
Abstract
Smoking behavior is a threat for Indonesian teenagers, including in the city of Jayapura, Papua province. The purpose of this study was to access Jayapura teenagers smoking behavior and knowledge including parents and other family members. The study was conducted on 78 respondents (grade 7, aged 11–14 years old), using cluster random sampling for selecting the public and private junior high school in Jayapura. The data collected was smoking behavior of respondents, parents and other family members (using self-reported questionnaire), and respondents’ knowledge about the dangers of smoking (using tests with Cronbach’s alpha 0.701). Data were analyzed descriptively and analytically using Chi-square, 95 % level of significant. The results showed 29.3 % of teenagers, 69.23 % of parents and 25.6 % of other family members were smokers, their knowledge was low (an average score of 60.81 out of 100), there was no significant statistical relationship between knowledge and smoking behavior among respondents (p = 0.079), and there is no significant relationship between teenagers behavior with the behavior of the parents (p = 0.609) and other family members (p = 0.578), 87 % of teenagers became smokers because there were individuals who smoke at home.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
There are three serious problems that threaten the teenagers’ future i.e. smoking behavior, alcohol and narcotics, psychotropic drugs, or hazardous substances. The teenager, 40 % of 210 million populations, is still a potential target of a third of the hazardous material [1]. Among the three of hazardous materials, the earliest materials known to the public especially by teenagers are cigarettes. Smoking behavior was the gateway of the other behavior, alcohol and drugs [2].
Either “Smoking” or “Being healthy” is a decision that must be chosen by individuals who already have sufficient information about smoking and its danger. Actually, teenagers (aged 12–14 years old) have not possessed fully enough information about it. They believe that smoking can withstand hunger, increase self-esteem, look more mature, and give a positive image for them. Smoking behavior in teenagers is a serious problem because it is the parents who fulfill their needs in general including cigarettes. For the poor, it can substitute food, education and health needs for the family. Lately, teenager inducement to smoke cigarette is getting earlier, i.e. 8–14 years [2]. The younger the teenager know how to smoke, the longer the family burden to bear the consequences. The impact of smoking on health should also be responsible either by the smoker or his family, namely as a result of passive smoking. Passive smokers, than smokers themselves, are higher risk for chronic diseases development.
The short term impact of smoking for health are coughing, fatigue, shortness of breath, and the absence of ability to smell and taste the flavor, while the long-term impact are lips, tongue, throat and lungs cancer, respiratory disorders, tuberculosis, heart disease, hypertension, osteoporosis, kidney disorders, fertility disorders, skin wrinkles and others [3]. Frequently the health risks can cause death, significant impact on mortality. The data showed 25 % of deaths due to coronary heart disease, 80 % of deaths due to chronic respiratory cases, and 90 % of deaths due to lung cancer. Study on Non-Hispanic teenage smokers with low social economic in the United States, showed that those who knew cigarettes early have a greater mortality risk significantly compared to those who know smoking at older age (late initiation) [4]. In addition to the family economic and health impact, teenage smokers in general would also be a potential predictor for a number of other social problems such as school drop-out, unhealthy sexual behavior and juvenile delinquency.
The Ministry of Health campaign on 10 Clean and Healthy Lifestyle Behaviour (PHBS) indicators, particularly the 10th indicator, “no smoking in the house”, should be applied to the family [5]. Data by province throughout Indonesia 2007–2013 showed increasing proportion of the population older than 15 years old who consume snuff and chewing tobacco continues to increase, from 34.2 to 36.3 %. The average national scale cigarettes smoked/day in population older than 10 years old was 12.3 cigarettes/day [6]. It could not be categorized mild, whereas mild was considered as the number of cigarettes smoked/day less than 5 cigarettes (Shiffman in Zhu, Sun, Hawkins, Pierce, and Cummings, 2003 in Astuti [2]). Until now there has been no national data on the teenager smoking behavior, aged 13–15 years old or equivalent to grade 7, 8, and 9 junior high school.
Papua province is the easternmost province of Indonesia, Jayapura City is the capital of the province. Eastern city of Jayapura Papua borders with neighboring countries, Papua Nuegini. The numbers of cigarettes smoked per day (older than 10 years old population) in exceeding the national rate (more than 12.3 cigarettes/day) [7]. The highest percentage of older than 10 years population who smoke is 80.1 % in Puncak Jaya, 80.0 % in Mimika, and 76.4 % in Jayapura [7]. That means, the non smoker data of the older than 10 years old population (including teenagers) are 19.9, 20 and 23.6 %, consecutively for the three areas. Teenagers who do not smoke in Jayapura city is the highest (23.6 %). These teenagers group need special attention in developing eternal non-smoker behavior.
Besides, another culture for Papua people is the behavior of drinking. The governor and law enforcement agencies regulate and prohibit the production, distribution, and sale of alcoholic beverages in a regulation of the Governor of Papua Act Number: 3/Instr-Gub/2016. In addition to the regional regulation, the Governor efforts hard to combat drinking in Papua as indicated in their assertion period 2013–2018. It was declared at a regional Papua mayors working meeting in Sasana Krida Jayapura City, March 29th–30th, 2016. The governor stated that Papua will be free of alcohol, which begins with confiscation step from distributors and nightlife bars [8].
Research at Columbia University, the United States stated that the teenage smokers had five times chances to become alcohol drinker [1]. On the basis of these results can be assumed that alcohol drinking behavior Papua society today is related to smoking behavior when they were teenagers. To anticipate the behavior of drinking alcohol at the future time, we should be aware of teenagers smoking behavior nowadays. The objective of this study is to access the smoking behavior and teenagers’ knowledge including parents and other family members in the city of Jayapura, Papua. The result of this study can be used as an input for policy makers in health promotion level.
Method
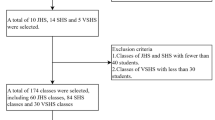
This was a survey research, conducted in Jayapura, Papua, Indonesia, in August 2015. Subjects were class 7 junior high school students (11–14 years old) from 1 Public school and 2 Private schools, cluster randomly selected, in Jayapura, with the total of 78 students, consisting of 26 students (from School “N”), 23 students (from School “H”), and 29 students (from School “P”). The research variables were the smoking behavior of respondents, knowledge of students about the dangers of smoking and smoking behavior of parents (father and mother), the smoking behavior of family members at home (brother and other members). Smoking behavior was collected from respondents by filling out the questionnaires (self reported questionaire). Students’ knowledge about the dangers of smoking was measured by using a test-questions. The knowledge test consisted of 7 statement items with 0.701 reliability Cronbach’s alpha. Knowledge score was between 0 and 100. Smoking behavior of parents (father/mother), the other members (brother/other members) at home, collected using questionnaires completed by respondents.
Result
Subjects, from 78 respondents, female (59 %) male (41 %), are 12 years old in average (range from 11 to 14 years old). Respondents who smoke were 23 respondents (29.3 %), scattered in three Schools. The average score of respondents’ awareness of the dangers of smoking was 60.81 and the average highest to lowest score was from school “N”, from school “H” and from school “P” orderly. Even in school “P” there was one person who scores zero (Table 1).
From the data, based on gender and age, the highest percentage was 56.52 % of male smokers and 60.86 % smokers at the age of 12 years (Table 2). The smoking respondents had higher knowledge than non smoking group but it was statistically not significant, p = 0.079 (Table 3). 69.23 % of respondents had parents who smoke. The highest number of parents who smoke was in school “P” (75.9 %). There are other family members (25.64 %) who live with the respondent who smoke. This condition is scattered over three schools, mostly in school “N”, 30.8 % (Table 4).
Among 23 respondents who smoke, 17 of them (73.9 %) had father who smoked. There was a tendency for respondents who smoke to act as the parents (father) behave. But statistically (Chi-square test) it did not show significancy (p = 0.604). It meant that there was no significant relationship between smoking behavior of respondents with smoking behavior of parents. In other words, the appearance of parents who smoke in the smoker the respondent is only by chance (Table 5).
Among 23 respondents who smoke, 7 of them (30.4 %) had other family members who live at home did smoke. There was no significant relationship between smoking behavior, smoking behavior of respondents with family members (p = 0.578). It meant that there was no significant relationship between the smoking behavior of respondents with smoking behavior of other family members. In other words, the appearance of other family members who smoke in smokers respondents was only by chance (Table 5). From 23 respondents who smoke, 20 of them (87 %) had individuals who smoke (father/mother/other family members) at home (Table 6).
Discussion
Subjects were selected because they needed special attention, for entering the changing of new environment, from elementary school to high school, the support for adapting and the search for identity. They tried to learn to be away from their parents and had a strong emotional bond with peers and preffered to try new things [9].
Respondents who smoke were 23 respondents (29.3 %). The result was smaller than other research findings in Bantul, Yogyakarta Province (50 % in 2012) [2]; in Semarang, Central Java Province (69.15 % in 2013) [10]. Based on the study in 2016 at one of the public junior high school in Bantul, the result showed that the male student of grade 8 (14–15 years old), 20 out of 32 students (62.5 %), had admitted to smoking (including trial smoker and habit smokers) [11]. The difference results of this research with other research lies in the age of the respondents. Respondents of this study were grade 7 students or equivalent to aged 12–13 years old, while other studies accessed respondents grade 8 and 9 students or the equivalent to aged 14–15 years old.
If the respondents have known a cigarette at the age of 12 years, it meant that they smoke at an early age (early initiation). Smokers, who knew cigarettes earlier, had a higher mortality risk than those who exposed later (late initiation), especially for those with low socio-economic status [12].
Percentage of respondents who smoke on male students (16.66 %) was higher than female students (12.82 %). Female respondents who smoke in Jayapura was quite high compared to other study in the district of Bantul, which is only 4.78 % of the female grade 9 students. It can be predicted that the percentage of female students smoke in Jayapura will be higher, when they were at grade 9.
The same pattern of different percentage of male smokers and young female in teenagers (junior high students), as in adult smokers, also reported. For adult smokers, it was reported that the frequency and intensity of use of cigarettes and khat (Catha edulis) in Yemen male smokers is higher than the female [13].
The average score of respondents knowledge of the dangers of smoking was 60.81 (the maximum score of 100). This score was lower than the average score of students with the same grade levels and using the same instrument conducted in Yogyakarta (72.185) [14]. This might be possible because of learning environment differences between the students in Yogyakarta and Jayapura. It is generally known that Yogyakarta is a city with iconic “student city”. There was no statistical relationship in smoking behavior between the respondent and the score of students knowledge about smoking and its dangers.
According to LW Green, one behavior determinant is predesposing factor such as knowledge. But there are still two other determinants besides predesposing, that was anabling factor and re-inforcing factor. Among respondents who smoke, 73.9 % of them had parents who smoke and 25.64 % of them have other family members who also smoke. If calculated altogether between parents and other relatives who smoke (who live with the respondent), it showed that 87 % of teenage smokers had individuals at home who smoke. Parents and other relatives who live together at home who smoke is a supporting factor (re-inforcing factor) that may affect the respondents smoking behavior. Considering that there are individuals who smoke at home, it is easy for respondents to get cigarettes from their home environment. This is an anabling factor and can influence the respondents smoking behavior [15]. According to Rigotti [16], the availability of cigarettes at home, derived from a parent, close friend, or other family member can be referred to as noncomercial sources. In addition, it can be explained by the concept of LW. Green that the respondent smoking behavior can also be explained by the Social Learning Theory: individual will act after seeing other people behave [15]. Respondent smoking behavior might be influenced by their parents or other members smoking behavior.
This study was used a self Reported questionair instruments so that data on smoking behavior was likely not stated honestly. In addition, the limited number of respondents influence the results of the data analysis.
Conclusions and Recommendations
Teenagers smoking behavior in Jayapura Papua has not been concerning (29.3 % of the 78 grade 7 students, aged 11–14 years). From the smokers percentage, male was higher than female. The highest percentage of teenage smokers was at the age of 12 years old.
The knowledge score about the dangers of smoking was low, average score 60.81 out of 100. There was no relationship between teenagers knowledge about the dangers of smoking and teenagers smoking behavior.
There was 69.23 % parents and 25.6 % other family members who smoke. There was no relationship between teenagers smoking behavior and parents or other family members smoking behavior. Among teenagers who smoke, the majority (87 %) had individuals who smoke at their home.
The results of this study can be used as an input for health policy makers in particulary to health promotion for young people in terms of prevention of early smoking behavior (early initiation) either through cooperation with educational institutions or health centers with agitation Clean and Healthy Lifestyle Behaviour (PHBS) implementation.
References
Nasional, B. N. (2009). Pencegahan Penyalahgunaan Narkoba. Jakarta: Badan Narkotika Nasional Pusat Pencegahan Lakhar.
Astuti, K. (2012). Gambaran Perilaku Merokok Pada Remaja di Kabupaten Bantul. Insight, 25(1), 77–87.
Promkes, P. (2012). Masalah Merokok di Indonesia. Jakarta: Pusat Promkes.
Han, B., Compton, W. M., & Blanco, C. (2016). Tobacco use and 12-month suicidality among adults in the United States. Nicotine & Tobacco Research. doi:10.1093/ntr/ntw136.
Kesehatan, K. (2010). Keputusan Kemenkes RI nomor 1529/Kemenkes/SK/X/2010 tentang Pedoman umum pengembangan desa dan kelutahan siaga aktif. Indonesia. Jakarta: Pusat Promosi Kesehatan, Sekjen Kemenkes RI.
Kesehatan, B. P. dan P. K. K. (2013). Penyajian Pokok-pokok Hasil Riset Kesehatan Dasar. Jakarta.
Kesehatan, K. (2013). Penyajian Pokok-pokok Hasil Riskesdas 2013. Jakarta.
Papua, T. A. (2016). Apa yang dilakukan Gubernur demi penyelamatan generasi muda Papua ke depan. Jayapura.
Soetjiningsih, S. (2004). Tumbuh Kembang Remaja dan Permasalahannya. Jakarta: Sagung Seto.
Metanorani, F. (2013). Pola perilaku merokok anak jalanan Kota Semarang. Semarang: Universitas Muhammadiyah Semarang.
Herawati, L. (2016). Model Parent Educator pada Pencegahan Perilaku Merokok Remaja Bantul Propinsi Daerah Istimewa Yogyakarta.
Williams, R. (2003). Parental awereness of adolescent substance use. Addictive Behaviors, 28(4), 803–809.
Bobrova, N., West, R., Malyutina, D., & Malyutina, S. B. M. (2010). Gender differences in drinking practices in middle aged and older Russians. Alcohol and Alcoholism, 45(6), 573–580.
Herawati, L., & Haryono, W. (2014). Model pencegahan dini perilaku merokok, minum alkohol, dan narkoba pada remaja. Yogyakarta.
Green, L. W., & Ottoson, J. A. (2006). Frame for planing ang evaluation: Precede-procede evolution and application of the model (10th ed.). Montreal, Quebec: In ans journees de sante publique.
Rigotti, N. A. (1999). Youth access to tobacco. Nicotine & Tobacco Research, 1(Suppl 2), 893–897.
Acknowledgments
This Study was funded by Ministry of Health Republic of Indonesia.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Herawati, L., Budiman, J.A., Haryono, W. et al. Jayapura Teenagers Smoking Behavior. J Community Health 42, 78–82 (2017). https://doi.org/10.1007/s10900-016-0232-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10900-016-0232-4