
Abstract
Taking coparenting into consideration is essential when assessing children and their relational environment, regardless of the family structure. This paper presents three studies we conducted with the aim of developing and validating a reliable instrument for the assessment of coparenting in Spanish. The first study consisted of developing the items to be included in the assessment tool and evaluation of this content by a panel of nine experts. In the second study, we explored both the psychometric properties and the factorial structure of the prototype instrument using a sample of 251 participants. The third study confirmed the factorial structure and tested measurement invariance, the reliability, and convergent and discriminant evidence of our tool in a general population sample of 312 participants. We obtained a 15-item unidimensional questionnaire, the Questionnaire for the Assessment of Coparenting (CECOP), with very good psychometric properties: excellent internal consistency with α of 0.97 and supported validity with the selected conceptually related metrics; convergent validity with the Instrument for the Assessment of Adaptation to Divorce–Separation’s (CADS) coparenting dimension and Questionnaire on Perceived Support from the Former Partner (CARE); and divergent validity with parenting and dyadic adjustment. Furthermore, the results in terms of measurement invariance across family structures and sex allowed us to assume the configural invariance between the groups. However, it was not possible to assume metric invariance. Finally, we also provide normative scores for its interpretation. The CECOP shows excellent psychometric properties and can be considered the first questionnaire in Spanish that assesses coparenting in any family structure, which also includes the triadic conceptualization of coparenting, providing valuable information on the relational environment in which children and adolescence live.
Highlights
-
The CECOP is the first instrument in Spanish that assesses coparenting across different family structures.
-
The CECOP is a valid and reliable unidimensional Spanish-language self-report instrument to assess coparenting.
-
This clinical assessment of coparenting, aimed at parents that have a child in common, is able to examine how they work together as parents while providing information regarding the relational environment in which children live.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Coparenting has emerged as a crucial element within family relationships across different family structures. It was initially conceptualized as occurring when parents were separated, but it has evolved and has become established as a crucial aspect of interfamilial relations regardless of family structure (Pruett et al., 2021; Walsh, 2016). Coparenting constitutes the part of the parent–parent/parental subsystem that reflects collaboration in childrearing aimed at the welfare of the child (Feinberg, 2003; Margolin et al., 2001). Consequently, it revolves around the triadic parent–parent –child system (Feinberg, 2003) and is a mediating mechanism between the marital relationship of the parents and the corresponding parent–child relationships (Bonds & Gondoli, 2007; Margolin et al., 2001). It is also a crucial aspect of children’s psychological adjustment (Baril et al., 2007) and of how children adjust psychologically to their position in the world and their role within the family (Teubert & Pinquart, 2010). Coparenting is dynamic and evolves along with the family structure, particularly it undergoes great changes when parents separate or reunite. Even though these changes might be particularly challenging, coparenting is fundamental in any family configuration, including among sets of parents who were never a couple, heterosexual families and situations of foster parenthood (Leal et al., 2022).
Coparenting was initially conceptualized as a multi-domain construct, with the following four interrelated and overlapping domains: support/undermining, joint family management, childrearing agreement, and division of labor (Feinberg, 2003). Childrearing agreement refers to the degree to which coparents agree on different child-related topics, while the division of labor is related to the division of responsibilities for daily childcare and household tasks. The binary support-undermining refers to the extent to which each parent supports the other, while the domain of joint family management refers to the executive subsystem between both parents (Feinberg, 2003). It is also worth mentioning Margolin’s model (Margolin et al., 2001), which conceptualizes coparenting based on three dimensions: conflict, cooperation and triangulation. In Teubert and Pinquart (2010)’s meta-analysis the authors propose a comprehensive assessment of coparenting based largely on Margolin’s and Feinberg’s model, finding that the main aspects of coparenting were cooperation, childrearing agreement, conflict, and triangulation, but this researchers places special emphasis on the interrelated, overlapping nature of these domains. Further studies of the interaction between these dimensions have identified two high-orders dimensions (conflict and support), along with several lower-order dimensions, including coparenting alliance, childrearing agreement, triangulation, division of labor, support and undermining between coparents, and joint family management of interactions (Mollà-Cusí et al., 2020; Saini et al., 2019). In light of all of this research, the quality of coparenting has been defined in terms of supportive (or cooperative) versus undermining (or competitive) (Feinberg, 2003; Saini et al., 2019), with these two overarching dimensions encompassing the other subdimensions described above.
Supportive coparenting refers to attitudes and actions that affirm, acknowledge and respect the other parent’s competency and authority as a parent (Feinberg, 2003). In contrast, competitive coparenting refers to undermining of the other parent through criticism, disparagement, and blame (Belsky et al., 1996; Feinberg, 2003; McHale, 1995). It has not yet been established whether there are two independent dimensions of coparenting or whether it is a single factor with two opposite extremes (competitive vs. cooperative) (Mollà-Cusí et al., 2020).
Numerous factors may predict psychopathology in children. Coparenting has been clearly established as a predictor of child adjustment, as it independently predicts children’s internalizing and externalizing problem behavior (Feinberg et al., 2012; Teubert & Pinquart, 2010; Zemp et al., 2018). This additional variance has been established in longitudinal studies as being different from both parenting (Belsky et al., 1996; Caldera & Lindsey, 2006; Karreman et al., 2008) and marital quality (Johnson et al., 1999; Kolak & Vernon-Feagans, 2008). Specifically, undermining coparenting has been established as a risk factor for externalizing behaviors, mostly, but also for some internalizing problems (Davies & Lindsay, 2001; Feldman et al., 2010; Solmeyer et al., 2014; Umemura et al., 2015; Murphy et al., 2016), while cooperative coparenting has been found to be a protective factor (McHale et al., 1999, 2000; Schoppe-Sullivan et al., 2001). Coparenting is thus known to affect child adjustment in two different ways: directly, by compromising the family’s stability; and indirectly, by impacting the individual parenting of each parent, that is, the dyadic relationship between each parent and their children (Davies & Cummings, 1994; Erel & Burman, 1995; Margolin et al., 2001). Consequently, establishing the quality of coparenting is essential in clinical practice when assessing a child who presents with externalizing or internalizing problems.
As seen in a recent review (Mollà Cusí et al., 2020), the instruments that are currently available to assess coparenting are limited to a few specific languages, were only developed for specific family structures (intact vs. separated families), and do not systematically include the assessment of other relevant aspects of family relationships, such as individual parenting. The CoPAFS (Saini et al., 2019) is the first instrument to assess coparenting across family structures, but it has been published as a pilot study and needs empirical validation studies. In Spanish, two instruments are available that include assessment of some aspects of the inter-parent relationship: the Instrument for the Assessment of Adaptation to Divorce–Separation (CAD-S; Yárnoz-Yaben & Comino, 2010) and the Questionnaire on Perceived Support from the Former Partner (CARE; Yárnoz-Yaben, 2010). The CAD-S aims to assess adaptation to divorce or separation, while the CARE focuses on the perception of the support that a divorced parent receives from their ex-partner for caring for their children. However, neither aims to evaluate coparenting itself, as described in the literature, nor does either consider a range of family types. Therefore, there is no instrument in Spanish which allows coparenting to be assessed in any given family structure, taking into consideration the triadic aspect from a systemic point of view, with regard to its impact on the mental health of the children and adolescents. That is, the dyadic conceptualization of coparenting refers to the relationship between the two coparents, while the triadic aspect includes a third person (Flaskas, 2012; Ugazio et al., 2020).
The present paper aims to fill this gap by both developing and validating a questionnaire suitable for use in Spanish as a means to evaluate coparenting in any family structure. The research we report was performed according to established criteria for developing and reviewing instrumental studies (Carretero-Dios & Pérez, 2005; Muñiz & Fonseca-Pedrero, 2019).
Study 1. Developing the Instrument: Developing the initial item pool
Study 1 aims to evaluate the item’ s content by testing whether aspects described in the literature, such as cooperation, conflict, or triangulation, were included.
Method
Participants
We engaged the services of nine experts, following the criteria of a minimum of three experts (Carretero-Dios & Pérez, 2005). The resulting panel was made up of people with a doctoral degree in psychology (PhD), clinical psychology (PsyD) or psychiatry (MD). In order to have a highly representative sample of professionals, we selected experts with different theoretical orientations (psychoanalysis, systemics, CBT, and humanistic psychology), fields of work (private and public practice, child–adolescent and adult patients), professional careers (academics or clinical practitioners), and years of clinical experience (ranging from 14 to 35).
Instruments
The panel of experts was given, both sent online and handed out on paper, a form with a grid. It contained sociodemographic questions, including some devised ad hoc on clinical expertise, as well as the proposed instrument items. They were asked to rate the comprehensibility and representativeness/adequacy of the proposed questions on a 3-point scale. There was also a column in which they could make comments on each item as well as space at the end of the form for comments or suggestions.
Procedure
We drew up the initial items in Spanish after reviewing the existing literature, using both comprehensive reviews on how coparenting should be defined and measured (Van Egeren & Hawkins, 2004), and reviews of existing questionnaires (Mollà Cusí et al., 2020). We focused on those with greater empirical value. That is, they had reported and published its psychometric properties and met the standards according to The Standards for Educational and Psychological Testing (American Educational Research Association, American Psychological Association & National Council on Measurement in Education, 2014).
After gathering all the experts’ opinions via the form described above, we proceeded to eliminate the items that were not pertinent and reword the unclear or badly written ones. Statistical analysis was performed to assess the degree of expert agreement. We applied the consensus criterion proposed by Hagen et al. (2008), defined a priori as >50% of respondents agreeing with a statement. Here, consensus was calculated as the percentage of experts who agreed that the item was representative or clear (those who marked it “clear” but not those who marked it “neither clear nor unclear” nor those who marked it as “unclear”), and consensus was then calculated for both variables (representativeness and clarity). At the same time, qualitative analysis was performed on the basis of the comments and suggestions made by the panel.
Once the final items were selected, we made sure that all the dimensions referred in the literature on coparenting were sufficiently represented.
Data analysis
The Delphi method was applied to analyse the item’s content of questionnaires in a multiple setting (Andrés et al., 2009). The Delphi method is a systematic anonymous process of gathering experts’ opinion on a given subject. It has been widely used in healthcare sciences to obtain consensus where previous research is limited or conflicted, such as diagnosis or to analyse the content validity of questionnaires (Andrés, 2009; Nasa et al., 2021). Thereby, expert consensus was determined by considering the percentage agreement.
Results
We initially developed 33 items, which were presented to the panel of experts. Fourteen of these items were accepted without changes because there was 100% agreement that they were clear and pertinent. Two items with less than 90% agreement (even though the common standard is 50%; Carretero-Dios & Pérez, 2005) were reformulated following the comments from the experts. One item that was determined to be clear by the panel was discarded because the research team considered it to be inadequate when we revised it. The remaining 16 items were discarded because there was no agreement of above 80%, even with the reformulations.
After this, the research team checked that there were enough items representing all the facets of coparenting described in the literature the meta-analysis of Teubert & Pinquart (2010), based on Margolin’s (2001) and Feinberg’s (2003) models, namely: (1) cooperation, (2) agreement on the care and upbringing of children, (3) conflict between parents, and (4) triangulation.
At the end of the first phase, we had a total of 16 items measuring the quality of coparenting that could be administered to an initial general population sample for statistical analysis.
Study 2. Item Analysis and Exploratory Factor Analysis
In order to assess the psychometric properties and explore the factorial structure of the CECOP, the 16 items selected were put to a general population sample.
Method
Participants
Participants were recruited at primary and secondary schools with the following two inclusion criteria: (a) Spanish families, (b) with at least one child in common. The only exclusion criterion was that the children could not be parents. We made that decision in order to exclude participants whose main role in the family was not being a parent or coparent and to be certain of measuring coparenting, also following past research (Saini et al., 2019).
Our sample consisted of 251 parents (both parents of some children responded, while in other cases only one did so, because it was not required that both parents participate), of whom 150 were cohabitating parents (59.8%) and 101 were separated parents (40.2%).
Table 1 presents the sociodemographic information of the sample and Table 2 the ages ranges of the children.
Instruments
The questionnaire was comprised of a sociodemographic section, including questions about coparenting and the relationship between the parents, such as possible separation/divorce, as well as the age of the children, and the 16 items selected in Study 1 to measure the quality of the coparenting. All items were rated on a 5-point frequency scale, ranging from 1 (Never) to 5 (Always).
Procedure
The study and their informed consent and data protection, was approved by the Ethics Committee and the Research Committee of Sant Joan de Déu Hospital (number PIC-95-17) and Ramon Llull University (case file CER URL 2017_2018_007).
Parents were recruited by directly suggesting that they participate, using an intentional non-probabilistic sampling method and in accordance with the inclusion criteria defined. We contacted primary and secondary schools in order to approach parents from the general population. An email from the school was sent with an invitation to participate containing a link to the online questionnaire and a presentation of the study. Before accessing the content on the online questionnaire, participants had to agree to participate in the study via the informed consent when accessing the link. The decision to participate was private and anonymous. Participants were allowed to answer on paper or online, according to their preference. The material was exactly the same, with only the format in which it was presented changing.
Data analysis
First, we carried out item analysis of the 16 CECOP items. The results showed that item 2 (“Colaboramos en el mantenimiento económico de nuestro/s hijo/s” [“We collaborate in the economic maintenance of our children”]) had a high mean and high indices of asymmetry and kurtosis. Therefore, according to psychometric standards (Ferrando et al., 2022), item 2 was excluded from the following analyses, because it displays non-discriminant characteristics. Second, exploratory factor analysis (EFA) was performed using a principal axis factoring (PAF) method via Mplus_8.3 software, in order to study the factorial structure of the CECOP. PAF allows gaining a parsimonious representation of observed correlations between variables and latent factors, operating under the theory of the common factor model (De Winter & Dodou, 2012). Furthermore, PAF is based on the reflective model, following the same logic of confirmatory factor analysis (CFA; see Study 3). We applied parallel analysis to assess the number of factors to be extracted (Hayton et al., 2004). Parallel analysis suggests that only factors which have eigenvalues higher than parallel eigenvalues should be extracted (Turner, 1998). After the number of factors was selected, the factor loading matrix was explored to ascertain the items in each latent factor. According to Tabachnick & Fidell (2007), an item represents a pure measure of the factor when its factor loading is >0.32, and items with lower factor loadings should be deleted.
Results
Table 3 presents the descriptive statistics of the 16 items in the CECOP (N = 251). These results indicated that item 2 should be deleted. The other 15 CECOP items presented moderate skewness and kurtosis. Specifically, skewness ranged from −1.55 to −0.6 and kurtosis ranged from −0.45 to 1.97. Therefore, we performed EFA on 15 items.
First, the results of the parallel analysis showed that just one factor, denominating coparenting, should be extracted. In fact, only factor 1 showed an eigenvalue higher than parallel eigenvalues. Factor 1 explained 74% of the total variance. Furthermore, fit indices were acceptable: SRMR was 0.025 and RMSEA was 0.078. Even though there are two items that have lower factor loadings, the study results support a unidimensional structure, given that factorial loadings are >0.60, fit indices of CFA and internal consistency coefficient are excellent, and that the content of these items doesn’t seem to measure different features of coparenting, according to literature criteria (Tabachnick & Fidell, 2007), which consider an item representative of a factor when it’s >0.32. Finally, the results of EFA also showed a good one-factor solution, with standardized factor loading varying from 0.60 to 0.92. See Fig. 1.

Scree-plot with parallel analyses on 15 items of CECOP
Study 3. Confirmatory Factor Analysis, Reliability and Convergent Evidence
Study 3 aimed to confirm the factor analysis and assess measurement invariance, the reliability and convergent evidence of the CECOP.
Method
Participants
A different sample from the one used in study one, this one made up of a total of 312 parents with at least one child in common (160 cohabiting and 152 separated), participated in study 3. Regarding the age range of the first son/daughter, 17.9% had less than 5 years old, 24.7% between 6 and 10 years old, 26.9% between 11–15 years old, 21.5% between 16 and 20 years old, 6.1% between 21 and 25 years old, 2.2% between 26 and 30 years old, and 0.6% more than 30 years old. Regarding the age range of the second son/daughter, 24.1% had less than 5 years old, 22.1% between 6 and 10 years old, 35.2% between 11–15 years old, 13.1% between 16 and 20 years old, 4.5% between 21 and 25 years old, and 1% between 26 and 30years old. Regarding the age range of the third son/daughter, 20.9% had less than 5 years old, 46.5% between 6 and 10 years old, 23.3% between 11–15 years old, and 9.3% between 16 and 20 years old. Table 4 presents the sociodemographic information of this sample.
This sample exceeds the classical conservative recommendation, as there are more than 20 cases per item, and the minimum is considered to be 5 to 10 cases per item (Worthington & Whittaker, 2006).
Instruments
The questionnaire was comprised of the sociodemographic section described in Study 2 and the remaining 15 items designed to assess coparenting. CECOP is presented in Table 5. Furthermore, for the convergent evidence analysis, we used the Parental Bonding Instrument (PBI; Parker et al., 1979), The Questionnaire for the Assessment of Basic Family Relationships (BFRI: CERFB in Spanish; Ibáñez Martínez et al., 2012), the Instrument for the Assessment of Adaptation to Divorce–Separation (Cuestionario de Adaptación al Divorcio-Separación; CAD-S), and the Questionnaire of the Perceived Support from the Former Partner (Cuestionario de Apoyo Percibido de la Expareja; CARE; Yárnoz-Yaben, 2010).
The Parental Bonding Instrument (PBI; Parker et al., 1979) is a 25-item self-administered questionnaire that assesses two parenting dimensions: care (12 items) and overprotection or control (13 items). It is rated on a 4-point Likert scale ranging from nothing to a lot. The scores on each scale describe a parenting style: optimal bonding (high care–low overprotection), absent or weak bonding (low care–low overprotection), affectionate constraint (high care–high overprotection), and affectionless control (low care–high overprotection). The Spanish adaptation (Ballús Creus, 1991) has good psychometric properties: a split-half reliability of 0.88 and 0.74, test–retest reliability of 0.76 and 0.63, and convergent evidence of 0.77 and 0.47 respectively for the care and overprotection scales. We gave this questionnaire to the total sample.
The Questionnaire for the Assessment of Basic Family Relationships (BFRI: CERFB in Spanish; Ibáñez Martínez et al. 2012) is a 25-item self-reported tool that assesses both the conjugal relationship and the individual parenting relationships in non-separated families. It is rated on a 5-point Likert scale. The parenting dimension has 11 items and scores range between 0 and 55, where higher scores indicate greater functionality. It represents the way in which the parental couple treat their children. The conjugal factor refers to how the people who exercise the parental role (generally, the parental couple) interact with each other. It includes 14 items and is assessed as a dichotomous dimension: harmonious and disharmonious conjugality. Both scales have shown a high degree of reliability, with α (Cronbach’s alpha) being 0.91 for the parenting scale and 0.92 for the conjugal scale, which will be used for the discriminant evidence. The conjugal relationship subscale was only applied to cohabiting parents, while the individual parenting relationship subscale was applied to the total sample.
The CAD-S (Yárnoz-Yaben & Comino, 2010) is a 20-item Spanish questionnaire that assesses adaptation to divorce of the parent who fills it out. Items are rated on a 5-point Likert scale. It includes four factors: psychological and emotional difficulties, conflict with the ex-partner, willingness to coparent, and negative consequences of the divorce for the children. It has acceptable reliability, measured as an α of 0.77 for the overall scale and a range from 0.65 to 0.81 for the subscales. The CAD-S was only given to separated parents.
The CARE (Yárnoz-Yaben, 2010) is an 8-item questionnaire that assesses divorced parents’ perceptions of the support they receive from their ex-partner for raising their children. It was created in Spanish and not validated in other languages. The items are rated on a 5. -point Likert scale. It has acceptable internal consistency, with an α of 0.79, and convergent and discriminant evidence, measured using the CAD-S. EFA shows a one-factor structure which explains 41.8% of the total variance. It adequately measures the level of collaboration between the ex-partners in child-rearing after divorce. The CARE was only given to separated parents.
Procedure
Parents were recruited using the same inclusion criteria, method, and research protocol as approved and described in the section describing the Procedure of Study 2.
Data analysis
The confirmatory factor analysis (CFA) was performed with Mplus_8.3 software using structural equation modeling (SEM; Worthington & Whittaker, 2006) in order to test the goodness of the one-factor model. The hypothesized model was tested using the maximum likelihood (ML) estimation. Goodness-of-fit was assessed with the root mean square error of approximation (RMSEA < 0.80), the standardized root mean square residual (SRMR < 0.80), the comparative fit index, and the Tucker-Lewis index (TLI) (CFI and TLI ≥ 0.95; Hooper et al., 2008). However, CFI and TLI values between 0.90 and 0.95 should be considered acceptable (Chirumbolo et al., 2017).
Furthermore, two measurement invariance analyses across family structures (cohabiting vs. separated) and across gender (women and men) were carried out in order to test whether the factorial structure was equivalent across groups. In line with the recommendations in the literature (Cheung et al., 2002), we first tested configural invariance model, in order to assess fit indices, and subsequently we compared to metric invariance model, via delta chi square Δχ². If the delta chi-square value is statistically significant, it indicates that metric invariance model provides a significantly worse than configural invariance model, i.e. metric invariance is not supported (Cheung et al., 2002).
We analysed convergent evidence and reliability, as well as assessing the normativity of the data, using IBM_SPSS_24.
Results
Confirmatory factor analysis, measurement invariance, convergent evidence analysis and reliability
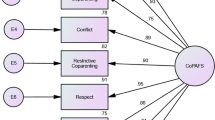
The coparenting model for CFA consists of 15 items and a single latent factor. Most of the fit indices were acceptable: CFI was0.949, NNFI was 0.941 and SRMR was 0.025. However, RMSEA was 0.099; slightly higher than the cut-off criteria. Therefore, our CFA model may be considered globally adequate, supporting the one-factor model previously suggested in Study 2 from our EFA. The standardized factor loadings were very high, ranging from 0.58 to 0.95 (see Fig. 2).

CFA model and factor loadings
In order to examine measurement invariance across family structures and across gender, first we assessed the configural invariance models (M0 for family structures and gender), in which all parameters were free to vary across group. M0 for family structures reached acceptable fit indices: CFI was 0.929, NNFI was 0.921, SRMR was 0.042 and RMSEA was 0.106. Also, M0 for gender reached acceptable fit indices: CFI was 0.917, NNFI was 0.909, SRMR was 0.044 and RMSEA was 0.117. Therefore, our results supported the presence of configural invariance, suggesting that the factorial configuration are the same for cohabiting and separated coparents as well as for women and men. Subsequently, we assessed the metric invariance models (M1 for family structures and gender), in which factor loadings were equivalent for different groups. M1 yielded lower fit indices: CFI was 0.918, NNFI was 0.906, SRMR was 0.105 and RMSEA was 0.112 for family structures and CFI was 0.916, NNFI was 0.907, SRMR was 0.083 and RMSEA was 0.124 for gender. Furthermore, the comparison between M1 and M0 showed a significant Δχ² both for family structures and for gender. Specifically, Δχ²(14) was significant: 63.05 for family structures and 50.05 for gender. Therefore, our results did not support metric invariance. Although this supports a unique factor, coparenting, by gender and family structure, items load differently for different groups.
Our convergent evidence results, as presented in Table 6, show the model has excellent external relationship considering the data. In fact, the CECOP was positively correlated to the conjugal factor of the CERFB for cohabiting parents, and to the coparenting factor of the CAD-S and CARE scales for separated parents. Furthermore, the CECOP was positively correlated to the care subscale of the PBI over the total sample; while it was negatively correlated to conflict and consequences of the CAD-S (for separated parents) and to the overprotection subscale of the PBI (over the total sample).
Our analysis of the internal consistency in the general population showed excellent internal consistency among the CECOP items (α = 0.97).
Normative table
Finally, the normative scores for the CECOP in the general Spanish population were obtained, as reported in Table 7.
Discussion
Coparenting has been established as a crucial element within family relationships and their effects on child development (Cowan & Cowan, 2000; Feinberg, 2003; McHale, 2007; Pruett et al., 2017; Pruett et al., 2021). However, until now there has been no suitably validated instrument to assess coparenting in Spanish.
The goal of this study was therefore to create a valid and reliable metric to assess coparenting in Spanish. A 15-item questionnaire was developed starting from a detailed literature review and following psychometric analysis. Our results show excellent internal consistency and confirm a one-factor structure.
One strength of this study is the extensive and thorough process we used to create and refine the items (Ferrando et al., 2022). Starting from a wide range of items (33 items), with broad consensus from a panel of experts (minimum 80%) and a detailed and exhaustive psychometric analysis of the items, we selected the best items with both excellent psychometric properties and excellent item’s content. Thus, the 15 items chosen are psychometrically excellent and constitute the questionnaire that we subsequently validated. Furthermore, we provided evidence of configural invariance across family structures and gender, although metric invariance is not supported. In other words, our results suggested that the 15 items in the test are adequate to measure Coparenting, but each item differently loads for different groups (cohabiting vs. separated; men and women).
Even though the CECOP was developed using all the aspects of a multi-faceted model, its factorial structure has resulted in a unifactorial model. This is not entirely against the theoretical conceptualizations of coparenting, as the dimensions described in the literature have been grouped into two high order factors, cooperation and conflict, which contain within them other lower-order dimensions (Saini et al. 2019). Indeed, these dimensions have been found to be interrelated and overlapping. Previous studies (Mollà-Cusí et al., 2020) reported that it has yet to be determined whether a single dimension ranging from support on one extreme to conflict on the other could represent coparenting better than other models or equally well, and our study supports this possibility. The two dimensions of the model (cooperation vs. conflict) will need to be further investigated, as this brings new possibilities to the current literature.
Furthermore, the CECOP scores correlate strongly (as expected) with other coparenting metrics (the CADS coparenting dimension and the total CARE score). At the same time, they are distinct from other basic measures of family relationships such as individual parenting (both dimensions of the PBI, the parenting dimension of the CERFB, and the individual dimensions of the CADS, such as individual psychological difficulties), which supports good convergent and discriminant evidence. Therefore, the CECOP contributes to comprehensive clinical assessment by providing an independent assessment of family relationships; specifically, of how parents work together as a team towards raising a child.
Normative data calculated with an extensive sample provide cut-off points in the general population that allow for interpretation of the scores generated by our new instrument. This will allow clinicians to identify which parents can benefit from interventions aimed at improving coparenting.
Our results show that the CECOP provides a valid and reliable assessment of coparenting and therefore it is a meaningful metric in the clinical field when working with parents that have a child in common, as it reflects how they work together as parents. Even though the CARE questionnaire is available in Spanish, it differs from CECOP in that CARE only measures the dyadic concept of coparenting, considering the support perceived from the ex-partner, and it is only aimed at divorced parents. In contrast, the CECOP is not limited by type of family structure and it includes the triadic aspect of coparenting (Feinberg, 2003), thereby providing more information regarding the relational environment in which children live.
Finally, our results should be interpreted taking into account several limitations of the study. Firstly, there is a significant difference in the number of men and women in our sample, with women accounting for around 75% of the sample. This was expected, as most studies of coparenting have similar sample statistics: up to 82% women (Saini et al., 2019; Yárnoz-Yaben & Comino, 2010). However, more studies with a higher proportion of men should be carried out in order to confirm and generalize these results. Additionally, even though recent reports establish that coparenting does not vary as a function of socio-economic status (SES; Schoppe-Sullivan et al., 2021), we did not assess SES implications and cannot replicate these findings. Secondly, even though using a community sample is necessary as a first step when validating a questionnaire, it does not allow extraneous variables to be controlled, which should be included in future studies. The normative table also needs to be interpreted with caution, as the sample of the study was non-probabilistic. Furthermore, the studies involved only heterosexual participants; future studies should consider including other types of parents’ sexual orientations. Regarding its psychometric properties, future studies examining test-retest reliability would be of interest, as well as studies of how this unifactorial instrument fits with the two dimensionalities of the current model. Another future direction would be to assess both parents of a child. Assessing the agreement on their coparenting could be an interesting additional support for the validity.
Thirdly, there are limitations inherent to data collection when performed both on paper and online. However, increasing evidence regarding collection methods shows that there are no significant differences between the two formats (Gosling et al., 2004; Hunter, 2012). It is our opinion that this mixed mode facilitates participation, as families can choose according to their preference. It also allows for more representative samples as it facilitates participation of families around the country, and it reduces both response time and collection efforts by simultaneously allowing face-to-face or online (an email address was provided) resolution of questions and contact with the team. Both systems guaranteed participant confidentiality.
This instrument has the limitations of any self-reported measure, mainly the bias of being answered from the respondent’s point of view. Notwithstanding this, the extensive and established use of self-reports in psychology contexts, both clinical and research, proves that the advantages outweigh this limitation when responses are interpreted by qualified, experienced professionals with other clinical information available. Moreover, there are different observational tools available if an external behaviorally anchored measurement is needed (Carneiro et al., 2006; Favez et al., 2006; McHale et al., 2001; McConnell & Kerig, 2002).
In conclusion, the current study indicates that the CECOP is a valid and reliable one-factor measure for assessing coparenting in Spanish families. The excellent psychometric properties show that this brief 15-item measure is sufficient to provide conceptual and empirical information on particular coparenting practices. Its use allows a more comprehensive clinical assessment by providing information on the family environment of given children or adolescents from a systemic point of view. The normative data improve this assessment by establishing cut-off points that indicate how functional the coparenting is. Moreover, the fact that it is a short and self-reported instrument has the added value of making it suitable for clinical settings where time is limited. However, considering the importance of assessing family relationships in clinical settings, the psychometric properties of the CECOP should be studied with clinical populations, so cut-off points for different mental health disorders can be established and thereby more value can be provided when it is applied in clinical settings. Further validation of this instrument should study whether there is a need to adapt some items or provide different cut-off points regarding children’s ages. Future studies should focus on studying the relationship between coparenting and children’s development and psychological adjustment. That will also allow further studies of the relationship between coparenting and psychopathology. Finally, studies focusing on the predictive evidence of the CECOP would also be of interest, as this would facilitate its use to assess change during psychological and family interventions.
Data Availability
The data that support the findings of this study are available from the corresponding author, LMC, upon reasonable request.
References
American Educational Research Association, American Psychological Association, & National Council on Measurement in Education (2014). Standards for educational and psychological testing. Washington, DC: American Educational Research Association.
Andrés, A., Saldaña, C., & Gómez-Benito, J. (2009). Establishing the stages and processes of change for weight loss by consensus of experts. Obesity (Silver Spring, Md.), 17(9), 1717–1723. https://doi.org/10.1038/oby.2009.100.
Ballús Creus, C. (1991). Adaptación del Parental Bonding Instrument [Adaptation of the Parental Bonding Instrument]. [Doctoral Dissertation]. Barcelona: Escuela Profesional de Psicología Clínica.
Baril, M. E., Crouter, A. C., & McHale, S. M. (2007). Processes linking adolescent well-being, marital love, and coparenting. Journal of Family Psychology, 21(4), 645–654. https://doi.org/10.1037/0893-3200.21.4.645.
Belsky, J., Woodworth, S., & Crnic, K. (1996). Trouble in the second year: three questions about family interaction. Child Development, 67(2), 556–578. https://doi.org/10.2307/1131832.
Bonds, D. D., & Gondoli, D. M. (2007). Examining the process by which marital adjustment affects maternal warmth: the role of coparenting support as a mediator. Journal of Family Psychology, 21(2), 288–296. https://doi.org/10.1037/0893-3200.21.2.288.
Caldera, Y. M., & Lindsey, E. W. (2006). Coparenting, mother-infant interaction, and infant-parent attachment relationships in two-parent families. Journal of Family Psychology, 20(2), 275–283. https://doi.org/10.1037/0893-3200.20.2.275.
Carneiro, C., Corboz-Warnery, A., & Fivaz-Depeursinge, E. (2006). The prenatal Lausanne Trilogue Play: A new observational assessment tool of the prenatal co-parenting alliance. Infant Mental Health Journal, 27(2), 207–228. https://doi.org/10.1002/imhj.20089.
Carretero-Dios, H., & Pérez, C. (2005). Normas para el desarrollo y revisión de estudios instrumentales [Standards for the development and review of instrumental studies]. International Journal of Clinical and Health Psychology, 5(3), 521–551. http://www.aepc.es/ijchp/articulos_pdf/ijchp-158.pdf.
Cheung, G. W., & Rensvold, R. B. (2002). Evaluating goodness-of-fit indexes for testing measurement invariance. Structural Equation Modeling, 9(2), 233–255. https://doi.org/10.1207/S15328007SEM0902_5.
Chirumbolo, A., Urbini, F., Callea, A., Lo Presti, A., & Talamo, A. (2017). Occupations at risk and organizational well-being: an empirical test of a job insecurity integrated model. Frontiers in Psychology, 8, 2084. https://doi.org/10.3389/fpsyg.2017.02084.
Cowan, C. P., Cowan, P. A., Pruett, M. K., & Pruett, K. (2007). An approach to preventing coparenting conflict and divorce in low-income families: strengthening couple relationships and fostering fathers’ involvement. Family Process, 46(1), 109–121. https://doi.org/10.1111/j.1545-5300.2006.00195.x.
Cowan, C. P., & Cowan, P. A. (2000). When partners become parents: The big life change for couples. Lawrence Erlbaum Associates Publishers.
Davies, P. T., & Cummings, E. M. (1994). Marital conflict and child adjustment: An emotional security hypothesis. Psychological Bulletin, 116(3), 387–411. https://doi.org/10.1037/0033-2909.116.3.387.
Davies, P. T., & Lindsay, L. L. (2001). Does gender moderate the effects of marital conflict on children? In J. H., Grych & F.D. Fincham (Eds.), Interparental conflict and child development (pp. 64–97). Cambridge University Press.
De Winter, J. C. F., & Dodou, D. (2012). Factor recovery by principal axis factoring and maximum likelihood factor analysis as a function of factor pattern and sample size. Journal of Applied Statistics, 39(4), 695–710. https://doi.org/10.1080/02664763.2011.610445.
Erel, O., & Burman, B. (1995). Interrelatedness of marital relations and parent-child relations: a meta-analytic review. Psychological Bulletin, 118(1), 108–132. https://doi.org/10.1037/0033-2909.118.1.108.
Favez, N., Frascarolo, F., Carneiro, C., Montfort, V., Corboz-Warnery, A., & Fivaz-Depeursinge, E. (2006). The Development of the family Alliance from Pregnancy to Toddlerhood and Children Outcomes at 18 Months. Infant and Child Development, 15(1), 59–73. https://doi.org/10.1002/icd.430.
Feinberg, M. E. (2003). The internal structure and ecological context of coparenting: a framework for research and intervention. Parenting, 3(2), 95–131. https://doi.org/10.1207/S15327922PAR0302_01.
Feinberg, M. E., Brown, L. D., & Kan, M. L. (2012). A multi-domain self-report measure of coparenting. Parenting, 12(1), 1–21. https://doi.org/10.1080/15295192.2012.638870.
Feldman, R., Masalha, S., & Derdikman-Eiron, R. (2010). Conflict resolution in the parent-child, marital, and peer contexts and children’s aggression in the peer group: a process-oriented cultural perspective. Developmental Psychology, 46(2), 310–325. https://doi.org/10.1037/a0018286.
Ferrando, P. J., Lorenzo-Seva, U., Hernández-Dorado, A., & Muñiz, J. (2022). Decálogo para el Análisis Factorial de los Ítems de un Test [Decalogue for the Factor Analysis of Test Items]. Psicothema, 34(1), 7–17. https://doi.org/10.7334/psicothema2021.456.
Flaskas, C. (2012). The space of reflection: thirdness and triadic relationships in family therapy. Journal of Family Therapy, 34, 138–156. https://doi.org/10.1111/j.1467-6427.2012.00587.x.
Gosling, S. D., Vazire, S., Srivastava, S., & John, O. P. (2004). Should we trust web-based studies? A comparative analysis of six preconceptions about internet questionnaires. The American psychologist, 59(2), 93–104. https://doi.org/10.1037/0003-066X.59.2.93.
Hagen, N. A., Stiles, C., Nekolaichuk, C., Biondo, P., Carlson, L. E., Fisher, K., & Fainsinger, R. (2008). The Alberta Breakthrough Pain Assessment Tool for cancer patients: a validation study using a Delphi process and patient think-aloud interviews. Journal of Pain and Symptom Management, 35(2), 136–152. https://doi.org/10.1016/j.jpainsymman.2007.03.016.
Hayton, J. C., Allen, D. G., & Scarpello, V. (2004). Factor Retention Decisions in Exploratory Factor Analysis: A Tutorial on Parallel Analysis. Organizational Research Methods, 7(2), 191–205. https://doi.org/10.1177/1094428104263675.
Hooper, D., Coughlan, J. P., & Mullen, M. R. (2008). Structural equation modelling: guidelines for determining model fit. Electronic Journal of Business Research Methods, 6(1), 53–60. https://doi.org/10.21427/D7CF7R.
Hunter, L. (2012). Challenging the reported disadvantages of e-questionnaires and addressing methodological issues of online data collection. Nurse researcher, 20(1), 11–20. https://doi.org/10.7748/nr2012.09.20.1.11.c9303.
Ibáñez Martínez, N., Linares, J. L., Vilaregut Puigdesens, A., Virgili Tejedor, C., & Campreciós Orriols, M. (2012). Propiedades psicométricas del Cuestionario de Evaluación de las Relaciones Familiares Básicas (CERFB) [Psychometric properties of the Basic Family Relations Inventory (BFRI)]. Psicothema, 24(3), 489–494. http://www.psicothema.com/pdf/4044.pdf.
Johnson, V. K., Cowan, P. A., & Cowan, C. P. (1999). Children’s classroom behavior: The unique contribution of family organization. Journal of Family Psychology, 13(3), 355–371. https://doi.org/10.1037/0893-3200.13.3.355.
Karreman, A., van Tuijl, C., van Aken, M. A. G., & Deković, M. (2008). Parenting, coparenting, and effortful control in preschoolers. Journal of Family Psychology, 22(1), 30–40. https://doi.org/10.1037/0893-3200.22.1.30.
Kolak, A. M., & Vernon-Feagans, L. (2008). Family-level coparenting processes and child gender as moderators of family stress and toddler adjustment. Infant and Child Development, 17(6), 617–638. https://doi.org/10.1002/icd.577.
Leal, D., Gato, J., Coimbra, S., Tasker, F., & Tornello, S. (2022). The prospective co-parenting relationship scale (PCRS) for sexual minority and heterosexual people: Preliminary validation. International Journal of Environmental Research and Public Health, 19(10), 6345 https://doi.org/10.3390/ijerph19106345.
Margolin, G., Gordis, E. B., & John, R. S. (2001). Coparenting: a link between marital conflict and parenting in two-parent families. Journal of Family Psychology, 15(1), 3–21. https://doi.org/10.1037/0893-3200.15.1.3.
McConnell, M. C., & Kerig, P. K. (2002). Assessing coparenting in families of school-age children: Validation of the Coparenting and Family Rating System. Canadian Journal of Behavioural Science / Revue canadienne des sciences du comportement, 34(1), 44–58. https://doi.org/10.1037/h0087154.
McHale, J. P. (1995). Coparenting and triadic interactions during infancy: the roles of marital distress and child gender. Developmental Psychology, 31(6), 985–996. https://doi.org/10.1037/0012-1649.31.6.985.
McHale, J. P. (2007). When infants grow up in multiperson relationship systems. Infant Mental Health Journal, 28(4), 370–392. https://doi.org/10.1002/imhj.20142.
McHale, J., Johnson, D., & Sinclair, R. (1999). Family dynamics, preschoolers’ family representations, and preschool peer relationships. Early Education Development, 10(3), 373–401. https://doi.org/10.1207/s15566935eed1003_8.
McHale, J. P., Kuersten-Hogan, R., & Lauretti, A. (2001). Evaluating coparenting and family-level dynamics during infancy and early childhood: The Coparenting and Family Rating System. In P. K. Kerig & K. M. Lindahl (Eds.), Family observational coding systems: Resources for systemic research (pp. 151–170). Lawrence Erlbaum Associates Publishers.
Mollà Cusí, L., Günther-Bel, C., Vilaregut Puigdesens, A., Campreciós Orriols, M., & Matalí Costa, J. L. (2020). Instruments for the Assessment of Coparenting: A Systematic Review. Journal of Child and Family Studies, 29(9), 2487–2506. https://doi.org/10.1007/s10826-020-01769-3.
Muñiz, J., & Fonseca-Pedrero, E. (2019). Diez pasos para la construcción de un test [Ten steps for test development]. Psicothema, 31(1), 7–16. https://doi.org/10.7334/psicothema2018.291.
Murphy, S. E., Jacobvitz, D. B., & Hazen, N. L. (2016). What’s so bad about competitive coparenting? Family-level predictors of children’s externalizing symptoms. Journal of Child and Family Studies, 25(5), 1684–1690. https://doi.org/10.1007/s10826-015-0321-5.
Nasa, P., Jain, R., & Juneja, D. (2021). Delphi methodology in healthcare research: How to decide its appropriateness. World journal of methodology, 11(4), 116–129. https://doi.org/10.5662/wjm.v11.i4.116.
Parker, G., Tupling, H., & Brown, L. B. (1979). A parental bonding instrument. British Journal of Medical Psychology, 52(1), 1–10. https://doi.org/10.1111/j.2044-8341.1979.tb02487.x.
Pruett, M. K., Pruett, K. D., Cowan, C. P., & Cowan, P. A. (2017). Enhancing paternal engagement in a coparenting paradigm. Child Development Perspectives, 11(4), 245–250. https://doi.org/10.1111/cdep.12239.
Saini, M., Pruett, M. K., Alschech, J., & Suschchyk, A. R. (2019). A pilot study to assess Coparenting Across Family Structures (CoPAFS). Journal of Child and Family Studies, 28(5), 1392–1401. https://doi.org/10.1007/s10826-019-01370-3.
Pruett, M. K., Alschech, J., & Saini, M. (2021). The impact of coparenting on mothers’ COVID-19-related stressors. Social Sciences, 10(8), 311 https://doi.org/10.3390/socsci10080311.
Schoppe-Sullivan, S. J., Mangelsdorf, S. C., & Frosch, C. A. (2001). Coparenting, family process, and family structure: Implications for preschoolers’ externalizing behavior problems. Journal of Family Psychology, 15(3), 526–545. https://doi.org/10.1037/0893-3200.15.3.526.
Solmeyer, A. R., Feinberg, M. E., Coffman, D. L., & Jones, D. E. (2014). The effects of the family foundations prevention program on coparenting and child adjustment: a mediation analysis. Prevention Science: The Official Journal of the Society for Prevention Research, 15(2), 213–223. https://doi.org/10.1007/s11121-013-0366-x.
Tabachnick, B. G., & Fidell, L. S. (2007). Using multivariate statistics (5th ed.) (pp. 677). Allyn & Bacon/Pearson Education.
Teubert, D., & Pinquart, M. (2010). The association between coparenting and child adjustment: a meta-analysis. Parenting, 10(4), 286–307. https://doi.org/10.1080/15295192.2010.492040.
Turner, N. E. (1998). The effect of common variance and structure pattern on random data eigenvalues: Implications for the accuracy of parallel analysis. Educational and Psychological Measurement, 58(4), 541–568. https://doi.org/10.1177/0013164498058004001.
Ugazio, V., Pennacchio, R., Fellin, L., Guarnieri, S., & Anselmi, P. (2020). Explaining symptoms in systemic therapy. Does triadic thinking come into play? Frontiers in Psychology, 11, 597. https://doi.org/10.3389/fpsyg.2020.00597.
Umemura, T., Christopher, C., Mann, T., Jacobvitz, D., & Hazen, N. (2015). Coparenting problems with toddlers predict children’s symptoms of psychological problems at age 7. Child Psychiatry and Human Development, 46(6), 981–996. https://doi.org/10.1007/s10578-015-0536-0.
Van Egerenl, L. A., & Hawkins, D. P. (2004). Coming to terms with coparenting: implications of definition and measurement. Journal of Adult Development, 11(3), 165–178. https://doi.org/10.1023/B:JADE.0000035625.74672.0b.
Walsh, F. (2016). Applying a family resilience framework in training, practice, and research: mastering the art of the possible. Family Process, 55(4), 616–632. https://doi.org/10.1111/famp.12260.
Worthington, R. L., & Whittaker, T. A. (2006). Scale development research: a content analysis and recommendations for best practices. The Counseling Psychologist, 34(6), 806–838. https://doi.org/10.1177/0011000006288127.
Yárnoz-Yaben, S., & Comino, P. (2010). El CAD-S, un instrumento para la evaluación de la adaptación al divorcio-separación [The CAD-S, an instrument for the evaluation to divorce-separation]. Psicothema, 22(1), 157–162. http://www.psicothema.com/pdf/3711.pdf.
Yárnoz-Yaben, S. (2010). Cuestionario de Apoyo Recibido de la Ex pareja (CARE): un instrumento breve para evaluar la co-parentalidad post divorcio [Questionnaire of the Support Received from the Former Partner (CARE): a brief instrument to assess post-divorce co-parenting]. Revista de Psicopatología y Psicología Clínica, 15(2), 133–142.
Zemp, M., Johnson, M. D., & Bodenmann, G. (2018). Within-family processes: interparental and coparenting conflict and child adjustment. Journal of Family Psychology, 32(3), 299–309. https://doi.org/10.1037/fam0000368.
Funding
This work was supported by the Spanish Ministerio de Ciencia, Innovación y Universidades (via grant RETOS 2017: PSI2017-83146-R). Open Access funding provided thanks to the CRUE-CSIC agreement with Springer Nature.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Ethical approval
The authors affirm having followed professional ethical guidelines in preparing this work. These guidelines include obtaining informed consent from human participants, maintaining ethical treatment and respect for the rights of human or animal participants, and ensuring the privacy of participants and their data, such as ensuring that individual participants cannot be identified in reported results or from publicly available original or archival data.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mollà Cusí, L., Vilaregut Puigdesens, A., Callea, A. et al. Questionnaire for the Assessment of Coparenting (CECOP): Development and Validation. J Child Fam Stud (2024). https://doi.org/10.1007/s10826-024-02886-z
Accepted:
Published:
DOI: https://doi.org/10.1007/s10826-024-02886-z