
Abstract
Undocumented migrants face major barriers in accessing prevention and health care. Whereas the association between low socioeconomic status and poor health is well documented only few studies have addressed specific health issues in undocumented migrants. The aim of the present study is to describe sexual and reproductive health behaviors of undocumented migrants in Geneva. This descriptive cross sectional study included consecutive undocumented migrants presenting from November 2007 to February 2008 to a health facility offering free access to health care to this population. Following informed consent, they completed a self administered questionnaire about their socio-demographic profile and sexual and reproductive health behaviors. A total of 384 patients were eligible for the study. 313 (82%) agreed to participate of which 77% (241 patients) completed the survey. Participants were mainly young, Latino-American, single, well-educated and currently working women. They had multiple partners and reported frequently engaging in sexual intercourse. Use of contraceptive methods and strategies of prevention against sexually transmitted infections (STI) were rare. Nearly half of the women had had at least one induced abortion and 40% had had an unplanned pregnancy. One in four participants reported a current or past STI or other genital infection. The results of our study suggest that undocumented migrants engage in frequent and high risk sexual intercourse with insufficient use of contraceptive methods and suboptimal strategies of prevention against STI. Our study underlines the real need for specific sexual and reproductive educational programs targeting this hard to reach population.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Undocumented migrants leave their country above all because of difficult economic conditions, but also to improve the educational future of their children and provide financial support for their families [1, 2]. Geneva hosts between 8,000 and 12,000 undocumented migrants (migrants without legal residency permit) representing 1.8–2.8% of the local population [3]. Economic difficulties in the context of low paying and unsteady jobs, language limitations, separation from family, discrimination and cultural barriers render the immigration process difficult and stressful [2, 4]. Difficult living conditions, exclusion from the health care system due to lack of medical insurance coverage and fear of immigration authorities contribute to an increased risk of poor health in this population [2, 5].
The association between low socioeconomic status and poor health is well documented and several studies have shown that physical and mental health problems are highly prevalent in vulnerable populations, such as asylum seekers, refugees, homeless and detainees [6–13]. Only few studies have addressed specific health issues in undocumented migrants. This is probably due the transient and clandestine nature of this hard-to reach population. Studies to date suggest a higher risk of mental health problems, Chlamydia trachomatis infection and latent tuberculosis infection [14–19]. Undocumented women have been shown to lack knowledge in family planning and contraceptive methods, with a higher rate of unintended pregnancies and delayed prenatal care [20–22]. Both their experience in their home country and their present situation with poor access to preventive health care are incriminated in the high rate of premature voluntary termination of pregnancy, unintended pregnancies and delayed prenatal care observed in the receiving country. Studies are conflicting concerning the magnitude of complications during pregnancy, delivery and post-partum [20–22].
Higher prevalence of sexually transmitted infection and unintended pregnancy could be related to high risk sexual behaviors. Yet, this remains a hypothesis as to our knowledge no previous study has described the sexual and reproductive health behaviors of undocumented migrants. As a result, the aim of the present study was to explore and better describe these behaviors in undocumented migrants living in Geneva.
Methods
Study Design and Population
Despite mandatory universal insurance coverage in Switzerland, more than 90% of Geneva’s undocumented migrants remain uninsured [23]. Since 1996, this population can access free or low cost care in Geneva through the “community mobile unit” of Geneva University Hospitals. The unit provides primary care for around 3,000–3,500 undocumented migrants each year.
This descriptive cross sectional study included all consecutive undocumented migrants who presented from November 2007 to February 2008 to the mobile unit and agreed to participate in a related study estimating the prevalence of Chlamydia trachomatis infection in this population [17].
Inclusion criteria were: capacity to provide formal consent and to communicate in French, English, Spanish or Portuguese, age ≥ 18, absence of a legal residency permit, and the absence of treatment for Chlamydia trachomatis infection in the past 3 months.
Procedure
Following informed consent, participants were asked to complete a self administered questionnaire about socio-demographic profile (sex, age, civil status, origin, parity for women, type of household, education, occupation) and sexual and reproductive health behaviors (type and frequency of use of contraceptive methods including condom use, age at first sexual intercourse, frequency of sexual intercourses, number of sexual partners, number of sexual intercourses with sex workers, uro-genital complaints, past or current sexually transmitted infections (STI) and other genital infections, induced abortions and unplanned pregnancies). According to other authors, we defined a cut-off of six lifetime sexual partners as high risk exposure. [24–26] Questionnaires were available in French, English, Spanish and Portuguese. The original was written in French, translated and back-translated by a trilingual gynecologist (English, Portuguese, French) and a bilingual primary care physician (Spanish, French) and then pre-tested in all four languages with 20 patients each time. A multilingual investigator was available onsite to provide help in answering the questionnaires.
Statistical Analysis and Ethical Considerations
We performed Chi-square and Fisher’s exact tests to compare proportions of sexual characteristics in men and women for categorical variables, and unpaired student t-tests to compare means for continuous variables. All analyses were performed using Stata version 10 (Stata Corp LP).
All undocumented migrants gave written consent after having received detailed oral and written explanations. The study was approved by the ethics committee of Geneva University Hospitals (protocol number 06-134).
Results
Of 384 patients eligible to participate in the related study on the prevalence of Chlamydia trachomatis infection, 313 (82%) agreed to participate, of which 241 (77%) completed the questionnaire (73.9% women, mean age 32.6, SD 8.0, min 18, max 50).
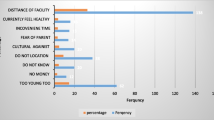
Lack of time was the most common reason for not completing the questionnaire.
Table 1 summarizes the socio-demographic characteristics of the 241 participants by gender. 91% of undocumented women (vs. 70% of the undocumented men, P < 0.01) came from South and Central America, mainly from Bolivia and Brazil. They were mostly single, and less than 20% lived alone. They had a relatively high level of education and 70% of women (vs. 48% of men, P < 0.01) were currently employed. None of the undocumented migrants has been excluded due to recent treatment for CT infection.
Table 2 presents the sexual and reproductive health behaviors of participants by gender. All but one participant (99.6%) were sexually active and mean age at first sexual intercourse with penetration was slightly higher for women than for men (18.6, SD 3.7 vs. 16.4, SD 3.1, P < 0.01). Nearly 40% reported more than one sexual intercourse per week, without significant gender differences. Men generally reported higher sexual risk behaviors than women with nearly half of them having had 6 or more sexual partners in their lifetime (women: 15%, P < 0.01), 8% of men reporting 2 or more sexual partners in the past 3 months (women: 1.1%, P = 0.02), and 28% indicating they had had sex with a sex-worker at least once in their lifetime (women: 4%, P < 0.01). Only 19% of women used the contraceptive pill and nearly 80% of them did not use a condom during the last sexual intercourse. In contrast, 41% of men reported using a condom during the last sexual intercourse with penetration. More than one-third of participants reported not having used any contraceptive method during last sexual intercourse; approximately 50% had not used a condom during the last year and only 20% reported using a condom during each intercourse, without significant gender differences. Finally, nearly 50% of women reported having had at least one induced abortion and 40% reported having had an unplanned pregnancy.
Fifty-two undocumented migrants (women: 26%, men: 10%, P = 0.03) reported one or more current or past STI or other genital infection (cervicitis, endometritis or salpingitis (n = 6), genital herpes (5), genital ulcer (4), Hepatitis B (4), gonococcus (4), HPV (3), condyloma (3), urethritis (2), Hepatitis C (2), dysplasia of the uterine cervix, vulva or vagina (2), Chlamydia (1), other infections (25).
65% of women (men 28%, P < 0.01) reported uro-genital complaints in the last week, mainly lower abdominal pain (35%), unusual vaginal discharge (23%), pollakiuria (19%) and dysuria (18%). Men reported pollakiuria (16%), dysuria (12%) and lower abdominal pain (7%). Only one man reported discharge from the penis.
Discussion
Main Findings and Comparisons with Other Studies
This study highlights the high sexual and reproductive risk behaviors of a population of undocumented migrants. In this population of mainly young, Latino-American, single and well-educated participants, unprotected intercourse, lack of adequate contraception and history of multiple partners were common. One-third had used no contraceptive method during last sexual intercourse and approximately half had not used a condom in the past year.
In view of this it is not surprising that nearly half the women reported having had at least one induced abortion in their lifetime, 40% had had an unplanned pregnancy, 65% reported uro-genital symptoms in the past week and 25% of participants had a current or past STI or other genital infection.
Surprisingly few previous studies provide information on the sexual and reproductive health of undocumented migrants. In a study conducted among female sex workers in Hong Kong, 30% of which were undocumented migrants, condom use with non commercial partners was similarly low and reports of previous STI were high as in our study [27]. With the exception of two studies on obstetric care, the few other studies that provide information on sexual and reproductive health characteristics of undocumented migrants have all, to our knowledge, been conducted in the same setting as the present study, i.e., the “community mobile unit” of Geneva University Hospitals [18, 20–22, 28].
In a prospective cohort of pregnant women undergoing induced abortion, participants were almost twice as likely not to use any contraception if they were undocumented migrants compared to women with a legal residency permit (23% vs. 15%) [18]. Moreover, 48% of pregnant undocumented women with unintended pregnancies but wishing to deliver did not use any contraception (vs. 33% in a control group consisting of a sample of pregnant women with legal residency permit wishing to deliver) [22]. Our study also confirms the high rate of unintended pregnancies highlighted in two previous studies: 75 and 83% in two samples of undocumented pregnant women wishing to deliver (vs. 21% in the control group) [21, 22]. These results probably also reflect the inappropriate use of contraceptive methods in this population.
The comparison of our findings with those from studies of legal residents in Switzerland further emphasizes the high sexual and reproductive risk behaviors in our sample of undocumented migrants. In a prospective study of contraceptive use among 103 women (mean age: 27, non Swiss: 48%) in Geneva 6 months after termination of pregnancy, 84% used contraception (69% oral contraception), as opposed to 69% (19% oral contraception) 1–3 weeks before termination of pregnancy (compared to 67% who used contraception, of which 19% oral contraception, in our sample of undocumented migrants) [29, 30]. Therefore, in terms of contraceptive use, our population of illegal immigrants was similar to that of legal residents in Switzerland requesting termination of pregnancy.
The rate of induced abortions was clearly higher in undocumented migrants than in the general population: 46% compared to 1–3% for Swiss and foreign legal residents in Switzerland [31–33].
The mean number of lifetime sexual partners (2–5) was similar to that reported by residents in Switzerland in a telephone survey conducted between 1987 and 1994 [34]. Caution is needed when comparing our findings with these old data however, as sexual attitudes and behaviors are likely to have evolved during this period and sexual characteristics may be underreported in telephone surveys [35]. AIDS prevention campaigns in Switzerland may have led to a reduction in the mean number of reported lifetime sexual partners in the overall population since 1994. In a recent study in which 517 young Swiss men undergoing compulsory military recruitment (18–26 years) were asked to complete a questionnaire on sexual behaviors, 13% reported not having ever had a sexual partner vs. 0% in our sample of illegal residents and 60% reported having had two or more partners vs. 85% for men in our study [36]. Condom use was much higher in these Swiss men compared to the men involved in our study (always: 33% vs. 18%, never: 15% vs. 45%). However, comparison is difficult because the study participants were younger than those in our study. In the study conducted by Dubois-Arber et al. condom use in 1994 was also higher with 56% of 17–30 years-old respondents and 42% of 31–45 years-old respondents reporting constant use [34].
Finally, a higher proportion of undocumented migrant men reported having had sex with a sex-worker compared to legal residents (30% compared to 21.5% for men aged 31–45 and 26% compared to 11.5% for men aged 17–30) [37]. On this subject underreporting is likely but the extent to which this may have affected both Jeannin et al’s telephone survey and our own study is unknown. It is of note that in the study by Dubois-Arber et al., only 1–3% reported sex with prostitutes both in 1987 and 1994 [34].
To our knowledge, the current study is the first to identify significant gender differences in the sexual and reproductive behaviors of undocumented migrants. In our sample of 241 participants, undocumented men reported having sex since a younger age than women. They had more sexual partners and were more likely to have sexual intercourse with sex workers, but reported less past or current STI and less uro-genital complaints. In view of the fact that STI are frequently asymptomatic in men, further research should inform the need for specific STI screening programs in this high risk male population [38]. However, the related study showed Chlamydia infection was more frequent among undocumented males in Geneva than in the general population yet the prevalence of this infection (4%) did not seem high enough to warrant systematic screening [17, 36]. By contrast, there were no significant differences between men and women in relation to the frequency of sexual intercourse.
The results of this study highlight the need to further develop sexual and reproductive preventive programs in this population. This is a challenge as this population remains difficult to reach and is not frequently in contact with health professionals.
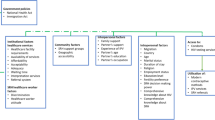
The cost of health care is a major barrier to reaching this population since more than 90% of undocumented migrants lack health insurance (it is expensive and they have to pay themselves). Another important barrier to accessing this population is the language barrier. Cultural and social factors additionally complicate communication between local health providers and undocumented migrants [39]. The “community mobile unit” in Geneva partially addresses these barriers yet the results of our study highlight the need for specific programs delivered to this vulnerable population, providing language and culturally appropriate education on contraception, family planning and risks of transmission of STI.
Strengths and Limitations of the Study
To our knowledge, this is the first study exploring in detail the sexual and reproductive health behaviors in this hard-to-reach population. Another strength is the prospective and systematic inclusion of a relatively large number of participants. Finally, participation rate was high (nearly 80%) despite the sensitive nature of the topic under study. In addition, there were only few missing data. A self-administered questionnaire was probably the best choice in this situation, in order to promote more truthful responses to sensitive questions as compared to face-to-face interviews [35].
Our study shows also some limitations. First, undocumented migrants participating in our study may not be representative of the total undocumented population in Geneva because of the predominance of Latin American women in our sample and recruitment of participants within a health care facility. The proportion and the age and gender distribution of Latin Americans in our study was however similar to that described in other sources [40]. In addition, the “community mobile unit” is the only point of care for this population in Geneva. Second, our study rests entirely on the answers to a questionnaire, without confirmation by biological measurements (for current or past infections for example), medical records (for induced abortions or unplanned pregnancies for example), physical examination (for some current infections) or proxy respondents (family members, friends, sexual partners). As social bias would tend to favor underreporting of sexual and reproductive risk behaviors, use of this questionnaire may have provided more conservative estimates of the prevalence of risk behaviors in this population. Finally, no control group was included in our study limiting the possibilities of comparing results with that of legal residents in Geneva.
Conclusion
The results of this study highlight the high rates of sexual and reproductive risk behaviors in this population of mainly young, Latino-American, single, well-educated and currently employed women. They underline the need for specific and culturally accepted educational programs targeting this hard-to-reach population.
References
Berk ML, Schur CL, Chavez LR, et al. Health care use among undocumented Latino immigrants. Health Aff (Millwood). 2000;19(4):51–64.
Cavazos-Rehg PA, Zayas LH, Spitznagel EL. Legal status, emotional well-being and subjective health status of Latino immigrants. J Natl Med Assoc. 2007;99(10):1126–31.
Wolff H, Besson M, Holst M, et al. Social inequalities and health: experiences of a mobile health care unit in Geneva. Rev Med Suisse. 2005;1(34):2218–22.
Cabassa LJ, Zayas LH, Hansen MC. Latino adults’ access to mental health care: a review of epidemiological studies. Adm Policy Ment Health. 2006;33(3):316–30.
Berk ML, Schur CL. The effect of fear on access to care among undocumented Latino immigrants. J Immigr Health. 2001;3(3):151–6.
Dorling D, Mitchell R, Pearce J. The global impact of income inequality on health by age: an observational study. BMJ. 2007;335(7625):873.
Gerritsen AA, Bramsen I, Deville W, et al. Physical and mental health of Afghan, Iranian and Somali asylum seekers and refugees living in the Netherlands. Soc Psychiatry Psychiatr Epidemiol. 2006;41(1):18–26.
McMahon JD, Macfarlane A, Avalos GE, et al. A survey of asylum seekers’ general practice service utilisation and morbidity patterns. Ir Med J. 2007;100(5):461–4.
Fazel M, Wheeler J, Danesh J. Prevalence of serious mental disorder in 7000 refugees resettled in western countries: a systematic review. Lancet. 2005;365(9467):1309–14.
Keyes EF. Mental health status in refugees: an integrative review of current research. Issues Ment Health Nurs. 2000;21(4):397–410.
Mollica RF, Sarajlic N, Chernoff M, et al. Longitudinal study of psychiatric symptoms, disability, mortality, and emigration among Bosnian refugees. JAMA. 2001;286(5):546–54.
Fazel S, Khosla V, Doll H, et al. The prevalence of mental disorders among the homeless in western countries: systematic review and meta-regression analysis. PLoS Med. 2008;5(12):e225.
Fazel S, Danesh J. Serious mental disorder in 23000 prisoners: a systematic review of 62 surveys. Lancet. 2002;359(9306):545–50.
Rasmussen A, Rosenfeld B, Reeves K, et al. The subjective experience of trauma and subsequent PTSD in a sample of undocumented immigrants. J Nerv Ment Dis. 2007;195(2):137–43.
Eisenman DP, Gelberg L, Liu H, et al. Mental health and health-related quality of life among adult Latino primary care patients living in the United States with previous exposure to political violence. JAMA. 2003;290(5):627–34.
Sullivan MM, Rehm R. Mental health of undocumented Mexican immigrants: a review of the literature. ANS Adv Nurs Sci. 2005;28(3):240–51.
Jackson Y, Sebo P, Aeby G, et al. Prevalence and associated factors for Chlamydia trachomatis infection among undocumented immigrants in a primary care facility in Geneva, Switzerland: a cross-sectional study. J Immigrant Minority Health. 2010. doi:10.1007/s10903-010-9354-4.
Wolff H, Lourenco A, Bodenmann P, et al. Chlamydia trachomatis prevalence in undocumented migrants undergoing voluntary termination of pregnancy: a prospective cohort study. BMC Public Health. 2008;8:391.
Bodenmann P, Vaucher P, Wolff H, et al. Screening for latent tuberculosis infection among undocumented immigrants in Swiss healthcare centres; a descriptive exploratory study. BMC Infect Dis. 2009;9:34.
Reed MM, Westfall JM, Bublitz C, et al. Birth outcomes in Colorado’s undocumented immigrant population. BMC Public Health. 2005;5:100.
Wolff H, Stalder H, Epiney M, et al. Health care and illegality: a survey of undocumented pregnant immigrants in Geneva. Soc Sci Med. 2005;60(9):2149–54.
Wolff H, Epiney M, Lourenco AP, et al. Undocumented migrants lack access to pregnancy care and prevention. BMC Public Health. 2008;8:93.
Wolff H. Bilan annuel et statistiques de l’unités mobile de soins communautaires (UMSCO). Annual report and statistics of the community mobile unit (UMSCO). 2006. Cited 1 November 2009; Available from: http://umsco.hug-ge.ch/mission_prestations/chiffres-cles.html.
Oh MK, Cloud GA, Wallace LS, et al. Sexual behavior and sexually transmitted diseases among male adolescents in detention. Sex Transm Dis. 1994;21(3):127–32.
van Valkengoed IG, Morre SA, van den Brule AJ, et al. Low diagnostic accuracy of selective screening criteria for asymptomatic Chlamydia trachomatis infections in the general population. Sex Transm Infect. 2000;76(5):375–80.
Gotz HM, van Bergen JE, Veldhuijzen IK, et al. A prediction rule for selective screening of Chlamydia trachomatis infection. Sex Transm Infect. 2005;81(1):24–30.
Wong WC, Wun YT, Chan KW, et al. Silent killer of the night: a feasibility study of an outreach well-women clinic for cervical cancer screening in female sex workers in Hong Kong. Int J Gynecol Cancer. 2008;18(1):110–5.
Lu MC, Lin YG, Prietto NM, et al. Elimination of public funding of prenatal care for undocumented immigrants in California: a cost/benefit analysis. Am J Obstet Gynecol. 2000;182(1 Pt 1):233–9.
Bianchi-Demicheli F, Perrin E, Ludicke F, et al. Contraception and sexuality after termination of pregnancy: a comparison between Lugano and Geneva. Swiss Med Wkly. 2001;131(35–36):515–20.
Bianchi-Demicheli F, Perrin E, Bianchi PG, et al. Contraceptive practice before and after termination of pregnancy: a prospective study. Contraception. 2003;67(2):107–13.
Addor V, Narring F, Michaud PA. Abortion trends 1990–1999 in a Swiss region and determinants of abortion recurrence. Swiss Med Wkly. 2003;133(15–16):219–26.
Balthasar H, Spencer B, Addor V, et al. Voluntary pregnancy termination in the canton of Vaud in 2002. Rev Med Suisse Romande. 2004;124(10):645–8.
Johnston W. Historical abortion statistics, Switzerland.2008. Cited 1 November 2009; Available from: http://www.johnstonarchive.net/policy/abortion/ab-switzerland.html.
Dubois-Arber F, Jeannin A, Konings E, et al. Increased condom use without other major changes in sexual behavior among the general population in Switzerland. Am J Public Health. 1997;87(4):558–66.
Armstrong B, White E, Saracci R. Principles of exposure measurement in epidemiology. New York: Oxford University Press; 1992.
Baud D, Jaton K, Bertelli C, et al. Low prevalence of Chlamydia trachomatis infection in asymptomatic young Swiss men. BMC Infect Dis. 2008;8:45.
Jeannin A, Rousson V, Meystre-Agustoni G, et al. Patterns of sex work contact among men in the general population of Switzerland, 1987–2000. Sex Transm Infect. 2008;84(7):556–9.
Lewis DA, Pillay C, Mohlamonyane O, et al. The burden of asymptomatic sexually transmitted infections among men in Carletonville, South Africa: implications for syndromic management. Sex Transm Infect. 2008;84(5):371–6.
Blochliger C, Tanner M, Hatz C, et al. Asylum seekers and refugees in ambulatory health care: communication between physician and patient. Praxis (Bern 1994). 1997;86(19):800–10.
Syndicat interprofessionel de travailleuses et travailleurs. Pour mettre au jour l’économie de l’ombre. [To reveal the shadow economy]. Geneva: S.I.T.; 2003.
Acknowledgments
This study was supported by institutional grants from the Geneva University Hospitals (R&D fund) and the General directorate of health, Department of economy and health, Geneva Canton.
Conflict of interest statement
The authors declare no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sebo, P., Jackson, Y., Haller, D.M. et al. Sexual and Reproductive Health Behaviors of Undocumented Migrants in Geneva: A Cross Sectional Study. J Immigrant Minority Health 13, 510–517 (2011). https://doi.org/10.1007/s10903-010-9367-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10903-010-9367-z