
Abstract
The study of religious orientation thus far has neglected the influence of race/ethnicity as well as all four religious orientations (intrinsic, extrinsic, pro-religious and nonreligious) in explaining differences in both physical and psychological health. A representative sample of 250 Hispanics and 236 non-Hispanic Whites in Utah was drawn and analysed for differences in health (self-rated health, life satisfaction, exercise) according to race/ethnicity, religious orientation and religious attendance. Responses to the Religious Orientation Scale differed significantly by race/ethnicity, indicating that future studies of religious orientation should take cultural context into account. For both Whites and Hispanics, pro-religious individuals reported the highest life satisfaction scores, which highlight the utility of employing the fourfold religious orientation typology.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Religion is an important aspect in the lives of most Americans, and it has been estimated that 92% of Americans profess a belief in God (Pew Forum on Religion and Public Life 2008). Despite the large percentage of Americans who believe in God, the way in which religion influences individuals varies by denomination, culture, ethnicity and location. Analysing how these differences ultimately influence health has been the topic of numerous research articles.
Of all the many facets of religion, one of the most widely studied is religious orientation. Religious orientation and its linkages to health, especially mental health, is a field with a history and an established literature. Most studies that analyse connections between religious orientation and health can trace their theoretical foundations back to the work of Gordon Allport (1950). Allport’s early work focused on understanding why religious individuals were found to be relatively more prejudiced. He postulated that there were two types of religion, mature and immature religion, later classified as intrinsic and extrinsic religion, respectively (Allport 1963). He classified extrinsic individuals as those who use their religion to obtain emotional comfort, social support or enhance one’s social network for personal gain. Intrinsic individuals were classified as those whose religion was an end in itself. These individuals were religious for the purposes of developing a deeper personal relationship with God. Allport developed a metric for measuring religious orientation, the Religious Orientation Scale (ROS), and tested his theory of religious orientation (Allport and Ross 1967). He found that intrinsic individuals were less prejudiced than average, and extrinsic individuals were more prejudiced than average.
Since the publication of Allport’s work and the development of the ROS, a myriad of research has come forth seeking to understand the relationship between religious orientation, or religious motivation, and health. Today, it is one of the most widely used metrics in the scientific study of religion. A review published in the 1980s found that, by that time, over 70 studies had been published which investigated linkages between religious orientation and either physical or mental health (Donahue 1985). Today, a search on Medline querying the phrase “religious orientation” yields over 300 peer-reviewed articles.
A criticism that has been associated with the ROS is its usage as a bipolar scale with intrinsic orientation on one end and extrinsic orientation on the other (Hood 1970; Kirkpatrick and Hood 1990; Masters 1991; Kirkpatrick and Hood 1991; Cohen et al. 2005). This approach can fail to account for the combinations of intrinsic and extrinsic motivation and their novelty in explaining differences in health within a population. One way to avoid this problem is to use one of the modified versions of Allport’s original instrument. Over time, the ROS has been modified for conceptual clarity and greater validity across ages and the religious orientations themselves (Gorusch and Venable 1983; Gorsuch and McPherson 1989). These modifications yield the intrinsic and extrinsic scales as separate, uncorrelated variables and introduce two classifications of religious orientation, pro-religious (high intrinsic, high extrinsic) and nonreligious (low intrinsic, low extrinsic), which have been discussed in previous research (Hood 1970, 1978). This approach, which incorporates all four religious orientations, is known as the fourfold typology.
While most studies that utilize the ROS examine psychological health and well-being, there are some studies that have used the ROS to study linkages between religious orientation and physical health (Masters et al. 2004; Masters et al. 2005; Powell et al. 2003; McCullough et al. 2000; Hart et al. 2004; Ellison and Levin 1998; Seybold and Hill 2001). Most of these are associated with cardiovascular health and find intrinsic orientation to be significantly associated with reductions in blood pressure and cardiovascular disease. None of them, however, include an analysis of the pro-religious and nonreligious orientations. Even among studies of mental health, analysis of the fourfold typology is typically lacking, dated or of a small sample size (Hood 1970; Kirkpatrick and Hood 1990; Levin et al. 1998; Meyer et al. 1992). Studies that incorporate pro-religious and nonreligious orientations will make a contribution to the religious orientation literature.
Although many studies have explored connections between religious orientation and health, few have done so within a cultural context. Of the handful of studies that have been published that analyze religious orientation in other cultures, most of these have been performed among African Americans (Colbert et al. 2009; Turner-Musa and Wilson 2006; Sanchez and Carter 2005; Maltby and Day 2003), although some comparisons between African Americans and White populations do exist (Nelson 1989). None of them analyze the fourfold typology, but instead look only at intrinsic and extrinsic orientations. Rarely is race used as an explanatory variable in the analysis of religious orientation.
Interest in Hispanic populations has begun to arise in the literature, but it still remains heavily understudied. A recent study analysed the relationship between religiosity/religious orientation and political alignment among Whites, Blacks and Hispanics and found much weaker associations for Blacks and Hispanics than for Whites (Cohen et al. 2009), underscoring the need for studies to explore religious orientation within the context of race/ethnicity. This study only analysed intrinsic religiousness, however, and did not include dimensions of health. Another study found modest effects between religious importance and reduced depression for Hispanics in California but called for more research that explores the relationship between religious involvement and health of Hispanics, the largest minority group in the United States (Ellison et al. 2009). While this research did not study religious orientation, it did discuss that studies of Hispanic religiosity would be even more valuable if they were able to make some comparisons among religious preferences. In relation to physical health, an 8-year follow-up study of Mexican Americans found that weekly religious attendance was associated with reduced mortality (Hill et al. 2005). It should be noted, however, that only looking at religious attendance can be misleading due to selection bias in that it is easier for healthy individuals to attend religious services than those who have poor health. Incorporating additional measures of religiosity, therefore, can strengthen the analyses of the influence of religious involvement on health (George et al. 2002).
Research that can identify how connections between religious orientation and health compare according to race/ethnicity will enhance understanding of the relationship between religion and health. While several studies have validated the ROS with international populations, including Taiwanese students, Thai Buddhists and Iranian Muslims (Chen and Liu 2009; Tapanya et al. 1997; Watson et al. 2002), few studies exist that compare measures of religiosity between Hispanics and other racial/ethnic groups in the United States, especially in regard to the fourfold typology of religious orientation. Testing how the scales of intrinsic and extrinsic religion correlate with the health of Hispanics as well as White non-Protestant populations would therefore be a contribution to the literature.
The purposes of this study were to compare responses of religious preference and religious orientation (intrinsic, extrinsic, pro-religious, nonreligious) in a sample of Hispanics and non-Hispanic Whites and then to compare how these responses correlate with the measures of both physical and psychological health.
Methods
Sample
A sample of 250 Hispanic and 250 non-Hispanic residents of Utah were obtained through random digit dialing (RDD). The Hispanic population was over sampled to ensure an equal number of Hispanics and non-Hispanics. The RDD sample of both Hispanic and non-Hispanic groups was purchased from STS (Scientific Telephone Sampling). The sample was purchased targeting the listed numbers for people with Hispanic surnames. The sample was representative of the population of the state of Utah. RDD is a sampling method in which phone numbers are generated using a known area code for a known geography. The sample generated was compared against a list of known bad/disconnected numbers to ensure that the sample was as accurate as possible.
Of the non-Hispanic respondents, 236 were Whites, 2 were Blacks and 12 listed their race/ethnicity as “other.” Analyses are based on 236 White respondents and 250 Hispanic respondents. The response rate was 59%. Institutional Review Board approval was obtained in January 2010, from Brigham Young University.
Instrument
The questionnaire included items on religious orientation, health behaviour and mental health. Questions concerning religious orientation were taken from Gorsuch and McPherson’s (1989) fourfold typology metric for measuring religious orientation. This metric contains 14 questions: eight of them pertain to intrinsic religious orientation, and six of them pertain to extrinsic religious orientation. Each question is asked on a five-point Likert scale (“strongly agree,” “tend to agree,” “neutral,” “tend to disagree,” and “strongly disagree”). Consequently, the intrinsic scale ranges from 8–40, and the extrinsic scale ranges from 6–30. The classifications under this typology are the following: (1) Intrinsically Religious, (2) Extrinsically Religious, (3) Pro-religious and (4) Nonreligious. According to the metric, Intrinsically Religious individuals were classified as those whose intrinsic scale scores were equal to or above the intrinsic scale’s neutral score (24) and whose extrinsic scale scores were below the extrinsic scale’s neutral score (18). Extrinsically Religious individuals were classified as those whose extrinsic scale scores were equal to or above the scale’s neutral score and whose intrinsic scale scores were below the scale’s neutral score. Pro-religious individuals were classified as those whose extrinsic and intrinsic scores were equal to or above each scale’s neutral score. Nonreligious individuals were classified as those whose intrinsic and extrinsic scores fell beneath the neutral score on both metrics and therefore did not claim strong religious motivations, although they still claimed a religious preference. Respondents who indicated that they did not have a religious preference were not asked questions regarding religious orientation.
Survey questions regarding physical health behaviours included exercise, tobacco and alcohol consumption, and hours of sleep per night. Respondents were also asked to self-rate their health as “excellent,” “very good,” “good,” “fair,” or “poor,” and these responses were given the values of 100, 75, 50, 25 and 0, respectively. The Satisfaction with Life Scale (SWLS), developed by Diener et al. (1985), was also included in the survey. This five-question metric was included because it has been related to psychological well-being across a number of studies. Each question in the SWLS has a seven-point scale, and responses from the five questions were summed, creating a total SWLS scale that ranges from 5–35. The combination of using tested instruments such as the fourfold typology and the Satisfaction with Life Scale was made in order to reduce instrument bias in measuring the correlates between religious orientation and the overall health of the sample.
Variables Considered
Dependent variables: religious orientation (fourfold typology as well as raw intrinsic and extrinsic scores), life satisfaction, self-rated overall health and minutes of exercise per week.
Independent variables: age, gender, religious orientation, religious preference, religious attendance, marital status, cigarette use and life satisfaction.
Statistical Techniques
Initial analyses included testing for distributional differences in both demographics and religious orientation responses between Whites and Hispanics. We then tested for correlates of intrinsic and extrinsic scale scores. Respondents were grouped according to religious orientation (intrinsic, extrinsic, pro-religious and nonreligious), and we evaluated whether mediating variables were involved with religious orientation. The association between religious behaviour (church attendance and religious orientation) and both physical and mental health was also explored.
General linear and chi-square models were estimated. Analysis of covariance was also used to evaluate and compare means among groups, adjusting for age and gender. Analyses were performed using the Statistical Analysis System (SAS) software, version 9.2 (SAS Institute Inc., Cary, NC, USA 2007).
Results
Summary statistics for the sample are presented in Table 1. White respondents were predominantly women and tended to be older than Hispanic respondents, which were predominantly men. Both White and Hispanic respondents tended to be married, the level of education in Whites was higher than that of Hispanics, and the level of smoking was higher in Hispanics. Among Whites, the most common religious preference was Latter-day Saint, followed by Roman Catholic, “other” religious preference, no religious preference and Protestant. For Hispanics, Roman Catholic was most common, followed by Latter-day Saint, no religious preference, “other” religious preference and Protestant. Whites were more likely than Hispanics to attend religious services weekly. Whites were more likely to report excellent or very good health, and Hispanics were more likely to report good or fair health. Both groups were almost equally likely to report poor health. Significant differences between the two groups existed for gender, age, marital status, education, smoking, religious preference, religious attendance and self-rated health. All subsequent analyses controlled for age and gender and tested for possible mediating effects that involved marital status, education, smoking and religious preference. There were no significant differences between Whites and Hispanics with respect to alcohol drinking, hours of physical activity per week and BMI.
The distribution, mean and standard deviation for each of the questions on the 14-item Religious Orientation Scale are presented in Table 2. Responses tended towards the more religious end of the scales. Significant differences in mean scores were found for three questions that pertain to the intrinsic scale (questions 3, 10 and 14) and four questions that pertain to the extrinsic scale (questions 6, 9, 11 and 13). Additional analysis (data not shown) found that adding marital status to the model significantly decreased the mean score for question 3 in both Whites and Hispanics. Adding the smoking variable significantly decreased the mean score in question 3 for both Whites and Hispanics and significantly decreased mean scores in question 11 among Hispanics while increasing them among Whites. The education variable increased Hispanic mean scores in questions 3, 10 and 14 while decreasing the mean score in question 11. It had the opposite effect on the White samples, increasing the mean score in question 11 while decreasing mean scores in questions 3, 10 and 14. Religion increased the Hispanic mean score in question 3 while it decreased mean scores in questions 10 and 14. It decreased White mean scores in questions 3, 10 and 14.
The distribution, mean and standard deviation for each of the questions on the 5-item Satisfaction with Life Scale are presented in Table 3. Responses tended towards the more satisfied end of the scale. Significant differences in mean scores were found for only one question (question 4), for which Hispanics reported more satisfaction than Whites.
Initial assessment of the mean scores on the intrinsic and extrinsic scales of the Religious Orientation Scale identified a significant interaction effect between race/ethnicity and religious preference, education, religious attendance and self-rated health. Consequently, the scores from these scales were stratified accordingly (Table 4). For Whites, Latter-day Saints had the highest intrinsic scores, followed by Roman Catholics, Protestants and members of other faiths. On the extrinsic scale, Latter-day Saints also had the highest scores, followed by members of “other” faiths, Protestants and Roman Catholics. For Hispanics, Latter-day Saints had the highest intrinsic scores, followed by Protestants, members of other faiths and Roman Catholics. The mean extrinsic scores did not differ significantly by religious preference.
For both Whites and Hispanics, more education was associated with higher intrinsic scores and lower extrinsic scale scores for Hispanics up to 16 years of education. No significant differences in mean extrinsic scores were found for Whites. For both Whites and Hispanics, progressively frequent religious attendance was associated with progressively higher intrinsic scores. In general, higher extrinsic scores for Whites were associated with more frequent religious attendance, and no relationship was found between extrinsic scores and religious attendance for Hispanics. Higher levels of self-rated health were associated with higher intrinsic scores. No other relationships were found to be significant.
There were no significant differences in the distribution of religious orientation between Whites and Hispanics (P = 0.69). However, significant differences in distribution were discovered among religious preferences (Table 5). Latter-day Saints were more likely to be pro-religious and less likely to be nonreligious or extrinsic than the other religious preferences. Protestants and “other” religious preferences were more likely to be nonreligious than either Latter-day Saints or Roman Catholics.
The association between total minutes of exercise per week and religious preference was significantly modified by race/ethnicity (P = 0.016). Consequently, the results presented in Table 6 are stratified accordingly. Among religious orientations in Whites, nonreligious individuals exercised the most, followed by extrinsics, pro-religious and intrinsics. For Hispanics, pro-religious exercised the most, followed by extrinsics, nonreligious and intrinsics; however, for both Whites and Hispanics, the differences in mean minutes of exercise were not statistically significant. Significant differences in exercise were found for both Whites and Hispanics according to religion. For Whites, members of other faiths exercised the most, followed by Roman Catholics, those with no religious preference, Latter-day Saints and Protestants. For Hispanics, Protestants exercised the most, followed by members of other faiths, those with no religious preference, Latter-day Saints and Roman Catholics.
The association between religious orientation and mean scores for self-rated overall health is presented in Table 7. Significant associations were not found when the sample was stratified by race/ethnicity, but significant differences were found for the sample as a whole. Intrinsics reported the best overall health, followed by pro-religious, nonreligious and extrinsic orientations.
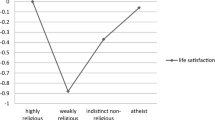
Life satisfaction mean scores were found to vary by race/ethnicity. A significant association between SWLS scores was found for Hispanics but not for Whites; however, a significant association for the sample as a whole was present even after controlling for race/ethnicity (see Table 8). For both Whites and Hispanics, pro-religious individuals reported the highest life satisfaction, followed by extrinsic, intrinsic and nonreligious for Hispanics and intrinsic, extrinsic and nonreligious for Whites. More frequent attendance was associated in a graded fashion with increased life satisfaction scores for both Whites and Hispanics, and the gradient was steepest for Whites. Lastly, for both Whites and Hispanics, those who had ever smoked reported significantly lower life satisfaction than those who had never smoked.
Discussion
This study found that responses to one-half of the questions on the Religious Orientation Scale differed significantly by race/ethnicity, education and religious preference. Hispanics on average scored a full point lower than Whites for all three of the reverse-scored intrinsic-scale questions (3, 10 and 14). These questions ask participants to compare the importance of their religion with the other factors that affect daily life. Hispanics were less likely to report that religion was of greatest importance, that it affected daily life, and that religious belief was of great importance if one lived life in a good way. It is likely that these differences between Whites and Hispanics arise both from differences in ethnic culture and religion, since, after controlling for race/ethnicity, Roman Catholics still had significantly lower intrinsic scale scores than Latter-day Saints (Whites were more likely to be Latter-day Saint, and Hispanics were more likely to be Roman Catholic). Previous studies have shown that ROS responses can vary between nations (Lavricˇ and Flere 2008), but studies to date have not tested for response differences in scale questions for Hispanic populations. The findings of this study indicate that future analyses of religious orientation need to be cautious about possible differences in ROS responses due to race/ethnicity. The SWLS was much less prone to racial/ethnic differences.
One criticism of the religious orientation literature is that it has predominantly focused on Whites and Protestant populations (Hill and Pargament 2003; Hall et al. 2008). The findings of this study provide additional weight to that criticism, as significant differences in intrinsic/extrinsic scores were found between Latter-day Saints, Roman Catholics, Protestants and “other” religious preferences, and interaction effects were found between race/ethnicity and many of the demographic and religious questions. Additional research that incorporates race/ethnicity and religious diversity into its analysis will contribute greatly to the literature and shed light on the differential effects associated with religious orientation in varying cultures and ethnicities.
Previous studies have analysed the association between education and religious orientation. Studies among Taiwanese students have found a positive correlation between education and intrinsic religiousness (Liu 2010) and that education can moderate the relationship between religious orientation and ethical ideology (Chen and Liu 2009). This study found that increased education was associated with increased intrinsic scores for both Whites and Hispanics, while no relationship was found between increased education and extrinsic scores. A possible explanation is that increased education may be associated with higher intrinsic motivation in general, and this motivation carries into religious life. The lack of an education trend in terms of increasing or decreasing extrinsic scores suggests that the external social/emotional motivations and influences of religion do not vary greatly as one becomes more educated.
The association between increased church attendance and increasing intrinsic scores for both Whites and Hispanics is not surprising: it is logical that those who feel more intrinsically motivated to be religious will attend religious services more frequently than those who do not claim such strong motivations. What is surprising is that increased extrinsic motivation does not go hand-in-hand with increased church attendance for either Whites or Hispanics. While it is true that religious services can offer social outlets to members, it does not appear that increased motivation to receive the social benefits of religion translates into increased attendance at religious services. It may be that a difference exists, rather, in the point at which an individual achieves satiation of social benefits of religion. Some may obtain those benefits from infrequent attendance, while others may need frequent attendance in order to obtain those benefits.
In terms of health, those who are more intrinsically motivated appear to have better self-rated health, while increased life satisfaction differs by race/ethnicity; however, for both Whites and Hispanics, it is the combination of intrinsic and extrinsic motivations that is associated with the highest life satisfaction. It is possible that when answering the question regarding self-rated overall health, responses were oriented more towards physical health, which has been shown by previous studies to be associated with intrinsic religious orientation. When answering the life satisfaction questions, psychological health was also being assessed, and this may be a better proxy of true “overall health.” For this question, it would follow that pro-religious individuals would have the highest life satisfaction, as they would accrue the physical benefits of intrinsic orientation and the social capital benefits of extrinsic orientation. Previous studies have shown that intrinsic and pro-religious individuals are better able to cope during times of difficulty (Meyer et al. 1992); however, the lack of studies which have analysed pro-religious individuals in terms of either self-rated health or life satisfaction is of concern. This study’s use of the fourfold typology allows for analysis of health effects associated with combinations of intrinsic and extrinsic religious orientation. Being nonreligious is associated with the lowest mean life satisfaction scores for both Whites and Hispanics. Little research has been done on the nonreligious orientation, but one study did find a low occurrence of health-promoting behaviours among this group (Turner-Musa and Wilson 2006). It is likely that nonreligious individuals miss out on the potential health benefits associated with either intrinsic or extrinsic orientation.
The relationship between religious preference and total minutes of exercise per week was significantly modified by race/ethnicity. For Roman Catholics, the average number of minutes exercised each week was 51% greater for Whites than for Hispanics. On the other hand, among Protestants the average number of minutes exercised each week was 458% greater for Hispanics than for Whites. This difference in emphasis on exercise between Whites and Hispanics is unclear. Average minutes exercised per week were similar for White and Hispanic Latter-day Saints. With the exception of White Protestants and Hispanic Roman Catholics, Latter-day Saints have lower average levels of exercise, which is consistent with previous research involving physical activity among religious groups in Utah (Merrill and Thygerson 2001).
It is interesting to note that higher religious attendance was associated with higher life satisfaction in Whites, while no association was found for Hispanics. Again, this underscores the importance of taking race/ethnicity into account when conducting analyses on the association between religion and health. A likely explanation is that Whites were predominantly Latter-day Saints, while Hispanics were predominantly Roman Catholic. The strong Latter-day Saint culture in Utah, with its emphasis on regular church attendance, may mean that Whites who do not attend religious services frequently may feel more separated from the general community at-large than Hispanics. This finding is consistent with those of Ellison et al. (2009), who found church attendance to be inconsistently associated with depressive symptoms in Hispanics. They also reported that data on Hispanic religious attendance and life satisfaction are limited, and they listed only one study that has explored the subject (Levin et al. 1996). Levin, Markides and Ray found that for older generations of Mexican Americans in Texas, increased religious attendance was associated with life satisfaction. It is clear that more research is still needed on this subject.
The strong association between SWLS score and smoking history is also of note. Previous studies have found associations between smoking and life satisfaction (Grant et al. 2009; Strine et al. 2008). Surprisingly, this relationship was found among those who had ever smoked, even though the majority of them were no longer smoking. It is likely that having a history of smoking is a proxy for physical and psychological health problems that are associated with lower life satisfaction.
Limitations
This study was conducted among a statewide representative sample of Utah residents, and the distribution of religious preferences in the sample differs from that of the general US population. Therefore, it is unlikely that nationwide generalizability of our results apply; however, the finding that ROS responses differ by race/ethnicity is likely to be more generalizable to the US population as a whole. Bias may have also resulted from respondents self-rating their health, but due to the anonymous nature of this study, we do not anticipate this to be a problem.
Conclusion
To our knowledge, this is the first study to compare religious orientation and health between Whites and Hispanics. We found that responses on the ROS differed significantly by race/ethnicity for half of the scale’s questions. Race/ethnicity was found to be a moderating variable for many of the demographic and religious questions, and there were several variables (life satisfaction, church attendance, education, self-rated health) that had significant associations with one racial group but not the other. That significant associations between religious orientation and health were found for Hispanics is encouraging for showing cross-cultural applicability of the ROS, but the fact that responses differed by race/ethnicity demonstrates that future studies of religious orientation should incorporate a cultural context into their analyses. The question of race has been neglected in studies of religious orientation, especially for Hispanics, who make up the largest minority group in the United States. This study fills a gap in the literature in regard to race and religious orientation, and further research is needed on linkages between race, religious orientation and health.
This study also demonstrates the utility of the fourfold typology in relating religious orientation to health. Studies that analyze the pro-religious and nonreligious orientations are rare, and the research presented in this paper demonstrates that pro-religious individuals report the highest life satisfaction in both the White and Hispanic populations. The fact that life satisfaction scores between the two high-intrinsic groups (intrinsic, pro-religious) differed significantly indicates that future research regarding religious orientation and health should look at these groups separately instead of lumping them into a singular “high-intrinsic” category. This study further contributes to the literature by utilizing all four religious orientation types in its analysis. Research regarding the pro-religious and nonreligious groups remains a rich area of study.
References
Allport, G. W. (1950). The individual and his religion: A psychological interpretation. New York: Macmillan.
Allport, G. W. (1963). Behavioral science, religion, and mental health. Journal of Religion and Health, 2(3), 187–197.
Allport, G. W., & Ross, M. J. (1967). Personal religious orientation and prejudice. Journal of Personality and Social Psychology, 5(4), 432–443.
Chen, S., & Liu, C. (2009). Relationships between personal religious orientation and ethical ideologies. Social Behavior and Personality, 37(3), 313–320.
Cohen, A. B., Hall, D. E., & Koenig, H. G. (2005). Social versus individual motivation: Implications for normative definitions of religious orientation. Personality and Social Psychology Review, 9(1), 48–61.
Cohen, A. B., Malka, A., Hill, E. D., Thoemmes, F., Hill, P. C., & Sundie, J. M. (2009). Race as a moderator of the relationship between religiosity and political alignment. Personality and Social Psychology Bulletin, 35(3), 271–282.
Colbert, L. K., Jefferson, J. L., Gallo, R., & Davis, R. (2009). A study of religiosity and psychological well-being among African Americans: Implications for counseling and psychotherapeutic processes. Journal of Religion and Health, 48, 278–289.
Diener, E., Emmons, R. A., Larson, R. J., & Griffin, S. (1985). The satisfaction with life scale. Journal of Personality Assessment, 49, 71–75.
Donahue, M. J. (1985). Intrinsic and extrinsic religiousness: Review and meta-analysis. Journal of Personality and Social Psychology, 48(2), 400–419.
Ellison, C. G., & Levin, J. S. (1998). The religion-health connection: Evidence, theory, and future connections. Health Education and Behavior, 25(6), 700–720.
Ellison, C. G., Finch, B. K., Ryan, D. N., & Salinas, J. J. (2009). Religious involvement and depressive symptoms among Mexican-origin adults in California. Journal of Community Psychology, 37(2), 171–193.
George, L. K., Ellison, C. G., & Larson, D. B. (2002). Explaining the relationship between religious involvement and health. Psychological Inquiry, 13(3), 190–200.
Gorsuch, R. L., & McPherson, S. E. (1989). Intrinsic/Extrinsic measurement: I/E-revised and single-item scales. Journal for the Scientific Study of Religion, 28(3), 348–354.
Gorusch, R. L., & Venable, G. D. (1983). Development of an age universal I-E scale. Journal for the Scientific Study of Religion, 22(2), 181–187.
Grant, N., Wardle, J., & Steptoe, A. (2009). The relationship between life satisfaction and health behavior: A cross-cultural analysis of young adults. International Journal of Behavioral Medicine, 16, 259–268.
Hall, D. E., Meador, K. G., & Koenig, H. G. (2008). Measuring religiousness in health research: Review and critique. Journal of Religion and Health, 47, 134–163.
Hart, A., Jr., Tinker, L. F., Bowen, D. J., Satia-Abouta, J., & McLarren, D. (2004). Is religious orientation associated with fat and fruit-vegetable intake? Journal of the American Dietetic Association, 104, 1292–1296.
Hill, P. C., & Pargament, K. I. (2003). Advances in the conceptualization and measurement of religion and spirituality. The American Psychologist, 58(1), 64–74.
Hill, T. D., Angel, J. L., Ellison, C. G., & Angel, R. J. (2005). Religious attendance and mortality: An 8-year follow-up of older Mexican Americans. Journal of Gerontology: SOCIAL SCIENCES, 60B(2), S102–S109.
Hood, R. W., Jr. (1970). Religious orientation and the report of religious experience. Journal for the Scientific Study of Religion, 9(4), 285–291.
Hood, R. W., Jr. (1978). The usefulness of indiscriminately pro and anti categories of religious orientation. Journal for the Scientific Study of Religion, 17(4), 419–431.
Kirkpatrick, L. A., & Hood, R. A., Jr. (1990). Intrinsic-extrinsic religious orientation: The boon or bane of contemporary psychology of religion? Journal for the Scientific Study of Religion, 29(4), 442–462.
Kirkpatrick, L. A., & Hood, R. A., Jr. (1991). Rub-a-dub-dub: Who’s in the tub? Reply to masters. Journal for the Scientific Study of Religion, 30(3), 318–321.
Lavricˇ, M., & Flere, S. (2008). The role of culture in the relationship between religiosity and psychological well-being. Journal of Religion and Health, 47, 164–175.
Levin, J. S., Markides, K. S., & Ray, L. A. (1996). Religious attendance and psychological wellbeing in Mexican Americans: A panel analysis of three-generations data. The Gerontologist, 36, 454–463.
Levin, J. S., Wickramasekera, I. E., & Hirshberg, C. (1998). Is religiousness a correlate of absorption? Implications for psychophysiology, coping, and morbidity. Alternative Therapies in Health and Medicine, 4(6), 72–76.
Liu, S. (2010). The relationship between personal religious orientation and emotional intelligence. Social Behavior and Personality, 38(4), 461–467.
Maltby, J., & Day, L. (2003). Religious orientation, religious coping and appraisals of stress: Assessing primary appraisal factors in the relationship between religiosity and psychological well-being. Personality and Individual Differences, 34, 1209–1224.
Masters, K. S. (1991). Of boones, banes, babies, and bath water: A reply to the Kirkpatrick and Hood discussion of the intrinsic-extrinsic religious orientation. Journal for the Scientific Study of Religion, 30(3), 312–317.
Masters, K. S., Hill, R. D., Kircher, J. C., Lensagrav-Benson, T. L., & Fallon, J. A. (2004). Religious orientation, aging, and blood pressure reactivity to interpersonal and cognitive stressors. Annals of Behavioral Medicine, 28(3), 171–178.
Masters, K. S., Lensegrav-Benson, T. L., Kercher, J. C., & Hill, R. D. (2005). Effects of religious orientation and gender on cardiovascular reactivity among older adults. Research on Aging, 27(2), 221–240.
McCullough, M. E., Hoyt, W. T., Larson, D. B., Koenig, H. G., & Thoreson, C. (2000). Religious involvement and mortality: A meta-analytic review. Health Psychology, 19(3), 211–222.
Merrill, R. M., Thygerson, A. L. (2001). Religious preference, church activity, and physical exercise. Preventive medicine, 33, 38–45.
Meyer, M. S., Altmaier, E. M., & Burns, C. P. (1992). Religious orientation and coping with cancer. Journal of Religion and Health, 31(4), 273–279.
Nelson, P. B. (1989). Ethnic differences in intrinsic/extrinsic religious orientation and depression in the elderly. Archives of Psychiatric Nursing, 3(4), 199–204.
Pew Forum on Religion and Public Life. (2008). Religious beliefs and practices: Diverse and politically relevant. US religious landscape survey. Retrieved from http://religions.pewforum.org/pdf/report2-religious-landscape-study-full.pdf.
Powell, L. H., Shahabi, L., & Thoreson, C. E. (2003). Religion and spirituality: Linkages to physical health. The American Psychologist, 58(1), 36–52.
Sanchez, D., & Carter, R. T. (2005). Exploring the relationship between racial identity and religious orientation among African American college students. Journal of College Student Development, 46(3), 280–295.
Seybold, K. S., & Hill, P. C. (2001). The role of religion and spirituality in mental and physical health. Current Directions in Psychological Science, 10(1), 21–24.
Strine, T. W., Chapman, D. P., Balluz, L. S., Moriarty, D. G., & Mokdad, A. H. (2008). The associations between life satisfaction and health-related quality of life, chronic illness and health behaviors among US community-dwelling adults. Journal of Community Health, 33, 40–50.
Tapanya, S., Nicki, R., & Jarusawad, O. (1997). Worry and intrinsic/extrinsic religious orientation among Buddhist (Thai) and Christian (Canadian) persons. International Journal of Aging and Human Development, 44(1), 73–83.
Turner-Musa, J. O., & Wilson, S. (2006). Religious orientation and social support on health- promoting behaviors of African-American college students. Journal of Community Psychology, 34(1), 105–115.
Watson, P. J., Ghorbani, N., Davison, H. K., Bing, M. N., Hood, R., Jr., & Gharamaleki, A. F. (2002). Negatively reinforcing personal extrinsic motivations: Religious orientation, inner awareness and mental health in Iran and the United States. International Journal for the Psychology of Religion, 12, 255–276.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Merrill, R.M., Steffen, P. & Hunter, B.D. A Comparison of Religious Orientation and Health Between Whites and Hispanics. J Relig Health 51, 1261–1277 (2012). https://doi.org/10.1007/s10943-010-9432-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10943-010-9432-x