and positive affect, both in relation to the more adaptive groups and the “High Psychological Control—High Monitoring” profile. This finding, which suggests that the use of psychological control in the absence of parental monitoring is particularly detrimental for adolescents’ psychological adjustment, can be understood on the basis of SDT through the lens of adolescents’ psychological needs. Adolescents in the “High Psychological Control—Low Monitoring” profile likely perceive their parents as both unpredictable and intrusive, with these perceptions undermining both adolescents’ need for competence (i.e., they do not know how to meet parental expectations) and their need for autonomy (i.e., they feel pressured to comply with unclear standards). On the basis of SDT, it can be assumed that this combined threat to the needs for autonomy and competence elicits greater reactance against parental authority, as indicated by externalizing problems (Ryan and Deci 2017; Van Petegem et al. 2015), or greater submissive compliance, as indicated by internalizing problems (Brenning et al. 2019). An alternative interpretation for the observed difference between the controlling profiles is that the provision of parental monitoring in the “High Psychological Control—High Monitoring” profile buffers to a certain extent the effects of psychological control by reducing maladjusted behavior and improving positive outcomes. Although controlling parenting thwarts adolescents’ need for autonomy, monitoring attempts may contribute at least to some extent to satisfaction of the needs for relatedness and competence. Parental monitoring, even when occurring in a controlling climate, may give adolescents a sense that their parents are concerned for their wellbeing and care for them (Hamza and Willoughby 2011). In addition, the fact that parents outline rules and regulation may provide a sense of predictability and knowing what to do, which is central to underpin adolescents’ sense of competence (Farkas and Grolnick 2010; Grolnick et al. 2014).
Summarizing the observed pattern of findings, two conclusions stand out. First, the quality of parenting style (i.e., autonomy-supportive vs. controlling) is of key importance to understand effects of parental monitoring. High parental monitoring was related to better wellbeing and adjustment outcomes when combined with high levels of autonomy support, while it was related to worse outcomes when combined with high levels of psychological control. Second, the presence vs. absence of monitoring made more of a difference when parenting was predominantly controlling than when the style was perceived to be predominantly autonomy-supportive.
The Role of Clinical Status
This study not only examined differences between monitoring-related profiles in terms of adolescents’ (mal)adjustment but is also among the first to formally compare these effects between matched groups of referred and non-referred youth. Because of conflicting hypotheses in the literature and inconsistent indirect evidence (e.g., Mason et al. 1996; Savard et al. 2013; Van Petegem et al. 2015), no a priori hypothesis about the potential moderating role of adolescents’ risk status was formulated. Findings showed that clinical status did not moderate any of the relations between profiles and psychological (mal)adjustment indicators. As such, associations between the parenting profiles and the outcomes were essentially similar for referred and non-referred adolescents.
These results are inconsistent with arguments that adolescents at risk for problems would benefit more from monitoring or even from a controlling parental approach (Mason et al. 1996). Yet, findings are in line with the extended Spectrum Hypothesis (Van Leeuwen et al. 2007), which conceptualizes psychological disorders, not as discrete taxons, but as extremes of a continuum in which the distribution of referred and non-referred individuals partially overlaps. This means that sample differences would only affect mean-level scores and the distribution of participants across profiles, but not the nature or strength of the investigated relations. This is exactly the pattern of findings obtained in the current study. Specifically, referred youth were proportionally more present in the profiles characterized by the presence of psychological control. These findings are also consistent with SDT, according to which autonomy-supportive and controlling parenting appeal to fundamental and largely universal processes, including psychological need satisfaction and internalization (Ryan and Deci 2017; Soenens et al. 2018).
Limitations
Findings should be considered in light of the study limitations. First, its cross-sectional design precluded examination of causality. Although most of the research with a developmental view has examined how parenting shapes child’s behaviors, growing literature from a transactional perspective recognizes that the demanding nature of some difficult behaviors evokes changes in parenting, which in turn may foster or curtail the development of problematic behavior (Sameroff 2009). Accordingly, a longitudinal design is required to unravel the causal association between parenting profiles and outcomes as well as to investigate the developmental trajectories of individuals belonging to distinct profiles. Second, assessments of perceived parenting and psychological outcomes were based on adolescents’ self-reports, which may artificially inflate the strength of these associations through share method variance. Although it was a deliberate choice to focus on adolescents’ perceptions of parenting in the current study (which is the first to identify profiles of monitoring and autonomy-relevant parenting), further research should replicate the current initial findings using a multi-informant (adolescents and parents) and multi-method (self-report and observation) approach. Such research is important not only to strengthen the validity of the assessment of parenting but also to gain insight in factors that determine adolescents’ perceptions of parental behavior. Indeed, there is substantial variability in the way adolescents perceive parental behavior. One and the same parental behavior (e.g., a parent simply asking what the adolescent did with friends after school) can be experienced as an inherently intrusive and controlling practice by one adolescent and as a more harmless or even well-meant practice by another adolescent. These interindividual differences in the perception of parental behavior can be affected by several factors, including the adolescent’s need satisfaction in relation to his/her parents, developmental history, personality, and cultural background (Soenens et al. 2015). In addition to identifying such individual differences, multi-method and multi-informant research allows for an investigation of the independent role of these different sources of information (Ratelle et al. 2018) and to examine whether discrepancies between different sources relate to adolescent adjustment (De Los Reyes and Ohannessian 2016). It could be examined, for instance, whether adolescents who report a more controlling parental style of monitoring than reported by parents themselves are even more at risk for maladjustment (above and beyond the effect of a controlling style as such). Third, this study did not differentiate between maternal and paternal behavior. Fathers and mothers may differ in their mean-level engagement in parenting practices and may also affect adolescents’ outcomes differently (Cabrera et al. 2011). Thus, future research may want to examine whether similar profiles could be identified in mothers and fathers or whether the gender composition of the parent-adolescent dyad influence the relations between profiles and outcomes. Finally, adolescents were not screened for psychopathology to be assigned to one sample or another. Although referred adolescents displayed significantly higher levels of externalizing and internalizing problems, it remains possible that a few individuals in the non-referred sample met diagnostic criteria for psychological disorders or that a few referred adolescents did not showed clinically elevated problems.
Conclusion
During adolescence, youth increasingly spend more unsupervised time and parental strategies to monitor adolescents’ behavior become more important. However, so far, the role of parental active monitoring efforts on adolescents’ psychological and behavioral adjustment has been quite controversial. Research has found limited, if any, evidence for the presumed beneficial and protective effects of active monitoring. On the basis of SDT, this study addressed the possibility that the effectiveness of parental monitoring depends on whether it occurs against the background of an autonomy-supportive or more controlling parenting climate. Using a person-centered approach, this study identified five parenting configurations; two in which high monitoring was combined with either high autonomy support or high psychological control; two in which low monitoring was combined with either high autonomy support or high psychological control; and an average profile. Profile membership was related to different levels of well-being (i.e., life satisfaction and positive affect) and problem behavior (i.e., externalizing and internalizing). Consistently across referred and non-referred groups, adolescents displaying the most optimal pattern of outcomes were classified in the profile high on monitoring and autonomy support. In contrast, the combinations of high psychological control with low, followed by high monitoring, were related to the worst outcomes.
When replicated in methodologically stronger (e.g., longitudinal and multi-informant) studies, these findings may have practical implications. From an applied perspective, results suggest that prevention and intervention parenting programs should not only focus on training parents to actively monitor the adolescents’ behavior, but also on adopting an autonomy-supportive rather than a controlling parenting-approach. Recent attempts to increase parents’ engagement in autonomy-supportive interactions through interventions have yielded promising results (Joussemet et al. 2014, 2018). In addition, given the robustness of the profiles identified among referred and non-referred adolescents, these findings may be informative for tailored interventions. Information of the specific combinations of parenting behaviors that characterize each profile could facilitate giving parents a more personalized advice or, even, referring them to intervention programs that are tailored to their profile and needs (see e.g., Allen et al. 2019). For instance, parents who fail to articulate guidelines and keep track of their youth’ behavior may benefit from an intervention that reinforces the importance of parents’ monitoring, while simultaneously providing them with resources to listen to the adolescent’s perspective, validate his or her feelings, and provide meaningful rationales when following up these regulations. However, the intervention contents related to the importance of monitoring may be less important for parents for who already clearly communicate rules and follow up these regulations yet using a controlling approach. Instead, these parents would need an intervention that provide them with resources to continue monitoring their adolescent behavior but adopting a more autonomy-supportive style.
Notes
Single-group LPA was replicated in the larger non-referred group compromising 1056 adolescents, including the individuals already matched. Although none of the solutions showed a minimum BIC or aBIC value as they decrease with each successive model, the decrease tended to plateau at around five profiles. Similarly, the BLRT was significant for each model comparison. However, as indicated by the Loglikelihood Difference value the added improvement of each solution became smaller when more than five profiles were retained. The entropy value for the five-profile model was higher than for any other solution (0.89) except for the simpler model with two profiles. Thus, these results provided additional trust in the five-profile solution as the most appropriate solution to describe the data of the non-referred group.
References
Achenbach, T. M., & Rescorla, L. A. (2001). Manual for the ASEBA school-age forms and profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth, & Families.
Ahmad, I., Smetana, G. J., & Klimstra, T. (2015). Maternal monitoring, adolescent disclosure, and adolescent adjustment among Palestinian refugee youth in Jordan. Journal of Research on Adolescence, 25(3), 403–411.
Allen, E. S., Grolnick, W. S., & Córdova, J. V. (2019). Evaluating a Self-Determination Theory-based preventive parenting consultation: the parent check-in. Journal of Child and Family Studies, 28(4), 732–743.
Atienza, F. L., Pons, D., Balaguer, I., & García-Merita, M. (2000). Psychometric properties of the Satisfaction with Life scale in adolescents. Psicothema, 12(2), 314–319.
Aunola, K., Viljaranta, J., & Tolvanen, A. (2017). Does daily distress make parents prone to using psychologically controlling parenting? International Journal of Behavioral Development, 41(3), 405–414.
Bacchini, D., Concetta-Miranda, M., & Affuso, G. (2011). Effects of parental monitoring and exposure to community violence on antisocial behavior and anxiety/depression among adolescents. Journal of Interpersonal Violence, 26(2), 269–292.
Barber, B. K. (1996). Parental psychological control: revisiting a neglected construct. Child Development, 67(6), 3296–3319.
Boyce, W., Torsheim, T., Currie, C., & Zambon, A. (2006). The Family Affluence Scale as a measure of national wealth: Validation of an adolescent self-report measure. Social Indicators Research, 78, 473–487.
Brenning, K., Antrop, I., Van Petegem, S., Soenens, B., De Meulenaere, J., Rodríguez-Meirinhos, A. et al. (2019). I won’t obey!: psychologically controlling parenting and (non)-clinical adolescents’ responses to rule-setting. Journal of Clinical Psychology, 75(6), 1034–1046.
Cabrera, N. J., Fagan, J., Wight, V., & Schadler, C. (2011). The influence of mother, father, and child risk on parenting and children’s cognitive and social behaviors. Child Development, 82, 1985–2005.
Caron, A., Weiss, B., Harris, V., & Catron, T. (2006). Parenting behavior dimensions and child psychopathology: specificity, task dependency, and interactive relations. Journal of Clinical Child and Adolescent Psychology, 35(1), 34–45.
Costa, S., Cuzzocrea, F., Gugliandolo, M. C., & Larcan, R. (2016). Associations between parental psychological control and autonomy support, and psychological outcomes in adolescents: The mediating role of need satisfaction and need frustration. Child Indicators Research, 9(4), 1059–1076.
Costello, E. J., Copeland, W., & Angold, A. (2011). Trends in psychopathology across the adolescent years: what changes when children become adolescents, and when adolescents become adults? Journal of Child Psychology and Psychiatry, 52(10), 1015–1025.
Crocetti, E., Van der Graaff, J., Moscatelli, S., Keijsers, L., Koot, H. M., Rubini, M. et al. (2016). A longitudinal study on the effects of parental monitoring on adolescent antisocial behaviors: the moderating role of adolescent empathy. Frontiers in Psychology, https://doi.org/10.3389/fpsyg.2016.01726
Darling, N., & Steinberg, L. (1993). Parenting style as context: an integrative model. Psychological Bulletin, 113(3), 487–496.
De Los Reyes, A., & Ohannessian, C. M. (2016). Introduction to the special issue: discrepancies in adolescent–parent perceptions of the family and adolescent adjustment. Journal of Youth and Adolescence, 45(10), 1957–1972.
Diener, E. D., Emmons, R. A., Larsen, R. J., & Griffin, S. (1985). The satisfaction with life scale. Journal of Personality Assessment, 49(1), 71–75.
Dishion, T. J., & McMahon, R. J. (1998). Parental monitoring and the prevention of child and adolescent problem behavior: a conceptual and empirical formulation. Clinical Child and Family Psychology Review, 1(1), 61–75.
Dishion, T. J., Nelson, S. E., & Kavanagh, K. (2003). The family check-up with high-risk young adolescents: preventing early-onset substance use by parent monitoring. Behavior Therapy, 34(4), 553–571.
Enzle, M. E., & Anderson, S. C. (1993). Surveillant intentions and intrinsic motivation. Journal of Personality and Social Psychology, 64(2), 257–266.
Ewing, B. A., Osilla, K. C., Pedersen, E. R., Hunter, S. B., Miles, J. N., & D’Amico, E. J. (2015). Longitudinal family effects on substance use among an at-risk adolescent sample. Addictive Behaviors, 41, 185–191.
Farkas, M. S., & Grolnick, W. S. (2010). Examining the components and concomitants of parental structure in the academic domain. Motivation and Emotion, 34(3), 266–279.
Grolnick, W. S., & Pomerantz, E. M. (2009). Issues and challenges in studying parental control: toward a new conceptualization. Child Development Perspectives, 3(3), 165–170.
Grolnick, W. S., Raftery-Helmer, J. N., Marbell, K. N., Flamm, E. S., Cardemil, E. V., & Sanchez, M. (2014). Parental provision of structure: implementation and correlates in three domains. Merril-Palmer Quarterly, 60(3), 355–384.
Grolnick, W. S., Ryan, R. M., & Deci, E. (1991). Inner resources for school achievement: motivational mediators of children’s perceptions of their parents. Journal of Educational Psychology, 83(4), 508–517.
Hamza, C. A., & Willoughby, T. (2011). Perceived parental monitoring, adolescent disclosure, and adolescent depressive symptoms: a longitudinal examination. Journal of Youth and Adolescence, 40(7), 902–915.
Inguglia, C., Liga, F., Lo Coco, A., Musso, P., & Ingoglia, S. (2018). Satisfaction and frustration of autonomy and relatedness needs: associations with parenting dimensions and psychological functioning. Motivation and Emotion, 42(5), 691–705.
Joussemet, M., Landry, R., & Koestner, R. (2008). A Self-Determination Theory perspective on parenting. Canadian Psychology, 49(3), 194–200.
Joussemet, M., Mageau, G. A., & Koestner, R. (2014). Promoting optimal parenting and children’s mental health: a preliminary evaluation of the how-to parenting program. Journal of Child and Family Studies, 23(6), 949–964.
Joussemet, M., Mageau, G. A., Larose, M. P., Briand, M., & Vitaro, F. (2018). How to talk so kids will listen & listen so kids will talk: a randomized controlled trial evaluating the efficacy of the how-to parenting program on children’s mental health compared to a wait-list control group. BMC Paediatrics. https://doi.org/10.1186/s12887-018-1227-3
Keijsers, L., Branje, S. J. T., VanderValk, I. E., & Meeus, W. (2010). Reciprocal effects between parental solicitation, parental control, adolescent disclosure, and adolescent delinquency. Journal of Research on Adolescence, 20(1), 88–113.
Keijsers, L., & Laird, R. D. (2014). Mother–adolescent monitoring dynamics and the legitimacy of parental authority. Journal of Adolescence, 37(5), 515–524.
Kerr, M., & Stattin, H. (2000). What parents know, how they know it, and several forms of adolescent adjustment: further support for a reinterpretation of monitoring. Developmental Psychology, 36, 366–380.
Kerr, M., & Stattin, H. (2003). Parenting of adolescents: action or reaction? In A. Booth & A. C. Crouter (Eds), Children’s influence on family dynamics: the neglected side of family relationships (pp. 121–151). Mahwah, NJ: Erlbaum.
Kerr, M., Stattin, H., & Burk, W. J. (2010). A reinterpretation of parental monitoring in longitudinal perspective. Journal of Research on Adolescence, 20(1), 39–64.
Kincaid, C., Jones, D.J., Sterrett, E., & McKee, L. (2012). A review of parenting and adolescent sexual behavior: the moderating role of gender. Clinical Psychology Review, 32(3), 177–188.
LaFleur, L. K., Zhao, Y., Zeringue, M. M., & Laird, R. D. (2016). Warmth and legitimacy beliefs contextualize adolescents’ negative reactions to parental monitoring. Journal of Adolescence, 51, 58–67.
Laird, R. D., Marrero, M. D., & Sentse, M. (2010). Revisiting parental monitoring: evidence that parental solicitation can be effective when needed most. Journal of Youth and Adolescence, 39(12), 1431–1441.
Laird, R. D., Pettit, G. S., Bates, J. E., & Dodge, K. A. (2003). Parents’ monitoring-relevant knowledge and adolescents’ delinquent behavior: evidence of correlated developmental changes and reciprocal influences. Child Development, 74(3), 752–768.
Lamborn, S. D., Mounts, N. S., Steinberg, L., & Dornbusch, S. M. (1991). Patterns of competence and adjustment among adolescents from authoritative, authoritarian, indulgent, and neglectful families. Child Development, 62(5), 1049–1065.
Lansford, J. E., Godwin, J., Al-Hassan, S. M., Bacchini, D., Bornstein, M. H., Chang, L., Chen, B. B. et al. (2018). Longitudinal associations between parenting and youth adjustment in twelve cultural groups: cultural normativeness of parenting as a moderator. Developmental Psychology, 54(2), 362–377.
Larson, R. W., Richards, M. H., Moneta, G., Holmbeck, G., & Duckett, E. (1996). Changes in adolescents’ daily interactions with their families from ages 10 to 18: disengagement and transformation. Developmental Psychology, 32(4), 744–754.
Laurin, J. C., & Joussemet, M. (2017). Parental autonomy-supportive practices and toddlers’ rule internalization: a prospective observational study. Motivation and Emotion, 41(5), 562–575.
López-Gómez, I., Hervás, G., & Vázquez, C. (2015). An adaptation of the Positive and Negative Affect Schedules (PANAS) in a Spanish general sample. Psicología Conductual, 23(3), 529–548.
Mabbe, E., Soenens, B., Vansteenkiste, M., van der Kaap-Deeder, J., & Mouratidis, T. (2018). Day-to-day variation in autonomy-supportive and psychologically controlling parenting: the role of parents’ daily experiences of need satisfaction and need frustration. Parenting Science and Practice, 18(2), 86–109.
Mann, F. D., Kretsch, N., Tackett, J. L., Harden, K. P., & Tucker-Drob, E. M. (2015). Person × environment interactions on adolescent delinquency: sensation seeking, peer deviance and parental monitoring. Personality and Individual Differences, 76, 129–134.
Mason, C. A., Cauce, A. M., Gonzales, N., & Hiraga, Y. (1996). Neither too sweet nor too sour: problem peers, maternal control, and problem behavior in African American adolescents. Child Development, 67(5), 2115–2130.
Mackler, J. S., Kelleher, R. T., Shanahan, L., Calkins, S. D., Keane, S. P., & O’Brien, M. (2015). Parenting stress, parental reactions, and externalizing behavior from ages 4 to 10. Journal of Marriage and Family, 77(2), 388–406.
Musci, R. J., Uhl, G., Maher, B., & Ialongo, N. S. (2015). Testing gene × environment moderation of tobacco and marijuana use trajectories in adolescence and young adulthood. Journal of Consulting and Clinical Psychology, 83(5), 866–874.
Olivera-Aguilar, M., & Rikoon, S. H. (2018). Assessing measurement invariance in multiple-group latent profile analysis. Structural Equation Modeling: A Multidisciplinary Journal, 25(3), 439–452.
Pinquart, M. (2017a). Associations of parenting dimensions and styles with externalizing problems of children and adolescents: an updated meta-analysis. Developmental Psychology, 53(5), 873–932.
Pinquart, M. (2017b). Associations of parenting dimensions and styles with internalizing symptoms in children and adolescents: A meta-analysis. Marriage & Family Review, 53(7), 613–640.
Putnick, D. L., Bornstein, M. H., Hendricks, C., Painter, K. M., Suwalsky, J. T. D., & Collins, W. A. (2008). Parenting stress, perceived parenting behaviors, and adolescent self-concept in European American families. Journal of Family Psychology, 22(5), 752–762.
Racz, S. J., & McMahon, R. J. (2011). The relationship between parental knowledge and monitoring and child and adolescent conduct problems: a 10-year update. Clinical Child and Family Psychology Review, 14(4), 377–398.
Ratelle, C. F., Morin, A. J. S., Guat, F., & Duchesne, S. (2018). Sources of evaluation of parental behaviors as predictors of achievement outcomes. Motivation and Emotion, 42(4), 513–526.
Rekker, R., Keijsers, L., Branje, S., Koot, H., & Meeus, W. (2017). The interplay of parental monitoring and socioeconomic status in predicting minor delinquency between and within adolescents. Journal of Adolescence, 59, 155–165.
Rodríguez-Meirinhos, A., Antolín-Suárez, L., Brenning, K., Vansteenkiste, M., & Oliva, A. (2019). A bright and a dark path to adolescents’ functioning: the role of need satisfaction and need frustration across gender, age, and socioeconomic status. Journal of Happiness Studies. https://doi.org/10.1007/s10902-018-00072-9
Ryan, R. M., & Deci, E. L. (2017). Self-Determination Theory. Basic psychological needs in motivation, development and wellness. New York, NY: Guilford Press.
Sameroff, A. (2009). The transactional model of development: How children and contexts shape each other. Washington, DC: American Psychological Association.
Salvatore, J. E., Aliev, F., Bucholz, K., Agrawal, A., Hesselbrock, V., Hesselbrock, M., Bauer, L. et al. (2015). Polygenic risk for externalizing disorders: gene-by-development and gene-by-environment effects in adolescents and young adults. Clinical Psychological Science, 3(2), 189–201.
Savard, A., Joussemet, M., Emond Pelletier, J., & Mageau, G. A. (2013). The benefits of autonomy-support for adolescents with severe emotional and behavioral problems. Motivation and Emotion, 37(4), 688–700.
Sher-Censor, E., Assor, A., & Oppenheim, D. (2015). The interplay between observed maternal perspective taking and clear expectations: links with male adolescents’ externalizing and internalizing problems. Journal of Child and Family Studies, 24(4), 930–936.
Soenens, B., & Vansteenkiste, M. (2010). A theoretical upgrade of the concept of parental psychological control: proposing new insights on the basis of Self-Determination Theory. Developmental Review, 30(1), 74–99.
Soenens, B., Vansteenkiste, M., & Beyers, W. (2019). Parenting adolescents. In M. H. Bornstein (Ed.), Handbook of parenting, Vol. 1: parenting across the lifespan (pp. 111–167). New York, NY: Routledge.
Soenens, B., Vansteenkiste, M., Lens, W., Luyckx, K., Goossens, L., Beyers, W. et al. (2007). Conceptualizing parental autonomy-support: adolescent perceptions of promotion of independence versus promotion of volitional functioning. Developmental Psychology, 43(3), 633–646.
Soenens, B., Vansteenkiste, M., Luyckx, K., & Goossens, L. (2006). Parenting and adolescent problem behaviors: an integrated model with adolescent self-disclosure and perceived parental knowledge as intervening variables. Developmental Psychology, 42(2), 305–318.
Soenens, B., Vansteenkiste, M., & Niemiec, C. P. (2009). Should parental prohibition of adolescents’ peer relationships be prohibited? Personal Relationships, 16(4), 507–530.
Soenens, B., Vansteenkiste, M., & Van Petegem, S. (2015). Let us not throw out the baby with the bathwater: applying the principle of ‘universalism without uniformity’ to autonomy-supportive and controlling parenting. Child Development Perspectives, 9(1), 44–49.
Soenens, B., Vansteenkiste, M., Van Petegem, S., Beyers, W., & Ryan, R.M. (2018). How to solve the conundrum of adolescent autonomy? On the importance of distinguishing between independence and volitional functioning. In B. Soenens, M. Vansteenkiste, & S. Van Petegem (Eds), Autonomy in adolescent development: towards conceptual clarity (pp. 1–32). Abingdon, UK: Routledge.
Stattin, H., & Kerr, M. (2000). Parental monitoring: a reinterpretation. Child Development, 71, 1072–1085.
Steinberg, L., Fletcher, A., & Darling, N. (1994). Parental monitoring and peer influences on adolescent substance use. Pediatrics, 93(6), 1060–1063.
Thompson, K., Roemer, A., & Leadbeater, B. (2015). Impulsive personality, parental monitoring, and alcohol outcomes from adolescence through young adulthood. Journal of Adolescent Health, 57(3), 320–326.
Tiernan, K., Foster, S. L., Cunningham, P. B., Brennan, P., & Whitmore, E. (2015). Predicting early positive change in multisystemic therapy with youth exhibiting antisocial behaviors. Psychotherapy, 52(1), 93–102.
Tilton-Weaver, L. C., Burk, W. J., Kerr, M., & Stattin, H. (2013). Can parental monitoring and peer management reduce the selection or influence of delinquent peers? Testing the question using a dynamic social network approach. Developmental Psychology, 49(11), 2057–2070.
Trucco, E. M., Villafuerte, S., Heitzeg, M. M., Burmeister, M., & Zucker, R. A. (2016). Susceptibility effects of GABA receptor subunit alpha-2 variants and parental monitoring on externalizing behavior trajectories: risk and protection conveyed by the minor allele. Development and Psychopathology, 28(1), 15–26.
Van Leeuwen, K. G., Mervielde, I., De Clerco, B. J., & De Fruyt, F. (2007). Extending the spectrum idea: child personality, parenting and psychopathology. European Journal of Personality, 21(1), 63–89.
Van Petegem, S., Soenens, B., Vansteenkiste, M., & Beyers, W. (2015). Rebels with a cause? Adolescent defiance from the perspective of reactance theory and Self-Determination Theory. Child Development, 86(3), 903–918.
Van Petegem, S., Vansteenkiste, M., Soenens, B., Zimmermann, G., Antonietti, J. P., Baudat, S., & Audenaert, E. (2017). When do adolescents accept or defy to maternal prohibitions? The role of social domain and communication style. Journal of Youth and Adolescence, 46(5), 1022–1037.
Vansteenkiste, M., Aelterman, N., De Muynck, G., Haerens, J., Patall, E., & Reeve, J. (2018). Fostering personal meaning and self-relevance: a Self-Determination Theory perspective on internalization. The Journal of Experimental Education, 86(1), 30–49.
Vansteenkiste, M., Soenens, B., Van Petegem, S., & Duriez, B. (2014). Longitudinal associations between adolescent perceived degree and style of parental prohibition and internalization and defiance. Developmental Psychology, 50(1), 229–236.
Vansteenkiste, M., & Ryan, R. M. (2013). On psychological growth and vulnerability: Basic psychological need satisfaction and need frustration as a unifying principle. Journal of Psychotherapy Integration, 23, 263–280.
Vasquez, A. C., Patall, E. A., Fong, C. J., Corrigan, A. S., & Pine, L. (2016). Parent autonomy-support, academic achievement, and psychosocial functioning: a meta-analysis of research. Educational Psychology Review, 28(3), 605–644.
Villarreal, D., & Nelson, J. (2018). Parental monitoring and adolescent risk behaviors: the moderating role of adolescent internalizing symptoms and gender. Journal of Child and Family Studies, 27(11), 3627–3637.
Watson, D., Clark, A., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: the PANAS scales. Journal of Personality and Social Psychology, 54(6), 1063–1070.
Yap, M., Pilkington, P., Ryan, S.M., & Jorns, A. (2014). Parental factors associated with depression and anxiety in young people: a systematic review and meta-analysis. Journal of Affective Disorders, 156, 8–23.
Authors’ Contributions
ARM participated in the design and coordination of the study, drafted the manuscript, performed the measurement, conducted the statistical analyses, and interpreted the findings; MV helped to draft the manuscript and participated in the interpretation of the findings; BS helped to draft the manuscript and participated in the interpretation of the findings; AO participated in the design and coordination of the study, helped to draft the manuscript and participated in the interpretation of the findings; KB helped to draft the manuscript and participated in the interpretation of the findings; LAS conceived the study, participated in its design and coordination, helped to draft the manuscript and performed the measurement. All the authors read and approved the final manuscript.
Funding
This study was funded by the Spanish Ministry of Education and Professional Training by a research grant awarded to the first author (grant number: FPU 14/02888).
Data Sharing Declaration
The datasets generated and/or analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures involving human participants in this study were in accordance with the ethical standards of the Biomedical Research Ethics Review Board of Andalucia (Spain) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study and their legal guardians.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Rodríguez-Meirinhos, A., Vansteenkiste, M., Soenens, B. et al. When is Parental Monitoring Effective? A Person-centered Analysis of the Role of Autonomy-supportive and Psychologically Controlling Parenting in Referred and Non-referred Adolescents. J Youth Adolescence 49, 352–368 (2020). https://doi.org/10.1007/s10964-019-01151-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10964-019-01151-7