
Abstract
Based on current theories of depression, reciprocal links between loneliness and depressive symptoms are expected to occur. However, longitudinal studies on adolescent samples are scarce and have yielded conflicting results. The present five-wave longitudinal study from mid- to late adolescence (N = 428, M age at T1 = 15.22 years; 47% female) examined the direction of effect between loneliness and depressive symptoms, using cross-lagged path analysis. In addition, the robustness of these prospective associations was tested by examining the role of the Big Five personality traits (i.e., extraversion, conscientiousness, agreeableness, neuroticism, and openness) as explaining factors and moderators. Results indicated that loneliness and depressive symptoms influenced one another reciprocally, and these reciprocal associations were not attributable to their mutual overlap with personality traits. In addition, neuroticism was found to be a moderator, in that the bidirectional effects between loneliness and depressive symptoms were only found in adolescents high in neuroticism. Practical implications are discussed, and suggestions for future research are outlined.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
During the transition to adulthood, adolescents are faced with multiple developmental challenges, such as the formation of a personalized sense of identity and the establishment of stable peer relationships (Erikson 1968). Although most adolescents succeed in addressing these challenging tasks, others might experience considerable difficulties in doing so. Possibly due to the multiple changes occurring in social networks, loneliness and depressive symptoms are relatively common and interrelated problems in that period of life (Heinrich and Gullone 2006). Specifically, adolescents spend increasingly more time with peers, and less time with parents (Larson and Richards 1991). The ability to establish close peer relationships becomes increasingly important during adolescence. Previous research found, for example, that a lack of friendship intimacy is more strongly related to socio-emotional maladjustment (e.g., depression) in adolescence as compared to preadolescence (Buhrmester 1990). Therefore, adolescence is considered to be a critical period to study the occurrence of loneliness and depressive symptoms, and to examine how both constructs relate to one another and, possibly, even reinforce one another over time.
Although reciprocal links between loneliness and depressive symptoms are theoretically expected (e.g., Joiner 2000), empirical studies regarding cross-temporal associations between these two constructs in adolescence are scarce and are mostly limited to two measurement waves. Possibly as a consequence, these studies have yielded mixed findings (e.g., Lasgaard et al. 2011; Weeks et al. 1980). Because greater insight in the prospective associations between loneliness and depressive symptoms could inform intervention and prevention programs, additional research is needed. The present study represents the first empirical effort to examine reciprocal links between the two constructs across a longer time span (i.e., five annual measurement waves), covering the developmental period from mid- to late adolescence.
In light of the strong associations between personality traits and both loneliness and depressive symptoms (Asendorpf and van Aken 2003; Kotov et al. 2010), the present study investigated the role of the Big Five personality traits (i.e., extraversion, conscientiousness, agreeableness, neuroticism, and openness; McCrae and Costa 1987) in the prospective associations between loneliness and depressive symptoms. By examining both the explaining and moderating role of personality traits, the present study provides a particularly conservative test of the longitudinal associations between both phenomena. Finally, because the prospective associations between loneliness and depressive symptoms might be somewhat different for boys and girls, the role of gender as a moderator of the prospective links between loneliness and depressive symptoms was also explored.
Reciprocal Links Between Loneliness and Depressive Symptoms
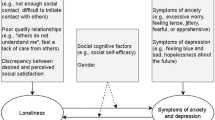
Theories of depression suggest strong and bi-directional links between loneliness and depressive symptoms. Suboptimal social relationships, social rejection, or a lack of social competence—all being germane to the experience of loneliness—may result in increases in depressive symptoms, as recognized by several leading depression theorists (Blatt 1990; Cole et al. 1997; Lewinsohn 1974). Thus, dissatisfaction with one’s social life (as evidenced in feelings of loneliness) may set the stage for dissatisfaction with multiple domains in life, and eventually for depressive symptoms. Conversely, depressive symptoms may give rise to feelings of loneliness as well. For example, Coyne’s (1976) interpersonal theory of depression presumes that depressive episodes produce an array of interpersonal problems and cause damage to close relationships. Specifically, depressed persons may elicit rejection by those with whom they interact (e.g., by excessive reassurance seeking; Joiner et al. 1992), which increases the risk for experiencing loneliness. Collectively, these theories emphasize that reciprocal links between loneliness and depressive symptoms might emerge.
Using cross-sectional assessments, numerous empirical studies confirmed the theoretically expected association between loneliness and depressive symptoms (for reviews, see Heinrich and Gullone 2006; Mahon et al. 2006). However, longitudinal data are needed to infer the temporal sequence between loneliness and depressive symptoms. Unfortunately, only a handful of studies employed such data in adolescence, and these studies produced conflicting results. A first study on college students found no evidence for any prospective relationship between loneliness and depressive symptoms, possibly due to the very brief interval (i.e., 5 weeks) between the two measurement waves (Weeks et al. 1980). Another two-wave study on high school students, which used a one-year time lag, indicated that depressive symptoms predicted subsequent feelings of loneliness, but not vice versa (Lasgaard et al. 2011). A third and final study, conducted on two independent samples of college students, indicated that loneliness was a consistent predictor of later depressive symptoms, whereas the reverse path was present but less consistent (Vanhalst et al. 2010). The mixed results of these short-term longitudinal studies indicate the need for a more extensive study in this developmental phase, as the true nature of cross-temporal links between loneliness and depressive symptoms can only be revealed fully through long-term studies. The present study, with five measurement waves, aims to meet this need.
Concurrent Links with Personality Traits
Previous research on underlying mechanisms in the cross-temporal associations between loneliness and depressive symptoms are scarce. To address this need, the present study examined the role of personality traits in this matter, both as explanatory factors and moderators. Five major personality traits are typically distinguished, collectively referred to as the Big Five. These dimensions are extraversion (i.e., the tendency to engage in social behaviors, and experience frequent positive moods), agreeableness (i.e., an individual’s sociability, empathy, and cooperativeness), conscientiousness (i.e., organizational and motivational aspects of a person’s behavior), neuroticism (i.e., the inability to deal with negative emotions, also referred to as the opposite of emotional stability), and openness (i.e., the way an individual seeks for and deals with new information) (Caspi et al. 2005; Klimstra et al. 2009; McCrae and Costa 1987). The present study focuses on all five personality traits as underlying mechanisms in the relationship between loneliness and depressive symptoms.
Numerous studies have documented associations between these personality traits and depressive symptoms, indicating that extraversion, neuroticism, and conscientiousness are the most consistent correlates of depressive symptoms (for reviews, see Klimstra et al. 2010; Kotov et al. 2010). Fewer studies focused on the associations between the Big Five personality traits and loneliness, and they all indicated that neuroticism and extraversion are important correlates of loneliness (e.g., Asendorpf and van Aken 2003; Cacioppo et al. 2006a; Stokes 1985). In sum, extraverted individuals were less likely to experience depressive symptoms and loneliness, whereas neurotic individuals were more likely to experience both types of internalizing problems.
These findings are not surprising given the widely replicated finding that extraversion is related to positive affect, whereas neuroticism is related to negative affect (for a review, see Larsen and Ketelaar 1991). Indeed, extraversion is considered to represent susceptibility to positive affect due to a strong sensitivity to reward, whereas neuroticism is considered to represent susceptibility to negative affect due to a strong sensitivity to signals of punishment (Eysenck 1987; Gray 1981). This increased susceptibility of neurotic individuals to experience negative affect, for instance, suggests that neuroticism might affect the prospective associations between loneliness and depressive symptoms. In the present study, we will focus on two possible ways in which personality traits may have an impact on the prospective associations between loneliness and depressive symptoms, that is, as explanatory variables or as a moderators.
Personality Traits as Explaining Factors
Personality traits may be the common factors that explain the occurrence of and associations between loneliness and depressive symptoms. Put differently, these associations might be spurious, due to their mutual overlap with an underlying vulnerability (i.e., certain personality traits) to both depression and loneliness. This type of links is implied in the spectrum model (Tackett 2006). The spectrum model posits that personality and psychopathology lie on a single continuum, with problem behavior being an extreme manifestation of certain personality traits. According to this model, personality traits such as neuroticism refer to a broader, more normative set of behaviors, whereas loneliness and depressive symptoms refer to a specific, more extreme set of behaviors. The spectrum model has previously been applied when studying the explanatory role of neuroticism in the co-morbidity between depressive symptoms and anxiety (e.g., Clark et al. 1994; Lamers et al. 2011). However, the only longitudinal study that examined whether personality traits explain the associations between loneliness and depressive symptoms was conducted in the elderly and was limited to neuroticism. Results of this particular study indicated that neuroticism did not explain the prospective associations between loneliness and depressive symptoms (Cacioppo et al. 2010). The present study checked the robustness of the prospective associations between loneliness and depressive symptoms in a much more demanding way, by including all Big Five personality traits as potential explanatory variables in the analysis.
Personality Traits as Moderators
Personality traits also may moderate the associations between loneliness and depressive symptoms. This would imply that these associations would be more pronounced for those adolescents with high or low scores on each of the Big Five personality traits. It could be, for example, that the prospective associations between loneliness and depressive symptoms are stronger among adolescents high in neuroticism compared to adolescents low in neuroticism. One specific model that might bear relevance in this context is the differential exposure-reactivity model (Bolger and Zuckerman 1995), as used in stress research. This model states that personality may influence not only the exposure to stress (e.g., the experience of loneliness) but also the responses to stress. These responses, in turn, may impact the association with, for example, depressive symptoms. Although personality traits were previously investigated as moderators in prospective associations in other domains (e.g., van der Vorst et al. 2007), they have never been examined as a moderator in the relationship between loneliness and depressive symptoms. The present study systematically examines the moderating effects of all Big Five personality traits on the prospective associations between loneliness and depressive symptoms.
Gender Differences
Overall, gender differences start to emerge on a wide number of behavioral and emotional problems during adolescence (Rose and Rudolph 2006). This is particularly true for depressive symptoms (Hankin et al. 1998; Nolen-Hoeksema and Girgus 1994), whereas mixed results are found for loneliness (for reviews, see Borys and Perlman 1985; Mahon et al. 2005). As female adolescents usually report higher depressive symptoms (Hankin et al. 1998; Nolen-Hoeksema and Girgus 1994), the prospective association between loneliness and depressive symptoms could be stronger for females. However, only few studies examined gender differences in the association between loneliness and depressive symptoms in adolescence. In general, these studies showed that the association between loneliness and depressive symptoms is comparably strong in male and female adolescents (e.g., Koenig et al. 1994; Lasgaard et al. 2011). Studies in adulthood, however, show mixed results, with some studies indicating no gender differences (e.g., Cacioppo et al. 2010), and other studies indicating that the association between loneliness and depressive symptoms is stronger for men than for women (e.g., Cacioppo et al. 2006b). Additionally, gender differences on the Big Five personality traits are considered in the present study, given the contradicting results in previous studies in adolescence (for a review, see Klimstra et al. 2009). In sum, the present study examined mean-level gender differences in loneliness, depressive symptoms, and personality traits, and further examined whether gender moderated the temporal associations between loneliness and depressive symptoms.
The Present Study
Mid-to-late adolescence is considered to be a critical developmental period for studying vulnerability to depression and loneliness (Hankin et al. 1998; Goossens 2006). However, despite the overly replicated strong association between both internalizing problems (Heinrich and Gullone 2006; Mahon et al. 2006), the prospective associations between loneliness and depressive symptoms only rarely have been investigated in this developmental phase. The present study aims to fill this important gap in the literature by investigating the temporal sequence between loneliness and depressive symptoms in a 5-year longitudinal study from mid- to late adolescence, by means of cross-lagged path analysis. This statistical procedure allows for accurate estimates of cross-time effects that link the constructs involved, with appropriate controls for all within-time associations (i.e., the correlation between the different variables at each point in time) and stability coefficients (i.e., prediction of a variable by its level at previous time points). Based on existing depression theories (e.g., Blatt 1990; Coyne 1976), we expected reciprocal associations to emerge.
The role of personality traits in these associations was examined in two different ways. First, we investigated whether the prospective associations between loneliness and depressive symptoms were explained by personality, by comparing a cross-lagged model with and without controlling for all Big Five personality traits. Second, we investigated whether the prospective associations between loneliness and depressive symptoms were different for adolescents with high versus low levels of specific Big Five personality traits (i.e., whether specific personality traits acted as moderators). Previous studies have shown that both neuroticism and extraversion are consistent correlates of loneliness and depressive symptoms in adolescence (e.g., Asendorpf and van Aken 2003; Klimstra et al. 2010), and that neuroticism represents a specific susceptibility to negative affect (Eysenck 1987; Gray 1981). Therefore, we specifically expected that neuroticism would explain or moderate the prospective associations between loneliness and depressive symptoms. Finally, the role of gender was examined. Although we expected adolescent girls to show more depressive symptoms compared to boys (Nolen-Hoeksema and Girgus 1994), no gender differences were expected in the prospective associations between loneliness and depressive symptoms (Cacioppo et al. 2010; Lasgaard et al. 2011).
Method
Participants and Procedure
Data from the “Family and Health” project, conducted in The Netherlands, were used for the present study. This longitudinal project examines different socialization processes related to various health behaviors in adolescents and their families, including alcohol use, smoking, and psychosocial adjustment (Harakeh et al. 2005; van der Vorst et al. 2005). Families with two parents and at least two children aged 13–16 years (no twins, nor mentally or physically disabled) were selected from the registers of 22 municipalities, both from rural and urban areas. Approximately 5,000 invitation letters were sent, and 885 families agreed to participate by returning the response forms. The remaining families were contacted by telephone to ascertain whether they met inclusion criteria, which was the case for 765 families. Because of financial constraints we only were able to select a maximum of 428 families, based on a further selection to obtain an equal distribution of sex and educational level of the adolescents. Trained interviewers visited the participants at home, asking all four family members to complete an extensive questionnaire individually. Each family received € 30 (about 45 US dollar) if all four family members completed the questionnaire. Additionally, after completion of three waves, five travel cheques of € 1,000 (about 1,500 US dollar) were raffled among the participating families.
So far, five annual waves that included measures of loneliness and depressive symptoms were collected between 2002 and 2006. At the first wave (T1), 428 families participated. Drop-out was low, with 416 families (97%) participating in the second wave (T2), 403 families (94%) participating in the third wave (T3), 356 families (83%) participating in the fourth wave (T4), and 313 families (73%) at the fifth wave (T5). Participants with and without complete data were compared using Little’s (1988) Missing Completely At Random (MCAR) test. This comparison yielded a non-significant Chi-square value (χ² (496) = 398.82, ns), suggesting that missing values could be reliably estimated. Missing values were estimated using the full-information maximum likelihood (FIML) procedure. In the present study, only data obtained from the oldest child in the family were used, because these individuals fell in the age range that spans mid- to late adolescence (Mage at T1 was 15.22 years, SD = .60). More than 95% of the adolescents were Caucasian, and there was an equal distribution of gender (53% was male) and educational level (29% followed preparatory secondary vocational education, 29% followed senior general secondary education, 40% followed pre-university education, and 2% followed other types of education). All primary analyses were conducted in Mplus (Version 4; Muthén and Muthén 2002).
Measures
Loneliness
The subscale peer-related loneliness of the Loneliness and Aloneness Scale for Children and Adolescents (Marcoen et al. 1987) was used to capture loneliness. The instrument was developed for use with Dutch-speaking participants and has high internal consistency and construct validity (Goossens et al. 2009). The subscale used in the present study contains 12 items answered on a 4-point Likert-type scale, ranging from 1 (never) to 4 (often). A sample item reads “I feel left out by my friends”. Cronbach’s alphas at T1-T5 varied between .90 and .94, with a mean of .92.
Depressive Symptoms
Depressive symptomatology was measured using a six-item questionnaire (Kandel and Davies 1982), which has been shown to have good concurrent validity in Dutch young adults (van Roekel et al. 2011). Items were answered on a 5-point Likert-type scale, ranging from 1 (never) to 5 (always). A sample item reads “During the last year, I felt unhappy, sad and depressed”. Cronbach’s alphas at T1-T5 varied between .78 and .87, with a mean of .82.
Personality Traits
Personality traits were assessed at T1 with the Dutch version of the Quick Big Five questionnaire (Goldberg 1992; Vermulst and Gerris 2005), which previously has been shown to have good internal validity (Akse et al. 2004). A 7-point Likert scale, ranging from 1 (completely untrue) to 7 (completely true), was used when scoring 30 items that assess five personality dimensions: Extraversion, Agreeableness, Conscientiousness, Neuroticism, and Openness. All dimensions are measured with 6 items each, such as: talkative (Extraversion), sympathetic (Agreeableness), systematic (Conscientiousness), worried (Neuroticism), and creative (Openness). Cronbach’s alpha was .84 for Extraversion, .77 for Agreeableness, .85 for Conscientiousness, .73 for Neuroticism, and .70 for Openness.
Results
Preliminary Analyses
Table 1 lists means and standard deviations by gender, along with correlations between loneliness and depressive symptoms at each time point. Stability coefficients (i.e., the correlation between two subsequent measurement occasions) were high for both loneliness (ranging between .62 and .67; all ps < .001) and depressive symptoms (ranging between .54 and .58; all ps < .001). Within-time correlations between loneliness and depressive symptoms ranged from .34 to .50 (all ps < .001), showing that loneliness and depressive symptoms co-occurred. As shown in Table 2, personality traits related somewhat differently to loneliness and depressive symptoms, that is, the direction of the correlations was the same, but the strength differed. Specifically, loneliness was related more strongly (and negatively) to extraversion (t (425) = 13.01, p < .001) and agreeableness (t (425) = 9.69, p < .001), whereas depressive symptoms were related more strongly (and positively) to neuroticism (t (425) = 9.49, p < .001). Furthermore, conscientiousness only was related negatively to depressive symptoms, but not to loneliness, and openness only was related negatively to loneliness, but not to depressive symptoms.
To investigate gender differences in loneliness and depressive symptoms, a MANOVA was performed with gender as fixed factor, and loneliness and depressive symptoms at all time points as dependent variables. This yielded a significant effect (Wilks’ λ = .88; F (10,280) = 3.78, p < .001; η² = .12). Follow-up analyses showed that female adolescents were higher on both loneliness and depressive symptoms at all time points, although the effect sizes of loneliness (η² ranging between .01 and .03) were smaller than the effect sizes of depressive symptoms (η² ranging between .04 and .09). Similarly, a MANOVA was performed with gender as fixed factor and the Big Five personality traits as dependent variables. This yielded a significant effect (Wilks’ λ = .96; F (5,409) = 3.16, p < .01; η² = .04. Follow-up analyses indicated that gender had a significant effect on neuroticism only, with female adolescents (M = 3.78; SD = .06) showing higher levels of neuroticism than male adolescents (M = 3.56; SD = .06; F (1,420) = 6.59, p < .05). Finally, analyses of variance with repeated measures (RANOVA) indicated a significant decrease in both depressive symptoms (Wilks’ λ = .75; F (4, 288) = 23.96, p < .001) and loneliness (Wilks’ λ = .95; F (4, 287) = 3.89, p < .01) over time, but there were no gender differences in the mean-level changes of either loneliness (Wilks’ λ = .95; F (4,286) = 0.21, ns) or depressive symptoms (Wilks’ λ = .99; F (4,287) = 0.18, ns).
Temporal Sequence of Loneliness and Depressive Symptoms
Various indices were used to evaluate model fit of the cross-lagged model (Kline 2005). The Chi-square (χ²) should be as small as possible, the Comparative Fit Index (CFI) should exceed .90 for a reasonable fit and .95 for a good fit to the data, and the Root Mean Square Error of Approximation (RMSEA) should be less than .05 for a close approximate fit, or between .05 and .08 for a reasonable fit to the data.
An unconstrained model with all stability paths, within-time correlations and cross-lagged paths in both directions was estimated (χ² (24) = 146.49, p < .001; CFI = .92; RMSEA = .11). Next, this model was compared with a model in which the following three parameters were constrained to be equal across time: (a) stability paths of depressive symptoms, (b) stability paths of loneliness, and (c) correlated changes between loneliness and depressive symptoms, that is, correlations between the residuals of loneliness and depressive symptoms at T2, T3, T4, and T5 (e.g., Asendorpf and van Aken 2003). The hypothesis of invariance would be rejected if the difference in the χ² index of both models is significant at p < .05 (Steiger et al. 1985). Results indicated that all stability paths and correlated changes could be considered equal across time (Δχ² (9) = 11.02, ns). In a next step, we constrained all cross-lagged paths from loneliness to depressive symptoms and all cross-lagged paths from depressive symptoms to loneliness, respectively, to be equal across time. Model comparison indicated that these constraints were allowed (Δχ² (15) = 24.30, ns), and loneliness was a stronger predictor of depressive symptoms (B = .13, p < .001) than vice versa (B = .07, p < .001). This final bidirectional model had an acceptable fit to the data (χ² (39) = 170.79, p < .001; CFI = .92; RMSEA = .09), and is represented in Fig. 1.

Final cross-lagged model with standardized path coefficients. Parameter estimates before the slash represent the estimates of the model without controls for personality traits; parameter estimates after the slash represent estimates of the model with controls for personality traits. T = Time. All p < .001
A multigroup comparison was used to examine gender differences. This approach compares a constrained model (e.g., a model in which the estimated cross-lagged parameters are set equal across gender) with an unconstrained model (e.g., a model in which these parameters are allowed to vary across gender). The hypothesis of invariance would be rejected if the difference in the χ² index of both models was significant at p < .05. Results indicated that the cross-lagged model fitted equally well for males and females (Δχ² (2) = 4.71, ns).
Role of Personality Traits
To investigate whether personality traits explain the prospective associations between loneliness and depressive symptoms, we compared our final cross-lagged model with the same model including controls for the Big Five personality traits. Therefore, paths from all five personality traits to depressive symptoms and loneliness at each time point were included in the model (Bollen 1989). This model had an acceptable fit to the data (χ² (77) = 215.52, p < .001; CFI = .92; RMSEA = .07). Loneliness and depressive symptoms were bidirectionally related, as was the case in the original model, and only small differences in parameter estimates between the two models emerged (see Fig. 1). Thus, the prospective associations between loneliness and depressive symptoms were not attributable to personality traits.
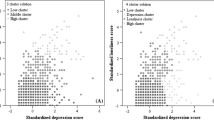
To investigate the moderating effects of personality traits, groups of participants with high versus low levels of each of the Big Five personality traits were determined through a median split procedure. Next, the parameters of the cross-lagged model were compared in both groups by means of a multigroup comparison for each Big Five trait. Results indicated that the model fitted equally well among high and low levels of extraversion (Δχ² (2) = 2.14, ns), conscientiousness (Δχ² (2) = 4.95, ns), agreeableness (Δχ² (2) = 0.28, ns), and openness (Δχ² (2) = 2.40, ns). However, a significant difference was found for neuroticism (Δχ² (2) = 7.56, p < .05). Specifically, the cross-paths between loneliness and depressive symptoms were significant in the group with high levels of neuroticism (B = .14 for the path from loneliness to depressive symptoms; B = .10 for the reverse path; all p < .001), but not significant in the group with low levels of neuroticism (B = .06 for the path from loneliness to depressive symptoms; B = .01 for the reverse path; ns).
Discussion
Both loneliness and depressive symptoms represent important and interrelated problems in adolescence (Allen and Sheeber 2009; Goossens 2006). However, findings on the direction of prospective links between these two types of internalizing problems were inconsistent (Lasgaard et al. 2011; Vanhalst et al. 2010; Weeks et al. 1980) and information on the role of personality traits and gender in these associations was limited, despite strong concurrent associations between the two constructs and personality traits (Asendorpf and van Aken 2003; Kotov et al. 2010). The present study, which relied on an extensive, five-wave design, contributed to extant literature in three important ways. First, cross-lagged path analysis indicated that loneliness and depressive symptoms influenced one another bidirectionally from mid- to late adolescence, with the direction from loneliness to depressive symptoms being stronger than the reversed direction. Second, this vicious circle between loneliness and depressive symptoms proved to be highly robust, as it could not be “explained away” by the Big Five personality traits when applying appropriate statistical controls. Third and finally, neuroticism was the only personality trait that acted as a moderator, in that the bidirectional associations between loneliness and depressive symptoms only emerged in relatively neurotic adolescents. This finding suggests a particular type of vulnerability for the development of internalizing problems in adolescents with high scores on neuroticism.
The Vicious Circle Between Loneliness and Depressive Symptoms: Potential Intervening Mechanisms
The reciprocal relationship between loneliness and depressives symptoms suggests that lonely adolescents are at risk for later depressive symptoms, and, conversely, depressed adolescents have an increased tendency to experience loneliness over time, as could be expected based on depression theories (Blatt 1990; Coyne 1976; Lewinsohn 1974). This finding integrates the results of two earlier studies on cross-lagged effects between loneliness and depressive symptoms in late adolescence. Whereas the study of Lasgaard et al. (2011) found a unidirectional association from depressive symptoms to subsequent levels of loneliness, the study of Vanhalst et al. (2010) found bidirectional associations, with the path from loneliness to subsequent depressive symptoms being stronger than the reverse path. However, these short-term longitudinal studies only may have shown a snapshot of the underlying, long-term bidirectional process occurring across adolescence as shown in the present five-wave longitudinal study. Our results, therefore, suggest that a cyclical process between loneliness and depressive symptoms might be at work that maintains and potentially enhances both forms of maladjustment.
Intervening mechanisms that perpetuate or interrupt the vicious circle between loneliness and depressive symptoms should be explored in future research. Previous research found that passive coping strategies in general, and rumination about loneliness in particular, partially mediated the relationship between loneliness and depressive symptoms (Vanhalst et al. 2010, in press). However, there are additional mechanisms that could explain why lonely adolescents are at risk for later depressive symptoms. For example, lonely people typically attribute their interpersonal failures to personal and unchangeable characteristics (e.g., shyness or low ability), and their interpersonal successes to luck or other external factors (Anderson 1999; Heinrich and Gullone 2006). This detrimental attribution style also was found to relate to depressive symptoms (Anderson 1999). Therefore, we suggest future research to focus on attribution style as a mediator between loneliness and depressive symptoms.
A possible intervening mechanism in the opposite direction (i.e., from depressive symptoms to loneliness) can be derived from Coyne’s (1976) interpersonal theory of depression. This theory postulates that the interpersonal behaviors and attitudes of depressed individuals tend to induce rejection by significant others. Several studies to date focused on reassurance seeking as an example of such rejection-evoking behavior (e.g., Joiner et al. 1992, 1999). Specifically, depressed individuals tend to seek reassurance from significant others to alleviate their doubts about whether others truly care about them. However, excessive reassurance seeking may evoke aggravating reactions from significant others, and ultimately lead to rejection, and, therefore, to experiences of loneliness. So far, reassurance seeking has been investigated mainly as a perpetuating factor in long-term depression, but in our opinion it also should be considered as a possible mediating factor in the association between depressive symptoms and loneliness. In sum, we suggest that future research investigates these possible intervening variables (i.e., coping, attribution style, and reassurance seeking) as contributors to loneliness, depressive symptoms, and the interplay between both variables. Examining these variables together has the additional advantage to distinguish between unique and shared effects, and to examine possible interactions.
Robustness of the Associations Between Loneliness and Depressive Symptoms
In a first set of additional analyses, the robustness of the vicious circle between loneliness and depressive symptoms was tested by statistically controlling for the effect of personality traits. In line with previous cross-sectional and longitudinal studies that had examined only the role of neuroticism (Cacioppo et al. 2006a, 2010), controlling for the Big Five personality traits at baseline did not alter the prospective associations between loneliness and depressive symptoms. Thus, personality traits did not explain the vicious circle between loneliness and depressive symptoms, showing that the associations between loneliness and depressive symptoms are fairly robust.
Looking for Vulnerable Subgroups: Moderating Role of Neuroticism
In a second set of additional analyses, we examined the moderating effects of gender and personality traits. By doing so, we could distinguish vulnerable subgroups of adolescents, that is, groups for whom the vicious circle linking loneliness to depressive symptoms was more pronounced than in others. First, consistent with previous studies (e.g., Lasgaard et al. 2011), gender did not affect the prospective associations between loneliness and depressive symptoms, although girls experienced more loneliness and depressive symptoms than boys at all measurement occasions. Hence, despite such mean differences, the actual sequence linking loneliness to depressive symptoms over time was virtually identical for boys and girls. Second, no differences in the strength of the prospective associations were found between adolescents with high versus low levels of extraversion, conscientiousness, agreeableness, or openness. However, neuroticism was found to moderate these prospective associations. Specifically, whereas bidirectional prospective effects were found for adolescents with high levels of neuroticism, no such effects were found for adolescents with low levels of neuroticism. The only vulnerable group identified in the present study, therefore, consists of adolescents with high scores on the personality trait of neuroticism.
Our results, therefore, indicate that neuroticism is a specific risk factor for the longitudinal co-morbidity between loneliness and depressive symptoms, because it increases the probability that the one internalizing symptom will evolve into the other. This may imply that neuroticism not only relates to higher levels of loneliness and depressive symptoms but also exacerbates those outcomes. This finding is in line with the definition of neuroticism (i.e., the inability to deal with negative emotions; Caspi et al. 2005), in that neurotic adolescents are unable to prevent their experience of loneliness from progressing into later depressive symptoms, and vice versa. The pattern of findings obtained is further compatible with the differential exposure-reactivity model, proposed by Bolger and Zuckerman (1995) as a framework for examining the relationships between personality and stress. The differential exposure-reactivity model states that personality may not only influence the exposure to stress but also the responses to stress. Applied to the variables of interest of the present study, personality traits (and particularly neuroticism) may be related not only to the experience of loneliness but also to the responses to loneliness, and therefore, to possible consequences such as depressive symptoms. However, additional research is needed to make clear statements about the role of neuroticism in the link between loneliness and depressive symptoms.
Practical Implications
Both the prospective results and the moderating role of neuroticism may have implications for prevention and intervention programs in clinical settings, but also in the school or family context. For example, parents or teachers could be encouraged to be attentive towards signs of enduring loneliness in their children or students, and to seek help before it evolves into depression. School counselors that treat adolescents with symptoms of loneliness or depression, should be particularly alert if these adolescents also show signs of neuroticism. Furthermore, a loneliness or neuroticism screening instrument could be employed to identify adolescents that are particularly at risk for depression, and, therefore, particularly might benefit from prevention programs (for cut-off scores for neuroticism and loneliness, see Costa and McCrae 1992, and Perry 1990, respectively). The vicious circle between loneliness and depressive symptoms can further be relevant for bullying intervention programs, as bullying is associated with both loneliness and depressive symptoms (Hawker and Boulton 2000).
Clinical intervention programs should aim to break the vicious circle that makes lonely people vulnerable for later depressive symptomatology and vice versa, to ensure that these internalizing problems do not escalate. One way to do so would be to improve emotional stability, given that emotional stability (i.e., low neuroticism) was found to be a protective factor against these internalizing problems reinforcing one another across time. Although core personality traits such as neuroticism are considered to be difficult to modify, specific facets of the different core traits may be more amendable (Costa and McCrae 1995; McCrae and Costa 1999). Therefore, future research should focus on specific facets of neuroticism and investigate which of these facets are particularly harmful or protective for the experience of loneliness, depressive symptoms or the association between the two. For example, previous research indicated that different facets of neuroticism (e.g., hostility, self-consciousness, or vulnerability) are differently related to positive and negative affect, life satisfaction, and happiness (Quevedo and Abella 2011). We further argue that the role of attribution styles in the association between loneliness and depressive symptoms is an important area for clinical practice, given the association between maladaptive attribution styles with both loneliness and depressive symptoms (Anderson 1999). Indeed, loneliness interventions that addressed maladaptive social cognition (including attribution style) had a larger effect size compared to any other type of intervention (i.e., addressing social support, social skills, and opportunities for social interventions; Masi et al. 2011).
Limitations and Conclusion
Although the present article yielded important information on the temporal sequence of loneliness and depressive symptoms, some limitations and suggestions for future research need to be mentioned. First, the adolescents in the present study were raised in intact two-parent families and were mainly Caucasian. Regarding family situations, previous research indicated that children from intact families had, on average, better psychological and psychosocial adjustment in comparison to children from divorced families (i.e., including lower scores on depressive symptoms and loneliness; Amato and Keith 1991). Regarding ethnicity, adolescents from ethnic minorities showed higher levels of depressive symptoms (Anderson and Mayes 2010) and loneliness (Bellmore et al. 2004) compared to adolescents from ethnic majorities. However, although mean differences in loneliness and depressive symptoms may be expected to emerge, studies in older adults indicated that the association between loneliness and depressive symptoms is similar across family situations and ethnicity (Cacioppo et al. 2006a, b). In sum, future studies in adolescence that are more balanced in terms of family situations and background are required to assess further the generalizability of our findings.
A second limitation of the present study may be related to shared method variance, caused by the exclusive use of self-report measures. However, loneliness and depressive symptoms are internal and subjective processes, which are most appropriately investigated with self-report measures. With respect to personality traits, other-reported measures could be used, although a recent study showed that these measures might be as informative about the raters’ personality as they are about the personality of the person being rated (Wood et al. 2010). Third, personality traits were measured only at baseline in the present study. Although personality traits are generally considered to be stable over time, a recent study indicated that certain personality traits (such as neuroticism) mature across adolescence (Klimstra et al. 2009). Therefore, future research should investigate the role of personality traits longitudinally, and examine whether changes in personality levels are accompanied by changes in the prospective effects between loneliness and depressive symptoms.
Despite the limitations mentioned, the present five-wave longitudinal study was the first to demonstrate that loneliness and depressive symptoms influence one another in mutual fashion from mid- to late adolescence. This type of developmental interplay cannot simply be reduced to the association that both types of internalizing problems have with any of the Big Five personality traits. Finally, as neuroticism was found to moderate the bidirectional associations between loneliness and depressive symptoms, adolescents who score high on the Big Five trait of neuroticism seem to represent a specific risk group that deserves special attention from all adults involved in the care of adolescents, professionally or otherwise.
References
Akse, J., Hale, W. W., Engels, R. C. M. E., Raaijmakers, Q. A. W., & Meeus, W. H. J. (2004). Personality, perceived parental rejection and problem behavior in adolescence. Social Psychiatry and Psychiatric Epidemiology, 39, 980–988.
Allen, N. B., & Sheeber, L. B. (Eds.). (2009). Adolescent emotional development and the emergence of depressive disorders. New York: Cambridge University Press.
Amato, P. R., & Keith, B. (1991). Parental divorce and the well-being of children: A meta-analysis. Psychological Bulletin, 110, 26–46.
Anderson, C. A. (1999). Attributional style, depression, and loneliness: A cross-cultural comparison of American and Chinese students. Personality and Social Psychology Bulletin, 25, 482–499.
Anderson, E. R., & Mayes, L. C. (2010). Race/ethnicity and internalizing disorders in youth: A review. Clinical Psychology Review, 30, 338–348.
Asendorpf, J. B., & van Aken, M. A. G. (2003). Personality-relationship transaction in adolescence: Core versus surface personality characteristics. Journal of Personality, 71, 629–666.
Bellmore, A. D., Witkow, M. R., Graham, S., & Juvonen, J. (2004). Beyond the individual: The impact of ethnic context and classroom behavioral norms on victims’ adjustment. Developmental Psychology, 40, 1159–1172.
Blatt, S. J. (1990). Interpersonal relatedness and self-definition: Two personality configurations and their implications for psychopathology and psychotherapy. In J. Singer (Ed.), Repression: Defense mechanisms and personality (pp. 299–335). Chicago: University of Chicago Press.
Bolger, N., & Zuckerman, A. (1995). A framework for studying personality in the stress process. Journal of Personality and Social Psychology, 69, 890–902.
Bollen, K. A. (1989). Structural equations with latent variables. New York: Wiley.
Borys, S., & Perlman, D. (1985). Gender differences in loneliness. Personality and Social Psychology Bulletin, 11, 63–74.
Buhrmester, D. (1990). Intimacy of friendship, interpersonal competence, and adjustment during preadolescence and adolescence. Child Development, 61, 1101–1111.
Cacioppo, J. T., Hawkley, L. C., Ernst, J. M., Burleson, M., Berntson, G. G., Nouriani, B., et al. (2006a). Loneliness within a nomological net: An evolutionary perspective. Journal of Research in Personality, 40, 1054–1085.
Cacioppo, J. T., Hughes, M. E., Waite, L. J., Hawkley, L. C., & Thisted, R. A. (2006b). Loneliness as a specific risk factor for depressive symptoms: Cross-sectional and longitudinal analyses. Psychology and Aging, 21, 140–151.
Cacioppo, J. T., Hawkley, L. C., & Thisted, R. A. (2010). Perceived social isolation makes me sad: 5-year cross-lagged analyses of loneliness and depressive symptomatology in the Chicago health, aging, and social relations study. Psychology and Aging, 25, 453–463.
Caspi, A., Roberts, B. W., & Shiner, R. L. (2005). Personality development: Stability and change. Annual Review of Psychology, 56, 453–484.
Clark, L. A., Watson, D., & Mineka, S. (1994). Temperament, personality, and the mood and anxiety disorders. Journal of Abnormal Psychology, 103, 103–116.
Cole, D. A., Martin, J. M., & Powers, B. (1997). A competency-based model of child depression: A longitudinal study of peer, parent, teacher, and self-evaluations. Journal of Child Psychology and Psychiatry and Allied Disciplines, 38, 505–514.
Costa, P. T., Jr., & McCrae, R. R. (1992). Revised NEO personality inventory and five factor inventory professional manual. Odessa, FL: Psychological Assessment Resources.
Costa, P. T., Jr., & McCrae, R. R. (1995). Domains and facets: Hierarchical personality assessment using the revised NEO personality inventory. Journal of Personality Assessment, 64, 21–50.
Coyne, J. C. (1976). Toward an interactional description of depression. Psychiatry: Journal for the Study of Interpersonal Processes, 39, 28–40.
Erikson, E. (1968). Identity, youth and crisis. New York: Norton.
Eysenck, M. (1987). Trait theories of anxiety. In J. Strelau & H. J. Eysenck (Eds.), Personality dimensions and arousal (pp. 79–97). New York: Plenum Press.
Goldberg, L. R. (1992). The development of markers for the big-five factor structure. Psychological Assessment, 4, 26–42.
Goossens, L. (2006). Affect, emotion, and lonelinesss in adolescence. In S. Jackson & L. Goossens (Eds.), Handbook of adolescent development (pp. 51–70). Hove, UK: Psychology Press.
Goossens, L., Lasgaard, M., Luyckx, K., Vanhalst, J., Mathias, S., & Masy, E. (2009). Loneliness and solitude in adolescence: A confirmatory factor analysis of alternative models. Personality and Individual Differences, 47, 890–894.
Gray, J. A. (1981). A critique of Eysenck’s theory of personality. In H. J. Eysenck (Ed.), A model for personality (pp. 246–276). New York: Springer.
Hankin, B. L., Abramson, L. Y., Moffitt, T. E., Silva, P. A., McGee, R., & Angell, K. E. (1998). Development of depression from preadolescence to young adulthood: Emerging gender differences in a 10-year longitudinal study. Journal of Abnormal Psychology, 107, 128–140.
Harakeh, Z., Scholte, R. H. J., de Vries, H., & Engels, R. C. M. E. (2005). Parental rules and communication: Their association with adolescent smoking. Addiction, 100, 862–870.
Hawker, D. S. J., & Boulton, M. J. (2000). Twenty years’ research on peer victimization and psychosocial maladjustment: A meta-analytic review of cross-sectional studies. Journal of Child Psychology and Psychiatry and Allied Disciplines, 41, 441–455.
Heinrich, L. A., & Gullone, E. (2006). The clinical significance of loneliness: A literature review. Clinical Psychology Review, 26, 695–718.
Joiner, T. E. (2000). Depression’s vicious scree: Self-propagating and erosive processes in depression chronicity. Clinical Psychology: Science and Practice, 7, 203–218.
Joiner, T. E., Alfano, M. S., & Metalsky, G. I. (1992). When depression breeds contempt: Reassurance seeking, self-esteem, and rejection of depressed college students by their roommates. Journal of Abnormal Psychology, 101, 165–173.
Joiner, T. E., Katz, J., & Lew, A. (1999). Harbingers of depressotypic reassurance seeking: Negative life events, increased anxiety, and decreased self-esteem. Personality and Social Psychology Bulletin, 25, 630–637.
Kandel, D. B., & Davies, M. (1982). Epidemiology of depressive mood in adolescents: An empirical study. Archives of General Psychiatry, 39, 1205–1212.
Klimstra, T. A., Hale, W. W., Raaijmakers, A. W., Branje, S. J. T., & Meeus, W. H. J. (2009). Maturation of personality in adolescence. Journal of Personality and Social Psychology, 96, 898–912.
Klimstra, T. A., Akse, J., Hale, W. W., Raaijmakers, Q. A. W., & Meeus, W. N. J. (2010). Longitudinal associations between personality traits and problem behavior symptoms in adolescence. Journal of Research in Personality, 44, 273–284.
Kline, R. B. (2005). Principles and practices of structural equation modeling (2nd ed.). New York: Guilford Press.
Koenig, L. J., Isaacs, A. M., & Schwartz, J. A. J. (1994). Sex-differences in adolescent depression and loneliness: Why are boys lonelier if girls are more depressed? Journal of Research in Personality, 28, 27–43.
Kotov, R., Gamez, W., Schmidt, F., & Watson, D. (2010). Linking “big” personality traits to anxiety, depressive, and substance use disorders: A meta-analysis. Psychological Bulletin, 136, 768–821.
Lamers, F., van Oppen, P., Comijs, H. C., Smit, J. H., Spinhoven, P., van Balkom, A. J. L. M., et al. (2011). Comorbidity patterns of anxiety and depressive disorders in a large cohort study: The Netherlands study of depression and anxiety (NESDA). Journal of Clinical Psychiatry, 72, 341–348.
Larsen, R. J., & Ketelaar, T. (1991). Personality and susceptibility to positive and negative emotional states. Journal of Personality and Social Psychology, 61, 132–140.
Larson, R., & Richards, M. H. (1991). Daily companionship in late childhood and early adolescence: Changing developmental contexts. Child Development, 62, 284–300.
Lasgaard, M., Goossens, L., & Elklit, A. (2011). Loneliness, depressive symptomatology, and suicide ideation in adolescence: Cross-sectional and longitudinal analyses. Journal of Abnormal Child Psychology, 39, 137–150.
Lewinsohn, P. M. (1974). A behavioral approach to depression. In R. J. Friendman & M. Katz (Eds.), The psychology of depression: Contemporary theory and research (pp. 157–178). Washington, DC: Winston-Wiley.
Little, R. J. A. (1988). A test of missing completely at random for multivariate data with missing values. Journal of the American Statistical Association, 83, 1198–1202.
Mahon, N. E., Yarcheski, A., Yarcheski, T. J., Cannella, B. L., & Hanks, M. M. (2006). A meta-analytic study of predictors for loneliness during adolescence. Nursing Research, 55, 308–315.
Marcoen, A., Goossens, L., & Caes, P. (1987). Loneliness in pre- through late adolescence: Exploring the contributions of a multidimensional approach. Journal of Youth and Adolescence, 16, 561–577.
Masi, C. M., Chen, H. Y., Hawkley, L. C., & Cacioppo, J. T. (2011). A meta-analysis of interventions to reduce loneliness. Personality and Social Psychology Review, 15, 219–266.
McCrae, R. R., & Costa, P. T. (1987). Validation of the 5-factor model of personality across instruments and observers. Journal of Personality and Social Psychology, 52, 81–90.
McCrae, R. R., & Costa, P. T. (1999). A five-factor theory of personality. In L. Pervin & O. P. John (Eds.), Handbook of personality: Theory and research (2nd ed., pp. 139–153). New York: Guilford Press.
Muthén, L. K., & Muthén, B. O. (2002). Mplus user’s guide. Los Angeles: Muthén & Muthén.
Nolen-Hoeksema, S., & Girgus, J. S. (1994). The emergence of gender differences in depression during adolescence. Psychological Bulletin, 115, 424–443.
Perry, G. R. (1990). Loneliness and coping among tertiary-level adult cancer patients in the home. Cancer Nursing, 13, 293–302.
Quevedo, R. J. M., & Abella, M. C. (2011). Well-being and personality: Facet-level analyses. Personality and Individual Differences, 50, 206–211.
Rose, A. J., & Rudolph, K. D. (2006). A review of sex differences in peer relationship processes: Potential trade-offs for the emotional and behavioral development of girls and boys. Psychological Bulletin, 132, 98–131.
Steiger, J. H., Shapiro, A., & Browne, M. W. (1985). On the multivariate asymptotic distribution of sequential Chi-square statistics. Psychometrika, 50, 253–264.
Stokes, J. P. (1985). The relation of social network and individual difference variables to loneliness. Journal of Personality and Social Psychology, 48, 981–990.
Tackett, J. L. (2006). Evaluating models of the personality-psychopathology relationship in children and adolescents. Clinical psychology Review, 26, 584–599.
van der Vorst, H., Engels, R. C. M. E., Meeus, W., Dekovic, M., & Van Leeuwe, J. (2005). The role of alcohol-specific socialization in adolescents’ drinking behaviour. Addiction, 100, 1464–1476.
van der Vorst, H., Engels, R. C. M. E., Dekovic, M., Meeus, W., & Vermulst, A. A. (2007). Alcohol-specific rules, personality and adolescents’ alcohol use: A longitudinal person-environment study. Addiction, 102, 1064–1075.
van Roekel, E., Engels, R. C. M. E., Verhagen, M., Goossens, L., & Scholte, R. H. J. (2011). Parental depressive feelings, parental support, and the serotonin transporter gene as predictors of adolescent depressive feelings: A latent growth curve analysis. Journal of Youth and Adolescence, 40, 453–462.
Vanhalst, J., Goossens, L., & Luyckx, K. (2010). Loneliness and depressed mood in adolescence: Longitudinal associations and the mediating and moderating effects of rumination: In L. Goossens (chair), Loneliness and depressed mood in adolescence: Longitudinal trends, childhood predictors, and gene-environment interactions. Symposium conducted at the 13th biennial meeting of the Society for Research on Adolescence (SRA), Philadelphia, US.
Vanhalst, J., Luyckx, K., Raes, F., & Goossens, L. (in press). Loneliness and depressive symptoms: The mediating and moderating role of uncontrollable ruminative thoughts. Journal of Psychology: Interdisciplinary and Applied.
Vermulst, A. A., & Gerris, J. R. M. (2005). QBF: Quick big five persoonlijkheidstest handleiding [Quick Big Five personality test manual]. Leeuwarden, The Netherlands: LDC Publications.
Weeks, D. G., Michela, J. L., Peplau, L. A., & Bragg, M. E. (1980). Relation between loneliness and depression: A structural equation analysis. Journal of Personality and Social Psychology, 39, 1238–1244.
Wood, D., Harms, P., & Vazire, S. (2010). Perceiver effects as projective tests: What your perceptions of others say about you. Journal of Personality and Social Psychology, 99, 174–190.
Acknowledgment
Funding was provided by Grant OT/08/013 of the Research Council, Catholic University of Leuven. The authors wish to thank Eveline Teppers and Prof. Dr. Bart Soenens for their advice on earlier versions of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Vanhalst, J., Klimstra, T.A., Luyckx, K. et al. The Interplay of Loneliness and Depressive Symptoms Across Adolescence: Exploring the Role of Personality Traits. J Youth Adolescence 41, 776–787 (2012). https://doi.org/10.1007/s10964-011-9726-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10964-011-9726-7