
Abstract
This study adopted a brief component analysis to examine the active variable in a tolerance for delay of reinforcement (TFD) intervention procedure to decrease tangible-maintained problem behavior for a male adolescent with autism. Antecedent-based functional analysis suggested that problem behavior occurred most when access to tangible items or activities was restricted. With the introduction of a TFD intervention procedure using a combination of a general delay cue and an explicit delay cue, the learner’s problem behavior decreased to a low level and he quickly learned to wait for access to preferred items for 10 min with no problem behavior. Two weeks after the learner met the mastery criterion, a component analysis was conducted through a brief ABA withdrawal design, to separate the relative contributions of the general delay cue and the explicit delay cue in the maintenance of the TFD intervention. The combination of general and explicit delay cues resulted in low levels of problem behavior and higher toleration of delays to reinforcement relative to the general delay cue alone. Implications and limitations are discussed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
There is evidence that using a tolerance for delay of reinforcement (TFD) intervention can be an effective approach to addressing problem behavior maintained by positive or negative reinforcement (e.g., Fisher et al. 2000; Grey et al. 2009; Hong et al. 2014; Reichle et al. 2010; Vollmer et al. 1999). Typically, TFD consists of four elements, including (a) identifying a baseline level of waiting duration prior to the occurrence of problem behavior, (b) specifying a delay cue, (c) delivering the delay cue throughout the waiting duration, and (d) specifying and delivering a release cue at the end of the waiting duration. The waiting duration is gradually increased until a learner meets a final criterion (Reichle et al. 2010).
In implementing TFD, Carr et al. (1994) suggested that it was easier to increase delay to reinforcement after a signal if the learner was engaged during the delay. Early use of TFD was reported by Kemp and Carr (1995) who successfully implemented a TFD procedure as a part of a multi-component intervention strategy with persons employed at a greenhouse. Prior to that, Carr and Carlson (1993) implemented a TFD procedure as part of a multi-component strategy for three persons who had severe intellectual disabilities. In the study by Carr and Carlson, TFD was implemented during escape attempts that occurred during community shopping. When a participant requested a preferred item, the interventionist delivered a delay cue (e.g., “…first let’s get one of the things on our shopping list and then we’ll come back”). Participants were allowed access to the preferred item after first given access to the next item on the list. Kern et al. (1997) successfully implemented TFD with a young woman who engaged in self-injurious behavior that produced escape from tasks and aggression that produced food (although the procedure was less effective in decreasing aggression). Despite the somewhat limited research addressing this procedure, we suspect that TFD is a procedure that practitioners may attempt to implement fairly often.
Other researchers, including Reichle et al. (2010), have suggested that some forms of the delay cue may afford a learner greater control over monitoring how much effort or how long he or she has to wait to obtain reinforcement. Reichle et al. examined the differential effects of general and explicit delay cues in increasing on-task behavior while decreasing escape-maintained problem behavior for two preschool children with autism and moderate to severe intellectual delays. A general delay cue consisting of a visual symbol denoting “almost done” accompanied by a verbal cue “almost done” was provided. An explicit delay cue was a verbal cue (i.e., “Do__ more” if the task involved concrete number of task units to work on; or “Just __ more” if the task was temporal in nature) accompanied by a visual cue of a timer that counted down the predetermined waiting time. Results showed that an explicit delay cue was more effective for improving task completion and decreasing escape-maintained problem behavior of two young children with autism.
Hong et al. (2014) compared the relative effects of general and explicit delay cues in TFD intervention procedures focused on tangibly maintained problem behavior for two children with autism spectrum disorders (ASD). Unlike the use of TFD prior to the occurrence of problem behavior, Hong et al. implemented the delay cue as a consequence to problem behavior. Specifically, if the learner showed the targeted problem behavior during 30 s waiting duration, the interventionist presented the general delay cue by pointing to a picture-based “Wait” card and saying “It’s my turn”. The explicit delay cue consisted of the interventionist counting down saying, “30, 29, 28, …1, and 0, it’s your turn!” with an accompanying visual timer for 30 s and saying “X seconds more” while pointing to the “Wait” card if the learner engaged in the targeted problem behavior. The investigators reported that both types of delay cues were effective in decreasing tangible-maintained problem behavior, although the explicit delay cue appeared to produce slightly better effects.
Although it appears that, for some learners, explicit delay cues may be somewhat more effective, general delay cues are also important. There are many novel situations that interventionists encounter where a previously established explicit delay cue cannot be implemented. For example, during a car trip to a library, the driver may not be able to specify an exact time of arrival. This situation must rely on a general delay cue. Consequently, some researchers (e.g., Reichle and Wacker 2014) suggested delivering a combination of explicit and general delay cues (e.g., “just do these [displaying two items], we are almost done”). In spite of the evidence of relatively greater effectiveness of the explicit delay cue condition in TFD intervention procedures, few studies have examined the relative component contributions of a combination of general and explicit delay cues during maintenance. That is, after the successful implementation of a TFD intervention using a combination of an explicit delay cue paired with a general delay cue, it remains unclear whether the intervention would continue to be effective if the explicit delay cue was extracted. The current study was implemented to examine the active component of a TFD intervention with both a general delay cue and an explicit delay cue during maintenance that had been implemented to address the tangible-maintained problem behavior in an adolescent with autism.
Method
Participant
Max was 18 years and 2 months old when the study began. One intellectual assessment was completed when he was 15 years old using Weschler Intelligence Scale—IV (Wechsler 2004) with a full scale IQ of 42. In addition, the Scales of Independence Behavior—Revised (SIB—R; Bruininks et al. 1996) was completed when he was 15 years old, with an overall Broad Independence Score of 4 years. Per a licensed physician’s report prior to his moving to the group home, he was diagnosed with autism, mild to moderate intellectual disability, and ADHD. It was also reported that he had a history of being diagnosed with a mood disorder and Tic disorder. According to the report by the staff at the group home, he was able to follow one- and two-step simple verbal directions most of the time. He was largely nonverbal. Max could produce some signs that were approximations of American Sign Language (ASL). Max’s signs could only be deciphered by familiar caregivers. Additionally, he was able to produce several spoken one-word utterances (e.g., “yes,” “more”, “drink”) that were only understandable to familiar persons. Usually Max accompanied spoken words with corresponding sign approximations. One year prior to the current investigation he began using an iPad equipped with Proloquo2Go software to supplement his communication. Per group home staff report, Max independently navigated the Proloquo2go application to locate approximately 100 symbols or written words to express his wants or needs. In general, communicative functions Max produced included requests or protests via signs, one-word spoken utterances, or his iPad-based speech-generating device. Typically when the staff could not understand his signs or one-word spoken utterances, Max was prompted to use his iPad for clarification.
Max had no difficulty ambulating about his environment but did require 24-hour supervision and support for activities of daily living. He was supported in a 1:1 staff ratio in the group home. He was very reliant on routine, consistency, and structure in his daily life. If something changed in his routine or there was an event he looked forward to (e.g., Halloween, visiting his family’s home), he could become anxious and make perseverative requests for the event. Group home staff members reported that Max participated in some team sports (e.g., soccer, basketball). However, he was reported to prefer non-team activities, such as walking, biking, watching movies (e.g., Toy Story), reading books (e.g., Berenstein Bear Book), painting, playing Uno, and playing on the computer (e.g., watching youtube videos on the computer). In addition, he liked eating and enjoyed eating outside.
Max was referred for intervention by his group home manager, who sought assistance in addressing his ongoing severe self injury (e.g., hitting himself on the head, legs, or onto the surface) and aggressive behavior (e.g., hitting, kicking, pinching others, throwing and/or breaking objects or property) that had resulted in injuries to both himself and others. Prior to the beginning of this investigation, Max was prescribed medication (i.e., fluoxetine 40 mg, risperidone 6 mg or 1 mg as needed for agitation, gabapentin 1200 mg, and divalproex 2000 mg) to help control his problem behavior. Despite the medication regimen, the staff reported that he still engaged in severe problem behavior. At the time of the study, the instructional objectives proposed by his school and the group home mainly focused on addressing his emotional regulation and expressing wants and needs in respectful and effective ways.
Settings and Materials
All procedures were implemented in Max’s group home that served 15 residents, with an approximately 1:1 or 1:2 staff-resident ratio. Max lived in a four-person apartment in the group home. The experimenters collected functional analysis data when the group home staff worked with Max in areas of the group home that included his bedroom, the living room of his apartment, laundry room, and computer room of the group home. Intervention was implemented by the group home staff. During each intervention session, Max sat in a chair at the end of the table and the group home staff sat beside him, while the experimenter(s) sat at the other side of the table.
Preferred food items serving as intervention materials were kept on the table out of Max’s reach but within his view. Food items were selected based on staff suggestions of reinforcing items followed by direct observations of Max in his natural environment. A preintervention reinforcer sampling procedure was also implemented in accordance with a protocol described by Fisher et al. (1992).
Dependent Measures and Definitions
Dependent variables included; (a) the occurrence of problem behavior (recorded using a 10 s partial-interval recording system throughout the functional analysis, TFD intervention, and component analysis), and (b) the latency to the occurrence of problem behavior (recorded in seconds using a digital timer throughout baseline, TFD intervention, and component analysis). Specifically, Max’s problem behavior consisted of self-injury, aggression, and perseverative requests. Self-injury was defined as hand-to-head, head-to-surface, and/or closed fist-to-leg hits. Aggression was defined as head butting, hitting, kicking, and/or pinching others, and/or hitting, kicking, throwing and/or breaking objects or property. Perseverative requests were defined as any request for an alternative activity or item that was unrelated to the activities or tasks at hand that occurred within 5 min of an initial request. Any time Max engaged in any of these three responses during a 10 s interval, the experimenter recorded the occurrence of problem behavior for that interval. Latency to the occurrence of problem behavior was defined as the interval between the start of the digital timer and the first occurrence of any of Max’s problem behavior as defined above. Notably, the latency to problem behavior was estimated through the 10 s partial-interval recording system. If the first occurrence of problem behavior was observed in the first 10 s interval, the latency was recorded as 10 s. Likewise, if it was observed in the second 10 s interval, the latency was recorded as 20 s, and so forth.
Independent Variables
Two independent variables included (a) a TFD procedure with a combined use of general and explicit delay cues, and (b) a TFD procedure only with the general delay cue. Specifically, the general delay cue was the delivery of a spoken cue (e.g., “just a little while longer”). The explicit delay cue was the delivery of 16 or 12 tokens onto a token board to mark the passage of time at a variable interval schedule of approximately 30 s. The interventionist began with 16 tokens on a 4 by 4 token board during the first intervention session, and then thinned it to 12 tokens on a 3 by 4 token board upon learning that the interventionist had inadvertently successfully used 12 tokens in the second intervention session. No effort was made to further thin the token use. During intervention, the combination of the general and explicit delay cues was applied. During the component analysis, the explicit delay cue was isolated and evaluated apart from the combined delay cues.
Experimental Design
The study was conducted in three phases. During Phase I, an antecedent-based experimental analysis was implemented in a multielement design to examine the conditions under which problem behavior was most likely to occur. During Phase II, a TFD intervention with the combined use of general and explicit delay cues was implemented and evaluated with a changing criterion design until Max was able to wait for preferred items for 10 min with no problem behavior across two consecutive sessions. During Phase III, an ABA withdrawal design was implemented to briefly examine whether the general delay cue was sufficient for the maintenance of the effectiveness of the TFD intervention.
Procedures
Phase I: Functional Analysis
For Max, an antecedent-based analysis (Anderson and Long 2002; Carr and Durand 1985) was implemented. The antecedent-based analysis allows observers to collect data on target behavior in the context of an individual’s naturally occurring activities, and consists of systematically manipulating antecedent variables but allowing the consequences to vary. An antecedent-based functional analysis was utilized in this study because Max’s group home staff had concerns about the possibility of a prolonged outburst following reinforcement of his problem behavior if an analogue consequence-based functional analysis (e.g., Iwata et al. 1982/1994) were implemented. During the antecedent-based analysis, Max was exposed repeatedly to four different antecedent conditions: play, no attention, demand, and restricted access to tangible. Table 1 lists detailed descriptions of the procedures for each condition.
In general, sessions were conducted during times of the day when activities pertaining to each antecedent condition normally occurred. Specifically, the play condition was conducted when it was time for Max to watch computer videos or movies with the staff in the computer room or his bedroom, to establish the antecedent of an enriched environment with available preferred items or activities and attention. The no attention condition was conducted when it was time for him to watch computer videos or movies alone in the computer room or his bedroom, to establish the antecedent of available preferred activities with no demands and no staff attention. The demand condition was conducted when it was time for him to do laundry in the laundry room or vacuuming in the living room, to establish the antecedent of task demands with an expectation of completion of household chores that were commonly required. The restricted access to tangible condition was conducted when it was time for him to wait for dinner at the dinner table in the living room or wait for the staff to turn on the computer for computer videos in the computer room for at least 5 min, to establish the antecedent of restricted access to preferred tangible items or activities.
Prior to each session, group home staff members were given specific instructions about the antecedent condition and were asked to respond to the problem behavior as they typically would (see Table 1). Each observation session lasted 5 min, unless the severity of self-injury or aggression led to bleeding that required immediate termination of the session, or the antecedent events changed naturally (e.g., Max completed the demands provided by the staff or consumed all edible items offered within 5 min). Bleeding occurred only once across all functional analysis sessions. It occurred in the condition of restricted access to tangible and in the final seconds of the session so session termination was not necessary.
Phase II: TFD Intervention with General and Explicit Delay Cues
The data from the restricted access to tangible condition served as the baseline data. For this evaluation, a TFD intervention with a combined use of general and explicit delay cues was implemented. An intervention session was implemented during each of 4 days and each session lasted 10 min.
The interventionist began each session by placing a plastic box containing an array of 5 to 7 preferred items (e.g., pop, cookies, chips, candy, chocolate) on the table, within Max’s reach. Then the interventionist said “show me what you want” while pointing to the box. After Max chose one item in the box by pointing at it, the interventionist said “OK. You want (name of object that Max had selected). You can wait just a bit.” Next, the interventionist moved the box out of Max’s reach on the table but within his view, and started the digital timer that had been set for 10 min. Throughout each 10 min session, the digital timer was kept so that only the interventionist could see it. A token board with 16 or 12 (see the prior explanation for the range) marked areas corresponding to the placement of tokens was placed on the table within the interventionist’s reach and Max’s view. The interventionist started counting in head, “Mississippi one, Mississippi two, … Mississippi thirty.” Contingent on approximately 30 s passing without problem behavior, the interventionist placed a token onto the token board and said “just a little while longer.” This continued until all 16 or 12 tokens were placed onto the token board so that all marked areas on the token board were fully occupied.
In the event that Max engaged in problem behavior, no token was delivered and the interventionist ignored the behavior and delivered a verbal redirection (“you need to wait for it”) in a neutral voice while pointing to the token board. Then, the interventionist re-started counting in head, “Mississippi one, Mississippi two, … Mississippi thirty.” Contingent on another approximately 30 s passing without problem behavior, the interventionist delivered a token onto the token board. The way the interventionist counted ensured that there was a waiting duration of approximately 30 s with no problem behavior prior to the delivery of a token. This participant’s performance resulted in the interventionist being able to provide all of the tokens throughout all 10 min sessions. The interventionist placed the last token onto the token board right before or when the timer rang signaling the end of each 10 min session, and said “Good waiting. You can have it now.” Then the interventionist handed Max the preferred item he selected at the beginning of the session for his consumption.
Phase III: Component Analysis of the Delay Cues
The initial TFD intervention with the general and explicit delay cues was implemented until Max could wait for 10 min with no problem behavior across two consecutive sessions. Two weeks later, the separate effects of the explicit delay cue were examined through a brief ABA withdrawal design across three consecutive 10 min sessions. The condition of TFD intervention with the combined use of the general and explicit delay cues was implemented as previously described.
During the withdrawal condition that involved the TFD intervention with only the general delay cue, the token board and tokens were not used or visible. At the beginning of the session, the interventionist instructed Max to choose a preferred item from an array of 5 to 7 objects and then told Max that he needed to wait. Throughout the session, contingent on an interval of approximate 30 s passing, the interventionist said “just a little while longer” when Max did not engage in any problem behavior. The interventionist delivered the spoken cue 15 times throughout the 10 min session. In the event that Max engaged in problem behavior, the interventionist ignored it and delivered a verbal redirection (“you need to wait for it”) in a neutral voice. When the timer rang, the interventionist said “Good waiting. You can have it now.” Then the interventionist handed Max the preferred item he selected at the beginning of the session.
Interobserver Agreement (IOA)
Response Reliability
A second observer independently recorded responses for a minimum of 50 % of all sessions, for each target dependent variable, throughout each phase of the study (functional analysis, TFD intervention, and component analysis). Agreement was computed by dividing agreements by agreements plus disagreements and multiplying by 100 for the occurrence of problem behavior. An agreement was scored if both observers recorded the same response emitted by Max for a given interval. A disagreement was scored when one observer coded an event as occurring in an interval, but the second observer did not code the same event in the same interval. Agreement for the latency to the occurrence of problem behavior was calculated by dividing the number of intervals with agreement by the total number of intervals with agreements plus disagreements and multiplying by 100. The IOA results are shown in Table 2.
Procedural Fidelity
Procedural fidelity involved task analyzing each step of the functional analysis, intervention, and component analysis procedures being implemented. Using an experimenter-developed checklist, a second observer independently observed the interventionist’s behavior for a minimum of 50 % of all sessions, throughout each phase of the study. The checklist for the functional analysis listed six steps including, (a) arranging the condition according to the time of the day when Max was scheduled for certain activities; (b) delivering the directive correctly to Max as instructed by the experimenter; (c) providing attention (e.g., verbal or nonverbal directions, praise statements) in accordance to the specific antecedent condition; (d) delivering demands in accordance to the specific antecedent condition; (e) providing access to tangible in accordance to the specific antecedent condition; and (f) addressing problem behavior as normal if problem behavior occurred. The checklist for TFD intervention and component analysis listed seven intervention procedures of the study including asking the participant to select a preferred item, moving the box containing preferred items out of the participant’s reach but within his view after his selection, starting the digital timer after delivering the directive “You can wait just a bit”, delivering the delay cue correctly, addressing problem behavior (if any) correctly, delivering the release cue right before or when the digital timer rang, and providing the access to the selected item at the end of the session. A second observer simultaneously scored the accuracy of implementation of each procedural step as an agreement or disagreement. At the end of the session, an item-by-item agreement was calculated (agreements divided by agreements plus disagreements multiplied by 100). Procedural fidelity results are also shown in Table 2.
Results
Functional Analysis
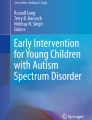
Figure 1 shows that the occurrence of problem behavior was most elevated during restricted access to tangibles (M = 24 %; range 7–50 %), and was at or near zero in the other three conditions. As Max exhibited more problem behavior when his access to preferred items or activities was restricted, the results suggested a functional relation between problem behavior and access to preferred activities. Thus, Max’s problem behavior appeared to be, at least in part, tangibly maintained.

Functional analysis results
TFD Intervention with the Combined Use of General and Explicit Delay Cues
The left side of Fig. 2 shows that during the baseline, Max was only able to wait for access to preferred items or activities approximately 37 s (range 10–90 s) prior to engaging in problem behavior. Throughout four sessions of the TFD intervention with the general and explicit delay cues, Max learned to wait for access to preferred items for 10 min without problem behavior quickly. Compared to the baseline, the occurrence of problem behavior during the TFD intervention decreased to a much lower level (M = 2 %; range 0–6 %).

TFD intervention and component analysis results. The circle with a line through it indicates that problem behavior did not occur during the 10 min session
Component Analysis of Delay Cues
The component analysis was intended to examine the effects of the explicit delay cue by separating it from the combined cues, and explore whether the general delay cue was sufficient for the maintenance of the effectiveness of the TFD intervention. The right side of Fig. 2 depicts the component analysis results for Max across three consecutive 10-min sessions. No problem behavior occurred when a TFD intervention with both the general and explicit cues was implemented. By contrast, problem behavior occurred in 35 % of the observed intervals when the explicit delay cue (the token board and tokens) was removed (i.e., leaving only a general delay cue “Just a little while longer”). In addition, the latency data, depicted on the right vertical axis, indicated that Max engaged in no problem behavior for the entire 10-min session when both the general and explicit delay cues were applied. Conversely, the latency to problem behavior was only 30 s when the explicit delay cue was removed.
Taken together, these results suggest that the TFD intervention using a combined delay cues (i.e., general and explicit delay cues) was effective in reducing Max’s problem behavior and increasing the length of appropriately waiting for preferred items. Further, the component analysis demonstrated that during maintenance the TFD intervention effect was relatively diminished when the explicit delay cue was removed from the combined delay cues.
Discussion
Results from the current investigation provide evidence for the utility of a TFD intervention strategy in addressing problem behavior in an adolescent with autism. This outcome provided corroboration of previous research findings (e.g., Hong et al. 2014; Reichle et al. 2010). Furthermore, this study provided some preliminary evidence on the importance of the explicit delay cue (i.e., the token board and tokens in this study) among the combined delay cues in obtaining better intervention effect. In the current investigation, the TFD intervention with only the general delay cue (i.e., only the verbal cue in this study) was less optimal than the combined explicit and general delay cues during the maintenance phase of intervention. It is possible that the efficacy of an explicit delay cue rests in the learner’s ability to monitor the amount of time or effort of engagement required prior to reinforcement delivery. In this sense, it may be much like an adult who is driving and begins to worry that he or she has followed an incorrect branch in the road; however, upon seeing a road sign indicating that he or she made the correct turn, ceases to worry. Of course a vital component of any signaled delay procedure involves making the learner attend to the delay cue associated with the delivery of reinforcement while at the same time making engagement in problem behavior less efficient in accessing reinforcement. In this sense, a TFD procedure should really be thought of as a treatment package rather than just a single cue.
In spite of the evidence generated in the current study, several limitations require attention. First, an antecedent-based functional analysis was used to examine the potential function(s) of the participant’s problem behavior, lessening the certainty of deriving a causal functional relation compared to a consequence-based functional analysis. Second, the intervention was only implemented in a quiet room in the group home. Further examinations of the effectiveness of the intervention in other settings of the group home (e.g., having access to you tube videos on the computer in the computer room) would help expand the utility of the TFD intervention. Third, the current study did not examine whether the explicit delay cue would be sufficient for obtaining the intervention effect (although this was found to be the case in Reichle et al. 2010). Finally, only one adolescent participated in the study, restricting the generality of findings to other adolescents with autism who have similar problem behavior maintained by access to preferred items or activities.
Future investigations should consider replications with a greater number of adolescents with autism. Additionally, it would be important to extend this intervention to behavior maintained by escape and attention seeking/maintaining in addition to a tangible function. Also, it is necessary to examine how much exposure to the TFD intervention using only a general delay cue may be sufficiently for the maintenance of the intervention effects. Finally, it is important to consider extending demonstrations of the efficacy of a TFD procedure in slightly different applications related to functional communication training. For instance, a TFD procedure can be used not only to extend waiting duration or engagement but to teach a learner to moderate his or her use of a communicative alternative to problem behavior. Reichle and Wacker (2014) described procedures in which a TFD procedure can be implemented after a mand has been produced. Over time, the delay may be increased between the TFD and mand. Thus, over time, the learner attends increasingly to the delay cue, learning that producing a mand does not result in immediate reinforcement if it occurs too early in an activity. In this way, a larger number of diverse applications of TFD procedures may be accumulated for learners with ASD and other developmental disabilities.
References
Anderson, C. M., & Long, E. S. (2002). Use of a structured descriptive assessment methodology to identify variables affecting problem behavior. Journal of Applied Behavior Analysis, 35(2), 137–154.
Bruininks, R. H., Woodcock, R. W., Weatherman, R. F., & Hill, B. K. (1996). Scales of independent behavior – Revised (SIB – R). Itasca: Riverside Publishing.
Carr, E. G., & Carlson, J. I. (1993). Reduction of severe behavior problems in the community using a multicomponent treatment approach. Journal of Applied Behavior Analysis, 26(2), 157–172.
Carr, E. G., & Durand, V. M. (1985). Reducing behavior problems through functional communication training. Journal of Applied Behavior Analysis, 18(2), 111–126.
Carr, E. G., Levin, L., McConnachie, G., Carlson, J. I., Kemp, D. C., & Smith, C. (1994). Communication based intervention for problem behavior: A user’s guide for producing positive change. Baltimore: Paul H. Brookes.
Fisher, W. W., Piazza, C., Bowman, L., Hagopian, L., Owens, J., & Slevin, I. (1992). A comparison of two approaches for identifying reinforcers for persons with severe and profound disabilities. Journal of Applied Behavior Analysis, 25, 491–498.
Fisher, W. W., Thompson, R. H., Hagopian, L. P., Bowman, L. G., & Krug, A. (2000). Facilitating tolerance of delayed reinforcement during functional communication training. Behavior Modification, 24, 3–29.
Grey, I., Healy, O., Leader, G., & Hayes, D. (2009). Using a time timer™ to increase appropriate waiting behavior in a child with developmental disabilities. Research in Developmental Disabilities: A Multidisciplinary Journal, 30, 359–366.
Hong, E. R., Neely, L., Rispoli, M. J., Trepinski, T. M., Gregori, E., & Davis, T. (2014). A comparison of general and explicit delay cues to reinforcement for tangible-maintained challenging behavior. Developmental Neurorehabilitation. doi:10.3109/17518423.2013.874378.
Iwata, B. A., Dorsey, M. F., Slifer, K. J., Bauman, K. E., & Richman, G. S. (1994). Toward a functional analysis of self-injury. Journal of Applied Behavior Analysis, 27, 197–209. Reprinted from Analysis and Intervention in Developmental Disabilities, 2, 3–20, 1982.
Kemp, D. C., & Carr, E. G. (1995). Reduction of severe problem behavior in community employment using a hypothesis-driven multicomponent intervention approach. Journal of the Association for Persons with Severe Handicaps, 20, 229–247.
Kern, L., Carberry, N., & Haidra, C. (1997). Analysis and intervention with two topographies of challenging behavior exhibited by a young woman with autism. Research in Developmental Disabilities, 18, 275–287.
Reichle, J. & Wacker, D. (2014). Functional communication training. Unpublished manuscript. Minneapolis, MN: University of Minnesota.
Reichle, J., Johnson, L., Monn, E., & Harris, M. (2010). Task engagement and escape maintained challenging behavior: differential effects of general and explicit cues when implementing a signaled delay in the delivery of reinforcement. Journal of Autism and Developmental Disorders, 40, 709–720.
Vollmer, T. R., Borrero, J. C., Lalli, J. S., & Daniel, D. (1999). Evaluating self-control and impulsivity in children with severe behavior disorders. Journal of Applied Behavior Analysis, 32(4), 451–466.
Wechsler, D. (2004). The Wechsler intelligence scale for children—fourth edition. London: Pearson Assessment.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Chen, M., McComas, J.J., Reichle, J.E. et al. Brief Component Analysis to Identify the Active Variable in the Maintenance of Tolerance for Delay of Reinforcement Intervention for an Adolescent with Autism. J Dev Phys Disabil 27, 393–404 (2015). https://doi.org/10.1007/s10882-015-9422-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10882-015-9422-8