
Abstract
Objectives
We report an investigation into processes of change in a randomized controlled trial of Stepping Stones Triple P (SSTP) and acceptance and commitment therapy (ACT) for families of children with cerebral palsy (CP). In comparison with the control group, the SSTP-only group showed improvements in child behavior problems and emotional symptoms and the SSTP-plus-ACT group showed benefits in child behavior problems, child hyperactivity, dysfunctional parenting styles, child functional performance in the mobility domain, child quality of life, and parental adjustment.
Methods
Sixty-seven parents of children with CP were randomly allocated to one of three groups: waitlist control, SSTP-only and SSTP-plus-ACT groups. We investigated three potential processes of change: parenting style, parental attitude to child emotion, and parental psychological flexibility. We used bootstrapping to perform the mediation analysis.
Results
Contrary to the existing literature, we find that neither dysfunctional parenting styles nor parental attitude to child emotion were significant mediators of the intervention effect on child behavior and adjustment. Consistent with existing literature, we find that psychological flexibility mediates the intervention effect on dysfunctional parenting styles (overreactivity confidence interval [CI] = −0.4750 to −0.115) and parental adjustment (depressive symptoms CI = −6.5641 to −0.5922; stress CI = −6.0546 to −0.4195).
Conclusions
Overall, our findings support the conclusion that ACT makes a unique contribution to parenting intervention.
Clinical Trial Registration
Australian New Zealand Clinical Trials Registry (00336291).
Similar content being viewed by others

Avoid common mistakes on your manuscript.
For psychological therapies to continue to improve and innovate, it is vital that researchers empirically test the proposed processes of change. We report an investigation into the processes of change in a randomized controlled trial (RCT) of the parenting interventions Stepping Stones Triple P (SSTP) and acceptance and commitment therapy (ACT) for families of children with cerebral palsy (CP; Whittingham et al. 2013). SSTP is a variant of the behavioral parenting intervention, the Positive Parenting Program “Triple P,” for families of children with disabilities (Sanders et al. 2003). Families within the RCT were randomly allocated to one of three groups: SSTP-only, SSTP-plus-ACT and waitlist control groups. All outcomes were parent report. The results of the RCT have already been published in two papers, as primary (Whittingham et al. 2014) and secondary (Whittingham et al. 2016) outcomes. In sum, the SSTP-only group, in comparison with the control group, benefitted in terms of child behavior problems and emotional symptoms (Whittingham et al. 2014). The SSTP-plus ACT group, in comparison with the control group, benefitted in terms of child behavior problems, child hyperactivity (Whittingham et al. 2014), dysfunctional parenting styles (Whittingham et al. 2014), child functional performance in the mobility domain (Whittingham et al. 2016), child quality of life (Whittingham et al. 2016), and parental adjustment (Whittingham et al. 2016). No significant differences were found between the two intervention groups at post intervention (Whittingham et al. 2014; Whittingham et al. 2016).
The results of this RCT are consistent with those of the wider literature, showing that SSTP (Tellegen and Sanders 2013) and ACT are both efficacious interventions (Ost 2008; Ruiz 2010, 2012). However, what can we say about the processes of change? In parenting interventions, such as Triple P, researchers have shown changes in parenting behavior to be the mechanism for changes in child behavior (Sanders and Dadds 1993). Recent studies examining mechanisms for change in parenting interventions support this viewpoint (Gardner et al. 2006; Gardner et al. 2010).
For ACT, the underlying theoretical model suggests that change in psychological flexibility is the key process for change and studies increasingly support this suggestion (Hayes et al. 2006). Dysfunctional parenting behavior, such as overreactivity, may result not just from a skills deficit, but also because the behavior serves a psychological function for the parent (Coyne and Wilson 2004; Dumas 2005; Murrell et al. 2008). ACT can address this psychological function. We can expect ACT to increase psychological flexibility and through such increase, reduce dysfunctional parenting style, and in turn, improve child behavior. In an RCT comparing SSTP and ACT with a waitlist control for families of children with acquired brain injury (ABI), the researchers found significant differences in psychological flexibility relating to parenting children with ABI for the intervention group (Brown et al. 2015). Further, changes in psychological flexibility mediated changes in parental adjustment and dysfunctional parenting (Brown et al. 2014).
Exposure to ACT may also change the way that parents respond to their child’s emotional life. Many authors have documented the links between parental acceptance of child emotions and child emotional development (Gottman et al. 1996; Gottman et al. 1997; Katz et al. 1999). The primary results of the aforementioned RCT for children with CP hinted at this possibility, since the SSTP-only group showed improvements in parent-reported child emotional symptoms relative to the control group, but the SSTP-plus-ACT group did not (Whittingham et al. 2014). It is difficult to understand how ACT could have undermined an intervention effect of SSTP. One plausible explanation is that ACT enhanced parental ability to recognize emotional symptoms in their children and the increased reporting of emotional symptoms negated the intervention effect.
In this study, we focus on testing hypothesized processes of change in an RCT of SSTP and ACT for families of children with CP. In particular, we predict that: (a) parenting style will mediate the intervention effect on child behavior and adjustment, (b) parental attitude to child emotion will mediate the intervention effect on child behavior and adjustment, (c) parental psychological flexibility will mediate the intervention effect on parenting style, and (d) parental psychological flexibility will mediate the intervention effect on parental adjustment.
Methods
Participants
Participants were parents of children (2–12 years) with a diagnosis of CP (all gross motor functioning severity levels), who self-identified as needing a parenting intervention. We recruited participants from the databases of the Queensland Cerebral Palsy and Rehabilitation Research Centre, the Cerebral Palsy League, and the Queensland Cerebral Palsy Register and through presentation at the Queensland Cerebral Palsy Health Service. We based ample size calculations on the primary outcome, child behavior, and on the primary study design, the RCT itself. An effect size of 0.25 was assumed because it is consistent with a clinically important difference of 0.5 SD and is comparable to the effect size for SSTP obtained with families of children with ASD, η² = 0.27 (Whittingham et al. 2009). Thus, the target sample sizes were 98 (power 0.8, 2-tailed, p = 0.05) and 110, accounting for attrition. We did not reach the recruitment goal and the final sample size was 67 (SSTP n = 22; SSTP + ACT n = 23; waitlist control n = 22).
Procedure
The published study protocol details the study design in full (Whittingham et al. 2013). This was an RCT with participating families randomly assigned to one of three groups: waitlist control, SSTP-only, and SSTP-plus-ACT groups. The waitlist control group was offered SSTP following post-intervention assessment for ethical reasons.
We completed the randomization process by computerized sequence generation with block randomization to ensure equal (or near equal) allocation of participants to groups. A staff member not involved in this study placed the group allocations in sealed, opaque, numbered envelopes. When a new family enrolled in the study, the coordinator opened the next envelope in sequence and randomized the family to one of the three aforementioned groups.
The interventions (SSTP and SSTP + ACT) were delivered in a combined group (3–10 families per group) and telephone format. SSTP consisted of six (2-h) group sessions plus three (30-min) telephone consultations, and psychologists with accreditation in SSTP delivered it. SSTP sessions included strategies for building a positive parent–child relationship, encouraging desirable behavior, teaching new skills and behaviors, managing misbehavior, and managing high-risk situations. For the SSTP-plus-ACT group, the ACT sessions (two 2-h group sessions) preceded SSTP. ACT sessions included identifying values, mindfulness, cognitive defusion, acceptance of emotions, and committed action. For some groups, a weekend workshop format was used (all group sessions in a single weekend) to allow for intervention delivery as an outreach program in far North Queensland. In all, 11 participants received the intervention via the weekend workshop format (SSTP = 4; SSTP + ACT = 4; waitlist control = 3). The therapist delivering the intervention completed an intervention protocol adherence checklist for every session. For 50% of sessions, a second therapist also rated the protocol delivery. The therapists were in complete agreement. In all circumstances, the therapists delivered the content in full. In 8.19% of sessions, the therapist did not play some aspect of the SSTP digital video disc (DVD) due to technical difficulties or time management issues.
Measures
We gathered demographic data using the Family Background Questionnaire (Sanders et al. 2009) and classified gross motor functional ability using the parent report version of the Gross Motor Function Classification System (Palisano 1997). All outcome measures were parent report, and these were completed online at baseline and immediately post intervention. Since our aim was to explore mediation pathways for intervention effects, we included only outcomes that demonstrated significant intervention effects as reported in the studies on the primary (Whittingham et al. 2014) and secondary (Whittingham et al. 2016) outcomes. We conducted all outcomes in this study immediately post intervention. We conducted follow up at six months but with significant attrition, and hence, do not examine it in this study.
Child behavior and adjustment
We used the Eyberg Child Behavior Inventory (ECBI) and the Strengths and Difficulties Questionnaire (SDQ) to measure child behavior and adjustment. The ECBI (Eyberg and Pincus 1999) produces two scales, the Intensity and the Problem scales, reflecting the intensity of child behavior problems and the number of such problems, respectively. Researchers agree that the ECBI shows high reliability and validity (Boggs et al. 1990; Eyberg and Ross 1978), and it showed excellent internal consistency in this study, for the Intensity (α = 0.95) and Problem (α = 0.90) scales. The SDQ measures child behavior and adjustment across five subscales: Emotional Symptoms, Conduct Problems, Inattention/Hyperactivity, Peer Problems, and Prosocial Behavior (Goodman 1997). The SDQ has good internal and test–retest reliability. Consistent with reported significant effects, we decided to use only the Emotional Symptoms (α = 0.69) and Hyperactivity (α = 0.77) subscales.
Dysfunctional parenting styles
We measured dysfunctional parenting styles using the Parenting Scale (PS). The PS (Arnold et al. 1993) is a measure of three dysfunctional discipline styles: Laxness, Overreactivity, and Verbosity. The PS shows strong reliability and validity. Consistent with reported significant effects, we decided to use only the Overreactivity (α = 0.81) and Verbosity (α = 0.67) subscales.
Parental psychological adjustment
We used the Depression Anxiety and Stress Scales (DASS; Lovibond and Lovibond 1995) to assess symptoms of depression, anxiety, and stress in adults. The DASS produces three subscales, each with good internal consistency: the Depression (Α = 0.91), Anxiety (Α = 0.84), and Stress (α = 0.90) scales. The DASS also has good discriminant and concurrent validity (Brown et al. 1997; Lovibond and Lovibond 1995). Consistent with reported significant effects, we decided to use only the Depression (α = 0.95) and Stress subscales (α = 0.94).
Parent psychological flexibility
The Acceptance and Action Questionnaire (AAQ) child disability version is an adaptation of the AAQ (Hayes et al. 2003), focusing on psychological flexibility since it relates to parenting a child with a disability (e.g., “I do things that I care about even when I feel sad about my child’s disability.”). Studies have shown the original AAQ to have good concurrent validity and adequate test–retest reliability (r = 0.64); its internal consistency in this study was fair (α = 0.80). We assigned scores in the AAQ child disability version such that higher scores reflect greater psychological flexibility.
Parental attitude toward child emotions
The Parent Beliefs about Negative Emotions Questionnaire measures parental attitudes toward their children’s emotions (Halberstadt et al. 2001; Halberstadt et al. 2008). In this study, we use two subscales: (1) Emotions are Dangerous (α = 0.80) and (2) Negative Emotions are Valuable (α = .0.81). The literature shows that this Questionnaire has good concurrent validity.
Data Analyses
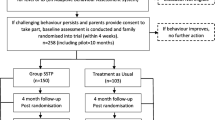
We conducted bootstrapping (with 10,000 re-samples) to determine mediation for each of the hypotheses. Bootstrapping is a nonparametric approach to mediation analysis that tests and empirically quantifies the indirect effect (ab) of the independent variable, X, on the dependent variable Y, as mediated by the tested mediator M (Preacher and Hayes 2008). We can also examine mediation pathways (a = effect of X on M, b = effect of M on Y) and the direct effects of X on Y (c); see Fig. 1.

Mediation pathways. Indirect effect of X on Y through M = ab. Direct effect of X on Y = c
We used the software SPSS 24 in combination with the Marco Process v2.16 (Hayes 2013). We used dummy coding to allow for the use of bootstrapping with a multicategorical independent variable (Hayes and Preacher 2014). We performed dummy coding so that the waitlist control group functions as the reference category. We measured the mediators and the dependent variables post intervention for pragmatic reasons. In all analyses, we used baseline assessments as covariates for both mediators and dependent variables. In bootstrapping, significant effects are indicated by confidence intervals (CIs) that do not span zero. In all cases, we reported a 95% CI.
Results
Preliminary Analysis and Assumption Testing
Less than 10% of data were missing, and the pattern of missing data was random. In generating scale scores, if < 30% of items were missing for that participant on that scale, we generated the scale score from the remaining items. If > 30% of items were missing for that participant, we excluded that participant from the analysis for that scale. We present sample characteristics in Table 1.
Does Parenting Style Mediate the Intervention Effect on Child Behavior and Adjustment?
We conducted a mediation analysis with Y = ECBI intensity scale, X = group allocation, and M = parental overreactivity and parental verbosity. We found that the direct effect of the intervention was significant for the SSTP-plus-ACT group, as shown by the CI that did not include zero (c = −19.7614, CI = −35.3514 to −4.714), but not for the SSTP-only group (c = 9.6484, CI = −24.7877 to 5.4908). We did not find significant indirect effects for the SSTP-plus-ACT group (overreactivity ab = 0.2359, CI = −7.5661 to 11.0890; verbosity ab = 0.12057, CI = −5.8496 to 11.8450) or the SSTP-only group (overreactivity ab = 0.1333, CI = −4.7545 to 8.7281; verbosity ab = 0.8247, CI = −3.4770 to 10.5300). Examining mediation pathways, we found that the intervention significantly affected overreactivity (a = −0.5933, CI = −1.0251 to −0.1615) and verbosity (a = −0.7642, CI = −1.3018 to −0.2267), but not for the SSTP-only group (overreactivity a = −0.3352, CI = −0.7811 to 0.1107; verbosity a = −0.5227, CI = −1.0779 to 0.0324). We found that parenting style did not significantly affect child behavior (overreactivity b = −0.3976, CI = −13.1474 to 12.3523; verbosity b = −1.5776, CI = −12.6226 to 9.4675).
We conducted a mediation analysis with Y = ECBI problem scale, X = group allocation, and M = parental overreactivity and parental verbosity. We found that the direct effect of the intervention was significant for the SSTP-plus-ACT (c = −6.8447, CI = −11.1147 to −2.5748) and the SSTP-only groups (−5.0736, CI = −9.3197 to −0.274). We did not find significant indirect effects for the SSTP-plus-ACT group (overreactivity ab = −1.3969, CI = −4.3567 to 0.3956; verbosity ab = 0.3991, CI = −1.1941 to 2.9220) or the SSTP-only group (overreactivity ab = −0.8173, CI = −3.5425 to 0.3756; verbosity ab = 0.3029, CI = −0.8094 to 2.5966). Examining mediation pathways, we found that the intervention significantly affected overreactivity (a = −0.5799, CI = −1.0279 to 0.1318) and verbosity (a = −0.7556, CI = −1.2993 to −0.2118) for the SSTP-plus-ACT group and verbosity (a = −0.5734, CI = −1.1422 to −0.0446) but not overreactivity (a = −0.3393, CI = −0.8079 to 0.1294) for the SSTP-only group. We found that parenting style did not affect the ECBI problem scale (overreactivity b = 2.4091, CI = −1.3588 to 6.1770; verbosity b = −0.5283, CI = −3.6460 to 2.5895).
Further, we conducted a mediation analysis with the Y = SDQ emotional symptoms subscale, X = group allocation, and M = parental overreactivity and parental verbosity. The direct effect of the intervention on child emotional symptoms was significant for the SSTP-only group (c = −1.1830, CI = −2.1190 to −0.2470) but not the SSTP-plus-ACT group (c = 0.0754, CI = −0.886 to 1.0375). We did not find significant indirect effects for the SSTP-plus-ACT (ab = −0.1656, CI = −0.7090 to 0.5295) or SSTP-only groups (ab = −0.1139, CI = 0.6701 to 0.2948). Examining mediation pathways, we found that the intervention significantly affected parental overreactivity (a = −0.5675, CI −0.9982 to −0.1368) and verbosity (a = −0.7451, CI = −1.2824 to −0.2077) for the SSTP-plus-ACT group but not the SSTP-only group (overreactivity a = −0.3189, CI = −0.7614 to 0.1235; verbosity a = −0.5123, CI = −1.0643 to 0.0397). Parenting style did not affect child emotional symptoms (overreactivity b = 0.2425, CI = −0.5433 to 1.0284; verbosity b = 0.223, CI = −0.4598 to 0.9044).
We conducted a mediation analysis with Y = SDQ hyperactivity/inattention subscale, X = group allocation, and M = parental overreactivity and parental verbosity. Our analysis revealed that the direct effect of the intervention on child hyperactivity was significant for the SSTP-plus-ACT group (c = −1.6257, CI = −2.9317 to −0.3197) but not the SSTP-only group (c = −0.6303, CI = −1.8756 to 0.6149). We did not find significant indirect effects for the SSTP-plus-ACT (ab = −4845, CI = −1.4487 to 0.3673) or the SSTP-only groups (ab = −0.3297, CI = −1.2026 to 0.1966). The intervention significantly affected parental overreactivity (a = −0.6041, CI = −1.0568 to −0.1514) and verbosity (a = 0.7798, CI = −1.3424 to −0.2172) for the SSTP-plus-ACT group but not the SSTP-only group (overreactivity a = −0.3379, CI = −0.7911 to 0.1152; verbosity a = −0.5306, CI = −1.0938 to 0.0326). Further, parenting style did not affect child hyperactivity (overreactivity b = −0.2954, CI = −1.3164 to 0.7274, verbosity b = 0.6213, CI = −0.2692 to 1.5118).
Does Parental Attitude to Child Emotion Mediate the Intervention Effect on Child Behavior and Adjustment?
We conducted a mediation analysis with Y = ECBI intensity scale, X = group allocation, and M = emotions are dangerous and negative emotions are valuable subscales of the parental attitude to child emotions questionnaire. The direct effect of the intervention on child behavior was significant for both the SSTP-plus-ACT (c = −22.2794, CI = −36.6505 to −7.9082) and the SSTP-only (c = −15.7921, CI = 31.1047 to −0.4795) groups. We did not find a significant indirect effect of the intervention on child behavior for the SSTP-plus-ACT (valuable ab = −1.5105, CI = −8.9719 to 1.3617; dangerous ab = 0.3450, CI = −1.0718 to 4.8310) or the SSTP-only (valuable ab = −1.4535, CI = −8.5030 to 1.3071; dangerous ab = 0.8591, CI = −0.8851 to 6.3554) groups. Examining mediation pathways, we found that the intervention did not affect parental attitudes to child emotion for either the SSTP-plus-ACT (valuable ab = −3.0958, CI = −9.2792 to 3.0876; dangerous ab = −1.3486, CI = −7.5763 to 4.8791) or the SSTP-only (valuable ab = −2.9792, CI = −9.4812 to 3.5229; dangerous ab = −3.3578, CI = −9.9064 to 3.1907) group. In addition, parental attitude to child emotion did not affect child behavior (valuable b = 0.4879, CI = −0.2275 to 1.2033; dangerous b = −0.2558, CI = −0.9661 to 0.4544).
Does Parental Psychological Flexibility Mediate the Intervention Effect on Parenting Style?
We conducted a mediation analysis with Y = parental overreactivity, X = group allocation, and M = psychological flexibility. The direct effect of the intervention on parental overreactivity was not significant for the SSTP-plus-ACT group (c = −0.3842, CI = −0.8068 to 0.0385) or the SSTP-only group (c = −0.1175, CI = −0.5386 to 0.3035). The CI for the indirect effect was entirely below zero for the SSTP-plus-ACT group, indicating a significant effect (ab = −0.1490, CI = −0.4750 to −0.115) but not for the SSTP-only group (ab = −0.0706, CI = −0.3098 to 0.430). Examining mediation pathways, we found that the intervention did not significantly affect psychological flexibility for either the SSTP-plus-ACT group (a = −6.5691, CI = −13.1754 to 0.0372) or the SSTP-only group (a = −3.1126, CI = −9.8988 to 3.6735). Further, psychological flexibility significantly affected parental overreactivity (b = 0.022, CI = 0.0050 to 0.403).
We conducted a mediation analysis with Y = parental verbosity, X = group allocation, and M = psychological flexibility. The direct effect of the intervention on parental verbosity was not significant for the SSTP-plus-ACT group (c = 0.3952, CI = −0.1491 to 0.9395) or the SSTP-only group (c = −0.1538, CI = −0.7000 to 0.3924). The indirect effect was not significant for the SSTP-plus-ACT group (ab = 0.3952, CI = −0.0004 to 0.0022) or the SSTP-only group (ab = −0.0198, CI = −0.2148 to 0.0353). Examining mediation pathways, we found that the intervention did not significantly affect psychological flexibility for either the SSTP-plus-ACT group (a = 3.8771, CI = −2.5762 to 10.3305) or the SSTP-only group (a = −1.9326, CI = −8.4786 to 4.6134). In addition, psychological flexibility did not significantly affect parental verbosity (b = 0.0102, CI = −0.0134 to 0.0339).
Does Parental Psychological Flexibility Mediate the Intervention Effect on Parenting Adjustment?
We conducted a mediation analysis with Y = depressive symptoms, X = group allocation, and M = psychological flexibility. The direct effect of the intervention on depressive symptoms was not significant for the SSTP-plus-ACT (c = −2.7432, CI = −6.7832 to 1.2968) or the SSTP-only groups (c = −0.3848, CI = −0.4.5531 to 3.7834). We found a significant indirect effect for the SSTP-plus-ACT group (ab = −2.7015, CI = −6.5641 to −0.5922), but not for the SSTP-only group (ab = −1.7384, CI = −5.2916 to 0.1265). Examining mediation pathways, we found that the intervention significantly affected psychological flexibility for the SSTP-plus-ACT group (a = −6.7601, CI = −12.5834 to −0.9369) but not for the SSTP-only group (a = −4.3502, CI = −10.5547 to 1.8543). Further, psychological flexibility significantly affected reported depressive symptoms (b = 0.3996, CI = 0.2125 to 0.5868).
We conducted a mediation analysis with Y = stress, X = group allocation, and M = psychological flexibility. The direct effect of the intervention on stress was not significant for the SSTP-plus-ACT (c = −3.3593, CI = −7.4662 to 0.7477) or the SSTP-only groups (c = −0.0073, CI = −4.1996 to 4.1849). We found a significant indirect effect for the SSTP-plus-ACT group (ab = −2.3367, CI = −6.0546 to −0.4195) but not for the SSTP-only group (ab = −1.1680, CI = −40.651 to 0.5970). The intervention significantly affected psychological flexibility for the SSTP-plus-ACT group (a = −6.4695, CI = −12.4130 to −0.5261) but not the SSTP-only group (a = −3.2338, CI = −9.5172 to 3.0496). Moreover, psychological flexibility significantly affected stress (b = 0.3612, CI = 0.1737 to 0.5487).
Discussion
The lack of significant indirect effects of the intervention on child behavior and adjustment through the mediator parenting style is inconsistent with the existing literature on processes of change in parenting interventions (Gardner et al. 2006; Gardner et al. 2010). Possibly, the lack of effect is owing to the limited sample size. If yes, one plausible explanation may be that the exact processes of change, in terms of parent behavior, vary between populations. In families with typically developing children seeking parenting intervention because of externalizing behavioral problems, changes in the way that parents respond to externalizing behavior, as measured by questionnaires assessing dysfunctional parenting styles—such as overreactivity—may be a key process of change. However, that aspect of parenting behavior may not be the key process of change for families of children with disabilities, such as CP. Instead, for children with disabilities the key processes of change may be parental ability to teach new skills and behaviors through processes such as chaining and to reinforce actively their functional behaviors across a variety of contexts. As these children learn and reinforce new skills, their externalizing behaviors may naturally decrease independently of changes in parental response to externalizing behavior per se. Measures of dysfunctional parenting style, such as the PS, do not capture these aspects of parenting behavior. Yet, teaching and reinforcing adaptive behaviors does form important aspects of the intervention SSTP. Future research is required to investigate this explanation.
We did not find that parental attitude to child emotion mediates the intervention effect on child behavior and adjustment. We consider it likely that the measure we chose was not sufficiently grounded in parental behavior in response to child emotion, as opposed to parental attitude. Further, for ACT to alter parental responses to their child’s emotion, this change probably needs to be targeted specifically in the intervention. Within this RCT, it was not—the ACT component focused on parental coping only.
The findings in this study regarding the significant indirect effects of the SSTP and ACT interventions on parenting style, specifically parental overreactivity, and parental adjustment, specifically parental depressive symptoms and stress, through the mediator psychological flexibility are consistent with those in the existing literature on psychological flexibility as key process of change in ACT interventions (Hayes et al. 2006). This finding, that psychological flexibility is a significant mediator, further supports the conclusion that ACT has benefits for parents and parenting, over and above existing behavioral parenting interventions. Notably, we measured the mediators and dependent variables post intervention for all analyses. Thus, caution must be exercised in making causal attributions. We cannot consider our results true mediations, because we measured the mediators and the post-intervention variables at the same point in time. The SSTP-plus-ACT group received an additional four hours of intervention and the possibility that the additional intervention dose rather than the content of the intervention is responsible for the effect cannot be excluded. It is also important to acknowledge the limited sample size and the fact that all of the measures were parent report and, therefore, shared variance could have influenced findings. Future research should continue to establish and explore the unique contributions of ACT to parenting intervention. This should include trialing ACT interventions that specifically target parental response to their child emotion as well as measuring parental response (rather than attitude) to child emotion as an outcome. If parental response to child emotion can be effectively targeted then the flow on effects on child adjustment and psychological flexibility could also be tested. Future research should aim to measure all aspects of parenting behavior targeted in parenting interventions, and not just parental behavior in response to child misbehavior. These aspects should include parental ability to teach new skills and behaviors and parental response to functional child behavior.
References
Arnold, D. S., O’Leary, S. G., Wolff, L. S., & Acker, M. M. (1993). The parenting scale: a measure of dysfunctional parenting in discipline situations. Psychological Assessment, 5, 137–144.
Boggs, S., Eyberg, S., & Reynolds, L. (1990). Concurrent validity of the Eyberg child behavior inventory. Journal of Clinical Child & Adolescent Psychology, 19(1), 75–78.
Brown, T. A., Chorpita, B. F., Korotitsch, W., & Barlow, D. H. (1997). Psychometric properties of the Depression Anxiety Stress Scales (DASS) in clinical samples. Behavior Research and Therapy, 35(1), 79–89.
Brown, F. L., Whittingham, K., Boyd, R. N., & McKinlay, L. (2015). Does stepping stones triple p plus acceptance and commitment therapy improve parent, couple and family adjustment following paediatric acquired brain injury? A randomised controlled trial. Behavior Research and Therapy, 73, 58–66.
Brown, F. L., Whittingham, K., & Sofronoff, K. (2014). Parental experiential avoidance as a potential mechanism of change in a parenting intervention for parents of children with pediatric acquired brain injury. Journal of Pediatric Psychology, 40(4), 464–474.
Coyne, L. W., & Wilson, K. G. (2004). The role of cognitive fusion in impaired parenting: an RFT analysis. International Journal of Psychology and Psychological Therapy, 4(3), 469–486.
Dumas, J. E. (2005). Mindfulness-based parent training: strategies to lessen the grip of automaticity in families with disruptive children. Journal of Clinical Child & Adolescent Psychology, 34(4), 779–791.
Eyberg, S. M., & Pincus, D. (1999). Eyberg child behavior inventory and Sutter-Eyberg student behavior inventory–revised: professional manual. Odessa, FL: Psychological Assessment Resources.
Eyberg, S., & Ross, A. (1978). Assessment of child behavior problems: the validation of a new inventory. Journal of Clinical Child & Adolescent Psychology, 7(2), 113–116.
Gardner, F., Burton, J., & Klimes, I. (2006). Randomised controlled trial of a parenting intervention in the voluntary sector for reducing child conduct problems: outcomes and mechanisms of change. Journal of Child Psychology and Psychiatry, 47(11), 1123–1132.
Gardner, G., Hutchings, J., Bywater, T., & Whitaker, C. (2010). Who benefits and how does it work? Moderators and mediators of outcome in an effectiveness trail of a parenting intervention. Journal of Clinical Child & Adolescent Psychology, 39(4), 568–580.
Goodman, R. (1997). The strengths and difficulties questionnaire: a research note. Journal of Child Psychology and Psychiatry, 38(5), 581–586. https://doi.org/10.1111/j.1469-7610.1997.tb01545.x.
Gottman, J. M., Katz, L. F., & Hoover, C. (1996). Parental meta-emotion philosophy and the emotional life of families: Theoretical models and preliminary data. Journal of Family Psychology, 16(3), 243–268.
Gottman, J. M., Katz, L. F., & Hoover, C. (1997). Meta-emotion: how families communicate emotionally. Mahwah, NJ: Lawrence Erlbaum.
Halberstadt, A. G., Dunsmore, J. D., McElwain, N. M., Eaton, K. L., & McCool, A. (2001). Parents’ beliefs about negative emotions. Raleigh: North Carolina State University. [Unpublished questionnaire].
Halberstadt, A. G., Thompson, J. A., Parker, A. E., & Dunsmore, J. D. (2008). Parents’ emotion-related beliefs and behaviors in relation to children’s coping with the 11 September 2001 terrorist attacks. Infant and Child Development, 17, 557–580.
Hayes, A. F. (2013). Introduction to mediation, moderation, and conditional process analysis. New York, NY: Guilford Press.
Hayes, A. F., & Preacher, K. J. (2014). Statistical mediation analysis with a multicategorical independent variable. British Journal of Mathematical and Statistical Psychology, 67, 451–470.
Hayes, S. C., Luoma, J. B., Bond, F. W., Masuda, A., & Lillis, J. (2006). ACT: model, processes and outcomes. Behavior Research and Therapy, 44, 1–25.
Hayes, S. C., Strosal, K. D., & Wilson, K. G. (2003). Acceptance and commitment therapy: an experiential approach to behavior change. New York, NY: Guilford Press.
Katz, L. F., Wilson, B., & Gottman, J. M. (1999). Meta-emotion philosophy and family adjustment: Making an emotional connection. In M. J. Cox & J. Brooks-Gunn (Eds.), The advances in family research series. Conflict and cohesion in families: Causes and consequences (pp. 131–165). Mahwah, NJ: Lawrence Erlbaum.
Lovibond, P. E., & Lovibond, S. H. (1995). The structure of negative emotional states: comparison of the depression anxiety stress scales (DASS) with the beck depression and anxiety inventories. Behavior Research and Therapy, 33, 335–343.
Murrell, A. R., Wilson, K. G., LaBorde, C. T., Drake, C. E., & Rogers, L. J. (2008). Relational responding in parents. Behavior Analyst Today, 9(3−4), 196–214.
Ost, L.-G. (2008). Efficacy of the third wave of behavioral therapies: a systematic review and meta-analysis. Behavior Research and Therapy, 46, 296–321. https://doi.org/10.1016/j.brat.2007.12.005.
Palisano, R. (1997). Development & reliability of a system to classify gross motor function in children with cerebral palsy. Developmental Medicine Child Neurology, 39, 214–223.
Preacher, K. J., & Hayes, A. F. (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods, 40, 879–891.
Ruiz, F. J. (2010). A review of acceptance and commitment therapy (ACT) empirical evidence: Correlational, experimental psychopathology, component and outcome studies. International Journal of Psychology and Psychological Therapy, 10(1), 125–162.
Ruiz, F. J. (2012). ACT versus traditional cognitive behavioral therapy: a systematic review and meta-analysis of current empirical evidence. International Journal of Psychology and Psychological Therapy, 12(2), 333–357.
Sanders, M. R., & Dadds, M. R. (1993). Behavioral family intervention. Boston, MA: Allyn and Bacon.
Sanders, M. R., Mazzucchelli, T., & Studman, L. (2003). Practitioner’s manual for standard Stepping Stones Triple P. Brisbane, Australia: Triple P International.
Sanders, M. R., Mazzucchelli, T. G., & Studman, L. J. (2009). Facilitator’s Manual for Group Stepping Stones Triple P for families with a child who has a disability. Brisbane, Australia: Triple P International.
Tellegen, C. L., & Sanders, M. R. (2013). Stepping stones triple P–Positive Parenting Program for children with disability: a systematic review and meta-analysis. Research in Developmental Disabilities, 34, 1556–1571.
Whittingham, K., Sanders, M. R., McKinlay, L., & Boyd, R. N. (2013). Stepping stones triple P and acceptance and commitment therapy for parents of children with cerebral palsy: trial protocol. Brain Impairment, 14(2), 270–280.
Whittingham, K., Sanders, M., McKinlay, L., & Boyd, R. N. (2014). Interventions to reduce behavioral problems in children with cerebral palsy: an RCT. Pediatrics, 133, e1249–e1257.
Whittingham, K., Sanders, M., McKinlay, L., & Boyd, R. N. (2016). Parenting intervention combined with acceptance and commitment therapy: a trial with families of children with cerebral palsy. Journal of Pediatric Psychology, 41(5), 531–542.
Whittingham, K., Sofronoff, K., Sheffield, J. K., & Sanders, M. (2009). Stepping stones triple P: an RCT of a parenting program with parents of a child diagnosed with an autism spectrum disorder. Journal of Abnormal Child Psychology, 37(4), 469–480. https://doi.org/10.1007/s10802-008-9285-x.
Acknowledgements
This work was supported by a National Health and Medical Research Council postdoctoral fellowship (K.W., grant number 631712); a National Health and Medical Research Council Career Development Fellowship (R.B., grant number 1037220) and a Smart State Fellowship (R.B).
Author information
Authors and Affiliations
Contributions
K.W. designed and executed the study and led the data analysis and write up of the paper. M.R.S. and L.M. collaborated on the design and the write up of the study. R.B. collaborated on the design and the write up of the study, and provided mentorship throughout.
Corresponding author
Ethics declarations
Conflict of Interest
Stepping Stones Triple P is owned by The University of Queensland and sublicensed to Uniquest, The University of Queensland’s Technology Transfer Company. Professor Sanders is a co-author of the Stepping Stones Triple P program and receives royalty payments from the publisher Triple P International in accordance with The University of Queensland’s Intellectual Property Policy. Dr Whittingham and Dr Boyd are both employed by The University of Queensland.
Ethical Approval
Ethical clearance was obtained from the Children’s Health Queensland Human Research Ethics Committee (HREC/09/QRCH/125), the University of Queensland Behavioral and Social Sciences Ethical Review Committee (2009001871), and the Cerebral Palsy League of Queensland Research Ethics Committee (CPLQ-2010/11/1033). All participating parents provided written consent.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Whittingham, K., Sanders, M.R., McKinlay, L. et al. Parenting Intervention Combined with Acceptance and Commitment Therapy: Processes of Change. J Child Fam Stud 28, 1673–1680 (2019). https://doi.org/10.1007/s10826-019-01386-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-019-01386-9