
Abstract
Despite evidence that food insecurity negatively impacts child health, health care providers play little role in addressing the issue. To inform potential primary care interventions, we sought to assess a range of challenges faced by food insecure (FI) families coming to an urban, pediatric primary care setting. A cross-sectional study was performed at a hospital-based, urban, academic pediatric primary care clinic that serves as a medical home for approximately 15,000 patients with 35,000 annual visits. Subjects included a convenience sample of caregivers of children presenting for either well child or ill care over a 4 months period in 2012. A self-administered survey assessed household food security status, shopping habits, transportation access, budgeting priorities, and perceptions about nutrition access in one’s community. Bivariate analyses between food security status and these characteristics were performed using Chi square statistics or Fisher’s exact test. The survey was completed by 199 caregivers. Approximately 33 % of families were FI; 93 % received food-related governmental assistance. FI families were more likely to obtain food from a corner/convenience store, utilize food banks, require transportation other than a household car, and prioritize paying bills before purchasing food. FI families perceived less access to healthy, affordable foods within their community. Thus, FI families may face unique barriers to accessing food. Knowledge of these barriers could allow clinicians to tailor in-clinic screening and create family-centered interventions.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Food security is defined by the US Department of Agriculture (USDA) as “access by all people at all times to enough food for an active, healthy life.”[1] In 2011, 20.6 % of households with children in the United States experienced food insecurity at some point in the preceding year [2]. Childhood food insecurity has been associated with negative health and development outcomes including more frequent common illnesses [3], iron-deficiency anemia [4], overweight or obese status [5, 6], increased likelihood of hospitalization [7], increased risk of developmental delays [8], and lower physical and psychosocial functioning [9].
Food insecurity is primarily driven by financial constraints, and although participation in food benefit programs such as the Supplemental Nutritional Assistance Program (SNAP), Special Supplemental Nutrition Program for Women, Infants and Children (WIC), and National School Lunch Program (NSLP) provides some relief, studies have shown that participation does not eradicate the problem [10–12.] While financial constraints directly affect food purchasing power, related constraints and barriers may also affect access to affordable, high-quality food. As a result, food insecure (FI) families often rely on inexpensive, energy dense foods and have lower consumption of fresh fruits and vegetables overall [13–15.]
Few studies have assessed the different challenges faced by FI and food secure (FS) families in providing adequate nutrition and none, to our knowledge, have examined them in the context of a pediatric primary care (PPC) encounter. This study aimed to compare characteristics of FI and FS populations and describe barriers to accessing healthy food for FI families within one PPC center. Specifically, we sought to better understand where FI families obtain food, modes of transportation used to access food, budgeting priorities, and perceptions about the food environment in one’s community. A better understanding of such characteristics could help to improve strategies to identify FI families and create or modify interventions in a way that is more tailored to the specific barrier or need that is faced.
Methods
Study Design and Data Collection
A cross-sectional study was performed at the PPC Center, a hospital-based, urban, academic PPC clinic that serves as a medical home for approximately 15,000 patients with 35,000 visits annually. A convenience sample of caregivers of children present for either well child or ill care completed a self-administered survey over a 4 months period in 2012. Participation was voluntary, and all English-speaking caregivers were eligible. The study was limited to English-speaking caregivers; <3 % of the clinic’s population was excluded as a result. Patient demographic information including age, gender, race, and insurance status was extracted from the electronic medical record, Epic (Epic Systems Corporation, Verona, Wisconsin). The study was reviewed by the Cincinnati Children’s Hospital Medical Center Institutional Review Board and determined to be exempt.
Survey Development
A 43-question survey was developed to assess food security status, access to food stores, and perceived barriers to obtaining food for one’s household. Initial survey questions addressed demographic information. Caregivers completing the survey were queried on their relationship to the patient being seen, their age, the number of children and adults living within their household, their educational attainment, and whether their child or household received governmental benefits through SNAP, WIC, or NSLP. The survey included 11 questions from the USDA’s Food Security Core-Module Questionnaire, including the standard 6-item indicator set for classifying households by food-security-status-level [1.] Consistent with the USDA’s classification criteria using the standard 6-item indicator set, we classified a household as having “low” food security if the respondent answered in the affirmative to 2–4 of the 6 questions, while households with affirmative answers to 5–6 of the questions were classified as having “very low” food security. Households with “low” and “very low” food security were grouped together and were defined as FI.
The next section of the survey focused on food shopping habits and barriers to accessing food using a set of questions developed de novo. Participants were asked where they obtained their household’s food; response options included supermarket chain, wholesale chain, small neighborhood grocery store, corner/convenience store, food bank/pantry, or other. They were first asked to select all places from which they obtain food and then to select the one place from which they get the majority of their household’s food. Participants’ reasons for choosing a particular food store were assessed and options included proximity to home, accessible to the bus line, convenience, low cost, wide variety, or other. Survey respondents were then asked about the mode of transportation used to get to their chosen food store with possible answers including household car, a car borrowed from family/friend/neighbor, a ride from family/friend/neighbor, the bus, walking, a taxi, or other. They were also asked the amount of time required to travel to the food store, and how frequently they go to the store for food. To gauge participants’ level of support and connectedness and coping strategies they were asked whether they had family and/or friends that they could count on to feed their family for a day. Participants were also asked about their household budgeting strategies and priorities (i.e., places where they spend their money first, such as on food, rent, utilities, etc.).
The survey’s final section addressed the participant’s perceptions about the food environment within their community using previously developed questions [16]. The food environment was assessed through availability of fresh and canned fruits and vegetables, and perceived hunger within the community. Potential barriers to getting desired food included transportation, number of stores, affordable healthy choices, and crime. Each question in this section used a 5-point Likert-based response scale where 1 indicated strong disagreement and 5 strong agreement.
Analysis
Descriptive statistics were used to report baseline sample characteristics as well as prevalence of USDA-defined household food insecurity. Bivariate analysis of food security status and food shopping habits, barriers to accessing food, and respondent’s perception of their community’s food environment were performed. Associations were assessed using Chi square statistics or Fisher’s exact test.
Analyses were performed using SAS statistical software (version 9.3, Cary, NC). Survey data was captured using Research Electronic Data Capture (REDCap), a secure, web-based application [17].
Results
A total of 247 caregivers were approached and 200 (81 %) completed the survey. One caregiver completed two surveys during two separate clinic visits, and the second survey was excluded from our analysis making the total number of completed surveys used for analysis 199. The median caregiver age was 27 years [interquartile range (IQR) 23–32]. The children of the caregivers were 56 % male, 74 % African American, and 22 % Caucasian with a median patient age of 2.1 years (IQR 0.6–6.2) (Table 1). Eighty-nine percent of children were publicly insured. A total of 73 % received SNAP, 59 % received WIC, and 58 % received NSLP. Children for whom surveys were completed were demographically equivalent to the patient population cared for at the PPC clinic.
Thirty-three percent of caregivers lived in households classified as FI. Caregivers in FI households were significantly more likely to report that there was at least 1 day in the past 30 days when their household did not have enough food to make a meal and did not have money or governmental benefits to buy food (Table 2). Additionally, caregivers in FI households were more likely to report, compared to those in FS households, that at some point in the last year their children were not eating enough food (53 vs. 8 %, p < 0.0001) and that some went an entire day without eating (6 vs. 0 %, p = 0.01) because there was not enough money to buy food. They were also significantly more likely to rely on low-cost food to feed their children (69 vs. 14 %, p < 0.0001).
Food shopping habits and transportation modes differed significantly between FI and FS households. While the majority of caregivers (97 %) reported primarily shopping for food at a supermarket, FI households, compared to FS households, were more likely to buy some portion of the household’s food from a convenience/corner store and get food from a food bank four or more times per year (Table 3). Additionally, caregivers from FI households were significantly more likely to use transportation other than a household car to get to the supermarket and report that transportation was a barrier to eating healthy. Although it did not reach statistical significance, shoppers in FI households were more likely to travel more than 15 min to the food store (p = 0.14).
Purchasing food was not always the first priority for FI household budgets; when money was limited, paying rent/mortgage, utilities, transportation costs, and phone service were often of higher priority (Table 3). Budgeting concerns involving food purchases were much more common in FI households compared to FS households (70 vs. 18 %, p < 0.0001). Twenty-five percent of caregivers in FI households, compared to 4 % in FS households, reported that there was nobody that they could count on to feed their family for a day if they ran out of food (p < 0.0001).
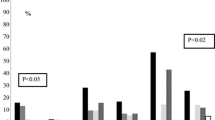
Perceptions of the food environment in one’s community varied between caregivers of FI and FS households. A significantly higher percentage of caregivers in FI households did not believe there were enough food stores, did not feel that they are able to get the types of food they wanted, and felt that healthy food choices were not affordable in their community (Table 3). Respondents from both FI and FS households believed people in their community were going hungry.
Discussion
Food insecurity is widespread in the United States despite its known detrimental impact on child health and development. One-third of households in our PPC clinic were FI, higher than the national average, despite the fact that 93 % of the entire population received at least one form of governmental assistance related to food (SNAP, WIC, NSLP). A better understanding of barriers and challenges faced by FI families could help to inform and tailor screening and intervention practices in PPC clinics such as our own.
Caregivers in FI households face many challenges trying to provide nutritious food for their family. While the vast majority of caregivers (97 %) primarily purchased food from a supermarket, FI families were more likely to utilize other sources of food such as convenience/corner stores and food banks. Convenience stores may be more readily available to residents in urban neighborhoods than supermarkets [18–20], but they typically have higher prices [20] and do not routinely stock healthy foods such as fresh fruits and vegetables [19–23]. Increasing the variety of fruits and vegetables available at a convenience store increased the odds that FI and low-income customers actually purchased such fresh produce [24]. Recognizing where families obtain food and acquiring knowledge about the quality of food available for purchase could be an opportunity for both in-clinic assessments as well as community-level advocacy.
Transportation was a barrier to obtaining food for FI households. Our FI families were less likely than FS families to use a household car to get to the food store; instead they relied on public transportation, transportation from non-household members, taxis or walking. Families who depend on public transportation or others’ cars, either by borrowing or getting a ride, have less flexibility in choosing when and where they obtain food and the quantity and types of food they purchase during a shopping trip [11, 25]. Without a household car, families may need to time shopping trips, either based on availability of a ride or the timing of public transportation, which may be an inconvenience. Although one may schedule a more convenient shopping trip by paying for a taxi, the expense of such a trip likely makes it impractical for most families. Walking to the store may be a convenient option for those who live close to the food store but limits the amount one may purchase.
The limited flexibility associated with transportation difficulties can be problematic for a family trying to maximize their food purchasing power by shopping at stores with less expensive, high-quality food. Often, the store with the best prices or most variety is not the one closest to home, and with inflexible transportation, a family may be forced to make sub-optimal food purchasing choices [25]. For example, a shopper who is dependent on someone else’s car or a taxi may make infrequent trips to the store and be forced to buy in bulk; this pattern, while likely less expensive may limit the amount of fresh produce purchased to avoid food spoiling. Alternatively, someone who relies on public transportation or walking may shop more frequently due to limited carrying capacity; this shopper may be more likely to buy fresh produce but is also likely to pay higher unit costs [25] and spend more money overall. Knowledge of where families shop and their mode of transportation could therefore be relevant to in-clinic guidance. This may also represent an area in which pediatricians can serve as advocates, influencing neighborhood development and planning.
FI households must prioritize spending to make ends meet; other bills may take priority over buying food. In our study, rent/mortgage and utilities were the most common bills prioritized over purchasing food. Others have shown that the odds of food insecurity increase for families with housing costs >30 % of their income [26]. For some, food spending may fall below the cost of a basic nutritious diet as housing costs rise [27]. Additionally, as utility costs vary with the season, so do food expenditures for low-income households. Low-income families reduce their food expenditures by approximately the same amount that they increase fuel expenditures during cold-weather months, the “heat or eat” phenomenon [28]. It is important for clinicians to consider such variations in spending and screen accordingly, maximizing the opportunity to connect families with pertinent resources.
Caregivers in FI households have different perceptions of their own community than those in FS households. FI caregivers were twice as likely to report not having enough food stores in their community and three times more likely to report that they could not get the food they want in their community. Interestingly, it is debatable whether better physical access to food can alleviate food insecurity for families with resource constraints [29]. Kirkpatrick and Tarasuk found no association between families living within 2 km of a supermarket and whether they were FI. Overall, our survey respondents recognized that hunger was an issue within their community, a perception that did not differ significantly between FI and FS respondents.
There were limitations to our study. First, this was a convenience sample of English-speaking caregivers. Given a similar demographic profile to the clinic population as a whole, and given that non-English speakers make up <3 % of our clinic population, we do not expect it to have greatly impacted our results. Second, this survey was conducted at a single clinic site with a modest sample size, making it less generalizable. Third, given its cross-sectional design, we cannot conclude that the barriers identified caused the food insecurity. Finally, this study demonstrates reported food shopping habits and not actual purchases. Therefore, we cannot make conclusions on the nutritional quality of food actually procured.
As we better understand how FI and FS households differ, it is imperative for clinicians to enhance screening practices to both identify food insecurity and elicit specific barriers. Clinicians then need to have on hand clinic- and community-based resources aimed at improving food access. They may benefit from strengthened partnerships with and/or knowledge of community organizations poised to intervene (e.g., food banks, neighborhood-based farmers’ markets, community gardens, etc.) [30–32]. Clinicians could also engage in community-level advocacy aimed at enhancing convenient and effective public transportation that may benefit their patient population.
Conclusions
Families in our urban, underserved PPC clinic were more likely to be FI than the national average despite the vast majority receiving food-related public benefits. FI households in this urban PPC population face a unique set of barriers to accessing nutritious food that include limited access to transportation, financial constraints related to paying bills, and perceived impediments within their community’s food environment. Knowledge of such barriers could allow clinicians to improve screening and create family-centered interventions in ways that more effectively meet individual patient and family needs.
Abbreviations
- FI:
-
Food insecure
- USDA:
-
US Department of Agriculture
- WIC:
-
Special Supplement Nutrition Program for Women Infants Children
- SNAP:
-
Supplemental Nutrition Assistance Program
- NSLP:
-
National School Lunch Program
- FS:
-
Food secure
- PPC:
-
Pediatric primary care
- IQR:
-
Interquartile range
References
Bickel, G., Nord, M., Price, C., Hamilton, W., Cook, J. (2000). Guide to measuring household food security. Revised 2000. Alexandria, VA: Office of Analysis, Nutrition, and Evaluation, Food and Nutritoin Service, US Department of Agriculture.
Coleman-Jensen, A., Nord, M., Andrews, M., Carlson, S. (2012). Household Food Security in the United States in 2011. US Department of Agriculture, Economic Research Service. Contract No.: ERR-141.
Alaimo, K., Olson, C. M., Frongillo, E. A., Jr, & Briefel, R. R. (2001). Food insufficiency, family income, and health in US preschool and school-aged children. American Journal of Public Health, 91(5), 781–786.
Skalicky, A., Meyers, A. F., Adams, W. G., Yang, Z., Cook, J. T., & Frank, D. A. (2006). Child food insecurity and iron deficiency anemia in low-income infants and toddlers in the United States. Maternal and Child Health Journal, 10(2), 177–185.
Casey, P. H., Simpson, P. M., Gossett, J. M., et al. (2006). The association of child and household food insecurity with childhood overweight status. Pediatrics, 118(5), e1406–e1413.
Metallinos-Katsaras, E., Must, A., & Gorman, K. (2012). A longitudinal study of food insecurity on obesity in preschool children. Journal of the Academy of Nutrition and Dietetics, 112(12), 1949–1958.
Cook, J. T., Frank, D. A., Berkowitz, C., et al. (2004). Food insecurity is associated with adverse health outcomes among human infants and toddlers. The Journal of nutrition, 134(6), 1432–1438.
Rose-Jacobs, R., Black, M. M., Casey, P. H., et al. (2008). Household food insecurity: associations with at-risk infant and toddler development. Pediatrics, 121(1), 65–72.
Casey, P. H., Szeto, K. L., Robbins, J. M., et al. (2005). Child health-related quality of life and household food security. Archives of Pediatrics and Adolescent Medicine, 159(1), 51–56.
Richards, R., & Smith, C. (2006). Shelter environment and placement in community affects lifestyle factors among homeless families in Minnesota. American journal of health promotion, 21(1), 36–44.
Wiig, K., & Smith, C. (2009). The art of grocery shopping on a food stamp budget: factors influencing the food choices of low-income women as they try to make ends meet. Public health nutrition, 12(10), 1726–1734.
Nord, M., & Romig, K. (2006). Hunger in the summer: seasonal food insecurity and the National School Lunch and Summer Food Service programs. Journal of Children and Poverty, 12(2), 141–158.
Kendall, A., Olson, C. M., & Frongillo, E. A., Jr. (1996). Relationship of hunger and food insecurity to food availability and consumption. Journal of the American Dietetic Association, 96(10), 1019–1024.
Leung, C. W., Ding, E. L., Catalano, P. J., Villamor, E., Rimm, E. B., & Willett, W. C. (2012). Dietary intake and dietary quality of low-income adults in the Supplemental Nutrition Assistance Program. The American journal of clinical nutrition, 96(5), 977–988.
Rose, D. (1999). Economic determinants and dietary consequences of food insecurity in the United States. The Journal of nutrition, 129(2), 517S–520S.
Hendrickson, D. S. C., & Eikenberry, N. (2006). Fruit and vegetable access in four low-income food deserts communities in Minnesota. Agriculture and Human Values, 23, 371–383.
Harris, P. A., Taylor, R., Thielke, R., Payne, J., Gonzalez, N., & Conde, J. G. (2009). Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. Journal of Biomedical Informatics, 42(2), 377–381.
Powell, L. M., Slater, S., Mirtcheva, D., Bao, Y., & Chaloupka, F. J. (2007). Food store availability and neighborhood characteristics in the United States. Preventive Medicine, 44(3), 189–195.
Sloane, D. C., Diamant, A. L., Lewis, L. B., et al. (2003). Improving the nutritional resource environment for healthy living through community-based participatory research. Journal of General Internal Medicine, 18(7), 568–575.
Chung, C., & Myers, S. L. (1999). Do the poor pay more for food? An analysis of grocery store availability and food price disparities. Journal of consumer affairs, 33(2), 276–296.
Andreyeva, T., Middleton, A. E., Long, M. W., Luedicke, J., & Schwartz, M. B. (2011). Food retailer practices, attitudes and beliefs about the supply of healthy foods. Public health nutrition, 14(6), 1024–1031.
O’Malley, K., Gustat, J., Rice, J., Johnson, C. C. (2013). Feasibility of increasing access to healthy foods in neighborhood corner stores. Journal of community health. Epub 2013/04/03.
Sharkey, J. R., Dean, W. R., & Nalty, C. (2012). Convenience stores and the marketing of foods and beverages through product assortment. American Journal of Preventive Medicine, 43(3 Suppl 2), S109–S115.
Martin, K. S., Havens, E., Boyle, K. E., et al. (2012). If you stock it, will they buy it? Healthy food availability and customer purchasing behaviour within corner stores in Hartford, CT. USA. Public health nutrition, 15(10), 1973–1978.
Clifton, K. (2004). Mobility strategies and food shopping fo low-income families: A case study. Journal of Planning Education and Research, 23(402), 402–413.
Kirkpatrick, S. I., & Tarasuk, V. (2011). Housing circumstances are associated with household food access among low-income urban families. Journal of urban health, 88(2), 284–296.
Kirkpatrick, S. I., & Tarasuk, V. (2007). Adequacy of food spending is related to housing expenditures among lower-income Canadian households. Public health nutrition, 10(12), 1464–1473.
Bhattacharya, J., DeLeire, T., Haider, S., & Currie, J. (2003). Heat or eat? Cold-weather shocks and nutrition in poor American families. American Journal of Public Health, 93(7), 1149–1154.
Kirkpatrick, S. I., & Tarasuk, V. (2010). Assessing the relevance of neighbourhood characteristics to the household food security of low-income Toronto families. Public health nutrition, 13(7), 1139–1148.
Jones, P., & Bhatia, R. (2011). Supporting equitable food systems through food assistance at farmers’ markets. American Journal of Public Health, 101(5), 781–783.
George, D. R., Kraschnewski, J. L., & Rovniak, L. S. (2011). Public health potential of farmers’ markets on medical center campuses: A case study from Penn State Milton S. Hershey medical center. American Journal of Public Health, 101(12), 2226–2232.
Carney, P. A., Hamada, J. L., Rdesinski, R., et al. (2012). Impact of a community gardening project on vegetable intake, food security and family relationships: A community-based participatory research study. Journal of Community Health, 37(4), 874–881.
Acknowledgments
The authors would like to thank Angela Howald for her help with data collection. This project was supported by funds from the Bureau of Health Professions (BHPr), Health Resources and Services Administration (HRSA), Department of Health and Human Services (DHHS), under the CCHMC NRSA Primary Care Research Fellowship in Child and Adolescent Health (T32HP10027). The information or content and conclusions are those of the authors and should not be construed as the official position or policy of, nor should any endorsements be inferred by the BHPR, HRSA, DHHS or the US Government (DeMartini). Dr. Beck is supported by the Cincinnati Children’s Hospital Medical Center Procter Scholar Award. The authors have no conflicts of interest or financial relationships to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
DeMartini, T.L., Beck, A.F., Kahn, R.S. et al. Food Insecure Families: Description of Access and Barriers to Food from one Pediatric Primary Care Center. J Community Health 38, 1182–1187 (2013). https://doi.org/10.1007/s10900-013-9731-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10900-013-9731-8