
Abstract
This meta-analysis was a systematic review of evidence on the effects of mindfulness-based stress reduction (MBSR) and mindfulness-based cognitive therapy (MBCT) on quality of life (QOL), pain, fatigue, anxiety, and depression in cancer patients. Until July 2020, PubMed, Cochrane Library, and Embase were searched for randomized controlled trials (RCTs). The study included 18 RCTs. The MBSR/MBCT intervention resulted in a significant effect on QOL (SMD 0.80, CI 0.28, 1.32, I2 = 94%). In subgroup analysis, MBSR/MBCT interventions had a significant effect in the early cancer stage on anxiety (SMD − 3.48, CI − 4.07, − 2.88), and QOL (SMD 4.30, CI 3.62, 4.99); in alleviating decreasing pain (SMD − 0.42, CI − 0.70, − 0.14) within 4 weeks after the end of intervention, and alleviating fatigue in younger participants (SMD − 0.64, CI − 1.09, − 0.19). MBSR/MBCT has short-term effects on cancer patients, especially in younger patients and early cancer stages.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Cancer was the second worldwide leading cause of death and is responsible for an estimated 9.6 million deaths in 2018 (World Health Organization, 2018). Cancer is mainly treated by surgery, chemotherapy, radiotherapy, and targeted therapy. During disease progression and treatment period, these patients can experience great physical and psychological trauma, which often include pain, anxiety, depression, fatigue, and reduced quality of life (QOL). These physical and psychological effects may be temporary or last for long periods and affect the willingness of patients to continue therapy and the efficacy of the treatment owing to treatment interruption, treatment discontinuation, reduced therapeutic efficacy, increased comorbidities, and reduced survival rate (Bower, 2014; Tsaras et al., 2018). Michaelides et al. reported that anxiety, fear, and stress are shown to be mediators in the causal pathway between pain and disability (Michaelides and Zis 2019). While treating cancer patients, it is necessary to take care of patients' physical health and psychological frustration, so as to improve the patients' quality of life and optimize the patients' treatment effect. Mindfulness-based therapy (MBT) or mindfulness-based intervention (MBI) is a form of non-invasive cognitive and psychological treatment that improves mindfulness. Lindsay et al. said that mindfulness is a way of paying attention to present-moment experience with a mental stance of receptivity and acceptance (Lindsay & Creswell, 2017). MBT can help patients to achieve psychological peace, effectively reduce anxiety, depression, and other negative emotions and pain, and improve QOL (Schellekens et al., 2017). The most commonly described MBTs include mindfulness-based stress reduction (MBSR) and mindfulness-based cognitive therapy (MBCT) (Lindsay & Creswell, 2017). Currently, literature on the effects of mindfulness in cancer patients mainly involves breast cancer patients (Haller et al., 2017; Zhang et al., 2015, 2017), and outcome indicators are limited to anxiety, depression, and QOL (Zhang et al., 2015, 2017). From 2009 to 2016, a search for papers yielded few related studies for inclusion in the literature review. In addition, the results reported for MBT are inconsistent. Conversely, Johannsen et al. showed that mindfulness can effectively alleviate anxiety and depression and improve the QOL of cancer patients, and Bower et al. showed that mindfulness can effectively alleviate pain, fatigue, and depression in cancer patients. Other studies, however, found that mindfulness does not exhibit any significant effects on the alleviation of pain (Lengacher et al., 2009), fatigue, anxiety, depression (Reich et al., 2017), and QOL (Lengacher et al., 2009; Reich et al., 2017). Therefore, in this study, we expanded the examination of the physical and psychological effects of MBT on patients diagnosed with all types of cancer to include its effects on five major aspects (QOL, pain, fatigue, anxiety, and depression). Thus, we updated the literature to include reports up to 2020.
Methods
This systematic review was conducted using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (PRISMA) (Moher et al., 2010) and the Cochrane Collaboration recommendations (Cochrane, 2019).
Search Strategy
The search strategy was based on the PICO using pre-specified search terms (Kang, 2016) to identify randomized controlled trials (RCTs). The inclusion criteria for PICO are as follows: (1) Types of participants: Adults 20 year old or older with a clinical diagnosis of cancer. (2) Types of interventions: Studies should have examined MBSR or MBCT as a main intervention. Non-face-to-face interventions such as online interventions were also excluded. Adapted MBSR or MBCT programs were allowed except mindfulness awareness practices (MAPS) (Bower, 2014), mindfulness-based cancer recovery (MBCR) (Blaes et al., 2016), and MBSR-added conscious yoga (Rahmani & Talepasand, 2015). (3) Types of comparisons: The control groups included at least one non-MBT such as usual care (no other treatment or wait-list-defined treatment as usual). (4) Types of outcomes: The primary outcome was the improvement of QOL which was patient self-reported, health related, or cancer related at postintervention. The secondary outcomes included pain, fatigue, anxiety, and depression symptom improvement.
A search of PubMed, Cochrane Library, and Embase for publications from the first available date to July 2020 with no language restrictions was conducted using the search terms: (“mindfulness-based cognitive therapy” or “mindfulness-based stress reduction” or “MBSR” or “mindfulness-based cognitive therapy” or “MBCT” or “mindfulness cognitive therapy”) and (“pain” or “quality of life” or “depression” or “anxiety” or “fatigue”) and “cancer”. In addition, we also found related systematic reviews and meta-analyses from these databases. Then, we checked their reference lists, as well as those of RCTs included in the review.
Data Extraction
Two authors (HHC and YLC) used the inclusion criteria to independently select the studies. From included studies, we extracted basic characteristics including first author’s name, year of publication, countries of study conducted, population, number of participants, age, gender distribution, duration of treatment, type of intervention, outcome variables, and the methodological quality. Quantitative data were extracted to calculate effect sizes. If multiple measurement tools were used in studies, we selected one measurement method that was deemed the most suitable for each of the outcome domains. Time point for outcome assessment was designed as postintervention. If multiple time point postintervention data were reported, we evaluated the data of the immediate time points up to 16 weeks after intervention initiation. If the results of the same studies were reported in more than one publication, we extracted result from the newest reporting study. Any disagreements were resolved by discussion or by seeking an independent opinion from a third author (LYL).
Statistical Analysis
Review Manager (RevMan) (The Nordic Cochrane Centre, 2012) was used for the meta-analysis. The results with p values (two-tailed) < 0.05 were considered statistically significant, except for the heterogeneity and publication bias tests. Inter-study heterogeneity was measured using Cochran’s Q statistical test. Substantial statistical heterogeneity between studies was defined as a statistically significant χ2 value (p < 0.10). I2 values of 0–24.9%, 25–49.9%, 50–74%, and 75–100% denoted no, low, moderate, and high heterogeneity (Higgins et al., 2003), respectively. A random effects model was used to pool the results. As all variables in the included studies had continuous data with different scales, we used standard mean difference (SMD) with 95% confidence interval (CI) to analyze the effect size of the studies. For QOL, positive SMDs indicated greater improvements due to mindfulness interventions. For pain, fatigue, anxiety, and depression, negative SMDs indicated greater reductions. Subgroup analyses were carried out due to the study characteristics to investigate the sources of heterogeneity, which included different MBT types (MBCT or MBSR), intervention programs (original or adapted), mean age of participants (> 50 year old or ≤ 50 year old), cancer stage, and assessment short-term effects after intervention (immediate, within 4 weeks after the end of intervention, and at 8 weeks after the end of intervention). The presence of publication bias was investigated by visual inspection of the funnel plots (Suurmond et al., 2017).
Risk of Bias Within Studies and Grades of Recommendation, Assessment, Development, and Evaluation
Two authors (LHL and GLT) evaluated the methodological quality of the included studies for major bias using the criteria developed by Revised Cochrane risk of bias 2.0 (RoB 2.0) (Cochrane, 2019) tool for randomized trials. This is a five-domain process and the risk of bias was rated as low, some concern, or high. Any judgments were rechecked by the review team (LHL and GLT) and discussed until a consensus was achieved. Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) were assessed using the GRADE working group recommendations (Cochrane, 2019). GRADE uses a high baseline rating for RCTs. This rating can be downgraded based on five assessment criteria. The ratings were assessed and discussed by all authors.
Results
Study Selection
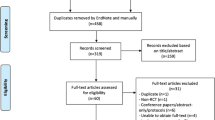
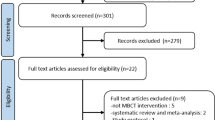
We identified 869 studies from electronic searches, of which 481 non-RCTs and 168 duplicates were excluded. After the first round of screening, 194 articles were deemed irrelevant; therefore, we retrieved 26 full-text articles for in-depth consideration. Eight of these articles were excluded for the following reasons: incomplete data (n = 1) and overlapping participants (n = 7). Finally, 18 independent RCTs were included in our systematic review. The study selection process is shown in Fig. 1.

Flow chart summarizing study identification and selection
Characteristics of Included Studies
The characteristics of the included studies are presented in Table 1. All studies were RCTs comparing MBSR or MBCT with “a usual care or waiting list or no treatment” control condition. The interventions included 14 studies of the MBSR program and 4 of the MBCT program. Nine studies consisted of women with breast cancer (Henderson et al., 2012; Hoffman et al., 2012; Johannsen et al., 2016; Kenne Sarenmalm et al., 2017; Lengacher et al., 2014; Reich et al., 2014, 2017; Wurtzen et al., 2013; Zhang et al., 2017), and the other studies included patients with lung cancer (n = 1) (Schellekens et al., 2017), thyroid cancer (n = 1) (Liu et al., 2019), and mixed-type cancer (n = 7) (Branstrom et al., 2010; Foley et al., 2010; Johns et al., 2015; Kingston et al., 2015; Lerman et al., 2012; Speca et al., 2000; van der Lee & Garssen, 2012). All interventions of MBT (MBCT or MBSR) included 5 adapted programs (< 8 week) (Johns et al., 2015; Lengacher et al., 2014, 2016; Reich et al., 2014; Speca et al., 2000), 4 adapted programs (8 weeks) (Bränström et al., 2010; Henderson et al., 2012; Kingston et al., 2015; Zhang et al., 2017), and 9 original programs (8 weeks) (Foley et al., 2010; Hoffman et al., 2012; Johannsen et al., 2016; Kenne Sarenmalm et al., 2017; Lerman et al., 2012; Liu et al., 2019; Schellekens et al., 2017; van der Lee & Garssen, 2012; Wurtzen et al., 2013). The mean age of participants in these studies was classified as above 50 year old for 12 studies (Branstrom et al., 2010; Foley et al., 2010; Johannsen et al., 2016; Johns et al., 2015; Kenne Sarenmalm et al., 2017; Lengacher et al., 2009; Lerman et al., 2012; Reich et al., 2014, 2017; Schellekens et al., 2017; van der Lee & Garssen, 2012; Wurtzen et al., 2013) and below or equal to 50 year old for 6 studies (Henderson et al., 2012; Hoffman et al., 2012; Kingston et al., 2015; Liu et al., 2019; Speca et al., 2000; Zhang et al., 2017). The time to post-treatment was immediately after the end of intervention (n = 14; Johannsen et al., 2016; Johns et al., 2015; Kenne Sarenmalm et al., 2017; Kingston et al., 2015; Lengacher et al., 2009; Lerman et al., 2012; Liu et al., 2019; Reich et al., 2014, 2017; Schellekens et al., 2017; Speca et al., 2000; van der Lee & Garssen, 2012; Wurtzen et al., 2013; Zhang et al., 2017), within 4-week postintervention (n = 3; Branstrom et al., 2010; Foley et al., 2010; Hoffman et al., 2012), and at 8-week post intervention (n = 1; Henderson et al., 2012). Cancer stages were classified into three groups. These included “early stage” defined according to the study of Henderson et al., “metastasis stage” defined as including participants of cancer stage IV (n = 5; Foley et al., 2010; Johns et al., 2015; Lerman et al., 2012; Schellekens et al., 2017; Speca et al., 2000), and the others were classified as “non-metastasis stage” (n = 7; Hoffman et al., 2012; Johannsen et al., 2016; Lengacher et al., 2009; Reich et al., 2014, 2017; Wurtzen et al., 2013; Zhang et al., 2017).
Risk of Bias Within Studies and Grades of Recommendation, Assessment, Development, and Evaluation
In four studies, the overall risk of bias was low, whereas in other studies, it was high. As shown in Figures S1–S2, most included RCTs were categorized as being at low risk of bias regarding the domains of follow-up compared with others. The risk of bias was high or unclear for performance, measurement, and reporting in a majority of studies. Risk of allocation sequence concealed was high in the study of Kingston et al. Risk of performance bias was high for 4 studies (no blinding of participants and personnel), 2 studies (no blinding of outcome assessment), and 8 studies (selective reporting). As shown in Table S1, the GRADE of evidence downgraded from high to low when unexplained heterogeneity and no implementation or information of blinding or allocation concealment were observed. A downgrading from high to moderate occurred when a study had high heterogeneity to accurately assess publication bias using funnel plots.
Publication Bias
Figure S3 shows the funnel plots of the studies reporting depression. The funnel plot was asymmetrical and did not show a small study with a negative size effect on the depression results.
Meta-analysis
In this systematic review, 18 RCTs that included 2033 patients were used to compare the effects of MBCT/MBSR to waiting list, or usual care. The data measured at postintervention were used to depict all outcomes. A meta-analysis was carried out based on the primary outcome, QOL, and secondary outcomes, which were pain, fatigue, anxiety, and depression.
Primary Outcome Measure
Quality of Life (QOL)
From the 10 papers, 1192 subjects were included in the meta-analysis (Fig. 2). The results showed that MBCT/MBSR intervention can significantly improve the QOL, with an SMD of 0.80 (95% CI 0.28–1.32, p < 0.001; I2 = 94%).

Forest plot of effects of MBCT/MBSR on the primary (QOL, n = 10)
Secondary Outcome Measure
Pain
From the four papers, 587 subjects were included in the meta-analysis (Figure S4a). The results showed that MBT intervention can significantly alleviate pain, with SMD of − 0.27 (95% CI − 0.44 to − 0.09, p < 0.01; I2 = 11%).
Fatigue
From the eight papers, 944 subjects were included in the meta-analysis (Figure S4b). The results showed that MBT intervention can significantly alleviate fatigue, with SMD of − 0.56 (95% CI − 0.84 to − 0.28, p < 0.001, I2 = 73%).
Anxiety
From the 14 papers, 1620 subjects were included in the meta-analysis (Figure S4c). The results showed that MBT intervention can significantly decrease anxiety, with SMD of − 0.53 (95% CI − 0.87 to − 0.19, p < 0.01, I2 = 90%).
Depression
From the 12 papers, 1433 subjects were included in the meta-analysis (Figure S4d). The results showed that MBT intervention can significantly decrease depression, with SMD of − 0.49 (95% CI − 0.70 to − 0.28, p < 0.001, I2 = 70%).
Subgroup Analyses
There was significant heterogeneity among the included studies in the result of MBT intervention for QOL, fatigue, anxiety, and depression. We performed subgroup analysis to figure out the source of heterogeneity.
Type of Intervention
In the subgroup analysis, there were no significant statistical differences found. However, there was a better trend in MBSR than MBCT intervention on improving the QOL (SMD 0.96, 95% CI 0.21–1.71, I2 = 96% vs. 0.45, 95% CI 0.21–0.69, I2 = 0%) (Fig. 2), and alleviating anxiety and depression (Figure S4c, S4d). There was a better trend in MBCT compared to MBSR intervention on decreasing pain (SMD − 0.55, 95% CI − 0.96 to − 0.15 vs. − 0.20, 95% CI − 0.37 to − 0.02, I2 = 0%) and fatigue (Figs. S4a–4b).
Treatment Programs
All included studies were focused on MBCT/MBSR interventions. These interventions were modified as original and adapted programs. In the subgroup analysis, no significant statistical differences were found, except in terms of improving QOL, the 8-week original plan had better results than the < 8-week adjusted plan (SMD 0.53, 95% CI 0.28–0.78, I2 = 58% vs. 0.11, 95% CI − 0.23 to 0.45; I2 = 51%; p < 0.001). (Table S2).
Short-Term Effects of Intervention
We analyzed short-term effects of intervention and classified it by the evaluation time into three groups: immediately, within 4 weeks, and within 8 weeks after the end of intervention. We found that there was a significant difference between groups in improving the QOL (SMD 0.11, CI − 0.23 to 0.45, I2 = 51% vs. 0.54, CI 0.28–0.79, I2 = 57% vs. 4.30, CI 3.62–4.99, p < 0.001) and alleviating anxiety. The short-term effects of MBT intervention showed a better trend effect within 4 weeks after the end of intervention than immediate effect in decreasing pain (SMD − 0.42, 95% CI, − 0.70 to − 0.14, I2 = 0% vs. − 0.17, 95% CI − 0.37 to 0.03, I2 = 0%) and fatigue (Table S3).
Cancer Stages
We performed the subgroup analysis for different cancer stages depending on early (e.g., study by Henderson et al.), non-metastasis, and metastasis stages. We found a significantly different effect of MBT intervention on QOL (SMD 4.30, CI 3.62–4.99, vs. 0.61, CI 0.23–1.00, I2 = 76% vs. 0.35, CI 0.06–0.64, p < 0.001) and anxiety between cancer stages of patients (Table S4; Fig. 3).

Forest plot of effects of cancer stages on a QOL and b anxiety, QOL quality of life
Age of Participants
The subgroup analysis by age of patients showed that MBT intervention results in younger age groups (mean age ≤ 50 year old) had better trend effect than older age groups (mean age > 50 year old) in improving QOL (SMD 1.93, 95% CI 0.07–3.79, I2 = 98% vs. 0.30, 95% CI 0.10–0.50, I2 = 39%) and alleviating anxiety (SMD − 0.92, 95% CI − 1.77 to -0.06 vs. − 0.23, 95% CI − 0.38 to − 0.09, I2 = 17%) (Table S5).
Discussion
This systematic review provided a comprehensive summary of the currently available RCTs that have explored the effects when MBCT/MBSR is used to alleviate pain, fatigue, anxiety, and depression, and improve QOL in cancer patients. The review included 18 RCTs and was updated to the year 2020. To the best of our knowledge, this is the only systematic review to examine pain alleviation in patients diagnosed with all types of cancer and to carry out a subgroup analysis based on MBCT/MBSR, original/adapted programs, short-term effects of intervention, cancer stages, and participants’ age.
Compared to similar studies, only six systematic reviews have examined the effects of MBSR/MBCT on cancer patients in the last 5 years (Castanhel & Liberali, 2018; Cillessen et al., 2019; Haller et al., 2017; Ngamkham et al., 2019; Schell et al, 2019; Zhang et al., 2019). Of these papers, five mainly examined breast cancer patients (Castanhel & Liberali, 2018; Haller et al., 2017; Ngamkham et al., 2019; Schellekens et al., 2017; Zhang et al., 2019); thus, only one was similar to our study as it was an analysis of patients diagnosed with all types of cancer (Cillessen et al., 2019). Furthermore, future studies are necessary in this area of mindfulness‐based interventions on patients diagnosed with all types of cancer because more than one in three cancer patients have experienced significant levels of psychological distress (Carlson et al., 2004). Mindfulness‐based interventions (MBI) have increasingly been used to reduce psychological distress in patients after cancer treatment. Cillessen et al. (2019) examined the pooled effects of several types of MBI, which included MBSR, MBCT, mindfulness-based art therapy (MBAT), and mindfulness-based cancer recovery (MBCR) on the decrease of combined measures of distress (e.g., the Hospital Anxiety and Depression Scale, HADS total score), anxiety, depression, fear of cancer recurrence, fatigue, sleep disturbances, and pain. MBIs appear efficacious in reducing psychological distress, but the effects were of small magnitude. However, MBIs adhering closely to the original interventions (MBSR and MBCT) appeared to have larger effects. In our study, we expanded the scope to discuss the different effects of the MBSR or MBCT interventions on both physical and psychological problems. There were no significant statistical differences between MBCT and MBSR intervention. In the subgroup analysis, MBSR and MBCT were modified as original and adapted programs and the 8-week original plan had better results than the < 8-week adjusted plan in improving QOL. This result warrants confirmation with future research that conducts a large clinical trial and that also monitors patients’ adherence to the intervention program.
This meta-analysis showed great heterogeneity between studies in the statistical analysis results for QOL, fatigue, anxiety, and depression except pain. When patients were classified by type of intervention, treatment programs, short-term effects of intervention, cancer stage, and participant’s age, the heterogeneity was decreased in the statistical analysis. A subgroup analysis for the intervention of MBCT and MBSR revealed that MBSR had better trend effect than MBCT in improving QOL, anxiety, and depression. On the contrary, MBCT had better trend effect in improving pain and fatigue in cancer patients. MBSR has been shown to improve mood disorders (Hoffman et al., 2012; Wurtzen et al., 2013) and reduce stress in cancer patients (Branstrom et al., 2010; Speca et al., 2000). Furthermore, MBSR improves physical functioning, which in turn leads to reduced anxiety in women with breast cancer (Lengacher et al., 2014). Evidence from nonrandomized, uncontrolled studies suggests that MBSR could improve the QOL (Branstrom et al., 2012). MBCT and MBSR are similar courses, with a principal difference being that MBCT includes cognitive therapy components, which are not a part of MBSR, and which are particularly relevant for people vulnerable to depression. These are similar to the results for MBSR intervention in our study. However, we could not observe a better effect of MBCT than MBSR intervention for alleviating depression. Only two studies were included in the subgroup analysis of MBCT intervention for depression. The study of Kingston et al. revealed no effect of MBCT intervention compared with usual care, but this small sample size (n = 13) may not be adequately representative of patients diagnosed with all types of cancer.
MBSR/MBCT programs adapted for the cancer context included intervention periods, 6 or 7 classes instead of 8, no retreat, brief psycho-education related to cancer-related fatigue, and shorter-guided home practices (Johns et al., 2015). Although < 8-week adapted programs could improve patient adherence for MBT programs, better trend effects were found for MBT interventions of the 8-week original programs than < 8-week adapted programs for improvement on QOL, pain, fatigue, anxiety, and depression in our meta-analysis. The 8-week original MBSR/MBCT intervention seemed more efficacious than < 8-week adapted programs on both psychological and physical problems.
According to Schell et al.’s meta-analysis, MBSR probably slightly reduces anxiety and depression, and presented an apparent beneficial effect on fatigue at the end of the intervention (12 week). We analyzed short-term effects of intervention in three separate comparisons (< 8 week, 8 week to 12 week, and above 12 week up to 16 week). MBCT/MBSR could persistently improve the QOL, anxiety until 16 weeks, consistently reduce pain and fatigue until 12 weeks, but only alleviate depression sustainably to 8 weeks.
The effects of MBCT/MBSR can be sustained, which may be related to the improvement of mindfulness skills after a period of practice. The study by Cillessen et al. (2019) showed that there was a statistically significant relationship between the improvement of mindfulness skills and the effect of outcome indicators. More research is needed to confirm it. However, since there were few studies following the effects of more than 8 weeks after the intervention, more research is needed to track the long-term effects. The effect of mindfulness in reducing depression was shown 8 weeks after the intervention, after which the effect declined. This suggests that depression may require further evaluation of its severity and additional treatment (Tiller, 2013) to enhance and maintain the effect of mindfulness therapy.
Cancer stage is also considered a factor affecting MBT intervention effect. We found a significantly different effect of MBSR/MBCT intervention on QOL and anxiety between cancer stages of patients. The MBSR/MBCT intervention had better effect on cancer patients with the early stage than non-metastasis, and metastasis stages. Physicians could give aggressively MBT intervention to cancer patients of early stage.
Psychological stress and depression in young women increase after a diagnosis of cancer compared to older women (World Health Organization, 2018). However, studies with younger participants reported greater reductions in psychological stress post‐intervention (Noone et al., 2018). Our study result showed that younger patients (≤ 50 year old) appeared to benefit more from MBSR/MBCT on QOL, fatigue, and anxiety than older patients (> 50 year old). Clinical oncologists could be advised that younger cancer patients may benefit from MBTs.
Limitations and Recommendations
The limitations of the present study include the overall high risk of bias, great heterogeneity between studies, and it included only four MBCT interventions. The overall high risk of bias was mainly due to no report of methods of sequence generation or allocation concealment, and partial data or usable results reported. The great heterogeneity between studies was observed in the statistical analysis results for QOL, fatigue, anxiety, and depression except pain. Despite our subgroup analysis to decrease heterogeneity, we understand that other factors might also affect short-term and long-term effects of the interventions. The evidence presented here is currently insufficient to draw clear conclusions. Future analysis can be carried out based on the content presented herein, considering standardized evaluation tools, classification of different subjects, and duration of intervention measures. We mainly examined the effects of different mindfulness therapies, including MBSR or MBCT, on psychological and physical improvements in cancer patients. In the future, the effects of comparing MBI with other psychosocial interventions should be examined. A meta-analysis can also be carried out on other outcome indicators, such as sleep quality, stress, and physical function. We can explore the different stages of cancer in patients to verify the effectiveness of MBTs and to explore the difference in the effectiveness of MBT for different degrees of symptoms.
Conclusions
The meta-analysis results showed that MBCT/MBSR can significantly and effectively improve the QOL and decrease the anxiety, depression, pain, and fatigue experienced by cancer patients. To verify our study results, we hope to carry out more comprehensive clinical trials in the future. With respect to the care of cancer patients, establishing standardized and effective psychological and physical treatment regimens will alleviate depression and increase tangible treatment outcomes.
Research Implications
Cancer patients often encounter psychological and physical torture when facing diseases and treatments. It is clinically recommended to applicate of MBSR/MBCT can significantly reduce pain, fatigue, anxiety, depression, and improve the quality of life for cancer patients. The application of the original 8-week mindfulness program was significantly more effective in improving the quality of life of cancer patients than the program less than 8 weeks. For early-stage cancer patients, mindfulness application is significantly better than late-stage patients in improving the quality of life and anxiety. The application of MBSR to cancer patients is significantly better than MBCT in improving the quality of life and anxiety. Clinical professionals choose appropriate mindfulness methods to alleviate patients' psychological and physical discomfort, which will help patients to cope with disease and treatment, improve the quality of life, and thereby, enhance the treatment effects.
Data Availability
Not applicable.
Code Availability
Not applicable.
References
Andersen, S. R., Würtzen, H., Steding-Jessen, M., Christensen, J., Andersen, K. K., Flyger, H., Mitchelmore, C., Johansen, C., Mitchelmore, C., Johansen, C., & Dalton, S. O. (2013). Effect of mindfulness-based stress reduction on sleep quality: Results of a randomized trial among Danish breast cancer patients. Acta Oncologica, 52(2), 336–344. https://doi.org/10.3109/0284186X.2012.745948
Blaes, A. H., Fenner, D., Bachanova, V., Torkelson, C., Geller, M., Haddad, T., Shanley, R., & Kreitzer, M. J. (2016). Mindfulness-based cancer recovery in survivors recovering from chemotherapy and radiation. Journal of Community and Supportive Oncology, 14, 351–358.
Bower, J. E. (2014). Cancer-related fatigue–mechanisms, risk factors, and treatments. Nature Reviews: Clinical Oncology, 11(10), 597–609. https://doi.org/10.1038/nrclinonc.2014.127
Branstrom, R., Kvillemo, P., Brandberg, Y., & Moskowitz, J. T. (2010). Self-report mindfulness as a mediator of psychological well-being in a stress reduction intervention for cancer patients–a randomized study. Annals of Behavioral Medicine, 39(2), 151–161. https://doi.org/10.1007/s12160-010-9168-6
Branstrom, R., Kvillemo, P., & Moskowitz, J. T. (2012). A randomized study of the effects of mindfulness training on psychological well-being and symptoms of stress in patients treated for cancer at 6-month follow-up. International Journal of Behavioral Medicine, 19(4), 535–542. https://doi.org/10.1007/s12529-011-9192-3
Carlson, L. E., Angen, M., Cullum, J., Goodey, E., Koopmans, J., Lamont, L., MacRae, J. H., Martin, M., Pelletier, G., Robinson, J., Simpson, J. S., Speca, M., Tillotson, L., & Bultz, B. D. (2004). High levels of untreated distress and fatigue in cancer patients. British Journal of Cancer, 90(12), 2297–2304. https://doi.org/10.1038/sj.bjc.6601887
Castanhel, F. D., & Liberali, R. (2018). Mindfulness-Based Stress Reduction on breast cancer symptoms: Systematic review and meta-analysis. Einstein, 16(4), eRW4383-eRW4383. https://doi.org/10.31744/einstein_journal/2018RW4383.
Cillessen, L., Johannsen, M., Speckens, A. E. M., & Zachariae, R. (2019). Mindfulness-based interventions for psychological and physical health outcomes in cancer patients and survivors: A systematic review and meta-analysis of randomized controlled trials. Psycho-Oncology. https://doi.org/10.1002/pon.5214
Cochrane. (2019). Cochrane Handbook for Systematic Reviews of Interventions version 6.0 (updated July 2019). Retrieved from http://www.training.cochrane.org/handbook
Foley, E., Baillie, A., Huxter, M., Price, M., & Sinclair, E. (2010). Mindfulness-based cognitive therapy for individuals whose lives have been affected by cancer: A randomized controlled trial. Journal of Consulting and Clinical Psychology, 78(1), 72–79. https://doi.org/10.1037/a0017566
Haller, H., Winkler, M. M., Klose, P., Dobos, G., Kummel, S., & Cramer, H. (2017). Mindfulness-based interventions for women with breast cancer: An updated systematic review and meta-analysis. Acta Oncologica, 56(12), 1665–1676. https://doi.org/10.1080/0284186X.2017.1342862
Henderson, V. P., Clemow, L., Massion, A. O., Hurley, T. G., Druker, S., & Hebert, J. R. (2012). The effects of mindfulness-based stress reduction on psychosocial outcomes and quality of life in early-stage breast cancer patients: A randomized trial. Breast Cancer Research and Treatment, 131(1), 99–109. https://doi.org/10.1007/s10549-011-1738-1
Henderson, V. P., Massion, A. O., Clemow, L., Hurley, T. G., Druker, S., & Hébert, J. R. (2013). A randomized controlled trial of mindfulness-based stress reduction for women with early-stage breast cancer receiving radiotherapy. Integrative Cancer Therapies, 12(5), 404–413. https://doi.org/10.1177/1534735412473640
Higgins, J. P., Thompson, S. G., Deeks, J. J., & Altman, D. G. (2003). Measuring inconsistency in meta-analyses. BMJ, 327(7414), 557–560. https://doi.org/10.1136/bmj.327.7414.557
Hoffman, C. J., Ersser, S. J., Hopkinson, J. B., Nicholls, P. G., Harrington, J. E., & Thomas, P. W. (2012). Effectiveness of mindfulness-based stress reduction in mood, breast- and endocrine-related quality of life, and well-being in stage 0 to III breast cancer: A randomized, controlled trial. Journal of Clinical Oncology, 30(12), 1335–1342. https://doi.org/10.1200/jco.2010.34.0331
Johannsen, M., O’Connor, M., O’Toole, M. S., Jensen, A. B., Hojris, I., & Zachariae, R. (2016). Efficacy of mindfulness-based cognitive therapy on late post-treatment pain in women treated for primary breast cancer: A randomized controlled trial. Journal of Clinical Oncology, 34(28), 3390–3399. https://doi.org/10.1200/jco.2015.65.0770
Johannsen, M., O’Connor, M., O’Toole, M. S., Jensen, A. B., & Zachariae, R. (2018). Mindfulness-based cognitive therapy and persistent pain in women treated for primary breast cancer: Exploring possible statistical mediators: Results from a randomized controlled trial. The Clinical Journal of Pain, 34(1), 59–67. https://doi.org/10.1097/AJP.0000000000000510
Johannsen, M., O’Toole, M. S., O’Connor, M., Jensen, A. B., & Zachariae, R. (2017). Clinical and psychological moderators of the effect of mindfulness-based cognitive therapy on persistent pain in women treated for primary breast cancer - explorative analyses from a randomized controlled trial. Acta Oncologica, 56(2), 321–328. https://doi.org/10.1080/0284186X.2016.1268713
Johns, S. A., Brown, L. F., Beck-Coon, K., Monahan, P. O., Tong, Y., & Kroenke, K. (2015). Randomized controlled pilot study of mindfulness-based stress reduction for persistently fatigued cancer survivors. Psycho-Oncology, 24(8), 885–893. https://doi.org/10.1002/pon.3648
Kang, H. (2016). How to understand and conduct evidence-based medicine. Korean Journal Anesthesiol, 69(5), 435–445. https://doi.org/10.4097/kjae.2016.69.5.435
Kenne Sarenmalm, E., Martensson, L. B., Andersson, B. A., Karlsson, P., & Bergh, I. (2017). Mindfulness and its efficacy for psychological and biological responses in women with breast cancer. Cancer Medicine, 6(5), 1108–1122. https://doi.org/10.1002/cam4.1052
Kingston, T., Collier, S., Hevey, D., McCormick, M. M., Besani, C., Cooney, J., & O’Dwyer, A. M. (2015). Mindfulness-based cognitive therapy for psycho-oncology patients: An exploratory study. Irish Journal of Psychological Medicine, 32(3), 265–274. https://doi.org/10.1017/ipm.2014.81
Lengacher, C. A., Johnson-Mallard, V., Post-White, J., Moscoso, M. S., Jacobsen, P. B., Klein, T. W., Widen, R. H., Fitzgerald, S. G., Shelton, M. M., Barta, M., Goodman, M., & Kip, K. E. (2009). Randomized controlled trial of mindfulness-based stress reduction (MBSR) for survivors of breast cancer. Psycho-Oncology, 18(12), 1261–1272. https://doi.org/10.1002/pon.1529
Lengacher, C. A., Reich, R. R., Paterson, C. L., Ramesar, S., Park, J. Y., Alinat, C., Johnson-Mallard, V., Moscoso, M., Budhrani-Shani, P., Miladinovic, B. Jacobsen, P. B., & Kip, K. E. (2016). Examination of broad symptom improvement resulting from mindfulness-based stress reduction in breast cancer survivors: A randomized controlled trial. Journal of Clinical Oncology, 34(24), 2827–2834. https://doi.org/10.1200/jco.2015.65.7874
Lengacher, C. A., Shelton, M. M., Reich, R. R., Barta, M. K., Johnson-Mallard, V., Moscoso, M. S., Paterson, C., Ramesar, S., Budhrani, P., Carranza, I. and Lucas, J., & Kip, K. E. (2014). Mindfulness based stress reduction (MBSR(BC)) in breast cancer: Evaluating fear of recurrence (FOR) as a mediator of psychological and physical symptoms in a randomized control trial (RCT). Journal of Behavioral Medicine, 37(2), 185–195. https://doi.org/10.1007/s10865-012-9473-6
Lerman, R., Jarski, R., Rea, H., Gellish, R., & Vicini, F. (2012). Improving symptoms and quality of life of female cancer survivors: A randomized controlled study. Annals of Surgical Oncology, 19(2), 373–378. https://doi.org/10.1245/s10434-011-2051-2
Lindsay, E. K., & Creswell, J. D. (2017). Mechanisms of mindfulness training: Monitor and Acceptance Theory (MAT). Clinical Psychology Review, 51, 48–59. https://doi.org/10.1016/j.cpr.2016.10.011
Liu, T., Zhang, W., Xiao, S., Xu, L., Wen, Q., Bai, L., Ma, Q., & Ji, B. (2019). Mindfulness-based stress reduction in patients with differentiated thyroid cancer receiving radioactive iodine therapy: A randomized controlled trial. Cancer Management and Research, 11, 467–474. https://doi.org/10.2147/CMAR.S183299
Michaelides, A., & Zis, P. (2019). Depression, anxiety and acute pain: Links and management challenges. Postgraduate Medicine, 131(7), 438–444. https://doi.org/10.1080/00325481.2019.1663705
Moher, D., Liberati, A., Tetzlaff, J., & Altman, D. G. (2010). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. International Journal of Surgery (london, England), 8(5), 336–341. https://doi.org/10.1016/j.ijsu.2010.02.007
Ngamkham, S., Holden, J. E., & Smith, E. L. (2019). A systematic review: Mindfulness intervention for cancer-related pain. Asia-Pacific Journal of Oncology Nursing, 6(2), 161–169. https://doi.org/10.4103/apjon.apjon_67_18
Noone AM, Howlader N, Krapcho M, Miller D, Brest A, Yu M. (2018). SEER Cancer Statistics Review, 1975–2015. Retrieved from https://seer.cancer.gov/csr/1975_2015/
Rahmani, S., & Talepasand, S. (2015). The effect of group mindfulness-based stress reduction program and conscious yoga on the fatigue severity and global and specific life quality in women with breast cancer. Medical Journal of the Islamic Republic of Iran, 29, 175.
Reich, R. R., Lengacher, C. A., Alinat, C. B., Kip, K. E., Paterson, C., Ramesar, S., Han, H. S., Ismail-Khan, R., Johnson-Mallard, V., Moscoso, M., Budhrani-Shani, P., & Park, J. (2017). Mindfulness-based stress reduction in post-treatment breast cancer patients: Immediate and sustained effects across multiple symptom clusters. Journal of Pain and Symptom Management, 53(1), 85–95. https://doi.org/10.1016/j.jpainsymman.2016.08.005
Reich, R. R., Lengacher, C. A., Kip, K. E., Shivers, S. C., Schell, M. J., Shelton, M. M., & Klein, T. W. (2014). Baseline immune biomarkers as predictors of MBSR(BC) treatment success in off-treatment breast cancer patients. Biological Research for Nursing, 16(4), 429–437. https://doi.org/10.1177/1099800413519494
Schell, L. K., Monsef, I., Wöckel, A., & Skoetz, N. (2019). Mindfulness-based stress reduction for women diagnosed with breast cancer. The Cochrane Database of Systematic Reviews, 3(3), CD011518-CD011518. https://doi.org/10.1002/14651858.CD011518.pub2.
Schellekens, M. P. J., van den Hurk, D. G. M., Prins, J. B., Donders, A. R. T., Molema, J., Dekhuijzen, R., van der Drift, M. A., & Speckens, A. E. M. (2017). Mindfulness-based stress reduction added to care as usual for lung cancer patients and/or their partners: A multicentre randomized controlled trial. Psycho-Oncology, 26(12), 2118–2126. https://doi.org/10.1002/pon.4430
Speca, M., Carlson, L. E., Goodey, E., & Angen, M. (2000). A randomized, wait-list controlled clinical trial: The effect of a mindfulness meditation-based stress reduction program on mood and symptoms of stress in cancer outpatients. Psychosomatic Medicine, 62(5), 613–622. https://doi.org/10.1097/00006842-200009000-00004
Suurmond, R., van Rhee, H., & Hak, T. (2017). Introduction, comparison, and validation of meta-essentials: A free and simple tool for meta-analysis. Research Synthesis Methods, 8(4), 537–553. https://doi.org/10.1002/jrsm.1260
The Nordic Cochrane Centre. (2012). Review Manager (RevMan). (Version 5.3) [Computer program]. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration.
Tiller, J. W. (2013). Depression and anxiety. Medical Journal Australia, 199(S6), S28-31. https://doi.org/10.5694/mja12.10628
Tsaras, K., Papathanasiou, I. V., Mitsi, D., Veneti, A., Kelesi, M., Zyga, S., & Fradelos, E. C. (2018). Assessment of depression and anxiety in breast cancer patients: prevalence and associated Factors. Asian Pacific Journal of Cancer Prevention, 19(6), 1661–1669. https://doi.org/10.22034/apjcp.2018.19.6.1661.
van der Lee, M. L., & Garssen, B. (2012). Mindfulness-based cognitive therapy reduces chronic cancer-related fatigue: A treatment study. Psycho-Oncology, 21(3), 264–272. https://doi.org/10.1002/pon.1890
World Health Organization. (2018). Cancer. Retrieved from https://www.who.int/news-room/fact-sheets/detail/cancer
Würtzen, H., Dalton, S. O., Christensen, J., Andersen, K. K., Elsass, P., Flyger, H. L., & Johansen, C. (2015). Effect of mindfulness-based stress reduction on somatic symptoms, distress, mindfulness and spiritual wellbeing in women with breast cancer: Results of a randomized controlled trial. Acta Oncologica, 54(5), 712–719. https://doi.org/10.3109/0284186X.2014.997371
Wurtzen, H., Dalton, S. O., Elsass, P., Sumbundu, A. D., Steding-Jensen, M., Karlsen, R. V., & Johansen, C. (2013). Mindfulness significantly reduces self-reported levels of anxiety and depression: Results of a randomised controlled trial among 336 Danish women treated for stage I-III breast cancer. European Journal of Cancer, 49(6), 1365–1373. https://doi.org/10.1016/j.ejca.2012.10.030
Zhang, J. Y., Zhou, Y. Q., Feng, Z. W., Fan, Y. N., Zeng, G. C., & Wei, L. (2017). Randomized controlled trial of mindfulness-based stress reduction (MBSR) on posttraumatic growth of Chinese breast cancer survivors. Psychology, Health & Medicine, 22(1), 94–109. https://doi.org/10.1080/13548506.2016.1146405
Zhang, M. F., Wen, Y. S., Liu, W. Y., Peng, L. F., Wu, X. D., & Liu, Q. W. (2015). Effectiveness of mindfulness-based terapy for reducing anxiety and depression in patients with cancer: A meta-analysis. Medicine (baltimore), 94(45), e0897-e1890. https://doi.org/10.1097/md.0000000000000897
Zhang, Q., Zhao, H., & Zheng, Y. (2019). Effectiveness of mindfulness-based stress reduction (MBSR) on symptom variables and health-related quality of life in breast cancer patients—A systematic review and meta-analysis. Supportive Care in Cancer, 27(3), 771–781. https://doi.org/10.1007/s00520-018-4570-x
Acknowledgements
We acknowledge Hsiao-Hsuan Cheng and Ya-Ting Hu for their support in the implementation of this project.
Funding
This work was supported by Kaohsiung Veterans General Hospital 429 (VGHKS107-D03-3).
Author information
Authors and Affiliations
Contributions
The authors confirm contribution to the paper as follows: study conception and design: PCL and PLH; data collection: LYL and LHL; analysis and interpretation of results: GLT, YHH, and JFT; draft manuscript preparation: YLC, CJW, and LYL. All authors reviewed the results and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no known competing financial interests or personal relationships that could influence the work reported in this paper.
Ethical Approval
Not applicable.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Lin, LY., Lin, LH., Tzeng, GL. et al. Effects of Mindfulness-Based Therapy for Cancer Patients: A Systematic Review and Meta-analysis. J Clin Psychol Med Settings 29, 432–445 (2022). https://doi.org/10.1007/s10880-022-09862-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10880-022-09862-z