
Abstract
This study uses data collected through the 2011 Miami-Dade Health Survey (n = 444) to test whether religious involvement is associated with three distinct control beliefs. Regression results suggest that people who exhibit high levels of religious involvement tend to report higher levels of the sense of control, self-control, and the health locus of control than respondents who exhibit low levels of religious involvement. Although this study suggests that religious involvement can promote perceptions of control over one’s own life, this pattern is apparently concentrated at the high end of the distribution for religious involvement, indicating a threshold effect.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Does religious involvement undermine or promote perceptions of control over one’s own life? Historically, scholars have speculated that religion undermines perceptions of control by socializing adherents to submit to higher powers (e.g., God) and to authoritative religious doctrines (Ellison and Burdette 2012; Mirowsky and Ross 2003; Wink et al. 2007). According to Mirowsky and Ross (2003: 200–201), “People can attribute the outcomes in their lives to luck, chance, family background, other people, God, and so on. All of these external attributions act as logical opposites of internal control: either I control my life or control rests elsewhere.” More recently, researchers have theorized that religious involvement can actually empower adherents by fostering supportive relationships with congregations and divine others. Ellison and Burdette (2012: 7) explain that “individuals often experience God as a partner, with whom they work in a collaborative fashion to resolve environmental stressors and manage negative emotions associated with personal problems.”
While both of these perspectives are at least theoretically viable, it is important to note that few empirical studies have formally tested the association between religious involvement and perceived control (Ellison and Burdette 2012). Therefore, the primary aim of this study is to test whether religious involvement is associated with higher or lower levels of three distinct control beliefs: the sense of control, self-control, and the health locus of control. In the pages that follow, we define the concept of religious involvement, distinguish among the control beliefs, and review previous studies of religious involvement and control beliefs. After describing the data and methods, we summarize the important results of our analyses. We end with a discussion of the implications and limitations of this work.
Theoretical Background
Key Concepts: Religious Involvement and Control Beliefs
Religious involvement, the focal independent variable in this study, is a complex and multidimensional construct (Ellison and Burdette 2012; Hill et al. 2011). According to Hill et al. (2011: 533), religious involvement refers to “observable feelings, beliefs, activities, and experiences in relation to spiritual, divine, or supernatural entities.” Religious involvement is a prevalent and powerful sociocultural force. For example, national estimates from a recent Poll (2013) show that a large percentage of US adults affiliate with religious groups (83 %) and rate religion as “very important” in their lives (56 %).
Although the control beliefs that represent the focal dependent variables in this study are related indicators of subjective alienation (Mirowsky and Ross 2003; Seeman 1983), it is important to recognize that they are treated as distinct in the empirical literature. According to Mirowsky and Ross (2003: 174), “The sense of personal control is a learned, generalized expectation that outcomes are contingent on one’s own choices and actions.” People with a high sense of control believe that they can exercise control over their lives and that they are personally responsible for the good and bad things that happen to them. People with a low sense of control believe that they are powerless over the course of their lives and that external forces direct their fate.
Health locus of control is a specific expression of the more generalized sense of control (Wallston et al. 1978). Wallston et al. (1978: 160) define the health locus of control as a “measure of people’s beliefs that their health is or is not determined by their behavior.” “Health internals” believe that they can control their own health and that their health outcomes are primarily driven by their own personal behavior. “Health externals” believe that their health is determined by external forces, including chance and powerful others.
Self-control is distinct from the general sense of control and the more specific health locus of control. It represents the ability to resist basic human drives. According to McCullough and Willoughby (2009: 72), self-control refers to “situations in which people engage in behaviors designed to counteract or override a prepotent response (e.g., a behavioral tendency, an emotion, or a motivation), such as assaulting someone who has angered them, resting after a hard day at work instead of painting the kitchen, or playing hooky instead of going to school.” They go on to explain that “when people exert self-control, they modify their response tendencies in a fashion that involves suppressing one goal so as to pursue another one that is judged to have greater long-term utility” (p. 72). While the sense of control and locus of control indicate beliefs concerning control over external outcomes in life, self-control assesses the normative self-regulation of internal drives.
As noted above, each of the three control beliefs is a conceptually related indicator of subjective alienation. Subjective alienation is a general concept that refers to the subjective perception of separation. All three control beliefs can be framed in this way (Mirowsky and Ross 2003; Seeman 1983). The sense of control indicates the degree to which the individual is separated from the general outcomes of life. The health locus of control indicates the degree to which the individual is separated from personal health-related outcomes. Finally, self-control indicates the degree to which the individual is separated from basic human drives. The important question is whether religious involvement contributes to or helps to overcome these various forms of subjective alienation. In the next section, we consider the empirical evidence linking religious involvement and each of the three control beliefs under study.
Previous Empirical Research
When considering the literature concerning religious involvement and perceptions of control, the strongest body of empirical work is in the area of the sense of control. Most of these studies indicate that religious involvement is positively associated with the sense of control (Ellison and Burdette 2012; Fiori et al. 2006; Hayward and Krause 2013; Krause and Van Tran 1989; Schieman 2008; Shrauger and Silverman 1971). This general pattern is consistent across measures of religiosity and the sense of control, and all but one of these studies (Shrauger and Silverman 1971) are based on data collected from probability samples of community-dwelling adults. With this in mind, it is important to note that research in the area of religious involvement and the sense of control is actually somewhat mixed. In fact, several studies report at least one null association between some measure of religious involvement and the sense of control (Ellison and Burdette 2012; Fiori et al. 2006; Krause and Van Tran 1989; Schieman 2008; Wink et al. 2007). There is even some evidence to suggest that religious involvement can be associated with higher levels of external control (Fiori et al. 2006) and lower levels of the sense of control (Ellison and Burdette 2012; Shaw and Krause 2001).
Several empirical studies have also examined the association between religious involvement and self-control. McCullough and Willoughby (2009) provide an excellent review of this literature. According to this review, most studies show that religious people tend to exhibit greater self-control than less religious people. This general pattern is consistent across measures of religiosity and self-control and methodologies (surveys and experiments). However, most of the empirical studies have been conducted by psychologists and are based on non-probability samples of college students. The review referenced one study conducted by sociologists (Welch et al. 2006), and our search of the literature confirmed this exception. In their analysis of data collected from a probability sample of adults living in Oklahoma City, Welch et al. (2006) found that personal religiosity (a multi-item index of religious beliefs and behaviors) was positively associated with behavioral self-control. This study is suggestive, but it is limited by the measurement of self-control. Welch et al. (2006) measure self-control with ten items, including behaviors related to drinking, smoking, and seatbelt use. This measurement strategy only indirectly assesses the perceived ability to resist basic human drives.
To the best of our knowledge, there is only one empirical study of the association between religious involvement and the general health locus of control (Levin and Schiller 1986). Using data collected from a non-probability sample of Appalachian adults, Levin and Schiller (1986) showed that church-affiliated adults were less likely to attribute their health outcomes to “chance” than those adults with no church affiliations. They also observed the highest internal health locus of control scores among Mormons, Episcopalians, and Catholics.
Current Explanations
Why do religious adults tend to believe that they can exercise control over their lives? A key theme in research concerning the sense of control is personal empowerment (Ellison and Burdette 2012; Schieman 2008). Specifically, religious adults are empowered by ties to supportive religious communities and divine relations. It is well established that religious adults tend to have more social support in their lives than their less religious counterparts (Hill et al. 2011; Rote et al. 2013). These social resources are likely to communicate to adherents that their lives are manageable because they are not alone. Divine relations with higher powers supplement ties within religious communities by viewing God as a partner or collaborator during difficult life conditions. Ellison and Burdette (2012: 7) explain that “The spirit of such coping approaches may be summed up in the New Testament passage ‘with Christ all things are possible’ or by the popular epigram ‘God is my co-pilot.’” Religious involvement might also contribute to the sense of control by promoting a sense of order in the world. Religious groups may accomplish this by imparting a divine plan and, by extension, a sense of meaning and purpose in life (Schieman 2008).
When explaining associations with the health locus of control, it is important to recognize that the body is often sanctified or imbued with religious significance (Hill et al. 2011). For example, many religious groups believe that the body is the “temple of the Holy Spirit.” Under the conditions of such meaning systems, controlling or maintaining one’s health becomes a matter of devotion. Religious groups support these efforts by socializing adherents through religious teachings that emphasize moderation and healthy living (e.g., biblical proscriptions against intoxication). For example, Levin and Schiller (1986: 26) attribute the high internal health locus of control scores among Mormons, Episcopalians, and Catholics to “heavily ritualized or behaviorally strict traditions.”
Theories concerning the association between religious involvement and self-control are the most compelling and well developed (Geyer and Baumeister 2005; McCullough and Willoughby 2009; Welch et al. 2006). First and foremost, religious adults are more apt to resist their basic human drives because religious groups provide sanctified moral codes or clear standards of right and wrong. These moral codes often carry with them the threat of guilt and shame, hell and damnation. As noted by Koenig (2009: 288), “Religious beliefs and practices provide guidelines for human behavior that reduce self-destructive tendencies and pathological forms of coping.” Religious adults are also motivated by processes related to social control (e.g., social sanctions within the religious community) and ritualized self-examination (e.g., through confession and prayer). Ultimately, scholars theorize that religious adults are better equipped to exercise self-control because they have well-developed “moral muscles” that have been conditioned through years of ritual adherence, moral socialization, and social control (Geyer and Baumeister 2005; McCullough and Willoughby 2009).
Hypotheses
Building on the conceptual and sampling limitations of previous research, the present study uses data collected from a probability sample of adults living in Miami-Dade County to examine the association between religious involvement and perceptions of control. Drawing from previous research and theory, we expect that religious involvement will be positively associated with the sense of control, the health locus of control, and self-control.
Data
The data for this study come from the 2011 Miami-Dade Health Survey (MDHS). The MDHS is based on a county-wide probability sample of 444 community-dwelling adults aged 18 and over residing in Miami-Dade County. Survey Sampling, Inc. generated the sample using a random-digit dialing design. The Office of Survey Research at the University of Texas at Austin executed the data collection process, which yielded a response rate of 60 %. The average computer-assisted telephone interview lasted approximately 45 min. The survey instrument was translated into Spanish using a back-translation procedure that included an English to Spanish translation by one translator, a Spanish to English translation by a second translator, and a comparison and reconciliation of translation discrepancies by a third translator. Surveys were administered by Spanish-speaking interviewers for respondents who were more comfortable answering in that language. The primary purpose of the MDHS is to examine the social life, health, and well-being of a unique and understudied population of adults living in Miami-Dade County. The data include detailed information concerning (1) the neighborhood environment, (2) psychosocial characteristics, (3) religious involvement, (4) immigration and acculturation, (5) race/ethnic identity and discrimination, (6) health behaviors, (7) physical health, (8) mental health, and (9) general sociodemographic characteristics.
Measures
Table 1 presents survey items and component loadings for religious involvement, the sense of control, self-control, and the health locus of control. Component loadings were estimated using principal components analysis, specifying a minimum eigenvalue of 1.00, with varimax rotation. All component loadings exceed 0.60.
Religious involvement is measured as the mean response to six items (α = 0.85). These items indicate several dimensions of religious involvement, including private religious involvement (item 1), public religious involvement (item 2), religious coping (items 3 and 4), spirituality (item 5), and religious salience (item 6). Response options for items 1 and 2 range from 0 (never) to 6 (more than once per day). Responses for items 3 and 4 range from 0 (never) to 4 (very often). Responses for items 5 and 6 range from 0 (strongly disagree) to 3 (strongly agree). To account for mixed question formats and response categories, each religious involvement item was standardized before indexing. Because preliminary analyses suggested the presence of threshold effects, the full distribution of the religious involvement index was divided into three groups to indicate high, moderate, and low levels of religious involvement. In subsequent multivariate analyses, low religious involvement serves as the reference category against which high and moderate levels are compared.
The sense of control is measured as the mean response to three items (α = 0.38) developed by Mirowsky and Ross (1991). These items indicate perceptions of control over good (items 7 and 8) and bad (item 9) conditions of life. Response categories for these items range from 0 (strongly agree) to 3 (strongly disagree). The item concerning responsibility for successes (item 8) was reverse coded so that higher index values indicate higher levels of personal control.
Self-control is measured as the mean response to two items (α = 0.52) developed by Grasmick et al. (1993). These items indicate two of the most prominent dimensions of self-control, including impulsivity (item 10) and risk-seeking (item 11). Response categories for these items range from 0 (strongly agree) to 3 (strongly disagree) so that higher index values indicate higher levels of self-control.
Health locus of control is measured as the mean response to two items (α = 0.59) developed by Wallston et al. (1978). These items (12 and 13) indicate a single dimension of the broader underlying concept—the internal health locus of control. Response categories for these items range from 0 (strongly disagree) to 3 (strongly agree) so that higher index values indicate higher levels of the health locus of control.
As suggested by previous studies of control beliefs (Hill et al. 2014; Ellison and Levin 1998; Mirowsky and Ross 2003), all models adjust for a range of background variables that may confound the association between religious involvement and perceptions of control. These variables include age (in years), gender (1 = female, 0 = male), race (dummy variables for non-Hispanic white, non-Hispanic black, Hispanic, and other race/ethnicity, with non-Hispanic white serving as the reference category), immigrant status (1 = immigrant, 0 = non-immigrant), language of interview (1 = Spanish, 0 = English), education (ordinal variable ranging from 0 = less than high school education to 3 = graduate level education), and household income (ordinal variable ranging from 0 = $5000–$10,000 to 9 = more than $125,000).
Statistical Procedures
Table 2 provides descriptive statistics for all study variables, including variable ranges, sample means, standard deviations, and alpha reliability estimates. In subsequent multivariate analyses, we employ ordinary least squares (OLS) regression to model the continuous control measures. Table 3 provides unstandardized and standardized OLS regression coefficients for all independent variables. Unstandardized OLS coefficients represent the estimated difference in the mean of Y for those who are one unit apart on X, controlling or holding constant all other predictors in the model. Standardized OLS coefficients represent the estimated standard deviation difference in Y for those who are one standard deviation apart on X, controlling for all other predictors in the model. Standardized OLS coefficients allow one to assess which variables in the regression model have the strongest effects on Y. In other words, which variables are associated with the biggest changes in Y per unit change in X?
Missing Data
We used multiple imputation by chained equations to replace missing values on all independent and dependent variables (White et al. 2011). Subsequent analyses are based on pooled estimates derived from 10 imputations.
Results
Descriptive Analyses
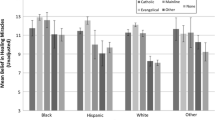
As shown in Table 2, nearly one-third of the respondents were classified into each of the low, moderate, and high religiosity groups. This distribution was established by design to capture any threshold effects. With respect to the dependent variables, the average respondent reported moderate to high levels of the sense of control, self-control, and health locus of control. On average, respondents were 57 years of age with at least some college experience. The majority (70 %) of respondents are women. In terms of race and ethnicity, the sample consists of non-Hispanic whites (31 %), Hispanic Americans (42 %), non-Hispanic blacks (14 %), and those of other races and ethnicities (13 %). Approximately half of the respondents are immigrants, and nearly one-third of the sample was interviewed in Spanish.
Multivariate Analyses
In Table 3, the regression estimates indicate that respondents in the high religious involvement group tend to report higher levels of the sense of control, self-control, and the health locus of control than respondents in the low religious involvement group, net of all background variables. Respondents in the moderate religious involvement group are not statistically different from respondents in the low religious involvement group. In other words, perceptions of control are comparable for respondents in the moderate and low religious involvement groups. Taken together, these results confirm a threshold effect. Religious adults only exhibit greater perceptions of control at the high end of the distribution for religious involvement.
An examination of standardized regression coefficients suggests that religious involvement is among the stronger correlates of control perceptions. In the sense of control regression, the magnitude of the standardized regression coefficient for high religious involvement is comparable to or greater than the standardized coefficients for black race and age, but noticeably smaller than the standardized coefficients for education and Spanish interview. In the self-control regression, the standardized coefficient for high religious involvement is larger than the standardized coefficients for age and education, but clearly smaller than the standardized coefficient for gender. High religious involvement is the only statistically significant predictor of the health locus of control.
Although we are not primarily concerned with background variable associations, we will briefly mention a few notable patterns. First, older respondents and respondents with more advanced degrees tend to report higher levels of the sense of control and self-control than their younger and lesser educated counterparts. Second, while non-Hispanic black respondents and respondents who completed the interview in Spanish tend to report lower levels of the sense of control, Hispanic respondents tend to report higher levels. Finally, women tend to report higher levels of self-control than men.
Discussion
We began this study by asking whether religious involvement undermines or promotes perceptions of control over one’s own life. Building on a limited body of community-based empirical work, this study used data collected from a probability sample of Miami-Dade adults to test whether religious involvement is associated with three distinct control beliefs: the sense of control, self-control, and the health locus of control.
Results obtained from a series of ordinary least squares regression models suggest that people who exhibit high levels of religious involvement tend to report higher levels of the sense of control, self-control, and the health locus of control than respondents who exhibit low levels of religious involvement. Perceptions of control are comparable for respondents who exhibit moderate and low levels of religious involvement. Although this study suggests that religious involvement can promote perceptions of control over one’s own life, this pattern is apparently concentrated at the high end of the distribution for religious involvement. Generally speaking, these results confirm previous studies of the sense of control (Ellison and Burdette 2012; Fiori et al. 2006; Hayward and Krause 2013; Krause and Van Tran 1989; Schieman 2008; Shrauger and Silverman 1971), self-control (McCullough and Willoughby 2009; Welch et al. 2006), and the health locus of control (Levin and Schiller 1986). To the best of our knowledge, this study is the first to demonstrate a threshold effect for the association between religious involvement and perceptions of control.
The results described in this study should be considered in the context of several notable limitations. First and foremost, all analyses are based on cross-sectional data. As a result, it is difficult to determine the direction of the relationship between religious involvement and perceptions of control. Although most studies seem to suggest that religious involvement can contribute to higher perceptions of control, it is also reasonable to speculate that adults with such perceptions might be selected into religious institutions. Although previous experimental research in the area of self-control suggests that this alternative model is not a serious concern (McCullough and Willoughby 2009), additional experimental and longitudinal research is needed to better establish the direction of the associations for the sense of control and the health locus of control.
The current study is also limited in terms of the measurement of control beliefs. While the sense of control is measured with three items, self-control and the health locus of control are measured with two items. Although results obtained from an exploratory factor analysis confirm that these items are sound indicators, reliability is rather low due to the small number of items. Such low reliability suggests that any observed associations are likely to be conservative. The conservative nature of this analysis is probably compounded by the small sample size and lower statistical power.
The final key limitation of the current study is generalizability. We have noted that most previous studies of religious involvement and perceptions of control are limited to data collected from non-probability samples of college students. The use of data collected from a probability sample of Miami-Dade adults clearly advances this body of work, but we cannot overstate the external validity of the data. Additional research with data collected from national probability samples or other regional probability samples is needed to confirm our results.
Conclusion
Despite these limitations, we are confident in the general finding that religious involvement helps to overcome various forms of subjective alienation. Assuming this general pattern is periodically replicated in subsequent research, we will eventually need to explain these patterns. If religious involvement promotes perceptions of control, why does it? To our knowledge, no empirical studies have addressed this fundamental question. It is also important to consider whether the effects of religious involvement are stronger or weaker for theoretically relevant subgroups. There is some evidence to suggest that religious involvement may be more strongly related to the sense of control for women and older adults (Fiori et al. 2006). Additional work is needed to confirm these patterns in self-control and the health locus of control. Testing variations according to other social statuses (e.g., social class and race/ethnicity) would also further our understanding. Lastly, it is important to at least consider the possibility that certain negative aspects of religious involvement (e.g., religious doubts and religious struggles) might actually undermine perceptions of control (Exline 2002; Pargament 2002; Wink et al. 2007). Research along these lines would add balance to a literature that seems to overemphasize the beneficial features of religious involvement.
References
Ellison, C. G., & Burdette, A. M. (2012). Religion and the sense of control among US adults. Sociology of Religion, 73, 1–22.
Ellison, C. G., & Levin, J. S. (1998). The religion-health connection: Evidence, theory, and future directions. Health Education & Behavior, 25, 700–720.
Exline, J. J. (2002). Stumbling blocks on the religious road: Fractured relationships, nagging vices, and the inner struggle to believe. Psychological Inquiry, 13, 182–189.
Fiori, K. L., Brown, E. E., Cortina, K. S., & Antonucci, T. C. (2006). Locus of control as a mediator of the relationship between religiosity and life satisfaction: Age, race, and gender differences. Mental Health, Religion and Culture, 9, 239–263.
Geyer, A., & Baumeister, R. (2005). Religion, morality, and self-control. In R. F. Paloutzian & C. L. Park (Eds.), Handbook of the psychology of religion and spirituality (pp. 412–432). New York: Guilford Press.
Grasmick, H. G., Tittle, C. R., Bursik, R. J., & Arneklev, B. J. (1993). Testing the core empirical implications of Gottfredson and Hirschi’s general theory of crime. Journal of Research in Crime and Delinquency, 30, 5–29.
Hayward, R. D., & Krause, N. (2013). Trajectories of late-life change in God-mediated control. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 68, 49–58.
Hill, T., Burdette, A., & Idler, E. (2011). Religious involvement, health status, and mortality risk. In R. Settersten & J. Angel (Eds.), Handbook of sociology of aging (pp. 533–546). New York: Springer.
Hill, T. D., Cook, H. H., & Whitfield, K. E. (2014). Race and ethnic variations in the education-control-distress model. Social Science Quarterly, 95, 269–285.
Koenig, H. G. (2009). Research on religion, spirituality, and mental health: a review. Canadian Journal of Psychiatry, 54, 283–291.
Krause, N., & Van Tran, T. (1989). Stress and religious involvement among older blacks. Journal of Gerontology, 44, S4–S13.
Levin, J. S., & Schiller, P. L. (1986). Religion and the multidimensional health locus of control scales. Psychological Reports, 59, 26.
McCullough, M. E., & Willoughby, B. L. (2009). Religion, self-regulation, and self-control: Associations, explanations, and implications. Psychological Bulletin, 135, 69.
Mirowsky, J., & Ross, C. E. (1991). Eliminating defense and agreement bias from measures of the sense of control: A 2 × 2 index. Social Psychology Quarterly, 54, 127–145.
Mirowsky, J., & Ross, C. E. (2003). Social causes of psychological distress. New Jersey: Transaction Publishers.
Pargament, K. I. (2002). The bitter and the sweet: An evaluation of the costs and benefits of religiousness. Psychological Inquiry, 13, 168–181.
Poll, G. (2013). Graph illustration of results from the 2012 Gallup Poll on religion. Retrieved December 15, 2013, from http://www.gallup.com/poll/1690/Religion.aspx.
Rote, S., Hill, T. D., & Ellison, C. G. (2013). Religious attendance and loneliness in later life. The Gerontologist, 53, 39–50.
Schieman, S. (2008). The religious role and the sense of personal control. Sociology of Religion, 69, 273–296.
Seeman, M. (1983). Alienation motifs in contemporary theorizing: The hidden continuity of the classic themes. Social Psychology Quarterly, 46, 171–184.
Shaw, B. A., & Krause, N. (2001). Exploring race variations in aging and personal control. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 56, S119–S124.
Shrauger, J. S., & Silverman, R. E. (1971). The relationship of religious background and participation to locus of control. Journal for the Scientific Study of Religion, 10, 11–16.
Wallston, K. A., Wallston, B. S., & DeVellis, R. (1978). Development of the multidimensional health locus of control (MHLC) scales. Health Education & Behavior, 6, 160–170.
Welch, M. R., Tittle, C. R., & Grasmick, H. G. (2006). Christian religiosity, self-control and social conformity. Social Forces, 84, 1605–1623.
White, I. R., Royston, P., & Wood, A. M. (2011). Multiple imputation using chained equations: Issues and guidance for practice. Statistics in Medicine, 30, 377–399.
Wink, P., Dillon, M., & Prettyman, A. (2007). Religion as moderator of the sense of control–health connection: Gender differences. Journal of Religion, Spirituality & Aging, 19, 21–41.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Pascoe, A.E., Hill, T.D., Mossakowski, K.N. et al. Religious Involvement and Perceptions of Control: Evidence from the Miami-Dade Health Survey. J Relig Health 55, 862–873 (2016). https://doi.org/10.1007/s10943-015-0081-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10943-015-0081-y