
Abstract
Evidence suggests cognitive styles are associated with depression; however, little research has examined cognitive styles in early childhood. Using developmentally appropriate, stress-inducing laboratory paradigms to assess young children’s cognitive vulnerability, the current study assessed negative and positive cognitive styles, their concurrent associations with well-established risk factors for depression in early childhood, and their stability from early to middle childhood. Participants included 173 preschool-aged children and their parents. Cognitive styles were assessed by coding children’s negative and positive self-referent and non-self-referent verbalizations and assistance-seeking verbalizations during stress-inducing laboratory tasks during early childhood (Wave 1; ages 3–5) and middle childhood (Wave 2; ages 6–10). Children’s Wave 1 verbalizations were concurrently associated with exposure to maternal depression, child negative and positive temperamental emotionality, and child externalizing psychopathology. Assistance-seeking verbalizations demonstrated homotypic continuity from Wave 1 to Wave 2, and both assistance-seeking verbalizations and negative non-self-referent verbalizations at Wave 1 predicted increases in negative self-referent verbalizations from Wave 1 to Wave 2. Findings suggest that cognitive styles can be observed in young children when using an ecologically valid assessment and are linked to risk factors for depression. Further research is warranted to elucidate the development of cognitive vulnerability in young children, which may inform prevention and early interventions targeting cognitive risk for depression.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Cognition plays a major role in theories of depression etiology and maintenance. Cognitive theories of depression, such as Beck’s (1987) cognitive theory and Teasdale’s (1988) information processing theory, emphasize the role of negative schemas and information processing related to the self, the world, and one’s future in the development and maintenance of depression. Substantial literature has documented links between depression and negative cognitive styles, including biases in attention, memory, appraisal, and self-referential processing, in adulthood, adolescence, and middle childhood (for reviews, see Jacobs et al. 2008; Joormann and Arditte 2015; Lakdawalla et al. 2007; Mathews and MacLeod 2005), yet few studies have examined depressive cognitive styles in early childhood. Prior research has established the presence of depression in children as young as age three, with prevalence rates ranging from 0 to 2% and significant associated impairment in the domains of school, home, and psychosocial functioning (for a review, see Dougherty et al. 2015). Although cognitive symptoms of depression are less common in young children due to their developmental stage (Bufferd et al. 2017), early emerging cognitive styles may identify preschoolers who are at risk for the later development of depression.
Methodological challenges likely contribute to the small body of evidence for cognitive vulnerability to depression in children under 5–6 years of age. Although evidence supports that depressive cognitions are present in young children, they may by undetected with current assessment measures due to their lack of developmental sensitivity (Murray et al. 2001). The assessment of cognitive styles and self-perception in children above age five has largely relied on self-report questionnaires and interviews such as the Children’s Attributional Style Questionnaire (CASQ; Seligman et al. 1984; Thompson et al. 1998), the Children’s Cognitive Style Questionnaires (CCSQ; Abela 1997), the Children’s Attributional Style Interview (CASI; Conley et al. 2001), the Cognitive Triad Inventory for Children (CTI-C; Kaslow et al. 1992), and the Berkeley Puppet Interview (BPI; Ablow and Measelle 1993) (for a review, see Jacobs et al. 2008). However, these self-report measures present notable shortcomings for assessing cognitive styles in younger children, including being beyond young children’s cognitive abilities (e.g., Cole et al. 2008; LaGrange et al. 2008), having low to fair internal consistency (Gladstone and Kaslow 1995), and assessing children’s accounts of how they would respond in hypothetical – rather than actual – situations (Jacobs et al. 2008). Alternative methods may be required to accurately and reliably capture these cognitive styles in young children.
Though more limited than studies incorporating self-report, several studies have used behavioral tasks to assess cognitive styles and biases. Many of these studies have documented greater encoding, attention to, and memory of negative relative to positive events or words in depressed relative to non-depressed children and adolescents (e.g., Auerbach et al. 2015; LeMoult et al. 2017). Prior work has incorporated behavioral tasks such as the Self-Schema Task, the self-referent encoding task (SRET), emotional recall and recognition memory tasks, and attentional dot-probe tasks (for a review, see Jacobs et al. 2008). While these studies leveraged behavioral tasks to assess cognitive processes, avoiding some of the biases associated with self-report, most studies using behavioral tasks in children and adolescents have been limited to children ages seven and older and focused more on attention and memory biases rather than cognitive styles.
The few studies which have used ecologically valid scenarios designed to elicit negative emotions, such as stress-inducing paradigms, have documented depressogenic cognitions and negative cognitive styles in early childhood, consistent with results when using similar paradigms in older children (Hayden et al. 2006, 2013; Taylor and Ingram 1999) and adolescents (Kelvin et al. 1999). For example, Smiley and Dweck (1994) developed a paradigm for 4- and 5-year-old children in which they completed unsolvable puzzles and then were asked to rate their emotions and goal confidence. Children who had performance goals in the tasks but low confidence in their own abilities had the most helplessness, demonstrating the ability to assess cognitions in preschoolers through low mood induction. Using a similar paradigm, Ziegert and colleagues (Ziegert et al. 2001) demonstrated cognitive, affective, and behavioral helplessness in kindergarteners, which predicted helplessness at both 1-year and 5-year follow-up. Murray and colleagues (Murray et al. 2001) also observed the presence of depressive cognitions in five-year-olds by assessing positive and negative verbalizations, facial expressions, and behavioral responses after exposure to a card game in which there was the threat of loss. Taken together, these findings provide support for the validity of depressogenic cognitive styles as early as the late preschool period when using developmentally-appropriate assessment measures and indicate that cognitive vulnerability to depression may begin early in life.
Relatively little is known about negative cognitions in early childhood, their correlates, and whether they have predictive validity in young children. Studying cognitive risk factors for depression in young children may provide targets for early intervention, particularly given increased neuroplasticity during this developmental period (Belsky and de Haan 2011; Luby 2010). The aim of the current study was to identify cognitive patterns which may increase risk for depression in preschool-aged children using ecologically valid behavioral tasks and to validate cognitive patterns as a potential risk factor by examining associations with well-established risk factors for depression, including maternal depression and child temperament and psychiatric symptoms and disorders, and their stability from early to middle childhood.
Prior work in older youth and adults has documented associations between negative cognitive style and well-established risk factors for depression, including parental depression and child temperament. First, negative cognitions assessed using self-report questionnaires in middle childhood, adolescence, and young adulthood have been linked to the presence of parental depression (e.g., Alloy et al. 2004; Garber and Flynn 2001; Garber and Martin 2002; Goodman and Gotlib 2002; Hayden et al. 2013). Parental depression may confer vulnerability to negative cognitive style and depression in children through modeling of negative cognitions (Garber and Flynn 2001), child exposure to greater parental hostility and less warmth (Lovejoy et al. 2000), a depressed parent’s impaired ability to respond to the child’s social and emotional needs (Goodman and Gotlib 1999), and a more stressful home context (Goodman and Gotlib 1999). Only one study examining maternal depression and child cognitions has been conducted in early childhood and found that preschoolers (age 5) exposed to maternal depression demonstrated greater negative cognitions of hopelessness, pessimism, and low self-worth assessed with a stress-inducing paradigm (Murray et al. 2001), which may reflect transmission of risk through the parenting environment in high-risk offspring. Second, child cognitive styles have been linked to temperamental risk for depression, which is characterized by low levels of positive emotionality and high levels of negative emotionality (Clark and Watson 1999; for a review, see Shankman and Klein 2003). For example, lower positive emotionality (PE) at age three predicted greater helplessness at age seven (Hayden et al. 2006), and higher negative emotionality (NE) at age seven predicted greater cognitive vulnerability to depression assessed up to four years later (Hong et al. 2017). Negative cognitive styles have also been found to mediate the association between high NE and greater depressive symptoms in young adults (Lakdawalla and Hankin 2008), as well as moderate associations between negative cognitions and depressive symptoms in adults (Hankin and Abela 2005) and between life stress and cognitive vulnerability to depression in adults and youth (Mezulis et al. 2006; for a review, see Hankin et al. 2009). However, no studies have examined associations between cognitive vulnerability and risk factors for depression in early childhood.
Despite little work examining the stability of depressogenic attributional styles in young children, negative cognitive styles have been observed across various developmental periods and may demonstrate change over the course of development. Using largely self-report measures, previous research has reported moderate stability of negative cognitions and cognitive styles from kindergarten to first grade (r = .41; Ziegert et al. 2001), within middle childhood (rs = .31–.60; Hayden et al. 2013; Hong et al. 2017; LaGrange et al. 2008), from pre-adolescence to mid-adolescence (Carter and Garber 2011) and within adolescence (r = .52; Hankin 2008), as well as moderate to high stability from late adolescence to early adulthood (Spearman’s rho = .62; Romens et al. 2009). Developmental theorists have posited that the relation between negative cognitions and depression becomes stronger over time due to increasing cognitive abilities (Nolen-Hoeksema et al. 1992; Turner and Cole 1994; Weisz et al. 2001). Although there is some fluctuation in negative cognitions over time (Hankin 2008), evidence supports that cognitive vulnerability to depression is likely to stabilize with age (Hankin et al. 2009), particularly during adolescence (Hankin and Abela 2005; LaGrange et al. 2008). Despite this data, no study to our knowledge has assessed the stability of negative cognitions from early to middle childhood, an examination which may delineate trajectories associated with increased risk for the development of depression.
The current study assessed children’s cognitive styles using developmentally-appropriate methods and aimed to validate these cognitive styles in young children by examining associations over time and with other risk factors for depression, namely maternal depression history and child temperament and psychiatric symptoms and disorders. Based on prior research in older youth (e.g., Conley et al. 2001; Goodman and Gotlib 2002; Hayden et al. 2006), we hypothesized that negative cognitive styles would be positively associated with maternal depression, high child NE, and low child PE, in addition to externalizing symptoms given that internalizing and externalizing symptoms often co-occur in young children (e.g., Gilliom and Shaw 2004). Furthermore, we hypothesized that negative cognitions would demonstrate low to moderate stability from early to middle childhood given that previous research suggests cognitive vulnerability to depression stabilizes later in development during adolescence (e.g., Hankin and Abela 2005). As little work has examined positive cognitive styles in young children, we explored their associations with risk factors for depression and stability over time but did not posit specific hypotheses related to positive cognitive styles. Finally, we examined sex differences in cognitive vulnerability. We hypothesized no sex differences given that the greater risk for females relative to males in depression and cognitive vulnerability to depression often does not emerge until adolescence (Hankin 2008; Mezulis et al. 2006; Nolen-Hoeksema 2012).
Method
Participants
The initial sample consisted of 175 preschool-aged children who participated in a study examining children’s neuroendocrine functioning and risk factors for psychopathology (Dougherty et al. 2013). At the initial early childhood assessment (Wave 1 [W1]), children were recruited from the Washington, D.C. metropolitan area through flyers distributed to schools, daycares, and healthcare centers (73.1%) and a commercial mailing list (26.9%) (Dougherty et al. 2013). Children who were between the ages of three and five years, had no significant medical or developmental disabilities, lived with at least one biological parent, and had an English-speaking biological parent with at least 50% legal custody were eligible. Of the initial sample of 175 children, 173 participated in the stress-inducing laboratory tasks to assess children’s cognitive styles at W1 (M = 56.39 months, SD = 10.14 months, range = 39–87 months; 48.6% male). Of those 173 participants, 95 children completed stress-inducing laboratory tasks to assess children’s cognitive styles at Wave 2 (W2) (M = 87.79 months, SD = 11.54 months, range = 66–120 months; 52.6% male) approximately three years later (M = 30.20 months, SD = 6.62 months). Thus, the final sample for concurrent W1 analyses was 173 children, and the final sample for longitudinal associations between W1 and W2 child verbalizations was 95 children. This study was approved by the University’s human subjects review board. Parents provided informed consent at both assessment waves, and child assent was obtained from children seven years of age and older at W2. Characteristics of the sample are presented in Table 1.
We compared participants who completed both assessments at W1 and W2 to those who only completed the W1 assessment on child sex, race, ethnicity, age, parental marital status, parental education, maternal depression history, and child psychiatric symptoms. One significant difference emerged: families who completed both waves were more likely to have a parent with at least a 4-year college degree (75.8%) than families who completed the first wave only (59.7%), χ2 (1, N = 172) = 5.09, p = 0.02.
Measures
Early Childhood Assessment (W1)
Cognitive Styles
We assessed children’s cognitive styles by coding child verbalizations during two stress-inducing laboratory tasks at W1. Descriptive information for children’s cognitive styles at both W1 and W2 are included in Table 2. One child and one experimenter were present during the tasks at W1. During the first task, children attempted to unlock a clear box with an inoperable set of keys in order to retrieve a desirable toy. During the second task, children unsuccessfully attempted to complete three trials of a timed matching game in the presence of an experimenter (Kryski et al. 2011). This task has previously been shown to activate children’s stress responses, increase negative affect, and decrease negative affect (Tolep and Dougherty 2014), supporting its validity as a stress-inducing paradigm.
Children were video-recorded during all laboratory tasks, and all child verbalizations during both tasks were coded and categorized into assistance-seeking statements, positive statements, or negative statements. We examined positive cognitive styles, along with negative cognitive styles, in young children because of the prominent role of positive emotionality and approach behaviors in theoretical models of depression (Clark and Watson 1999; Davidson 1992; Davidson et al. 2002). We also examined self-referent verbalizations separately from non-self-referent verbalizations given evidence that self-relevant content related to depressive thought is more negative than externally-focused content (for a review, see Wisco 2009). Moreover, less work has examined internal versus external attributional style in young children, and it is possible that non-self-referent statements become internalized to reflect more self-referent beliefs over time.
A verbalization was considered a discrete word, phrase, or sentence. Assistance-seeking verbalizations included those in which the child expressed the need for help or requested others to help (e.g., “Can you help me?” or “Can you do it?”). Positive verbalizations included those in which the child expressed confidence, persistence, hopefulness, or trying. Positive verbalizations were then subcategorized as either self-referent positive statements that included positive self-regard (e.g., “I’m good at this” or “Let me try this one”) or non-self-referent positive statements (e.g., “Maybe this piece will fit” or “This key will open it”). Negative verbalizations included those in which the child expressed failure, self-doubt, hopelessness, helplessness, or giving up. Negative verbalizations were also categorized as self-referent negative statements including negative self-regard (e.g., “I can’t do it” or “I’m not good at this”) or non-self-referent negative statements (e.g., “This is too difficult” or “It’s unfair”). For all categories of verbalizations, a proportion was calculated by taking the number of statements in that category divided by the total number of the child’s statements across the entire task. At W1, proportions were averaged across the two laboratory tasks to create a composite proportion score. Coders at W1 were a post-baccalaureate research assistant and an undergraduate research assistant extensively trained in the coding system. Coders watched the video-recorded laboratory tasks and transcribed all child verbalizations to categorize them. To prevent coder drift, coders met weekly to review coding, and the principal investigator (PI) was consulted on all ambiguous verbalizations. To assess interrater reliability, intraclass correlation coefficients (ICCs) were calculated on a subset of episodes from the transparent box task (n = 19) and the matching task (n = 8) and were generally good (average ICC = 0.88; see Table 2).
General Cognitive Ability
To ensure children possessed sufficient receptive language abilities to understand the tasks, we administered the Peabody Picture Vocabulary Test (PPVT; Dunn and Dunn 1997) at W1. During the PPVT, children are shown four pictures simultaneously and are asked to point to the picture that best illustrates the meaning of the stimulus word given by the examiner.
Maternal Depression History
The Structured Clinical Interview for DSM-IV, Non-Patient version (SCID-IV -NP; First et al. 1996) was used to assess maternal psychiatric history, including lifetime history of depression. Diagnostic information was obtained from 166 (96.0%) biological mothers. Interviews were conducted by telephone following the first laboratory visit at W1, which yields similar results as face-to-face interviews (Rohde et al. 1997). Given evidence of high co-occurrence between major depressive disorder (MDD) and dysthymic disorder (DD) in epidemiological studies (Kessler et al. 2005), maternal history of MDD or DD was collapsed into one variable to reflect lifetime maternal depression. At W1, 83 (50.0%) mothers met the diagnostic criteria for a lifetime history of depressive disorder. Using a life event calendar to aid recall (Belli et al. 2001), onset and offset dates were recorded during the SCID for each depressive episode to determine whether the depressive episode occurred during the child’s lifetime. Of the 83 mothers, 53 mothers were depressed during the child’s lifetime (child exposure to maternal depression). Kappa statistics for lifetime depressive disorder was excellent (kappa = 1.00, n = 16).
Observed Child Temperament
Eight standardized episodes from the Laboratory Temperament Assessment Battery (Lab-TAB; Goldsmith et al. 1995) were administered during the child’s first visit to the laboratory at W1 to elicit affect and temperament-relevant behaviors. Episodes are described in the order in which they were conducted: (1) Make That Car Go – experimenter and child raced remote-controlled racecars; (2) Transparent Box – child was given inoperable keys to open a transparent box that contained a desirable toy; (3) Exploring New Objects – child was presented with the opportunity to explore novel stimuli; (4) Pop-Up Snakes – experimenter and child played a practical joke on the parent and asked the parent to open what appeared to be a can of potato chips but actually contained coiled spring snakes; (5) Impossibly Perfect Green Circles – experimenter asked child to draw circles and mildly critiqued each one; (6) Popping Bubbles – experimenter and child played together with a bubble toy, (7) Snack Delay – child was instructed to wait for the experimenter to ring a bell before eating a small snack, and (8) Box Empty – child was given a wrapped empty box to open under the assumption that a prize was inside.
Episodes were videotaped and coded by experienced graduate and undergraduate students trained in the Lab-TAB coding system used previously in an independent sample (Dougherty et al. 2011; Olino et al. 2010). For all episodes, each display of positive and negative facial affect (i.e., positive affect, sadness, anger, fear) was rated on a 3-point scale and weighted based on the intensity of the affect (low, moderate, high). Weighted scores were summed for each episode and then averaged across all eight episodes. We only included child facial affect in order to limit overlap with the vocalization measure described above. In addition, global ratings of child temperament and behaviors, including sociability and interest/engagement, were rated on a 5-point scale for each episode and averaged across the eight total episodes (see Dougherty et al. 2011). We created composite scores of children’s positive emotionality (PE: positive facial affect, sociability, and interest/engagement) and negative emotionality (NE: facial sadness, facial anger, and facial fear). Inter-rater reliability, as indexed by the average ICC (n = 15), was .94 and .80, for child PE and NE, respectively.
Preschool Psychopathology
The Preschool Age Psychiatric Assessment (PAPA; Egger et al. 1999) is a parent-reported structured diagnostic interview used to assess current DSM-IV-TR psychiatric disorders in the prior three months for children ages two to six years. A total of 157 parents (91.1% mothers) completed the PAPA interview at the W1 visit. The following DSM-IV-TR diagnoses were assessed: any depressive disorder (major depressive disorder, dysthymic disorder, or depression-not otherwise specified [NOS]), any anxiety disorder (specific phobia, separation anxiety, social phobia, generalized anxiety disorder, agoraphobia, panic disorder, selective mutism), attention-deficit/hyperactivity disorder (ADHD), and oppositional defiant disorder (ODD). To examine inter-rater reliability, 15 audiotaped interviews were randomly selected and rated by a second interviewer. Interrater reliability for diagnoses ranged from moderate (kappa = 0.64) to excellent (kappa = 1.00). Fifty-one children (32.5%) met criteria at W1 for any internalizing disorder (any depressive or anxiety disorder), and 23 (14.6%) children met criteria for any externalizing disorder (ODD or ADHD).
Primary caregivers (93.0% mothers) also completed the Child Behavior Checklist/1½ -5 (CBCL/1½-5; Achenbach and Rescorla 2001), a 100-item questionnaire that assesses broadband internalizing (M = 8.50, SD = 6.26, range = 0–30) and externalizing (M = 12.05, SD = 7.74, range = 0–39.56) symptoms in children using a 3-point Likert scale ranging from “Never True” to “Very/Often True.” Parents completed the questionnaire using an online format prior to and following their first lab visit. The questionnaire exhibited good internal reliability for both internalizing (α = .84; 36 items) and externalizing (α = .90; n = 24 items) symptoms.
Middle Childhood Assessment (W2)
Cognitive Styles
At W2, children’s cognitive styles were evaluated using similar developmentally appropriate stress-inducing laboratory tasks. These tasks differed from tasks administered at W1 to ensure stressors were novel and age-appropriate to elicit stress in older children. Participants completed a modified version of the Trier Social Stress Task for Children (TSST-C; Buske-Kirschbaum et al. 1997) and an impossible puzzle task. Children were given a picture book with no words and instructed to tell a 4.5-min story in front of the experimenter and a “judge” after a 30 s preparation period. If children paused for more than 15 s or completed their story in under 4.5 min, they were instructed that a longer story was needed and to continue telling their story. Prior work supports the validity of this task as a stress-inducing paradigm by demonstrating increased levels of cortisol, a stress hormone, in children following the task (Kudielka et al. 2004). Following the story-telling task, children were presented with an impossible puzzle to complete and were told that it was an easy puzzle for young children. The puzzle was impossible because it contained pieces from two highly similar but different puzzles. During both tasks, the judge pretended to take notes on the child’s performance to elicit feelings of social evaluation. After the puzzle task, the judge exited the room to decide which prize the child would win while the child was allowed to color. Four and half minutes into the coloring period, the experimenter also left the room for 30 s to deliberate with the judge about which prize the child would win. Upon re-entry, the experimenter told participants they performed well on the tasks and presented them with their favorite prize.
Similar to W1, child verbalizations were coded and categorized into assistance-seeking statements, positive statements, or negative statements; positive and negative statements were further categorized as either self-referent or non-self-referent statements. Proportion scores were calculated similar to W1, with statements in each category divided by the total number of verbalizations. Coders at W2 were a post-baccalaureate research assistant and three undergraduate research assistants extensively trained in the coding system. To prevent coder drift, the coding team met weekly for supervision by the post-baccalaureate research assistant, and the study PI was consulted for categorizing ambiguous verbalizations. ICC scores of interrater reliability ranged from good to excellent (n = 15; average ICC = 0.94; see Table 2).
Data Analysis Plan
First, we examined associations between child verbalizations and potential covariates, including child age and sex, parental education and marital status, and child PPVT scores. Next, to investigate the validity of child verbalizations as a measure of children’s cognitive style, we examined bivariate correlations between preschoolers’ verbalizations and well-established risk factors for depression, including maternal depression history, observed child temperament, and parent-reported child internalizing and externalizing symptoms and disorders. Significant bivariate associations between child verbalizations and risk factors for depression were then examined in regression models controlling for significant covariates. Lastly, to investigate the stability of children’s cognitive styles over time, we examined bivariate correlations for both homotypic continuity (one type of verbalization predicting that same type of verbalization at follow-up) and heterotypic continuity (one type of verbalization predicting another type of verbalization at follow-up).
Results
We observed concurrent associations between W1 child verbalizations and demographic variables. At W1, child age was positively associated with W1 positive non-self-referent verbalizations (r = .24, p = .001), and males demonstrated more negative self-referent verbalizations than females, t(139.24) = 2.22, p = .03. Child PPVT scores were positively associated with W1 positive self-referent verbalizations (r = .17, p = .03) and W1 positive non-self-referent verbalizations (r = .18, p = .02). We next ran regression analyses controlling for these variables in their respective models. Specifically, child sex was included as a covariate in models examining negative self-referent verbalizations; child PPVT score was included as a covariate in models examining positive self-referent verbalizations; and both child age at W1 and child PPVT score were included as covariates in models examining positive non-self-referent verbalizations.
Concurrent Associations between Child Verbalizations and Maternal Depression History during Early Childhood (W1)
Concurrent bivariate associations between W1 verbalizations and maternal depression history are reported in Table 3. Maternal lifetime history of depression was not significantly associated with any child verbalizations at W1. However, children who were exposed to maternal depression demonstrated a lower proportion of positive self-referent verbalizations at W1 (M = −.20, SD = .60) than children who were not exposed to maternal depression (M = .08, SD = .83), t(136.40) = 2.40, p = .02. In addition, children exposed to maternal depression demonstrated a greater proportion of assistance-seeking verbalizations (M = .19, SD = .79) than children who had not been exposed to maternal depression (M = −. 07, SD = .78), t(164) = −2.04, p = .04). After controlling for child sex, the association between exposure to maternal depression and children’s positive self-referent verbalizations became non-significant (p = .07).
Concurrent Associations between Child Verbalizations and Child Temperament during Early Childhood (W1)
We observed significant concurrent associations between child verbalizations and observed child temperament at W1 (Table 3). Child PE at W1 was significantly positively associated with concurrent positive self-referent verbalizations and positive non-self-referent verbalizations. PE was also significantly negatively associated with concurrent W1 assistance-seeking verbalizations but was not concurrently associated with any negative self-referent or non-self-referent verbalizations at W1. In contrast, child NE at W1 was significantly negatively associated with concurrent positive self-referent verbalizations at W1 but was not concurrently associated with any other verbalizations at W1. All concurrent associations between child verbalizations and child temperament remained significant when analyzed using regression models that included relevant demographic covariates (ps < .04).
Concurrent Associations between Child Verbalizations and Preschool Psychopathology (W1)
We observed significant associations between children’s verbalizations at W1 and children’s psychiatric symptoms and diagnoses at W1 (Table 3). We found a significant concurrent negative association between CBCL externalizing symptoms at W1 and children’s W1 positive self-referent verbalizations but no other associations between CBCL externalizing symptoms at W1 and child verbalizations at W1. CBCL internalizing symptoms at W1 were not concurrently associated with any verbalizations at W1. A diagnosis of a W1 PAPA internalizing disorder was not significantly associated with any verbalizations at W1, whereas a diagnosis of a W1 PAPA externalizing disorder was concurrently associated with a greater proportion of negative self-referent verbalizations and a greater proportion of negative non-self-referent verbalizations. Of note, all concurrent associations between child verbalizations and child psychiatric symptoms and disorders remained significant when analyzed using regression models that included relevant demographic covariates (ps < .05).
Longitudinal Associations between Wave 1 and Wave 2 Child Verbalizations
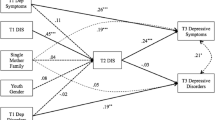
We examined longitudinal associations among child verbalizations (Table 4). First, we investigated homotypic associations. Assistance-seeking verbalizations at W1 and W2 were significantly positively associated, such that children who were more inclined to ask for help at W1 continued to be more inclined to ask for help at W2. No other homotypic associations were significant. With respect to heterotypic continuity in preschoolers’ verbalizations, assistance-seeking verbalizations at W1 were significantly positively associated with negative self-referent verbalizations at W2 and this association remained significant when controlling for children’s negative self-referent verbalizations at W1 (b = .06, SE = .01, p < .001). In addition, the proportion of negative non-self-referent verbalizations at W1 predicted the proportion of negative self-referent verbalizations at W2, and this association remained significant when controlling for children’s negative self-referent verbalizations at W1 (b = .05, SE = .01, p < .001). Thus, assistance-seeking and negative non-self-referent verbalizations at W1 both predicted increases in negative self-referent verbalizations from W1 to W2. No other heterotypic associations were observed.
Discussion
The current study examined negative and positive verbalizations and their relations to well-established risk factors for depression, including maternal depression, child temperament, and child internalizing and externalizing disorders and symptoms, in a sample of preschool-aged children. Overall, our study findings provide support for the use of developmentally appropriate, stress-inducing paradigms to assess cognitive styles in young children and suggest that cognitive risk for the development of depression may be present as early as the preschool years and persist over time. These findings underscore the importance of assessing cognitive styles in early childhood, which can be used to inform early intervention and prevention efforts and reduce the risk of depression and associated negative sequelae.
Assessment of Cognitive Style in Preschool-Aged Children
We found that both self-referent and non-self-referent negative and positive verbalizations can be observed in young children when developmentally appropriate stress-inducing paradigms are used. This finding supports our hypothesis and is consistent with existing literature (e.g., Murray et al. 2001) that posits that negative cognitions can be observed in young children using ecologically valid scenarios designed to elicit negative emotions. Our study expands the limited literature on negative cognitions in young children, which has typically featured neutral tasks. Neutral tasks may not induce the low mood needed to accurately assess latent negative cognitions (e.g., Persons and Miranda 1992). The stress tasks used in this study were also designed to imitate actual situations children may face in their daily lives, allowing us to measure responses to these ecologically valid situations rather than responses to hypothetical situations. Further, the use of developmentally-appropriate paradigms to examine these verbalizations addresses a methodological limitation that may contribute to why many prior studies have failed to find cognitive vulnerability to depression in children under six years of age. Thus, by utilizing these experimental manipulations, cognitive vulnerability to depression in young children can be further explored.
Associations between Preschoolers’ Verbalizations and Risk for Depression
Consistent with our hypothesis, we found that children who were exposed to maternal depression during their lifetime demonstrated fewer positive self-referent verbalizations in early childhood; however, we did not find support for associations between child exposure to maternal depression and children’s negative verbalizations in early childhood, which is inconsistent with prior literature (e.g., Garber and Flynn 2001; Murray et al. 2001). These inconsistencies may be attributable to developmental differences, such as using a sample of young children rather than adolescents (Garber and Flynn 2001), or methodological differences, such as type of stressor used (Murray et al. 2001). It is possible that negative cognitions may be more present in early adolescence and potential mediating factors during early childhood should thus be examined further. Nonetheless, the association between exposure to maternal depression and fewer positive self-referent verbalizations may be attributable to the early parenting environment given established associations between maternal depression and negative parenting behaviors, including increased hostility and criticism, greater disengagement, and less warmth and support (Lovejoy et al. 2000). Furthermore, children who experience maternal disengagement and fewer positive interactions with their mothers may incorporate this lack of validation and positive interactions into their schemas and therefore feel less positively about themselves. Overall, we may have found associations for positive verbalizations and not negative verbalizations in early childhood given evidence that negative cognitions strengthen with age (Hankin et al. 2009). Thus, children exposed to maternal depression may be more likely to demonstrate these negative cognitions as they age or, possibly, after longer exposure to maternal depression. The link between maternal depression exposure and child positive self-referent verbalizations became non-significant when controlling for children’s general language ability assessed with the PPVT. Children exposed to maternal depression also had lower PPVT scores; thus, children exposed to maternal depression may have a general language deficit that involves positive cognitive styles. More research investigating the language deficits of offspring exposed to depression and the possible role they play in cognitive risk is warranted.
We also found that exposure to maternal depression was associated with increased assistance-seeking verbalizations in early childhood. Abramson et al. (1978) revised theory of learned helplessness posits that children who view negative events as internal, stable, and global are vulnerable to learned helplessness. Increased assistance-seeking verbalizations may therefore suggest a lack of agency. This finding supports previous work by Nolen-Hoeksema and colleagues (Nolen-Hoeksema et al. 1995) documenting less persistence and enthusiasm and more frustration on puzzle tasks for offspring of depressed mothers. Moreover, Donovan et al. (1990) found that mothers who were more depressed and demonstrated higher depressogenic attributional styles were more likely to display helplessness themselves, as indicated by a greater number of failures and inattentiveness during a learning task involving how to respond to an infant’s cries. This helpless disposition in mothers could therefore contribute to modeling of negative cognitions for their children. In addition, previous research has shown that modeling of negative cognitions in depressed mothers is linked to negative cognitions in adolescent offspring (Garber and Flynn 2001). Therefore, children who have been exposed to maternal depression during their lifetime may model this learned helplessness, as evidenced by increased assistance-seeking verbalizations. The associations between maternal depression and child verbalizations were significant for exposure to maternal depression, rather than lifetime depression, suggesting that child exposure to maternal depression may confer greater risk for child depression through its effects on parenting and modeling.
We found that child observed temperamental PE was associated with greater positive self-referent and positive non-self-referent verbalizations in addition to fewer assistance-seeking verbalizations in early childhood. Given that children with high PE are generally characterized as more social, engaged, and having more positive mood (Depue and Collins 1999; Lucas et al. 2000; Watson and Clark 1997), it is not surprising that they exhibit more positive verbalizations during stressful tasks. These results may suggest that children with high PE demonstrate more resiliency to stress, while a less positive cognitive style may render children more vulnerable to the effects of stress. Further, this pattern of results is consistent with Hayden and colleagues’ (Hayden et al. 2006) findings that lower PE at age three predicted greater helplessness at age seven while higher PE at age three predicted more positive schematic processing at age seven. Young children who demonstrate more PE might thus be less susceptible to learned helplessness because they maintain a more positive mood during stressful tasks despite experiencing failure. Moreover, children with high PE may be more likely to have a sense of agency when solving problems and feel less discouraged after failure. High PE may be related to greater perceptions of self-competence and therefore reflect a protective factor against depression, particularly given that lower self-perceived competence in children has been linked to depression both concurrently (Measelle et al. 1998) and prospectively (Cole et al. 1996, 1997; Tram and Cole 2000; for a review, see Jacobs et al. 2008). However, contrary to our hypothesis and inconsistent with the literature (e.g., Hayden et al. 2006), we found that child PE was not associated with any negative verbalizations. Notably, however, Hayden and colleagues (Hayden et al. 2006) used self-reports to measure attributional style in older youth and thus methodological or developmental differences may account for this inconsistency. Our findings suggest that child PE may be a protective factor due to children’s resiliency to stress and positive mood. Overall, increased child PE may therefore indicate less susceptibility to learned helplessness and decreased vulnerability to depression in children.
We also found that child observed temperamental NE was associated with fewer positive self-referent verbalizations, indicating that children who demonstrate more NE may feel less positively about themselves. Further, since cognitive theories of depression posit that depression involves negative views of oneself (e.g., Abramson et al. 1978, 1989; Beck 1987), our results support higher NE as a potential risk factor for cognitive vulnerability to depression as evidenced by its association with fewer positive self-referent cognitions in early childhood. Overall, we may have observed associations with positive and not negative verbalizations for both child NE and PE because negative cognitions strengthen with age (Hankin et al. 2009), and therefore might not be present until later developmental periods, such as middle childhood and adolescence, when children develop a differentiated understanding of the self (Abela and Hankin 2008).
Finally, we also found that externalizing symptoms and disorders, but not internalizing symptoms and disorders, were associated with negative and positive self-referent verbalizations and negative non-self-referent verbalizations in early childhood. Interestingly, we found that increased parent-reported CBCL externalizing symptoms were associated with more positive self-referent verbalizations. Children who displayed externalizing symptoms appeared to feel more positively about themselves and their performance throughout the tasks. However, these positive verbalizations may actually be due to the fact that some children with externalizing symptoms may overestimate their actual competence (e.g., Owens et al. 2007) and possess less insight into their behavior (e.g., Hoza et al. 2005). On the one hand, this overestimation of confidence could possibly act as a protective factor against cognitive vulnerability to depression. However, on the other hand, exposure to repeated failure because of overestimation of competence could lead to negative outcomes such as decreased self-esteem over time. Therefore, associations between overestimation of competence in children with externalizing symptoms and cognitive vulnerability to depression over time warrants further investigation.
We also found that a PAPA externalizing disorder diagnosis was concurrently associated with greater negative self-referent and non-self-referent verbalizations. Previous research has documented a relatively high level of comorbidity between depression and externalizing psychopathology, including in young children with depression (e.g., Luby et al. 2003), which may suggest that similar negative cognitions underlie associations between early externalizing disorders and later depression. Therefore, negative views of the self associated with externalizing disorders in early childhood may confer later risk for depression. Of note, sex differences in the prevalence of externalizing disorders are frequently observed in early childhood (e.g., Egger and Angold 2006; Lavigne et al. 1996; Wichstrøm et al. 2012), which may explain why the link between the presence of a PAPA externalizing disorder and child negative self-referent verbalizations became statistically non-significant when controlling for child sex.
Homotypic and Heterotypic Continuity of Preschoolers’ Verbalizations
Contrary to our hypothesis, we found that neither negative verbalizations nor positive verbalizations demonstrated homotypic continuity from early to middle childhood, but we did observe stability in assistance-seeking verbalizations over time. Little research has examined the stability of verbalizations in young children. However, researchers have found that negative cognitive styles stabilize with age (Hankin et al. 2009) and may stabilize more in adolescence (Hankin and Abela 2005). It is possible that these verbalizations may not be stable in young children and this may be due to a variety of reasons, including changes in cognitive development over time (Cole and Turner 1993; Turner and Cole 1994; Weisz et al. 2001) or moderating factors such as changes in perceived self-efficacy due to both school entry and increased socialization from early to middle childhood (e.g., Bandura 1997). Moreover, estimates of stability in older youth and adults have assessed cognitions using various self-report measures (e.g., CASQ-R, CDAS, CCSQ, DAS; Carter and Garber 2011; Hankin 2008; Hayden et al. 2013; Hong et al. 2017; Romens et al. 2009) which may produce higher stability estimates than our measure of cognitive style. Nevertheless, we did find that assistance-seeking verbalizations demonstrated low to moderate stability from early to middle childhood. It is possible that children who demonstrate helplessness in early childhood might continue to demonstrate helplessness in middle childhood due to persistent fear of failure, contributing to lack of agency over time. Further research is needed to examine both the stability of verbalizations over time and potential moderating factors of verbalizations in young children across development. Such research could help to elucidate the development of cognitive vulnerability as a risk factor for depression in young children and subsequently inform intervention programs during this important developmental period.
Although we did not observe homotypic continuity in negative or positive verbalizations from early childhood to middle childhood, we did observe heterotypic continuity between early childhood and middle childhood verbalizations. First, we found that children who demonstrated greater negative non-self-referent verbalizations during early childhood demonstrated greater negative self-referent verbalizations in middle childhood, reflecting negative feelings about themselves and their performance even when controlling for negative self-referent verbalizations in early childhood. Cognitive theories of depression such as Abramson et al.’s (1978, 1989) hopelessness theory and Beck’s (1987) model of depression both posit that negative cognitive styles of depression involve negative views of oneself. Notably, this shift of negative verbalizations from an external locus in early childhood to an internal locus in middle childhood may suggest the development of a cognitive vulnerability to depression over time. Second, we found that children who demonstrated greater assistance-seeking verbalizations during early childhood demonstrated greater negative-self-referent verbalizations in middle childhood, even when controlling for negative self-referent verbalizations in early childhood. Research has documented that young children (ages 4–5) are sensitive to criticism, and that individual differences exist in the way that children respond to failure (Heyman et al. 1992; Kamins and Dweck 1999). Children who show a “mastery-oriented” response pattern attribute failure to external factors such as lack of effort or difficulty of the task rather than to their own abilities, whereas children who show a “helpless” pattern demonstrate more negative self-cognitions and give up easily. Thus, early assistance-seeking verbalizations may suggest feelings of helplessness, which could contribute to negative interpretations of the self and vulnerability to depression over time.
Study Strengths, Limitations, and Future Directions
The present study had a number of strengths. First, unlike many previous studies examining depressogenic cognitions in young children, we used experimental manipulations consisting of ecologically valid and developmentally appropriate scenarios designed to elicit negative emotions. Second, to our knowledge, this study is the first to examine both verbalizations related and unrelated to the self in a preschool-aged sample. Further, we found specific associations among self-referent and non-self-referent verbalizations and risk factors for depression that would not have been evident if we did not make this distinction. Therefore, this methodology may be useful for more clearly identifying those at risk for depression and delineating when cognitive vulnerability to depression arises in development. Third, we used a longitudinal design that allowed us to examine stability and change in verbalizations from early childhood to middle childhood. Fourth, maternal depression history and exposure were assessed at early childhood using a validated clinical interview. Fifth, child temperament was measured using an observational laboratory measure to reduce informant bias. Lastly, we examined verbalizations to assess cognitive risk factors for depression in early childhood, which is a developmental period before the typical onset age for the disorder (e.g., Twenge and Nolen-Hoeksema 2002; Kessler et al. 2001). Thus, studying cognitive risk factors for depression in young children could inform future early interventions for children at risk for depression.
The current study also had limitations. First, associations between verbalizations at early childhood and risk factors for depression such as maternal depression, child temperament, and child symptomatology were cross-sectional, and thus causation cannot be determined. Second, temperament was only assessed in a laboratory setting. Nevertheless, similar observational methods have been shown to predict behavior in other settings and over time (Durbin et al. 2007). Third, we did not correct for multiple testing, which may have increased Type I error. However, these analyses were exploratory and intended to inform future hypotheses. Fourth, we determined children’s psychopathology and symptomology using information from only one informant, primarily mothers. A multi-informant approach, including co-parents and teachers, should be used in future studies to increase the validity of these reports.
Fifth, we used two different stressor paradigms and while using identical stressor paradigms would more easily facilitate examination of change over time, novel paradigms were essential to induce stress sufficiently at follow-up, avoiding habitation effects from the initial stressor paradigm. Sixth, the stressor paradigms may not have been sufficiently stress-inducing for all children, although there are ethical concerns in using more potent stress-inducing lab tasks in young children. Nevertheless, prior studies support that mildly stress-inducing paradigms are sufficiently potent to induce children’s physiological and emotional responses (e.g., Gunnar et al. 2009; Kryski et al. 2011; Tolep and Dougherty 2014; Van Goozen et al. 2000). Lastly, families who participated at follow-up were more likely to have a parent with at least a 4-year college degree than families who participated at baseline only; this sampling difference may have impacted the results in unknown ways. Nevertheless, when we controlled for parental education in all analyses, results remained the same.
In sum, our findings demonstrate that negative and positive verbalizations both related and unrelated to the self can be elicited in young children using developmentally appropriate stress-inducing paradigms and that these verbalizations are associated with risk factors for depression, including child exposure to maternal depression, child observed temperament, and child externalizing symptoms and disorders. Our work expands the current literature regarding cognitive vulnerability to depression as little work has assessed negative and positive verbalizations in young children using developmentally sensitive measures. Future studies should continue to examine the validity and clinical utility of early emerging cognitive styles in young children. Early childhood may be an ideal period to intervene with young children at risk for depression given the greater behavioral and neural plasticity during this developmental period (Luby 2010). Importantly, findings could inform the development of intervention programs targeting cognitive vulnerability to depression, even in this young age group.
References
Abela, J. R. Z. (1997). The children’s cognitive style questionnaire. McGill University: Unpublished questionnaire.
Abela, J. R, & Hankin, B. L. (2008). Cognitive vulnerability to depression in children and adolescents. In: J.R. Abela & B. L. Hankin (Eds), Handbook of depression in children and adolescents (pp. 35–78). New York: The Guilford Press.
Ablow, J. C., & Measelle, J. R. (1993). Berkeley puppet interview: Administration and scoring system manuals. Berkeley: University of California.
Abramson, L. Y., Seligman, M. E., & Teasdale, J. D. (1978). Learned helplessness in humans: Critique and reformulation. Journal of Abnormal Psychology, 87(1), 49–74.
Abramson, L. Y., Metalsky, G. I., & Alloy, L. B. (1989). Hopelessness depression: A theory- based subtype of depression. Psychological Review, 96(2), 358–372.
Achenbach, T. M., & Rescorla, L. A. (2001). Manual for the ASEBA Preschool Form & Profiles. Burlington: University of Vermont, Research Center for Children, Youth, & Families.
Alloy, L. B., Abramson, L. Y., Gibb, B. E., Crossfield, A. G., Pieracci, A. M., Spasojevic, J., & Steinberg, J. A. (2004). Developmental antecedents of cognitive vulnerability to depression: Review of findings from the cognitive vulnerability to depression project. Journal of Cognitive Psychotherapy, 18(2), 115–134.
Auerbach, R. P., Stewart, J. G., Stanton, C. H., Mueller, E. M., & Pizzagalli, D. A. (2015). Emotion-processing biases and resting EEG activity in depressed adolescents. Depression and Anxiety, 32(9), 693–701.
Bandura, A. (1997). Self-efficacy: The exercise of control. New York, NY, US: W H Freeman/Times Books/ Henry Holt & Co..
Beck, A. T. (1987). Cognitive models of depression. Journal of Cognitive Psychotherapy, 1(1), 5-37.
Belli, R. F., Shay, W. L., & Stafford, F. P. (2001). Event history calendars and question list surveys: A direct comparison of interviewing methods. Public Opinion Quarterly, 65(1), 45–74.
Belsky, J., & de Haan, M. (2011). Annual research review: Parenting and children’s brain development: The end of the beginning. Journal of Child Psychology and Psychiatry, 52(4), 409–428.
Bufferd, S. J., Dougherty, L. R., & Olino, T. M. (2017). Mapping the frequency and severity of depressive behaviors in preschool-aged children. Child Psychiatry & Human Development, 48(6), 934–943.
Buske-Kirschbaum, A., Jobst, S., Wustmans, A., Kirschbaum, C., Rauh, W., & Hellhammer, D. (1997). Attenuated free cortisol response to psychosocial stress in children with atopic dermatitis. Psychosomatic Medicine, 59(4), 419–426.
Carter, J. S., & Garber, J. (2011). Predictors of the first onset of a major depressive episode and changes in depressive symptoms across adolescence: Stress and negative cognitions. Journal of Abnormal Psychology, 120(4), 779–796.
Clark, L. A., & Watson, D. (1999). Temperament: A new paradigm for trait psychology. In L. A. Pervin & O. P. John (Eds.), Handbook of personality: Theory and research (2nd ed.). New York: Guilford Press.
Cole, D. A., & Turner, J. J. (1993). Models of cognitive mediation and moderation in child depression. Journal of Abnormal Psychology, 102(2), 271–281.
Cole, D. A., Martin, J. M., Powers, B., & Truglio, R. (1996). Modeling causal relations between academic and social competence and depression: A multitrait-multimethod longitudinal study of children. Journal of Abnormal Psychology, 105(2), 258–270.
Cole, D. A., Martin, J. M., & Powers, B. (1997). A competency-based model of child depression: A longitudinal study of peer, parent, teacher, and self-evaluations. Journal of Child Psychology and Psychiatry, 38(5), 505–514.
Cole, D. A., Ciesla, J. A., Dallaire, D. H., Jacquez, F. M., Pineda, A. Q., LaGrange, B., et al. (2008). Emergence of attributional style and its relation to depressive symptoms. Journal of Abnormal Psychology, 117(1), 16–31.
Conley, C. S., Haines, B. A., Hilt, L. M., & Metalsky, G. I. (2001). The Children's attributional style interview: Developmental tests of cognitive diathesis-stress theories of depression. Journal of Abnormal Child Psychology, 29(5), 445–463.
Davidson, R. J. (1992). Prolegomenon to the structure of emotion: Gleanings from neuropsychology. Cognition and Emotion, 6, 245–268.
Davidson, R. J., Lewis, D. A., Alloy, L. B., Amaral, D. G., Bush, G., Cohen, J. D., et al. (2002). Neural and behavioral substrates of mood and mood regulation. Biological Psychiatry, 52, 478–502.
Depue, R. A., & Collins, P. F. (1999). Neurobiology of the structure of personality: Dopamine, facilitation of incentive motivation, and extraversion. Behavioral and Brain Sciences, 22(3), 49–569.
Donovan, W. L., Leavitt, L. A., & Walsh, R. O. (1990). Maternal self-efficacy: Illusory control and its effect on susceptibility to learned helplessness. Child Development, 61(5), 1638–1647.
Dougherty, L. R., Bufferd, S. J., Carlson, G. A., Dyson, M., Olino, T. M., Durbin, C. E., & Klein, D. N. (2011). Preschoolers’ observed temperament and psychiatric disorders assessed with a parent diagnostic interview. Journal of Clinical Child and Adolescent Psychology, 40(2), 295–306.
Dougherty, L. R., Tolep, M. R., Smith, V. C., & Rose, S. (2013). Early exposure to parental depression and parenting: Associations with young offspring's stress physiology and oppositional behavior. Journal of Abnormal Child Psychology, 41(8), 1299–1310.
Dougherty, L. R., Leppert, K. A., Merwin, S. M., Smith, V. C., Bufferd, S. J., & Kushner, M. R. (2015). Advances and directions in preschool mental health research. Child Development Perspectives, 9(1), 14–19.
Dunn, L. M., & Dunn, L. M. (1997). Peabody picture vocabulary test (3rd ed.). Circle Pines: American Guidance Service.
Durbin, E. C., Hayden, E. P., Klein, D. N., & Olino, T. M. (2007). Stability of laboratory-assessed temperamental emotionality traits from ages 3 to 7. Emotion, 7, 388–399.
Egger, H. L., & Angold, A. (2006). Common emotional and behavioral disorders in preschool children: Presentation, nosology, and epidemiology. Journal of Child Psychology and Psychiatry, 47(3/4), 313–337.
Egger, H. L., Ascher, B. H., & Angold, A. (1999). The preschool age psychiatric assessment (PAPA). Durham: Center for Developmental Epidemiology, Department of Psychiatry and Behavioral Sciences, Duke University Medical Center.
First, M. B., Spitzer, R. L., Gibbon, M., & Williams, J. B. W. (1996). Structured Clinical Interview for DSM-IV Axis I Disorders: Non-patient edition (version 2.0). New York, NY: New York State Psychiatric Institute Biometrics Research.
Garber, J., & Flynn, C. (2001). Predictors of depressive cognitions in young adolescents. Cognitive Therapy and Research, 25(4), 353–376.
Garber, J., & Martin, N. C. (2002). Negative cognitions in offspring of depressed parents: Mechanisms of risk. In S. H. Goodman & I. H. Gotlib (Eds.), Children of depressed parents: Mechanisms of risk and implications for treatment (pp. 121–153). Washington, DC: American Psychological Association.
Gilliom, M., & Shaw, D. S. (2004). Codevelopment of externalizing and internalizing problems in early childhood. Development and Psychopathology, 16(2), 313–333.
Gladstone, T. G., & Kaslow, N. J. (1995). Depression and attributions in children and adolescents: A meta-analytic review. Journal of Abnormal Child Psychology, 23(5), 597–606.
Goldsmith, H. H., Reilly, J., Lemery, K. S., Longley, S., & Prescott, A. (1995). The laboratory temperament assessment battery: Preschool version. Unpublished manuscript.
Goodman, S. H., & Gotlib, I. H. (2002). Children of depressed parents: Mechanisms of risk and implications for treatment. Washington, DC: American Psychological Association.
Goodman, S. H., & Gotlib, I. H. (1999). Risk for psychopathology in the children of depressed mothers: A developmental model for understanding mechanisms of transmission. Psychological Review, 106(3), 458–490.
Gunnar, M. R., Talge, N. M., & Herrera, A. (2009). Stressor paradigms in developmental studies: What does and does not work to produce mean increases in salivary cortisol. Psychoneuroendocrinology, 34(7), 953–967.
Hankin, B. L. (2008). Stability of cognitive vulnerabilities to depression: A short-term prospective multiwave study. Journal of Abnormal Psychology, 117(2), 324–333.
Hankin, B., & Abela, J. (2005). Depression from childhood through adolescence and adulthood: A developmental vulnerability and stress perspective. In B. L. Hankin & J. R. Abela (Eds.), Development of psychopathology: A vulnerability-stress perspective (pp. 245–288). Thousand Oaks: SAGE Publications Ltd..
Hankin, B. L., Oppenheimer, C., Jenness, J., Barrocas, A., Shapero, B. G., & Goldband, J. (2009). Developmental origins of cognitive vulnerabilities to depression: Review of processes contributing to stability and change across time. Journal of Clinical Psychology, 65(12), 1327–1338.
Hayden, E. P., Klein, D. N., Durbin, C. E., & Olino, T. M. (2006). Positive emotionality at age 3 predicts cognitive styles in 7-year-old children. Development and Psychopathology, 18(2), 409–423.
Hayden, E. P., Olino, T. M., Mackrell, S. V., Jordan, P. L., Desjardins, J., & Katsiroumbas, P. (2013). Cognitive vulnerability to depression during middle childhood: Stability and associations with maternal affective styles and parental depression. Personality and Individual Differences, 55(8), 892–897.
Heyman, G. D., Dweck, C. S., & Cain, K. M. (1992). Young children's vulnerability to self-blame and helplessness: Relationship to beliefs about goodness. Child Development, 63(2), 401–415.
Hong, R. Y., Lee, S. S., Tsai, F. F., & Tan, S. H. (2017). Developmental trajectories and origins of a core cognitive vulnerability to internalizing symptoms in middle childhood. Clinical Psychological Science, 5(2), 299–315.
Hoza, B., Mrug, S., Gerdes, A. C., Hinshaw, S. P., Bukowski, W. M., Gold, J. A., et al. (2005). What aspects of peer relationships are impaired in children with attention-deficit/hyperactivity disorder? Journal of Consulting and Clinical Psychology, 73(3), 411–423.
Jacobs, R. H., Reinecke, M. A., Gollan, J. K., & Kane, P. (2008). Empirical evidence of cognitive vulnerability for depression among children and adolescents: A cognitive science and developmental perspective. Clinical Psychology Review, 28(5), 759–782.
Joormann, J., & Arditte, K. A. (2015). Cognitive aspects of depression. In I. H. Gotlib & C. Hammen (Eds.), Handbook of depression (pp. 298–321). New York: Guilford.
Kamins, M. L., & Dweck, C. S. (1999). Person versus process praise and criticism: Implications for contingent self-worth and coping. Developmental Psychology, 35(3), 835–847.
Kaslow, N. J., Stark, K. D., Printz, B., Livingston, R., & Ling Tsai, S. (1992). Cognitive triad inventory for children: Development and relation to depression and anxiety. Journal of Clinical Child Psychology, 21(4), 339–347.
Kelvin, R. G., Goodyer, I. M., Teasdale, J. D., & Brechin, D. (1999). Latent negative self-schema and high emotionality in well adolescents at risk for psychopathology. Journal of Child Psychology and Psychiatry, 40(6), 959–968.
Kessler, R. C., Avenevoli, S., & Merikangas, K. R. (2001). Mood disorders in children and adolescents: An epidemiologic perspective. Biological Psychiatry, 49(12), 1002–1014.
Kessler, R. C., Chiu, W. T., Demler, O., & Walters, E. E. (2005). Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62(6), 617–627.
Kryski, K. R., Smith, H. J., Sheikh, H. I., Singh, S. M., & Hayden, E. P. (2011). Assessing stress reactivity indexed via salivary cortisol in preschool-aged children. Psychoneuroendocrinology, 36, 1127–1136.
Kudielka, B. M., Buske-Kirschbaum, A., Hellhammer, D. H., & Kirschbaum, C. (2004). HPA axis responses to laboratory psychosocial stress in healthy elderly adults, younger adults, and children: Impact of age and gender. Psychoneuroendocrinology, 29(1), 83–98.
LaGrange, B., Cole, D. A., Dallaire, D. H., Ciesla, J. A., Pineda, A. Q., Truss, A. E., & Folmer, A. (2008). Developmental changes in depressive cognitions: A longitudinal evaluation of the cognitive triad inventory for children. Psychological Assessment, 20(3), 217–226.
Lakdawalla, Z., & Hankin, B. L. (2008). Personality as a prospective vulnerability to dysphoric symptoms among college students: Proposed mechanisms. Journal of Psychopathology and Behavioral Assessment, 30(2), 121–131.
Lakdawalla, Z., Hankin, B. L., & Mermelstein, R. (2007). Cognitive theories of depression in children and adolescents: A conceptual and quantitative review. Clinical Child and Family Psychology Review, 10(1), 1–24.
Lavigne, J. V., Gibbons, R. D., Christoffel, K. K., Arend, R., Rosenbaum, D., Binns, H., et al. (1996). Prevalence rates and correlates of psychiatric disorders among preschool children. Journal of the American Academy of Child & Adolescent Psychiatry, 35(2), 204–214.
LeMoult, J., Kircanski, K., Prasad, G., & Gotlib, I. H. (2017). Negative self-referential processing predicts the recurrence of major depressive episodes. Clinical Psychological Science, 5(1), 174–181.
Lovejoy, M. C., Graczyk, P. A., O'Hare, E., & Neuman, G. (2000). Maternal depression and parenting behavior: A meta-analytic review. Clinical Psychology Review, 20(5), 561–592.
Luby, J. L. (2010). Preschool depression: The importance of identification of depression early in development. Current Directions in Psychological Science, 19(2), 91–95.
Luby, J. L., Heffelfinger, A. K., Mrakotsky, C., Brown, K. M., Hessler, M. J., Wallis, J. M., & Spitznagel, E. L. (2003). The clinical picture of depression in preschool children. Journal of the American Academy of Child & Adolescent Psychiatry, 42(3), 340–348.
Lucas, R. E., Diener, E., Grob, A., Suh, E. M., & Shao, L. (2000). Cross-cultural evidence for the fundamental features of extraversion. Journal of Personality and Social Psychology, 79(3), 452–468.
Mathews, A., & MacLeod, C. (2005). Cognitive vulnerability to emotional disorders. Annual Review of Clinical Psychology, 1, 167–195.
Measelle, J. R., Ablow, J. C., Cowan, P. A., & Cowan, C. P. (1998). Assessing young children's views of their academic, social, and emotional lives: An evaluation of the self-perception scales of the Berkeley puppet interview. Child Development, 69(6), 1556–1576.
Mezulis, A. H., Hyde, J. S., & Abramson, L. Y. (2006). The developmental origins of cognitive vulnerability to depression: Temperament, parenting, and negative life events in childhood as contributors to negative cognitive style. Developmental Psychology, 42(6), 1012–1025.
Murray, L., Woolgar, M., Cooper, P., & Hipwell, A. (2001). Cognitive vulnerability to depression in 5-year-old children of depressed mothers. Journal of Child Psychology and Psychiatry, 42(7), 891–899.
Nolen-Hoeksema, S. (2012). Emotion regulation and psychopathology: The role of gender. Annual Review of Clinical Psychology, 8, 161–187.
Nolen-Hoeksema, S., Girgus, J. S., & Seligman, M. E. (1992). Predictors and consequences of childhood depressive symptoms: A 5-year longitudinal study. Journal of Abnormal Psychology, 101(3), 405–422.
Nolen-Hoeksema, S., Wolfson, A., Mumme, D., & Guskin, K. (1995). Helplessness in children of depressed and nondepressed mothers. Developmental Psychology, 31(3), 377–387.
Olino, T. M., Klein, D. N., Dyson, M. W., Rose, S. A., & Durbin, C. E. (2010). Temperamental emotionality in preschool-aged children and depressive disorders in parents: Associations in a large community sample. Journal of Abnormal Psychology, 119(3), 468–478.
Owens, J. S., Goldfine, M. E., Evangelista, N. M., Hoza, B., & Kaiser, N. M. (2007). A critical review of self-perceptions and the positive illusory bias in children with ADHD. Clinical Child and Family Psychology Review, 10(4), 335–351.
Persons, J. B., & Miranda, J. (1992). Cognitive theories of vulnerability to depression: Reconciling negative evidence. Cognitive Therapy and Research, 16(4), 485–502.
Rohde, P., Lewinsohn, P. M., & Seeley, J. R. (1997). Comparability of telephone and face-to-face interviews in assessing axis I and II disorders. American Journal of Psychiatry, 154(11), 1593–1598.
Romens, S. E., Abramson, L. Y., & Alloy, L. B. (2009). High and low cognitive risk for depression: Stability from late adolescence to early adulthood. Cognitive Therapy and Research, 33(5), 480–498.
Seligman, M. E. P., Peterson, C., Kaslow, N. J., Tanenbaun, R. L., Alloy, L. B., & Abramson, L. Y. (1984). Explanatory style and depressive symptoms among school children. Journal of Abnormal Psychology, 93, 235–238.
Shankman, S. A., & Klein, D. N. (2003). The relation between depression and anxiety: An evaluation of the tripartite, approach-withdrawal and valence-arousal models. Clinical Psychology Review, 23(4), 605–637.
Smiley, P. A., & Dweck, C. S. (1994). Individual differences in achievement goals among young children. Child Development, 65(6), 1723–1743.
Taylor, L., & Ingram, R. E. (1999). Cognitive reactivity and depressotypic information processing in children of depressed mothers. Journal of Abnormal Psychology, 108(2), 202–210.
Teasdale, J. D. (1988). Cognitive vulnerability to persistent depression. Cognition and Emotion, 2(3), 247–274.
Thompson, M., Kaslow, N. J., Weiss, B., & Nolen-Hoeksema, S. (1998). Children's attributional style questionnaire—Revised: Psychometric examination. Psychological Assessment, 10(2), 166–170.
Tolep, M. R., & Dougherty, L. R. (2014). The conundrum of the laboratory: Challenges of assessing preschool-age children’s salivary cortisol reactivity. Journal of Psychopathology and Behavioral Assessment, 36(3), 350–357.
Tram, J. M., & Cole, D. A. (2000). Self-perceived competence and the relation between life events and depressive symptoms in adolescence: Mediator or moderator? Journal of Abnormal Psychology, 109(4), 753–760.
Turner, J. E., & Cole, D. A. (1994). Development differences in cognitive diatheses for child depression. Journal of Abnormal Child Psychology, 22(1), 15–32.
Twenge, J. M., & Nolen-Hoeksema, S. (2002). Age, gender, race, socioeconomic status, and birth cohort difference on the children's depression inventory: A meta-analysis. Journal of Abnormal Psychology, 111(4), 578–588.
Van Goozen, S. H., Matthys, W., Cohen-Kettenis, P. T., Buitelaar, J. K., & Van Engeland, H. (2000). Hypothalamic-pituitary-adrenal axis and autonomic nervous system activity in disruptive children and matched controls. Journal of the American Academy of Child & Adolescent Psychiatry, 39(11), 1438–1445.
Watson, D., & Clark, L. A. (1997). Extraversion and its positive emotional core. In R. Hogan, J. A. Johnson, S. R. Briggs, R. Hogan, J. A. Johnson, & S. R. Briggs (Eds.), Handbook of personality psychology (pp. 767–793). San Diego, CA, US: Academic Press.
Weisz, J. R., Southam-Gerow, M. A., & McCarty, C. A. (2001). Control-related beliefs and depressive symptoms in clinic-referred children and adolescents: Developmental differences and model specificity. Journal of Abnormal Psychology, 110(1), 97–109.
Wichstrøm, L., Berg-Nielsen, T. S., Angold, A., Egger, H. L., Solheim, E., & Sveen, T. H. (2012). Prevalence of psychiatric disorders in preschoolers. Journal of Child Psychology and Psychiatry, 53(6), 695–705.
Wisco, B. E. (2009). Depressive cognition: Self-reference and depth of processing. Clinical Psychology Review, 29(4), 382–392.
Ziegert, D. I., Kistner, J. A., Castro, R., & Robertson, B. (2001). Longitudinal study of young children's responses to challenging achievement situations. Child Development, 72(2), 609–624.
Funding
This research was funded by the University of Maryland (UMD) College of Behavioral and Social Sciences Dean’s Research Initiative Award (LRD) and the UMD Research and Scholars Award (LRD).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Katherine A. Leppert, Mary-Charlotte Wasserbach and Lea R. Dougherty declare that they have no conflict of interest.
Experiment Participants
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Leppert, K.A., Wasserbach, MC. & Dougherty, L.R. Cognitive Styles in Preschool-Age Children: Associations with Depression Risk and Evidence of Stability. J Psychopathol Behav Assess 41, 612–626 (2019). https://doi.org/10.1007/s10862-019-09726-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10862-019-09726-1