
Abstract
Huntington disease (HD) is a progressive neurodegenerative disorder. Presymptomatic genetic testing allows at-risk individuals to clarify their risk status. Understanding the characteristics and motivations of individuals seeking HD presymptomatic genetic testing better equips genetic counselors and other healthcare professionals to provide comprehensive and personalized care. The aims of this study were to (1) determine whether the average age when individuals seek presymptomatic HD genetic testing has decreased over time, (2) assess motivations for seeking testing, (3) explore whether there is a relationship between age and motivations, and (4) explore genetic counselors’ perceptions of the shift in age. Data from the US HD testing centers (N = 4) were analyzed. A small but statistically significant decrease in age of individuals seeking presymptomatic testing was observed (p = 0.045). HD community members (N = 77) were surveyed regarding presymptomatic testing motivations. Younger individuals were more likely than older individuals to cite “To learn whether or not you would develop HD” and “To make choices about further education or a career” compared to older individuals (p < 0.05). Conversely, older individuals more frequently cited “To give children a better idea of their risk” (p < 0.002). Sixteen percent of genetic counselors surveyed (6/37) perceived a change in age of testing. All of these respondents had provided HD testing for ten or more years and anecdotally believed the age at testing has decreased over time. Study results help providers personalize counseling based on patient’s age and serve as a starting point for more research into the relationship between age at testing and motivations for testing.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Huntington disease (HD) is a progressive, incurable neurological disorder characterized by motor deterioration, cognitive changes, and psychiatric disturbances. The average age of onset of motor symptoms of HD is 35–44 years, although age of onset can be highly variable (Shoulson and Young 2011; Quarrell et al. 2012; Koutsis et al. 2014). Most individuals with HD live about fifteen years after they begin to notice motor symptoms. Over time, individuals gradually lose the ability to walk, talk, and eventually require 24-hour care. HD follows an autosomal dominant inheritance pattern and has 100% penetrance for allele sizes with 40 or more CAG repeats (Warby et al. 2010). The combination of autosomal dominant inheritance, high penetrance for the most common disease-causing alleles, and (on average) adult onset are strong motivators for presymptomatic genetic testing for many individuals.
Huntington disease is relatively rare. HD affects about three out of every 100,000 individuals and is more common in individuals of Western European ancestry (Warby et al. 2010). It has been estimated that up to 43,000 individuals are affected with HD in the US, and 123,000 individuals are at 50% risk for HD (Fischer and Hayden 2014). Direct presymptomatic testing has been available since 1993 to determine whether or not an individual will develop HD in their lifetime. Since then, genetic data on both HD and other disorders have gradually become more widely available. New generations interact with all information, including genetic information, differently. Attitudes of adults at-risk for HD today have evolved since 1993 in reaction to everything from social media to the increasing variety of medically and personally available genetic information.
The average age of individuals who seek presymptomatic testing has been measured in studies, but never compared over time. The current study aimed to determine whether the average age of individuals seeking presymptomatic genetic testing for HD has decreased over time, to assess motivations for seeking genetic testing, and to explore whether there is a relationship between age and motivations.
Research on HD Testing Motivations and Individual Characteristics
Previous literature about HD predictive genetic testing has focused on patient decision-making and motivations for pursuing testing. In a retrospective cohort study in Montreal, Canada, from 1994 to 2008, patients were asked to articulate their top five motivations for seeking presymptomatic testing for HD (Dufrasne et al. 2011). Most frequently cited reasons for seeking testing included to relieve uncertainty about the risk of illness, to decide about having (further) children, to plan their future, to give offspring a better estimate of their personal risk, to investigate their beliefs of having already developed HD, and to start treatment if positive. These responses were not categorized by age of participant. Demographic characteristics of the sample included approximately equal proportions of male and female respondents, and an average age of 36.4 years of all participants. Age at testing was not analyzed over time or related to individuals’ motivations for seeking testing.
A statewide HD testing center in Australia conducted a medical record review to compile demographic data about those seeking presymptomatic genetic testing for HD at their center (Suffham and MacMillan 2014). This study reported an average age of 39.3 years. Other important results of the record review include motivations of individuals seeking testing. Some of the motivations cited are family planning, planning for the future, need to know, to inform children, and to obtain information. Other studies report similar mean ages of individuals seeking presymptomatic testing: 40.4 years from a study in Victoria, Australia (Trembath et al. 2006) and 30.0 years in a South African study (Sizer et al. 2012).
Life-Stage as an Important Factor
Taylor (2003) conducted a qualitative study using in-depth interviews of sixteen individuals at risk for HD. The main goal was to explore the decision-making process of individuals in the testing process. In this study, participants both seeking and declining genetic testing were interviewed. Participants selected were between 20 and 59 years of age. Highlights from interviews led to three main themes: HD testing as an opportunity to gain significant life knowledge, the right “not to know,” and testing as the perceived “right thing to do.” Taylor (2003) concluded that life-stage (e.g., marital status, pursuing education, whether or not they had children) is important in the presymptomatic testing process.
Considering life-stage as a critical variable in the decision to pursue presymptomatic HD testing, Duncan et al. (2007) interviewed four males and four females who had obtained predictive genetic testing between the ages of 17 and 25. Their study is unique in that importance is placed on the individuals’ experience before testing. Three themes of life before testing include: living as though gene-positive, engaging in risky behaviors, and having a complex past. Themes of life after testing for these individuals were living again and identity difficulties, which could be important possibilities for genetic counselors to discuss with individuals considering testing. The findings of their study are also relevant because they provide insight into the experiences of young people having genetic testing for HD.
Sparbel et al. (2008) studied young people at risk of developing HD who had not yet had genetic testing. The primary goal of their research was to gain insight into the lives of teens in families with HD. Although the focus group leader did not initiate the topic, predictive testing was brought up in each focus group. Of note, the teens rarely discussed future goals and careers, but they did discuss that they saw benefits of predictive testing for family planning. Most of the teens expressed a desire to obtain testing before starting a family because they “don’t want to risk giving it to someone else” (p. 331). This study highlights that teens aged 14–18 are actively considering whether or not to undergo presymptomatic genetic testing, and they may benefit from discussions about testing with genetic counselors or other healthcare providers.
“Reproductive decision-making” is a commonly cited reason given by individuals seeking presymptomatic genetic testing for HD (Quaid et al. 2010, p. 606). The Huntington Study Group PHAROS Investigators examined the reproductive decision making of at risk individuals who have chosen not to be tested. Detailed stories from individuals at risk of HD were coded into major themes for both individuals who had children and those who decided not to have children. Individuals who had children expressed “hope for a cure” and guilt, while those who did not have children were adamant to “stop HD” but scared about being alone if/when they develop HD because they had isolated themselves from relationships and a family (p. 611). Reproductive decision-making may be a motivating factor that is important for younger people when considering presymptomatic testing compared to older individuals who are nearing the end of their reproductive years.
Purpose of the Study
Recent research has focused on defining the motivations of individuals seeking presymptomatic genetic testing for HD (Dufrasne et al. 2011; Quaid et al. 2010; Suffham and MacMillan 2014). Previous studies have indicated that life stage and life events are important and influence individuals’ motivations for seeking testing (Duncan et al. 2007; Sparbel et al. 2008; Taylor 2003). Prior research also suggests motivations for pursuing genetic testing could vary by age group; however, the average age of individuals who seek presymptomatic testing has never been compared over time.
The purpose of this study is to determine whether the average age of individuals seeking presymptomatic genetic testing for HD has decreased over time, assess motivations for seeking genetic testing, and explore whether there is a relationship between age and motivations. By categorizing reasons for seeking testing, the present study provides an important first step in describing baseline motivations for genetic counselors to explore throughout the testing process.
The data obtained in this study could allow genetic counselors to modify their counseling based on the specific needs of the patient. By ensuring individuals going through the testing process have thoroughly explored their motivations for testing, genetic counselors can better help an individual discover the impact of knowing their HD status on their life. Additionally, HD has often been cited as a model for other diseases with an adult onset, such as familial cancers and Alzheimer’s disease. The information gained from studying HD could be utilized by genetic counselors to provide more personalized counseling to individuals at risk of developing other late onset genetic conditions.
Methods
Participants and Procedures
The current study involved data collection from three sources. The ascertainment protocol was approved by the Institutional Review Board at Virginia Commonwealth University (HM20001556).
HD Testing Centers
The first source of data was historical anonymized demographic information about individuals who sought presymptomatic genetic testing from HD testing centers. Each of the twenty-one Huntington’s Disease Society of America (HDSA) HD Centers of Excellence in existence in 2014 were contacted by email and sent a data collection form (described below). The HDSA launched a new HD Centers of Excellence initiative in 2014 to identify and credential new centers. Prior to this, the pool of twenty-one HD Centers of Excellence was stable for over ten years. Additionally, the same data collection form was sent to genetic counselors at other centers with an established history of conducting HD presymptomatic genetic testing, which were identified through genetic counselors who were members of the National Society of Genetic Counselors (NSGC).
Individuals at Risk
The second data source was individuals at risk for HD, who had undergone presymptomatic genetic testing or considered it. Participants meeting inclusion criteria were recruited at the 2014 HDSA Annual Convention in Louisville, Kentucky. Additionally, emails including a description of the study and a link to the survey were sent to support group leaders listed on the HDSA website for distribution to support group members. Participants in this portion of the study had to be at least eighteen years or older, be at risk for HD, and either have had testing before they started to show symptoms, or if they had not yet had genetic testing, they had to feel they were asymptomatic.
Genetic Counselors
The final data source was genetic counselors who provide HD counseling. Genetic counselors’ email addresses were obtained from a request posted on the general NSGC forum for genetic counselors who provide HD counseling, from the NSGC membership directory of genetic counselors who list neurogenetics as a specialty, as well as personal knowledge of the investigators. The survey was anonymous, but genetic counselors who worked at the participating HD testing centers were invited to participate, as well as any other willing genetic counselors.
Instrumentation
HD Testing Centers
An Excel spreadsheet was sent to each HD testing center. The contact person at each center was asked to provide anonymous demographic data on the first ten patients seeking predictive testing for HD per year from years 1996, 2002, 2008, and 2014. Ten patients for four time points were requested to limit burden on the individual providing data. The demographic data collected were age, gender, positive or negative test result, if the individual received their result, marital status at the time of testing, and number of children at the time of testing.
Individuals at Risk
Information from individuals who have had, or considered having, presymptomatic genetic testing was collected by survey and stored using the REDCap database system. The survey asked individuals about basic demographic information, whether or not they have had testing, when they had testing, who helped them through the testing process, and their motivations for considering testing. The survey used a combination of checklists and free response questions. Branching questions were used so that respondents’ answers to initial questions influenced the subsequent questions available to them. Individuals who had presymptomatic testing in the past or were considering it at the time of the survey were asked their motivations for testing. If they responded that they were not considering presymptomatic testing, then the survey ended. Current ages of these individuals were not collected. Ages were only collected for individuals who had already completed presymptomatic testing. A list of ten motivations for seeking testing was provided, and was created based on the findings of Dufrasne et al. (2011). Individuals were instructed to select any response that applied and were given the opportunity to write in any additional motivations they had for seeking testing.
Genetic Counselors
An eight-item multiple choice and free response survey was administered to genetic counselors who provide services for individuals with or at risk for HD. Genetic counselors were asked how long they have been providing counseling for HD, approximately how many patients they see annually, and whether they perceive a shift in age. If they did perceive a shift in age, they were asked if they believed individuals are being tested at a younger or older age now compared to the past. Surveys were administered and data were stored with the REDCap database system.
Data Analysis
HD Testing Centers
Statistical analysis was performed using the program R (R Core Team 2015). Linear regression was used to determine the relationship between year of testing and age at testing. Covariate analyses were included to determine whether additional factors influenced the relationship between year of testing and age at testing.
Individuals at Risk
Data from individuals at risk of developing HD were coded and exported from the REDCap database. Linear regression was used to model the relationship between year of testing and age at testing for this sample. The relationship between motivation for testing and age at testing was measured, as well as the relationship between motivation for testing and year of testing. Descriptive statistics were utilized to describe demographic information and frequently cited motivations.
Genetic Counselors
Data from the genetic counselor survey were also exported from the REDCap database and coded. Frequency counts were used to quantify genetic counselors’ responses. Descriptive statistics were utilized to determine the characteristics of the respondents.
Results
Age and Other Characteristics of Individuals Seeking Testing from HD Testing Centers
A total of seven HD testing centers completed the data collection form and provided information on 156 individuals seeking testing. The amount of data available at each time point varied by center (median = 18 individuals per center over the 4 time points requested; one center provided data for only 3 individuals over the time points requested, and another center provided data for 52 individuals over the time points requested). Data from three testing centers were excluded because the only patient information available was from 2014 (n = 21). Thus, information for 135 individuals seeking testing at 4 different centers was used for analysis. Table 1 summarizes the characteristics of the sample. The median age of individuals seeking presymptomatic genetic testing was 34 years; the mean was 36 years (SD = 11.96 yrs).
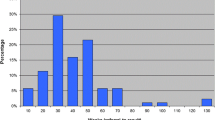
Age at testing was compared to year at testing. A linear model was used to identify the relationship between age at testing and year of testing. Figure 1 plots data from 1996, 2002, 2008, and 2014 against age of testing. The age of testing was significantly lower at more recent time points (p = 0.045). The slope was − 0.333 and 3% of the variance in age at testing can be explained by year at testing (r2 = 0.030). This relationship was not modified by gender (p = 0.558).

Age at testing vs year of testing from HD testing centers
Figure 2 shows the interaction effect of relationship status on the relationship between age at testing and year of testing (p = 0.03). The difference in slope between those who were in a relationship at the time of testing and those who were not can be observed. Decreasing age of testing was more prominent among people who were not married or in a committed relationship.

Interaction between relationship status and the effect of age at testing on year of testing
Characteristics of Survey Respondents at Risk of HD
The total number of completed surveys from the HDSA Annual Convention and online respondents was 89. One survey was omitted because the individual completing the survey was not at risk of developing HD. Characteristics of individuals from this survey are listed in Table 2.
Out of 88 study-eligible individuals who completed the survey, 44 individuals had already had presymptomatic genetic testing for HD. These individuals were asked to provide their age at testing, as well as the year in which they were tested. There was no statistically significant association between age of testing and year of testing.
Individuals who already had, or were considering presymptomatic genetic testing for HD were asked to select their motivations for testing. The motivations are shown in Table 3. The most frequently cited motivations were “To learn whether or not you would develop HD” (75.3%) and “To plan for your future” (49.4%).
Additionally, each motivation was tested to determine if age correlated with motivation. Three motivations were significantly correlated with age. Individuals who were tested at younger ages were significantly more likely to cite “To learn whether or not you would develop HD” and “To make choices about further education or a career” compared to individuals who had testing at older ages (p < 0.05). The average ages of individuals who cited these motivations were 27.33 and 25.00 years old, respectively. Conversely, “To give children a better idea of their risk” was more frequently cited as a motivation for testing by older individuals than younger individuals (p < 0.002). Motivations were compared to year of testing to determine whether motivations have changed over time, and none of the listed motivations were significantly correlated with year at testing.
A total of six individuals cited “other” motivations. Individuals who indicated “other” motivations were asked to describe their additional motivations. The following are representative responses:
“My father was showing some progressive signs and I wanted to see also as proof for his condition; the changes in his behavior he was in denial of.” (sought testing at age 27)
“Long term disability, medicare, SSI” (not yet tested, age not reported)
“To create a sense of urgency to the most important things in my life” (sought testing at age 46)
“I had been diagnosed with depression; since I had heard that was one of the major early symptoms of HD I wanted to know if there might be a relationship between the two (before seeking treatment for either)” (sought testing at age 19)
Genetic Counselors Perceptions of the Age of Individuals Seeking Presymptomatic Genetic Testing Over Time
Thirty-seven genetic counselors who provide genetic counseling for individuals seeking presymptomatic genetic testing for HD were surveyed about their perceptions regarding the average age of individuals seeking presymptomatic genetic testing. Of the 37 total respondents, six genetic counselors reported anecdotally believing that individuals were seeking testing at younger ages now than those who sought testing in the past. All six of these counselors had at least 10 years of experience providing counseling for individuals seeking presymptomatic HD testing. The remaining 31 respondents did not feel that the age of individuals seeking testing was different now than in the past. Genetic counselors who perceived a change in age were asked to provide possible reasons for the shift to a younger age. Results are shown in Table 4. Two respondents provided “other” reasons:
“Acceptance of IVF with PGD, and more interest in trying to eradicate HD through family planning”
“The first group of people being tested were those at risk who had been waiting a long time for testing to be available, so I think the cohort of those interested in testing was skewed to older individuals. I see a real mix now, of younger folks using the results for life planning and those who are approaching age of symptom onset.”
Discussion
This study examined the demographics and motivations of individuals seeking presymptomatic genetic testing for Huntington disease (HD). Specifically, the study aimed to determine whether the average age when individuals seek presymptomatic HD genetic testing has decreased over time, assess motivations for seeking testing, and explore whether there is a relationship between age and motivations.
Decreasing Age at Testing Over Time
This study demonstrates a small but statistically significant decrease in age at presymptomatic genetic testing over time, based on data obtained from four Huntington’s Disease Society of America (HDSA) HD Centers of Excellence. This finding is corroborated by the perceptions of a few genetic counselors that the age of individuals seeking HD testing is decreasing. There also was a non-statistically significant downward trend observed in a survey of individuals at risk of HD who have had presymptomatic genetic testing to learn their HD status. These results suggest individuals are seeking presymptomatic genetic testing for HD at a younger age now than in the past. To our knowledge, these are the first published empirical data specifically demonstrating this phenomenon. A potential explanation for the observed trend is exemplified by one genetic counselor’s response to the survey question asking about reasons for a decrease in age at testing: when presymptomatic genetic testing for HD became available in 1993, there was a rapid influx of older individuals seeking testing who had been waiting for the test to become available. In more recent years, the average age could have stabilized to a younger age.
In the present study, the relationship between age at testing and year of testing was modified by whether or not the individual was married/in a committed relationship at the time of testing (Fig. 2). For individuals in a relationship at the time of testing, there has not been a change in the age at which they sought testing. However, there has been a significant decrease in the age at testing for individuals who were not in a relationship at the time of testing. It appears that since HD testing first became available, people in committed relationships have sought testing at an average age of about 31; however, in more recent years, single individuals have sought testing at younger ages compared with single individuals in years past. Individuals in a relationship may pursue testing to provide information for other family members, whereas individuals who were not in a relationship may seek testing based more on personal reasons. These reasons could include relieving uncertainty and deciding about further education or a career, motivations which, in this study, were correlated with a younger age.
The age at which individuals found out they were at risk for HD was not collected, and this could also significantly impact the age at which they sought testing. When controlling for whether or not an individual had children at the time of testing, there was no longer a significant effect of age at testing on year of testing. This may be because having children was highly correlated with older age (r2 = 0.21). Additionally, gender does not appear to have modified the effect of age at testing on year at testing.
Motivations of Individuals Seeking Testing
The second aim of the current research was to assess the motivations for testing of individuals at risk for HD and to compare motivations to age at testing. The most frequently cited motivation was “To learn whether or not you would develop HD,” which was listed as a motivation by 75% of respondents. This is consistent with the study by Dufrasne et al. (2011). The frequency of the remaining motivations is also consistent with the findings of Dufrasne et al. (2011), except in the current study “To help make decisions about participating in research” was cited by 31.2% of respondents, and was never mentioned in the free responses of those studied by Dufrasne and colleagues. This could be because of the difference in the method used to collect motivations; Dufrasne et al. used open-ended surveys, and the current study listed motivations on a checklist. Individuals seeking testing could be considering participation in research, but this may not be their primary motivation, and may not be in the forefront of their decision making unless prompted.
Regression analysis revealed that age predicts three of the listed motivations. Individuals who were tested at younger ages were significantly more likely to cite “To learn whether or not you would develop HD” as a motivation for seeking presymptomatic genetic testing. Overall, this finding is consistent with the literature; young people tend to have a higher interest in genetic testing (Aro et al. 1997). This could be due to increased use of technology for information seeking in younger generations. Genetic counselors surveyed about their perception about reasons for a change in age cited that “individuals seeking testing are more accepting and trusting of technology, science, and genetic testing.” Additionally, increased awareness and acceptance of preimplantation genetic diagnosis and in vitro fertilization techniques could lead to more motivation to pursue presymptomatic testing, learn their HD status, and attempt to eliminate HD in their family using assisted reproductive techniques.
Younger individuals were also more likely to cite “To make choices about further education or a career” compared to individuals who had testing at older ages. Younger individuals may be more likely to be at a time in their life where they are completing school or starting their career, so they would be more likely to use presymptomatic testing for HD to help them decide about education or a career.
“To give children a better idea of their risk” was more frequently cited as a motivation for testing by older individuals. Older individuals are more likely to have already had children and to have older children, so these individuals would be more likely to seek testing to provide their children with a better estimate of their risk.
There were not any significant correlations between motivation and year at testing. These findings suggest that motivations for seeking testing do not appear to be changing over time.
Practice Implications
Understanding the demographics and motivations of individuals seeking presymptomatic testing for HD can help genetic counselors and other healthcare professionals provide more personalized and effective genetic counseling services. Genetic counselors should be aware that the motivations for testing might differ between younger and older individuals seeking testing. Based on the findings of this study, younger individuals may be more likely to seek testing to answer questions about uncertainty of their status and to help make decisions about future education. Genetic counselors should be prepared to explore these topics more in depth than other topics in a session with a younger individual. For instance, they may spend less time exploring “giving children a better idea of their risk,” a motivation that was more likely to be endorsed by older individuals. It is important for genetic counselors to thoroughly explore the possible impacts of discovering one’s HD status so that the individual seeking testing is prepared to receive her or his results. This study also found that some individuals are considering participation in research, so genetic counselors should be prepared to discuss clinical trials and research participation.
Research Recommendations
In order to determine whether there has, in fact, been a change in age over time or whether this is simply an artifact of a large number of older individuals initially seeking testing, additional studies should be completed to measure a larger sample from a greater number of HD testing centers over more time points. Additionally, analyses to determine whether the observed change in age at testing is center specific, and whether there are any additional factors contributing to the decreasing age at testing, are recommended, especially given the very small percentage of the variance accounted for by year of testing in this study. Assessing individuals’ motivations for NOT going forward with presymptomatic genetic testing could also provide valuable information for genetic counselors working with individuals considering presymptomatic HD testing. Our study did not request socioeconomic or ethnicity data. Demographic differences other than age may influence motivations for presymptomatic genetic testing now and over time.
Study Limitations
HD Testing Centers
One limitation of the current study is the low response rate and relatively small sample size. Requests for data were sent to all of the HDSA Centers of Excellence (N = 21) in existence at that time, and usable data were only received from three centers. Increasing the sample size would increase the power of the study and help increase the generalizability of the findings.
Additionally, patient information was requested only for the first ten patients per year from each HD testing center in an attempt to increase the number of testing centers responding by limiting the burden of unfunded data reporting. We also limited the number of patients per year to reduce the opportunity for a very busy clinic to bias the results. Therefore, the sample is not completely random and could be biased.
Individuals at Risk
Another limitation involves the survey of individuals at risk for HD. Only those respondents who had already had presymptomatic genetic testing were asked their age. Therefore, comparison between age and motivation was only possible for those who already had testing, not for individuals who are currently considering testing.
A portion of the individuals at risk of HD who participated in the study were recruited at the HDSA national convention. This represents a convenience sample and could have led to an ascertainment bias, favoring individuals interested in research and advocacy. This is especially plausible given that the current study identified “To make decisions about participation in research” as a relatively frequently cited motivation for seeking testing, a finding not corroborated by other studies. Additionally, this study relied on self-reported retrospective data, which decreases the reliability of the findings compared to prospective data obtained immediately around genetic testing.
Conclusion
This study describes a small but statistically significant decrease in the age of individuals seeking presymptomatic genetic testing for Huntington disease over time. Additionally, three motivations for testing were correlated with age at testing. These motivations do not appear to have changed over time. Genetic counselors should be aware that the motivations for testing might differ between younger and older individuals seeking testing.
References
Aro, A., Hakonen, A., & Hietala, M. (1997). Acceptance of genetic testing in a general population: age, education and gender differences. Patient Education and Counseling, 32, 41–49.
Dufrasne, S., Roy, M., Galvez, M., & Rosenblatt, D. (2011). Experience over fifteen years with a protocol for predictive testing for Huntington disease. Molecular Genetics and Metabolism, 102, 494–504.
Duncan, R., Gillam, L., Savulescu, J., Williamson, R., Rogers, J., & Delatycki, M. (2007). “Holding your breath”: interviews with young people who have undergone predictive genetic testing for Huntington disease. American Journal of Medical Genetics, 143A, 1984–1989.
Fischer, E., & Hayden, M. (2014). Multisource ascertainment of Huntington disease in Canada: prevalence and population at risk. Movement Disorders, 29, 105–114.
Koutsis, G., Karadima, G., Kladi, A., & Panas, M. (2014). Late-onset Huntington’s disease: diagnostic and prognostic considerations. Parkinsonism & Related Disorders, 20, 726–730.
Quaid, K., Swenson, M., Sins, S., Harrison, J., Moskowitz, C., Stepanov, N., et al. (2010). What were you thinking?: individuals at risk for Huntington disease talk about having children. Journal of Genetic Counseling, 19, 606–617.
Quarrell, O., O'Donovan, K. L., Bandmann, O., & Strong, M. (2012). The prevalence of juvenile Huntington’s disease: a review of the literature and meta-analysis. PLoS Currents, 4.
R Core Team. (2015). R: a language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing URL http://www.R-project.org/.
Shoulson, I., & Young, A. B. (2011). Milestones in Huntington disease. Movement Disorders, 26, 1127–1133.
Sizer, E., Haw, T., Wessels, T., Kromberg, J., & Krause, A. (2012). The utilization and outcome of diagnostic, predictive, and prenatal genetic testing for Huntington disease in Johannesburg, South Africa. Genetic Testing and Molecular Biomarkers, 16, 58–62.
Sparbel, K., Driessmack, M., Williams, J., Schutte, D., Tripp-Reimer, T., McGonigal-Kenney, M., et al. (2008). Experiences of teens living in the shadow of Huntington disease. Journal of Genetic Counseling, 17.
Suffham, T., & MacMillan, J. (2014). Huntington disease: who seeks presymptomatic genetic testing, why and what are the outcomes? Journal of Genetic Counseling.
Taylor, S. (2003). Predictive genetic test decisions for Huntington’s disease: context, appraisal and new moral imperatives. Social Science and Medicine, 58, 137–149.
Trembath, M., Tassicker, R., Collins, V., Mansie, S., Sheffield, L., & Delatycki, M. (2006). Fifteen years of experience in predictive testing for Huntington disease at a single testing centre in Victoria, Australia. Genetics in Medicine, 8(11), 673–680.
Warby, S., Graham, R., & Hayden, M. (2010). Gene reviews: Huntington disease. Retrieved from: http://www.ncbi.nlm.nih.gov/books/NBK1305/
Acknowledgements
Funding for the genetic counselor survey was provided by the Virginia Commonwealth University Huntington Disease Program. Study data were collected and managed using REDCap electronic data capture tools hosted at the Virginia Commonwealth University. The project was supported by CTSA award No. UL1TR000058 from the National Center for Advancing Translational Sciences. Its contents are solely the responsibility of the authors and do not necessarily represent official views of the National Center for Advancing Translational Sciences or the National Institutes of Health. This project was conducted to fulfill a degree requirement.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Melissa A. Holman, John Quillin, Timothy P. York, Claudia M. Testa, Ami R. Rosen, and Virginia W. Norris declare that they have no conflict of interest.
Human Studies and Informed Consent
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000 (5). Protected health information was not collected from patients included in the study, and consent was not obtained to answer the anonymous survey.
Animal Studies
No animal studies were carried out by the authors for this article.
Rights and permissions
About this article

Cite this article
Holman, M.A., Quillin, J., York, T.P. et al. The Changing Age of Individuals Seeking Presymptomatic Genetic Testing for Huntington Disease. J Genet Counsel 27, 1157–1166 (2018). https://doi.org/10.1007/s10897-018-0233-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10897-018-0233-9