
Abstract
We tested the hypothesis that living near a walking or cycling trail was associated with greater odds of walking. This has been previously studied in healthy and unselected populations, but to our knowledge has not been studied in patients attending community clinics. A cross-sectional survey was completed by 1211 persons in five community clinics that serve poor populations. We performed univariate analysis and developed a multivariate logistic regression model for walking adjusting for 12 independent variables including self-rated health, frequent mental distress, lifestyle and demographic variables, and environmental characteristics of the neighborhood including perceived proximity to a walking or cycling trail. Compared to those who reported not living close to a trail, persons who reported living near a trail were more likely to meet recommended levels of walking of at least 30 minutes fives times per week (unadjusted odds ratio = 1.49, 95% confidence intervals = 1.04–2.13). In the multivariate model, male gender (unadjusted odds ratio = 1.63, 95% confidence intervals = 1.15–2.30), having three or more convenient destinations (unadjusted odds ratio = 1.78, 95% confidence intervals = 1.37–2.32), and living near a trail (unadjusted odds ratio = 1.45, 95% confidence intervals = 1.01–2.09) were positively associated with walking at statistically significant levels. The odds of walking were lower in non-Hispanic blacks (odds ratio = 0.59, 95% confidence intervals = 0.40–0.87) and current smokers (odds ratio = 0.66, 95% confidence intervals = 0.57–0.76). For patients attending community clinics, environmental strategies to encourage walking may include mixed-land-use neighborhoods and construction of trails.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Researchers have demonstrated an increasing interest in the effects of a neighborhood’s environmental characteristics on walking by the neighborhood’s residents1. Recent reviews have emphasized that the study of this issue is in its infancy, and much more study is needed to understand this relationship.1–6 Walking is recommended for the prevention and treatment of many common conditions including hypertension, diabetes, coronary heart disease, stroke, osteoporosis, colon cancer, breast cancer and, among older adults, fall-related injuries.7,8 Neighborhood environmental characteristics that encourage walking might result in better health and provide population-based strategies for health promotion.
Public health and transportation experts have postulated that establishing walking trails is a cost-effective way to promote walking.9,10 Among healthy community residents some studies have established an association between walking and living in proximity to a trail.11–17 Other studies have failed to find such an association.18,19 Persons living close to a trail are more likely to use them than persons who live further away.14,18 However, the use and awareness of neighborhood trails is low.20,21
We previously examined the relationship of neighborhood walkability to self-rated health in persons attending community clinics, and demonstrated that persons who perceived that they had no walking destinations were significantly less healthy than persons who perceived that they had five or more places to walk.22 The present study was designed to examine the association of certain neighborhood environmental characteristics, including perceived proximity to a trail, and walking by patients attending community clinics. Patients attending these clinics are the type of high-risk persons who are most likely to benefit from regular walking. We believe that this is the first study to examine walking and neighborhood environmental characteristics in such a population.
Methods
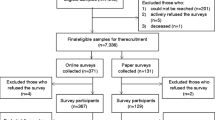
We used a cross-sectional survey to test the hypothesis that patients who walked perceived that they lived close to a walking or cycling trail, and that this effect was independent of their health, mental health, demographic characteristics, lifestyle habits and other neighborhood environmental characteristics that might predict walking. The sample population was drawn from five community clinics that primarily serve low-income and underserved populations. Patients were asked to complete a survey and drop it into a box. Participation was voluntary. Persons under age 18 were excluded. This study was begun in January 13, 2005, and completed April 27, 2005. Completed survey forms were received from a total of 1237 persons. Complete information was obtained from 1211 subjects and this was the group used in the analysis. The study was granted exempt status by the Institutional Review Board of the Texas Tech University Health Sciences Center.
Clinic 1 is a university-based family medicine clinic providing a full range of primary care services to cross-generational patients. It is staffed by family medicine physicians and residents. Census was approximately 85 patients daily, of which, less than 5% were non-English speaking. Approximately 38% of these patients are uninsured or are covered by Medicaid. Clinic 2 serves women and children, providing obstetrical, well care (including immunizations), and acute care services to a targeted high-risk, low socioeconomic population. Approximately 80% of these patients are uninsured or are covered by Medicaid. It is staffed by pediatric and OB-GYN physicians and residents. Approximately 30% of the clinic patients do not speak English. Clinic 3 provides primary care services to a population of indigent adults meeting residential and income screening requirements (no private insurance and income less than 135% of the federal poverty level). Eighty-three percent of the respondents at this clinic reported they were uninsured or had Medicaid. It is staffed by internal medicine physicians and residents. Clinic 4 was a general medical clinic at the local Veterans Affairs Medical Center (VAMC). This clinic is staffed by staff physicians, nurse practitioners, and physicians assistants employed by the VAMC. Approximately 53% of these patients have either Medicaid or the VAMC as their primary health care payor. Clinic 5 (Planned Parenthood Clinic) targets young adults and provides education, prevention and clinical services for contraception and treatment of sexually transmitted disease in addition to some midlife and pediatric services. Eighty – seven percent (87%) of respondents reported no insurance or Medicaid as their health care payor.
The dependant variable in this study was walking. Subjects were asked to list the number of times in the past week that they had walked for at least 30 minutes. The variable was coded on an ordinal scale: none, one-three times, and four or more times. Patients walking one-three times or four or more times were compared to those who did not walk at least once.
We adjusted the association between walking and living near a trail for twelve independent variables that included self-rated health, frequent mental distress, lifestyle and demographic variables, and other environmental characteristics of the neighborhood where they lived. Patients were asked to rate their own health (self-rated health) by answering whether in general they would say their health was excellent, very good, good, fair or poor. Excellent, very good, and good responses were combined to form a category called “good health” while fair and poor comprised “poor health”. Patients also rated their own mental health with a question that asked, “Now thinking about your mental health, which includes stress, depression, and problems with emotions, for how many days during the past 30 days was your mental health not good?” Patients who reported 14 or more days were classified as having frequent mental distress and those with less than 14 were classified as not having frequent mental distress.
Demographic characteristics and lifestyle variables were also used to adjust for the associations between perceived walking and living near a trail. Lifestyle variables included current smoking status (zero cigarettes on a typical day vs. any cigarettes smoked on a typical day) and obesity (yes vs. no). Obesity was defined as body mass index (BMI) equal to or more than 30. BMI was computed from self-reported height and weight. Demographic variables were race/ethnicity (Hispanic, non-Hispanic white, non-Hispanic black, non-Hispanic other), gender, age category (18–24, 25–34, 35–44, 45–54, 55 and older), and highest level of education achieved (less than high school, high school graduation or graduate equivalent degree, some college, or four-year college degree).
Leyden’s scale of walkability was modified for this population as described in our previous study.22 Persons who perceived that there were no convenient destinations were designated as living in neighborhood with poor walkability, whereas persons who perceived that there were one or more convenient destinations were designated as living a neighborhood with good walkability. The other neighborhood environmental characteristics that was tested was whether or not they perceived their neighbor as safe (“extremely safe” or “quite safe” considered yes, and “slightly safe” or “not at all safe” considered no).
Chi square tests were performed to test for any unadjusted associations between walking and each categorical independent variable. Since the outcome variable was ordered in scale, multivariate ordered logistic regression modeling was employed to determine if associations between perceived walkability and living near a trail remained significant after adjustment for the independent variables. Since the patient population was clustered in clinics, we adjusted the standard errors for intragroup correlation in the multivariate logistic regression analysis. Adjusted odds ratios and 95% confidence intervals were calculated for each independent variable. For the multivariate model, we used only those surveys where every item had been completed. Statistical analysis was performed using STATA® statistical software (Version 8.2).
Results
A total of 1851 surveys were distributed of which 1237 were returned for an overall response rate of 66.8%. Of these, 1211 met the eligibility criteria for inclusion in the final analysis. There was a wide variation in response rates between clinics and ranged from as low as 37.8% for clinic 3 to as high as 89.8% for clinic 2 (Table 1).
Of patients completing each respective item, 67.2% were female and 68.9% reported their ethnicity as non-Hispanic white. Other ethnicities reported were Hispanic (22.5%), non-Hispanic black (6.1%), and non-Hispanic other (2.5%). Nearly half (48.8%) were under age 35, and 29.3% were over 54 years of age. With regard to education, 16% had less than a high school education, 33.8% had a high school education or graduate equivalent degree, and 9.6% had a college degree. Over one-third (34.3%) reported their overall health as poor or fair, and 23.2% reported frequent mental distress (14 or more days in the past month with mental health was not good). Self reported obesity (BMI greater or equal to 30) rate was 32.1%, and 26.9% of responders reported that they were current smokers.
Using walking as the dependent variable, univariate analysis for twelve independent variables is shown in Table 2. Significance at the p < 0.05 level was demonstrated for living near a trail and five other independent variables: self-rated health, frequent mental distress, obesity, walking destinations and current smoking status. Perceived proximity to a trail was correlated with walking in the univariate analysis. Persons who perceived that they lived near a trail engaged in higher frequencies of walking at least thirty minutes in the past week (Table 3). Compared to those who reported not living close to a trail, persons who reported living close to a trail were more likely to meet recommended levels of walking of at least 30 minutes five days per week (65/435 vs. 71/670, unadjusted odds ratio = 1.49, 95% confidence intervals = 1.04 - 2.13) A higher percentage of persons who reported not living close to a trail were also sedentary (47.8% vs. 39.2%).
Results of the multivariate regression analysis, with adjusted odds ratios, are shown in Table 4. In the multivariate model, a clustering adjustment was made because samples were drawn from five different clinics. In the multivariate model, male gender, non-Hispanic Black race/ethnicity, walkability, living near a trail and smoking were statistically significantly associated with walking. The odds of walking were significantly lower for non-Hispanic Blacks (Adjusted odds ratio = 0.59, 95% confidence intervals = 0.40–0.87). Persons with frequent mental distress were significantly less likely to report one or more days of walking for at least 30 minutes in the unadjusted analysis only (Unadjusted odds ratio 0.63, 95% confidence intervals = 0.56 - 0.70). Persons who perceived three or more convenient destinations were more likely to report walking for at least 30 minutes (Adjusted odds ratio = 1.78, 95% confidence intervals = 1.37 – 2.32). The odds of walking were significantly lower for current smokers (Adjusted odds ratio = 0.66, 95% confidence intervals = 0.57–0.76).
Discussion
Our study examined the association of walking and various demographic, lifestyle, and neighborhood environmental characteristics in a group of community clinic patients. Previous studies have looked at this association in healthy or unselected populations.11–18 We believe that this is this first study to report such a relationship in a vulnerable population of patients using community clinics.
Many studies have demonstrated a high correlation between self-rated health and other measures of health.23–28 Since our patients had a high rate of poor self-rated health (34%) one would predict that this type of population is one that might benefit most from increased walking. Previous researchers have stated that population-based strategies should target these types of persons,29,30 and some have argued that to do so best serves the health of the entire population.31 In healthy and unselected populations, living near a trail has been associated with engaging in walking, meeting recommended levels of physical activity and less likelihood of being overweight.11–17, 32 Reed20 demonstrated that trail users are more likely women with higher education and more income. Our study demonstrates that that perceived proximity to a trail is associated with walking in patients attending community clinics, thus suggesting that these benefits extend to poor and vulnerable populations as well.
Our study also demonstrated that walkability and proximity to a city walking trail, but not neighborhood safety, were associated with increased walking in this community clinic population. Previous studies of walking and neighborhood safety by healthy persons have yielded conflicting results.33–37 Our study suggests that for community clinic patients, improving walkability and creating trails may be more successful in promoting walking than attempts to improve neighborhood safety.
Walkability (having more destinations available toward which to walk) also was significant in our study. This variable is at least as important as trails and suggests that zoning for mixed-use neighborhoods might be an efficient population-based strategy for cities to employ in their efforts to improve the health of vulnerable populations.
Our study has several limitations. Being a cross-sectional survey, it demonstrates associations and not does prove cause-and-effect. It is possible that persons interested in walking choose to live in walkable neighborhoods and near trails, and that these same persons would still walk even if they were forced to live in neighborhoods with low walkability and no trails. Several studies have demonstrated an association between walking and trails.11–17 We are aware of only one prospective study that examined walking before and after construction of a trail.21 This study did not demonstrate increased activity among residents living within two miles of a trail after its construction.21 Whether or not the same findings would occur among vulnerable populations is to our knowledge unknown. Gordon38 showed that the users of newly constructed trails are commonly new exercisers, and Brownson suggested that trails may be effective at reaching high risk sedentary populations.39 Like others,1, 4 we encourage researchers to look for opportunities to conduct such studies in their communities.
Our study is also limited by the fact that walkability and nearness to trails was self-reported and may not be accurate. Walkers might have been more aware of destinations because they walked in the neighborhood. Walkers might also judge proximity to a trail differently than non-walkers. However, recent studies have suggested that self-reported surveys of neighborhood environmental characteristics are reproducible and correlate with objective measurements of the neighborhood.14, 40–42
Conclusion
Many transportation and public health experts postulate that urban land design can provide important population-based strategies for promoting healthy behaviors such as walking.1–4 Our study adds evidence in support of this hypothesis. It also suggests that for community clinic patients with health problems and poor health behaviors, environmental strategies to encourage walking include zoning to promote mixed-land-use neighborhoods and construction of trails; and that these strategies may be more successful than attempts to improve neighborhood safety. Future research should address ways to increase the impact of trails on walking prevalence and frequency.
References
Committee on Physical Activity, Health, Transportation, and Land Use. Transportation Research Board, Institute of Medicine. Does the built environment influence physical activity? TRB Special Report 282. Washington, D.C.: National Academy of Sciences, 2005
McCormack G, Giles-Corti B, Lange A, Smith T, Martin K, Pikora TJ (2004) An update of the recent evidence of the relationship between objective and self-reported measures of the physical environment and physical activity behaviors. J Sci Med Sport 7(1 Suppl):81–92
Cunningham GO, Michael YL (2004) Concepts guiding the study of the impact of the built environment on physical activity for older adults: a review of the literature. Am J Health Promot 18:435–443
Sturm R (2005) Economics and physical activity: a research agenda. Am J Prev Med 28 (2 Suppl 2):141–149
Owen N, Humpel N, Leslie E, Bauman A, Sallis JF (2004) Understanding environmental influences on walking; review and research agenda. Am J Prev Med 27:67–76
Matson-Koffman DM, Brownstein JN, Neiner JA, Greaney ML (2005) A site-specific literature review of policy and environmental interventions that promote physical activity and nutrition for cardiovascular health: what works?. Am J Health Promot 19:167–193
U.S. Department of Health and Human Services. Physical Activity and Health. A Report of the Surgeon General. Washington DC; 1996
U. S. Department of Health and Human Services. Physical Activity: Fundamental to Preventing Disease. Office of the Assistant Secretary for Planning and Evaluation, Washington DC; 2002
Wang G, Macera C, Scuder-Soucie B, Schmid T, Pratt M, Buchner D (2004) Cost effectiveness of a bicycle/pedestrian trail development in health promotion. Prev Med 38:237–242
Wang G, Macera C, Scuder-Soucie B, Schmid T, Pratt M, Buchner D, et al. (2004) Cost analysis of the built environment: the case of bike and pedestrian trials in Lincoln, Neb. Am J Public Health 94:549–543
Huston SL, Evenson KR, Bors P, Gizlice Z. (2003) Neighborhood environment, access to places for activity, and leisure-time activity in a diverse North Carolina population. Am J Health Promot 18:58–69
Parks SE, Housemann RA, Brownson RC. (2003) Differential correlates of physical activity in urban and rural adults of various socioeconomic backgrounds in the United States. J Epidemiol Community Health 57:29–35
King WC, Brach JS, Belle S, Killingsworth R, Fenton M, Kriska AM (2003) The relationship between convenience of destinations and walking levels in older women. J Health Promot 18:74–82
Troped PJ, Saunders RP, Pate RR, Reininger B, Ureda JR, Thompson SJ (2001) Association between self-reported and objective physical environmental factors and use of a community rail-trail. Prev Med 32:191–200
Booth ML, Owen N, Bauman A, Clavisi O, Leslie E (2000) Social - cognitive and perceived environmental influences associated with physical activity in older Australians. Prev Med 31:15–22
Brownson RC, Baker EA, Housemann RA, Brennan LK, Bacak SJ (2001) Environmental and policy determinants of physical activity in the United States. Am J Public Health 91:1995–2003
Troped PJ, Saunders RP, Pate RR, Reininger B, Addy CL (2003) Correlates of recreational and transportation physical activity among adults in a New England community. Prev Med 37:304–310
Hoehner CM, Brennan Ramirez LK, Elliott MB, Handy SL, Brownson RC (2005) Perceived and objective environmental measures and physical activity among urban adults. Am J Prev Med 28 (2 Suppl 2):105–116
Foster C, Hillsdon M, Thorogood M (2004) Environmental perceptions and walking in English adults. J Epidemiol Community Health 58:924–928
Reed JA, Ainsworth BE, Wilson DK, Mixon G, Cook A (2004) Awareness and use of community walking trails. Prev Med 39:903–908
Evenson KR, Herring AH, Huston SL (2005) Evaluation change in physical activity with the building a multi-use trail. Am J Prev Med 28(2 Suppl 2):177–185
Rohrer J, Pierce JR Jr, Denison A (2004) Walkability and self-rated health in primary care patients. BMC Family Practice 5:29
Burstrom B, Fredlund P (2001) Self rated health: Is it as good a predictor of subsequent mortality among adults in lower as well as in higher social classes?. J Epidemiology Community Health 55:836–840
Finch BK, Hummer RA, Reindl M, Vega WA (2002) Validity of self-rated health among Latino(a)s. Amer J Epidemiol 155:755–759
Shadbolt B, Barresi J, Craft P (2002) Self-rated health as a predictor of survival among patients with advanced cancer. J Clin Oncol 20:2514–2519
Meurer LN, Layde PM, Guse CE (2001) Self-rated health status: a new vital sign for primary care?. WMJ 100(7):35–39
Shi L, Starfield B, Politzer R, Regan J (2002) Primary care, self-rated health, and reductions in social disparities in health. Health Serv Res 37:529–550
Heidrich J, Liese AD, Lowell H, Keil U (2002) Self-rated health and its relation to all-cause and cardiovascular mortality in southern Germany. Results from the MONICA Augsburg cohort study, 1984–95. Ann Epidemiol 12:338–345
Eyler AA, Brownson RC, Bacak SJ, Housemann RA (2003) The epidemiology of walking for physical activity in the United States. Med Sci Sports Exerc 35:1529–1536
Siegel PZ, Brackbill R, Health GW (1995) The epidemiology of walking for exercise: implications for promoting activity among sedentary groups. Am J Public Health 85:706–710
Greenberg MR, Renne J (2005) Where does walkability matter the most? An environmental justice interpretation of New Jersey data. J Urban Health 82:90–100
Giles-Corti B, MacIntyre S, Clarkson JP, Pikora J, Donovan RJ. (2003) Environmental and lifestyle factors associated with overweight and obesity in Perth, Australia. Am J Health Promot 18:93–102
Siminski RR, Poston WS, Petosa RL, Stevens E, Katzenmoyer LM (2005) Features of the neighborhood environment and walking by U.S. adults. Am J Prev Med 28:149–155
Humpel N, Owen N, Iverson D, Leslie E, Bauman A (2004) Perceived environmental attributes, residential location, and walking for particular purposes. Am J Prev Med 26:119–17
Giles-Corti B, Donovan RJ (2003) Relative influence of individual, social environmental, and physical environmental correlates of walking. Am J Public Health 93:1583–1589
Weinstein A, Feigley P, Pullen P, Mann L, Redman L (1996) Neighborhood safety and the prevalence of physical activity - selected states, 1996. MMWR 48:143–146
King AC, Castro C, Wilcox S, Eyler AA, Sallis JF, Brownson RC (2000) Personal and environmental factors associated with physical inactivity among different racial-ethnic groups of U.S. middle aged and older women. Health Psychol 19:354–364
Gordon PM, Zizzi SJ, Pauline J. Use of a community trail among new and habitual exercisers: a preliminary assessment. Prev Chronic Dis [serial online] 2004 Oct. Available at http://www.cdc.gov/pcd/issues/2004/oct/04_0058.htm; accessed 09 August 2005
Brownson RC, Baker EA, Boyd RL, et al (2004) A community-based approach to promoting walking in rural areas. Am J Prev Med 27:28–34
Gauvin L, Richard L, Craig CL, et al (2005) From walkability to active living potential: an “ecometric” validation study. Am J Prev Med 28 (2 Suppl 2):126–133
Saelens BE, Sallis JF, Black JB, Chen D (2003) Neighborhood-based differences in physical activity: an environment scale evaluation. Am J Public Health 93:1552–1558
Leslie E, Saelens B, Frank L, Owen N, Bauman A, Coffee N, Hugo G (2005) Residents’ perception of walkability attributes in objectively different neighborhoods: a pilot study. Health Place 11:227–236
Acknowledgments
The Amarillo Veterans Affairs Medical Center provided in-kind support for this project.
Author information
Authors and Affiliations
Corresponding author
Additional information
J. Rush Pierce, Jr., is Health Authority for the Amarillo Bi-City-County Health District, Amarillo, Texas, and Associate Professor and Chief, Division of Preventive Medicine, Department of Internal Medicine, Texas Tech University Health Sciences Center, Amarillo, Texas; Anne V. Denison, Ahmed A. Arif, Assistant Professor, and James E. Rohrer, Professor, are with the Division of Health Services Research, Department of Family and Community Medicine, Texas Tech University Health Sciences Center, Lubbock, Texas
Rights and permissions
About this article
Cite this article
Pierce, J.R., Denison, A.V., Arif, A.A. et al. Living near a trail is associated with increased odds of walking among patients using community clinics. J Community Health 31, 289–302 (2006). https://doi.org/10.1007/s10900-006-9014-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10900-006-9014-8