
Abstract
Childhood physical abuse predicts emotional/behavioral, self-regulatory, and social problems. Yet factors from multiple ecological levels contribute to children’s adjustment. The purpose of this study was to examine the degree to which the social-emotional adjustment of physically abused children in first grade would be predicted by a set of child-, parent-, and family-level predictors in kindergarten. Drawing on a short-term longitudinal study of 92 physically abused children and their primary caregivers, the current study used linear regression to examine early childhood child (i.e., gender, IQ, child perceptions of maternal acceptance), parent (i.e., parental mental health), and family relationship (i.e., sensitive parenting, hostile parenting, family conflict) factors as predictors of first grade internalizing and externalizing symptomatology, emotion dysregulation, and negative peer interactions. We used a multi-method, multi-informant approach to measuring predictors and children’s adjustment. Internalizing symptomatology was significantly predicted by child IQ, parental mental health, and family conflict. Externalizing symptomatology and emotion dysregulation were predicted by child IQ. Although a large proportion of variance in measures of adjustment was accounted for by the set of predictors, few individual variables were unique predictors of child adjustment. Variability in the predictors of adjustment for physically abused children underscores the need for individualized treatment approaches.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Child physical abuse is a major public health concern, with significant implications for children’s well-being. Of 676,569 children who were victims of maltreatment in 2011, 17.6 % (118,825) were victims of physical abuse (US DHHS 2012). Moreover, young children are at increased risk of physical abuse, with 40.3 % of all physical abuse reports occurring in children under age six (US DHHS 2012). Though a small subset of maltreated children, physically abused children may be of particular importance to scientific and clinical study as some evidence suggests they have differing profiles when compared with children who were non-maltreated or who experienced other maltreatment subtypes. Physical abuse during early childhood predicts an array of deleterious outcomes over the life course, including emotional/behavioral problems and psychopathology (Egeland et al. 2002; Manly et al. 2001), self-regulatory problems (Maughan and Cicchetti 2002; Shipman et al. 2007), and social and peer relationship problems (Dodge et al. 1997; Klimes-Dougan and Kistner 1990). From a developmental perspective, experiencing abuse in early childhood may interfere with children’s capacity to manage stage-salient tasks, such as the transition to school, resulting in increased risk for adjustment difficulties (Manly et al. 2001; Veltman and Browne 2001). Because success in the early school years sets the stage for later development, it is important to identify the risk and protective factors for maltreated children in order promote long-term behavioral/emotional, regulatory, and relationship success. Factors from multiple levels of influence, such as child perceptions of maternal acceptance, parental mental health, and parental responsive caregiving, can contribute to positive outcomes.
This study is framed by two developmental models. First, we incorporate a developmental psychopathology perspective, which views development as a progression through a series of hierarchical, stage-salient tasks (Sroufe and Rutter 1984). The successful resolution of each task serves as the basis of functioning in the next phase. In this way, early experiences (such as positive or negative parent–child relationships) are carried forward in development. However, dynamic transactions between the child and compensatory influences in the environment allow for change and “righting” of the developmental course (Sroufe and Rutter 1984). From this perspective, examinations of deviations and abnormal development are as illuminating as those of normative processes. The experience of childhood maltreatment is a deviation from the normative, expected environment (Cicchetti and Lynch 1995). To deepen our understanding of social development, it is important to understand whether normative developmental processes also explain the social development of physically abused children.
Developmental psychopathology views disorder and adaptation in terms of assets and liabilities, or risk and protective factors, cumulated over time, in keeping with the ecological-transactional model (Bronfenbrenner 1977, 1994; Sameroff and Chandler 1975). In this model, the child or developing person is viewed as embedded within a nested set of ecological systems varying in their proximity to the child. These ecological systems include: the child (and her biological, regulatory, and psychological states; ontogenic development); immediate contexts in which the child interacts, such as family, peers, and school (microsystems); linkages and processes between these immediate settings (mesosystems); the larger social environment which indirectly influences the child’s immediate setting, such as the parental workplace or government agencies (exosystems), and the overarching cultural context (macrosystem). These ecological systems are thought to interact and transact over time with the child to influence the child’s developmental outcomes.
The current study focused on the influence of child factors (ontogenic development) as well as parent characteristics and family relationship factors (two domains within the microsystem; Furstenberg et al. 1999) on physically-abused children’s adjustment. These microsystem influences were included since, from an ecological and developmental perspective, individuals with whom very young children have significant dyadic relationships are likely to exert the most developmental influence (Cicchetti et al. 2000) and since preschool social networks typically include mothers and fathers, followed by other relatives (Appleyard et al. 2007; Cauce et al. 1990). The specific selected factors have been shown to be predictive of child adjustment in non-abused and abused populations. There are some gaps in the current literature and not all factors have been examined within physical abuse populations, per se. In the review below, we first present research with non-abused populations, followed by physically abused populations for comparison/contrast. When research on physical abuse specifically was not available, research on child maltreatment more broadly was used.
Children’s intelligence (IQ) is related to their behavioral and relationship functioning. Using a normative sample of 290 preschoolers, Andersson and Sommerfelt (2001) reported that, for girls, lower IQ was significantly associated with mothers’ reports of externalizing behavior, even after controlling for maternal education and parenting styles. Similarly, Goodman (1995) found that, even within normal ranges of IQ, lower mean IQ was associated with youth conduct problems, above and beyond the effects of socioeconomic status and not mediated by academic achievement. Among the NSCAW sample of maltreated children, maltreated children were found to obtain lower scores on measures of intellectual functioning (IQ and achievement) compared to non-maltreated children (Crozier and Barth 2005). Moreover, using the same sample, Jaffee and Maikovich-Fong (2011) found that chronic (vs. situational) maltreatment was associated with both lower IQ and higher behavioral problems, although they did not test associations between IQ and behavior problems. A cross-sectional study examining clusters of academic, behavioral, and peer functioning in school among sexually-abused girls found that a significant proportion (22 %) of sexually-abused girls had simultaneous academic, behavioral, and peer problems (Daignault and Hebert 2009). Since longitudinal outcomes with physically abused children are not yet well understood, the current study will further this area of research by examining short-term longitudinal relations among IQ and later emotional, behavioral, and peer outcomes within a sample of physically abused children.
Beginning in early childhood, children’s gender is a significant predictor of behavioral/emotional, regulatory, and relationship functioning (Deater-Deckard et al. 1998; Dodge et al. 2006). A recent meta-analysis of 148 studies of children and adolescents reported significantly higher direct aggression for males, which in turn was associated with higher externalizing behavior, poor peer relations, and lower prosocial behavior (Card et al. 2008). Findings from the National Longitudinal Study of Youth demonstrate that girls exhibited higher self-regulation skills than boys from preschool to adolescence (Raffaelli et al. 2005). Among children with abuse histories, oppositional and aggressive behavior is well documented, particularly for males, and for physical abuse specifically (Lansford et al. 2002; Staudt 2001; Vandenberg and Marsh 2009). It is expected within the current study that physically abused males will have significantly more maladaptive emotional/behavioral, self-regulatory, and social outcomes.
The parental acceptance-rejection continuum has significant influence on child outcomes. Parental acceptance (i.e., the warmth dimension of parenting) is associated with a wide variety of positive outcomes, such as psychological well-being, prosocial behaviors, and positive peer relationships, whereas rejection is associated with depression and internalizing problems, acting out behavior and externalizing problems, and peer relationship difficulties (Rohner and Britner 2002). Maternal acceptance is a significant element of preschool children’s self-perceptions (Harter and Pike 1984) and is associated with young children’s attachment quality (Cassidy 1988). Available studies demonstrate no significant differences in perceived maternal acceptance between maltreated and non-maltreated children (Barnett et al. 1996; Vondra et al. 1990). Examination of the influence of maternal acceptance on physically abused children, specifically, is lacking, though it is expected to be relevant to children’s adjustment.
Although there are several parent-level factors that could have been selected as potential predictors of child adjustment, we selected overall mental health functioning because of the significant literature on links between maternal poor mental health (e.g., high parenting stress, elevated depression) and child maladjustment, including behavior problems, emotion regulation problems, and psychopathology (e.g., Bennett et al. 2012; Vidair et al. 2011). Sexually abused children with depressed mothers have higher behavioral and emotional adjustment problems (Kelly et al. 2002). Although little prior evidence is available for physically abused children, it is hypothesized that similar patterns will emerge in this study.
Parental sensitivity is generally associated with positive child adjustment, even among high-risk and maltreated samples. A longitudinal study of high-risk children found that emotionally responsive caregiving can ameliorate the effects of early adversity such as maltreatment (Egeland et al. 1993). In a cross-sectional study, maltreated children who reported more positive interactions with their mothers (i.e., secure relatedness) were less likely to demonstrate emotion regulation difficulties, which in turn were associated with fewer emotional and behavioral problems (Alink et al. 2009). Relationships among physically abusive families are often presumed to be globally negative. Yet, one cross-sectional study of physically abusive parents demonstrated substantial variation among abusive parents with regard to their warmth and sensitivity and that abused children who experienced such warmth and aggression showed better adaptation (less aggression, more positive social relationships) (Haskett et al. 2008). This study seeks to confirm these findings in a longitudinal sample of physically abused children.
Hostile parenting and harsh discipline are closely linked to elevated conduct problems and externalizing problems among children and adolescents (Ge et al. 1996; Nix et al. 1993). Longitudinal evidence following children from preschool to school entry suggests that children (particularly boys) with both early externalizing problems and hostile parenting in early childhood are more likely to show continued behavioral problems at the transition to school (Campbell et al. 2000). Although less evidence is available for longitudinal samples of physically abused children, as noted above, variations in parental behaviors even among abusive families have been documented, and it is predicted that among abused children, hostile parenting will predict more problematic child adjustment outcomes.
Family conflict in the home can also contribute to children’s developmental outcomes. Feldman et al. (2010) reported that conflictual relationships (i.e., observed parent–child conflict and marital conflict) predicted behavior problems among young children. A recent review of the literature indicated the significance of family and parental conflict in the development of delinquency and conduct disorder (Murray and Farrington 2012). Moreover, the combination of family conflict (especially intimate partner violence) and child abuse has consistently demonstrated maladaptive outcomes for children (McDonald et al. 2009). As such, for abused children, family conflict may increase the risk for maladaptive outcomes.
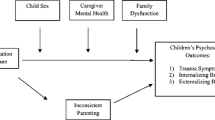
The current study is based on an investigation of 92 physically abused children and their primary caregivers followed from preschool through first grade. The study examines kindergarten assessments of child (i.e., gender, IQ, and maternal acceptance), parent (i.e., parent mental health), and family relationship (i.e., parental sensitivity, parental hostility, and family conflict) factors as predictors of emotional/behavioral (i.e., teacher-reported internalizing and externalizing symptoms), self-regulatory (i.e., teacher-reported emotion dysregulation), and social (i.e., observations of negative peer interactions) outcomes in first grade. This study is novel due to its inclusion of several levels of influence in the same study, with relevant data from multiple reporters and multiple measurement approaches (self-report, observation), over this critical time period. Additionally, this study includes a significant sample size of physically abused children, specifically. This study will help to illuminate developmental processes for children who have experienced harsh/abusive discipline in particular.
Method
Participants
Participants included 92 children (n = 57 or 62 % boys) and one of their parents or parent figures (n = 88 or 95 % mothers) enrolled in a short-term longitudinal study of abused children (Haskett et al. 2014). All children had an early childhood history of substantiated physical abuse or neglect involving inappropriate discipline (defined by North Carolina Statutes) within the year prior to study enrollment. In NC, cases of neglect involving inappropriate discipline include physical discipline resulting in injuries not considered “serious”; we included those cases because they would be designated as physical abuse in other states. Since access to detailed CPS records was not available (see procedures, below), dimensions of maltreatment experiences (e.g., other subtypes, chronicity/re-reports, severity, services received) are unknown. It is presumed that severity of abuse was likely in the mild to moderate range and multiple subtypes may have been limited since foster placement and experience of sexual abuse were exclusionary criteria. With three exceptions, the parent who maltreated the child participated in this study.
Preschool, kindergarten, and first grade children and their parents were recruited for participation in the larger longitudinal study. Yearly follow-up assessments were conducted for the preschool and kindergarten children through their first grade year. Retention over time was acceptable. Specifically, the majority of children (n = 56; 61 %) enrolled in the study in the spring prior to entering kindergarten and 79 % of those children were available for data collection in kindergarten and first grade. A total of 25 (27 %) children entered the study during the kindergarten year and approximately 70 % of those children were available for data collection in first grade. A total of 11 children (12 %) entered the study in first grade. For purposes of this particular investigation, data collected in kindergarten and first grade were included.
The majority (71.7 %) of participants were African American; 20.7 % were European American, and 7.6 % were Latino or biracial. Mean child age was 5.43 (SD = .50) at kindergarten and 6.13 (SD = .43) at first grade. Children were primarily from economically disadvantaged families: the mean of Hollingshead’s (1975) index of socioeconomic status was 3.69 (SD = 1.09) at kindergarten and 3.57 (SD = 1.08) at first grade. The mean age of parents was 33.03 (SD = 9.26) at kindergarten. About 25 % of parents were married at each time point.
Procedure
Due to university IRB restrictions, the researchers did not have access to Child Protective Services records for recruitment or for assessment of maltreatment experiences. Instead, a Child Protective Services social worker mailed recruitment letters that explained the project to eligible parents; those who were interested in participating voluntarily called the project office to enroll. Criteria for inclusion were a substantiated report of physical abuse or neglect involving inappropriate discipline and child age between 4 and 6 years. Exclusionary criteria included history of sexual abuse, non-proficient English language skills, and placement in foster care. Parents and children completed all assessment activities in a lab setting. Prior to data collection, parents gave informed consent and children gave assent for participation. Parents received a financial incentive to participate ($80 and $90 for kindergarten and first grade assessments, respectively). At each time point, teacher-report data and playground observations were collected at the school within 1 month of parent and child data collection. Teachers received compensation of $15. All procedures were approved by the university institutional review board.
Measures
The predictor (child, parent, family variables) and outcome (child adjustment) measures were assessed via multiple reporters and using a variety of approaches, as described below.
Measures of Predictors: Administered in Kindergarten
Child IQ
Children’s intellectual functioning was assessed in kindergarten using the Vocabulary and Matrices subtests of the Kaufman Brief Intelligence Test (KBIT; Kaufman and Kaufman 1990). Test–retest reliability (21 days) exceeds .90. Internal consistency as reported by the test developers is excellent, ranging from .88 to .98. Validity has been established with other measures of IQ and measures of academic achievement (Kaufman and Kaufman 1990). IQ scores were available for 90 children.
Maternal Acceptance
The 6-item Maternal Acceptance subscale of the Pictorial Scale of Perceived Competence and Social Acceptance (Harter and Pike 1984) was used to measure children’s self-perception of maternal acceptance in kindergarten. For each item, the participant was read a brief statement about a picture of two children depicting opposites (e.g., this child’s mom talks to him/her vs. does not talk to him/her; smiles at him/her vs. does not smile at him/her; plays with him/her vs. does not play with him/her). Participants were asked to point to the child that is most like them and then asked whether the picture is “a lot” like them or “a little” like them. Each item is scored one (less competent/less accepted) to four (more competent/more accepted) and subscale scores are generated by averaging item scores. Psychometric properties of the Pictorial Scale and the Maternal Acceptance subscale (α = .76 as reported by the test developer) are sound (Harter and Pike 1984) and supported by prior research (e.g., Mantzicopoulos et al. 2004). Maternal acceptance scores were available for 66 children.
Parental Mental Health
The Brief Symptom Index (BSI; Derogatis 1993) was administered at the kindergarten time point to measure parents’ symptoms of psychopathology. Parents are presented with a list of 53 “problems that people sometimes have” and are asked to indicate on a 4-point scale (0 = not at all; 4 = extremely) how much that problem distressed them within the last 7 days. Raw scores are converted to T-scores. For purposes of this study, T-scores for the Global Severity Index (GSI) were used. Test developers report good internal consistency (α = .85) and two-week test–retest reliability (r = .84) for the GSI. Strong validity of the BSI has been established (e.g., Hoe and Brekke 2008). Scores on the GSI were available for parents of 68 children.
Sensitive Parenting
In kindergarten, each parent–child dyad participated in a 24-minute play session divided into three situations (i.e., “free play” with a standard set of age-appropriate toys, an “instructions” task in which parents were told to ask their child to follow three directions, and a “teaching/frustration” segment in which the parent helped the child complete two puzzles while a timer ticked loudly). Parenting behavior was coded from videotapes by trained students blind to study hypotheses using a version of the Qualitative Ratings of Parent–Child Interactions (Paley et al. 2000). Seven-point parenting scales included Sensitivity, Positive Regard, Negative Regard, Intrusiveness, and Flat Affect. Scoring was completed separately for the three situations and mean scores across the three situations were generated. For purposes of this study, mean scores for Sensitivity were used. Indicators of Sensitivity included responsiveness to the child’s cues and balancing the child’s need for assistance with the child’s desire for autonomy. The inter-rater reliability coefficient for Sensitivity was ICC = .85 (based on a second coder for approximately 25 % of the dyads). Sensitivity scores were available for parents of 68 children.
Hostile Parenting
Self-report of parenting was assessed in kindergarten using the Preschool Parenting Measure (PPM; Sessa et al. 2001). Parents indicated the degree to which each item represented their relationship with their child, using a 4-point rating. Scales include Positive Affect, Responsiveness, Hostility, and Structure. The 5-item Hostility scale (e.g., “I snap at my child when he/she gets on my nerves”) was used in this study. Because this measure is relatively new, we examined internal consistency of the Hostility scale for our sample and it was acceptable (α = .77). According to the test developer, factor analyses support the four-factor structure of the measure and correlations among the scales confirm the dimensions are distinct (Sessa et al., 2001). Scores have been validated with measures of associated constructs (Sessa et al. 2001). Hostility scores were available for parents of 68 children.
Family Conflict
At the kindergarten assessment, children’s narratives about family relationships were elicited using five story stems from the MacArthur Story Stem Battery (Bretherton et al. 1990) that had been used in prior research with maltreated children (Toth et al. 2000). The story stems portray emotionally-laden family interactions (e.g., child injury, oppositionality, parental conflict) and are presented using dolls and props. At the conclusion of each story stem, the child was asked to “show me and tell me what happens now.” Audio and videotaped narratives were coded by trained students who were blind to study hypotheses following the MacArthur Narrative Coding Manual (Robinson et al. 1992). Procedures of Toth et al. (2000) were used to generate composite scores for children’s conflictual and moral-affiliative themes. In this study, the conflictual themes score was used to assess family relationship quality by the frequency of conflict and working models around family interactions that included conflictual themes (e.g., aggression, verbal disagreements). Inter-rater agreement based on a second coder for 25 % of the participants was r = .87 for conflictual themes. Narrative stories data were available for 64 children.
Measures of Child Adjustment: Administered in First Grade
Emotional/Behavioral Problems
The Child Behavior Checklist—Teacher Report Form (TRF; Achenbach and Rescorla 2001) is a 118-item teacher-report of children’s adjustment. In first grade, teachers rated how true each item was for the child over the past 6 months on a scale of zero (not true) to two (very or often true). For this study, we used TRF scores for the two broadband scales of child psychopathology: Internalizing symptomatology and Externalizing symptomatology. Reliability and validity of the TRF has been supported by over 40 years of research (see Achenbach and Rescorla 2001). TRF scores were available for 54 children.
Emotion Dysregulation
The Behavior Rating Inventory of Executive Functioning (BRIEF; Gioia et al. 2000) is a teacher-report measure used to assess children’s emotion regulation and executive functioning. In first grade, teachers indicated, on a 3-point scale (1 = never, 2 = sometimes, 3 = often), how frequently the child had problems with 86 behaviors in the past 6 months. Items are grouped into clinical scales and global indices. T-scores are generated by age and gender, with higher scores indicating worse functioning. For this study, the 9-item Emotional Control subscale (e.g., has explosive, angry outbursts, becomes upset too easily) was used as a measure of emotion regulation. Internal consistency of the scale for this sample was .95. Test developers report that scores are stable over time and there is evidence for convergent and discriminate validity (Gioia et al. 2000). Data on the BRIEF were available for 56 children.
Negative Interactions with Peers
Live observations by trained observers on the child’s playground were conducted in first grade using an interval coding system. For 30 minutes, coders recorded whether the child engaged in four target behaviors (engaged social behavior, negative behavior, rough play, and aggression) within each 15-second interval. The variable generated for use in this study was the percent of intervals in which negative behavior, rough play, or aggression occurred. Coders were trained to 90 % agreement with the primary coder. Inter-rater agreement (assessed for approximately 25 % of the observations with a second live coder) was κ = .97 for the variable used in this study. Observation data were available for 59 children.
Multiple Imputation of Missing Data
It should be noted that there are some missing data due to non-response at one or more time periods. The extent of missing data for study variables is reported following the description of each measure, above. There were no significant differences between participants with full data and those with missing data in either demographic characteristics (i.e., race, parent gender, child gender, SES) or study variables. Of the 92 participants in the study, 35 had complete records on all study variables. Discarding participants with any missing values would have yielded a much smaller sample, with a high risk for parameter bias, inflation of variance, and reduced power (Schafer 1997). Examination of the 57 records containing missing values indicated that missingness stemmed largely from non-response during entire waves of data collection at one or more time points in the study: 15 non-responses at first grade; nine at kindergarten; and 11 missing at both time points. These 11 participants were included because two analysis variables and some of the auxiliary imputation variables were observed for these 11, indicating that imputed values were likely to be stable for analysis. In addition, there were scattered non-responses (i.e., participants’ non-responses to single items within a data collection period) at kindergarten and first grade as a result of participants’ selective non-response to certain items (n = 22). A test to determine whether these missing values were missing completely at random (MCAR) indicated that the null hypothesis of no relationship was rejected (χ2 = 191.57; p < 0.01), suggesting that bias would result from deletion (Little 1988).
An imputation model was constructed including all independent and dependent variables, as well as seven additional “auxiliary” variables that had the potential to help explain the missing values (Schafer 1997). The auxiliary variables used in the imputation included: first grade maternal acceptance, first grade parental mental health (Global Severity Index from the BSI), first grade children’s representations (conflictual and moral-affiliative themes from the narrative story stems), family race, parent gender, and Hollingshead rating for SES. The concept behind auxiliary variables in multiple imputation is that there are two models in every scenario in which missing data are present (Graham 2009): the analysis model (which is being tested) that expresses the relationships between the predictors and the outcome, and a missing data model that causes the missing values in any variables in the analysis model. The missing data model is unknown, but it is likely that there are variables in the missing data model that are not included in the analysis model. An imputation model with no auxiliary variables implies an assumption that the analysis and missing data models are equivalent. If this assumption is not true, then the ability of multiple imputation to reduce bias is challenged. By including auxiliary variables, we acknowledge that additional information beyond the variables in the analysis model is needed. Given the limits on sample size, a very rigorous approach was used to select the auxiliary variables for this study with the potential for the highest impact to reduce bias.
Because the actual missing data generation process was not known, multiple imputation cannot be assumed to completely eliminate bias, but a robust imputation model has the potential to reduce bias to a negligible level, regardless of whether the missing values occurred in kindergarten or first grade (Graham 2009). Because of the high proportion of participants with missing values, the data were imputed 15 times, generating 15 separate versions of the data (Graham et al. 2007). The analysis model was then run on each of these 15 versions, with the parameter estimates from each version combined according to rules that average the parameter estimates and inflate the standard errors to reflect the uncertainty of the imputed values (Graham 2009). This inflation in standard errors is reflected in lower t tests and greater likelihood of type I errors relative to models run on data without missing values. SAS Proc MI was used to conduct the imputation and Proc MIAnalyze was used to combine the 15 sets of parameter estimates (SAS Institute 2002–2004). In an imputed analysis, the sample size used in the analysis is the within-imputation sample size, which in this case was 92.
Results
Descriptives of and Correlations among Imputed Variables
Prior to testing study hypotheses using the imputed data, descriptive statistics were generated to determine the average sample characteristics in terms of the child and family factors of interest and a correlation matrix examined interrelations among the study variables. Table 1 provides a summary of these preliminary analyses. We tested for multicollinearity among the variables and the VIF and Tolerance values provided no indication of collinearity. All predictors were included for analysis in the subsequent regression models because of their theoretical importance and documented relations in prior research.
Kindergarten Factors Predicting First Grade Outcomes
In order to determine which child and family factors in kindergarten predicted first grade outcomes, a series of linear regression models was conducted using the imputed data described previously. Four individual linear regression models were performed to examine each first grade outcome measure in question, including internalizing and externalizing symptomatology, emotion dysregulation, and negative interactions with peers. For each linear regression model, child gender and IQ served as predictor variables along with kindergarten measures of maternal acceptance, parental mental health, sensitive parenting, hostile parenting, and family conflict. See Tables 2, 3, 4 and 5 for the regression results of each model.
In regards to the kindergarten child and family factors predicting first grade internalizing behavior problems, three significant results and one trend toward significance were found (Table 2). First, child IQ significantly predicted first grade internalizing symptomatology, such that lower IQs predicted higher levels of teacher-reported internalizing symptomatology. Second, parental mental health at kindergarten significantly predicted first grade internalizing symptomatology. Specifically, lower levels of parental mental health problems were (unexpectedly) associated with higher levels of internalizing symptomatology. Third, family conflict in kindergarten significantly predicted internalizing symptomatology in first grade, indicating that higher levels of family conflict predicted higher levels of internalizing symptomatology. Child perceptions of maternal acceptance were associated with internalizing at the trend level, with higher maternal acceptance being associated with lower internalizing symptomatology.
The regression model examining kindergarten child and family factors predicting first grade externalizing symptomatology resulted in one significant finding (Table 3). Specifically, child IQ significantly predicted first grade externalizing symptomatology, such that lower IQs predicted higher levels of teacher-reported externalizing symptomatology. Similarly, the regression model of kindergarten child and family factors predicting first grade emotion dysregulation resulted in one significant finding and two findings at the trend level (Table 4). Child IQ significantly predicted first grade emotion dysregulation, indicating that lower IQs predicted higher levels of teacher-reported emotion dysregulation. Sensitive parenting and hostile parenting demonstrated associations at the trend level, such that lower sensitive parenting and lower hostile parenting were associated with higher emotion dysregulation. Finally, the regression model of kindergarten child and family factors predicting first grade negative interactions with peers (Table 5) did not produce any significant findings, although maternal acceptance and sensitive parenting demonstrated associations at the trend level, such that higher maternal acceptance and higher sensitive parenting were associated with more observed negative interactions with peers.
Discussion
Drawing on a short-term longitudinal study of 92 physically-abused children and their primary caregivers, the current study used linear regression to examine early childhood child (i.e., gender, IQ, child perceptions of maternal acceptance), parent (i.e., parental mental health), and family relationship (i.e., sensitive parenting, hostile parenting, family conflict) factors as predictors of first grade internalizing and externalizing symptomatology, emotion dysregulation, and negative peer interactions. Strengths of study include its examination of differing ecological levels of influence as well as multiple areas of functioning assessed over time among a sample of physically-abused children during the transition to school, a critical developmental period. Additionally, multiple assessment approaches and multiple reporters were used. Our models captured a high proportion of variance in children’s first grade adjustment (ranging from 34 to 44 %), in spite of the fact that few individual predictors were significant as unique predictors.
With regard to internalizing symptomatology, even after accounting for child and parent factors, family relationship factors (specifically, family conflict) predicted internalizing symptoms in first grade. Whereas much of the previous research with young children has outlined effects of family-level factors on behavior problems such as delinquency and conduct problems (Feldman et al. 2010), the current study underscores adjustment difficulties along the internalizing dimension for young abused children. It is possible that conflict within the home of abused children leads to rumination on and worries about family stability at this time of change and transition to school. Regarding parent factors, however, the results did not support prior literature regarding the role of maternal mental health functioning predicting child internalizing symptoms in both non-abused (e.g., Goodman and Gotlib 2002) and sexually abused children (Kelly et al. 2002). Among this sample of physically abused children, maternal mental health problems unexpectedly were associated with lower levels of child internalizing difficulties. These findings may suggest different responses among physically abused children than non-abused and sexually abused children. It is possible that physically abused children of mothers with high levels of distress actually hide their own internal distress, perhaps particularly when conflict in the home is present. Thus, they may not express or exhibit their internalizing states in the classroom, perhaps in a subconscious effort to protect their mothers. Further examinations with similar populations are needed to validate these findings.
Children’s IQ accounted for a significant portion of variance of emotional, behavioral, and self-regulation outcomes. Specifically, children with higher IQ in kindergarten had lower internalizing symptoms, externalizing symptoms, and emotion dysregulation in first grade according to their teachers. Although it is possible that these associations represent a halo effect such that teachers were rating cognitively brighter children more positively across multiple domains, these findings seem consistent with extant literature, underscoring the possibility of a relevant issue for maltreated children. Associations between IQ and social and behavioral adaptation have been found previously in general populations (Andersson and Sommerfelt 2001; Goodman 1995). Among maltreated samples, several studies have demonstrated that maltreated children are more likely to have lower IQ and school achievement (Crozier and Barth 2005; Jaffee and Maikovich-Fong 2011; Perez and Widom 1994), as well as co-occurring academic, behavioral, and peer problems (Daignault and Hebert 2009; Jaffee and Maikovich-Fong 2011). Maltreatment may influence a variety of factors (e.g., chronic stress that impacts brain development; poor language and social stimulation between parent and child that limits child cognitive development; see Jaffee and Maikovich-Fong 2011) resulting in lower child cognitive functioning. Our findings suggest that impaired cognitive functioning among maltreated children (in kindergarten), in turn, may impede children’s later capacity to manage stress and regulate their emotions (in first grade). Yet, the current study also suggests a protective role that IQ can play in maltreated children’s adjustment, such that those with higher IQ had fewer internalizing and externalizing symptoms as well as less emotion dysregulation a year later. Future examinations regarding the direction of effects in these associations could illuminate potential pathways for intervention.
None of the child, parent, or family factors examined in this study significantly predicted peer interactions in the school setting. It is possible that these brief, one-time observations on the playground did not represent the child’s global “peer relationships” very well. This possibility is supported by the fact that the playground observations were not related to TRF scores (internalizing and externalizing). In other analyses with this sample, playground observations of aggression, specifically, relates to TRF Aggression scores (at the same time point). Thus, the observations may be capturing a very specific behavior fairly well, though not a broader construct of negative peer relationships. Future research with multiple observations of a wider variety of behaviors might more accurately capture this construct, which in turn could relate to predictors in a variety of contexts.
We initially were perplexed that aspects of parenting did not significantly predict externalizing problems, emotion dysregulation, or behavior with peers (and sometimes indicated unexpected directions of effects at the trend level) given a substantial literature to support our hypotheses. However, we recently identified a high level of instability in parenting observations over time for the current sample; in particular, there are linear declines in sensitivity over the three-year period of the larger study (Haskett et al. 2014). Given this instability, it is not surprising that sensitivity in the child’s kindergarten year did not predict the child’s adjustment in first grade. To illustrate, it might be expected that a child who experienced relatively high sensitivity in kindergarten would fare well in first grade; if, however, the parents’ sensitivity decreased over the course of the next year, the child might respond to that decline with an increase in behavior problems and poor regulation of emotions. In that case, sensitivity in kindergarten would be unrelated to child behavior in first grade. Future research examining changes in risk and protective factors over time might provide a more nuanced understanding of the role of parenting in abused children’s adjustment. Moreover, because of the nature of our sample (all abusive parents, representing an extreme form of parenting), it is also possible that there is a restricted range of parenting. Although we do not have clear evidence of restriction in range on parenting variables, to the extent that it exists, it could account, at least in part, for the failure to find expected links between parenting and child adjustment.
Implications
Our findings should be interpreted with some degree of caution pending replication; however, there are a few clinical implications of these results. Children’s cognitive functioning was especially relevant to the prediction of later externalizing problems such as aggression, noncompliance, and disruptive behavior at school. This domain of functioning has received relatively little attention in prior research but could have important implications for treatment efforts. Although child IQ, per se, may not be a malleable intervention target, preschool programs or early childhood home visitation programs that target children’s language, communication, and nonverbal problem solving skills could minimize physically abused children’s behavior problems and thereby improve their chances of school success. For example, evidence from intervention studies with low-income, high-risk children has demonstrated significant effects on school readiness at age five (Early Head Start; Love et al. 2013) and intellectual development and academic achievement through adolescence (Abecedarian Project; Campbell et al. 1998). Additionally, the findings highlight the importance of considering the role of family conflict in possibly reducing the risk of internalizing disorders among abused children. The need for individualized treatment approaches targeting salient protective processes was highlighted by our findings. For example, multi-modal, family interventions to address family conflict (in addition to child therapy alone) may make additional contributions to ameliorating physically abused children’s internalizing symptomatology. Current evidence-based models designed for physically abused youth that incorporate individual and conjoint sessions, such as Alternatives for Families: A Cognitive-Behavioral Therapy, would be useful in addressing these issues (Kolko 1996).
Limitations and Future Directions
Some limitations of this study point to possible directions for future research. First, our sample was primarily African American families of lower SES, and primarily mothers, which could hinder the capacity to generalize findings beyond this population. The sizable majority of African American children within this sample is not unexpected, as there is some evidence that African American children tend to be overrepresented in child welfare caseloads (e.g., Fluke et al. 2003), as well as within the child welfare population in the study county. Yet most prior research on links between risk factors and child adjustment has been conducted with samples comprised largely of European American families. It is possible that some of the differences in our findings from past research (e.g., lack of significant associations or unexpected directions for maternal acceptance, sensitive and hostile parenting) could be related to ethnicity or income. For example, these constructs might relate differently among lower-income African American physically abused samples such as ours; alternatively, there might be other, unexplored, more relevant variables for understanding adjustment of young physically abused African American children (e.g., racial socialization). The possible influence of ethnicity on links between risk factors and child adjustment should be pursued in future studies with more representative samples of children who have experienced physical abuse.
Our study was limited to specific ecological factors. Given that the models explained a significant proportion, but not all the variance in the outcomes, other relevant child, parent, family factors deserve future examination. For example, the influence of children’s personal understanding of the discipline and abuse they have experienced should be examined in future investigations. The effects of additional levels of influence (such as interventions or family support services delivered to the families) may also be relevant to children’s outcomes. Moreover, our study looked solely at the main effects of these ecological factors. The ecological-transactional model holds that the levels of influence interact and transact with each other to influence development (Sameroff and Chandler 1975); further, risks tend to co-occur, with cumulative risks more predictive of outcomes than single risk factors (Sameroff 2000). Future studies with larger samples should explore the influence of interactions among risks and effects of cumulative risk. As noted above, many ecological factors may change over time, suggesting the need for examination of child outcome in the context of these changing risk and protective factors. Thus, although the current study provides a first step in understanding the ecological contributors to physically abused children’s development, future examinations of interactions among predictors and changes in predictors (e.g., parental sensitivity) over time are warranted to more fully explicate this developmental model.
Additionally, our study focused on a sample of physically abused children, and IRB restrictions related to access to CPS records did not allow for the assessment of additional dimensions of maltreatment (e.g., co-occurring subtypes of maltreatment, severity, chronicity). Although the current study reveals important and heretofore relatively unexplored findings related to physically abused children, additional dimensions of their maltreatment experiences warrant investigation. For example, using a large longitudinal study of maltreated children, English et al. (2005) found that maltreatment subtype in combination with chronicity and severity best predicted socialization outcomes whereas subtypes combined with age at maltreatment onset best predicted externalizing outcomes and adaptive functioning. Moreover, understanding the interplay between subtypes is also imperative. Herrenkohl and Herrenkohl (2009) reported that children often experience multiple forms of maltreatment simultaneously; however, the frequency of these co-occurrences is difficult to establish due to varying research methodologies and data sources. When the results of various studies of co-occurring subtypes of maltreatment are taken together, it has been estimated that 33–94 % of maltreated children experience multiple forms of maltreatment. Given this high rate of co-occurrence, research considering the effects of multiple maltreatment experiences is also needed (Herrenkohl and Herrenkohl 2009). For example, recent study of preschool children in the foster care system (Pears et al. 2008) used latent profile analysis to identity naturally occurring subgroups or profiles of maltreatment based on the various subtypes and found differential adjustment outcomes (internalizing, externalizing, cognitive functioning) based on profile membership. Future studies with greater specificity in the dimensions and profiles of maltreatment could further elucidate patterns of development.
Finally, our sample focused on children’s adjustment at the transition to school. Because developmental contexts and the influence of ecological factors vary across time, there is a need for examination of processes with older children experiencing later developmental transitions such as emerging adulthood, when instability in the parent-teen relationship can lead to tension as adolescents mature into independent adults (Arnett 2000).
Summary
The current study examined a variety of ecological factors predicting emotional/behavioral, self-regulatory, and social problems among physically-abused children. Findings revealed variability in the influence of various factors depending on the outcome of interest, suggesting the need for individualized approaches to treating abused children as they transition to school. Continued examination of a variety of risk and protective factors, and their interplay across time, will further explicate the pathways to adaptation for physically abused children.
References
Achenbach, T. M., & Rescorla, L. A. (2001). Manual for the ASEBA school-age forms and profiles. Burlington: University of Vermont, Research Center for Children, Youth, and Families.
Alink, L. R. A., Cicchetti, D., Kim, J., & Rogosch, F. A. (2009). Mediating and moderating processes in the relation between maltreatment and psychopathology: Mother-child relationship quality and emotion regulation. Journal of Abnormal Child Psychology, 37, 831–843.
Andersson, H. W., & Sommerfelt, K. (2001). The relationship between cognitive abilities and maternal ratings of externalizing disorders in preschool children. Scandinavian Journal of Psychology, 42, 437–444.
Appleyard, K., Egeland, B., & Sroufe, L. A. (2007). Direct social support for young, high-risk children: Relations with behavioral and emotional outcomes across time. Journal of Abnormal Child Psychology, 35, 443–457.
Arnett, J. J. (2000). Emerging adulthood: A theory of development from the late teens through the twenties. American Psychologist, 55, 469–480.
Barnett, D., Vondra, J. I., & Shonk, S. M. (1996). Self-perceptions, motivation, and school functioning of low-income maltreated and comparison children. Child Abuse and Neglect, 20, 397–410.
Bennett, A. C., Brewer, K. C., & Rankin, K. M. (2012). The association of child mental health conditions and parent mental health status among US children, 2007. Maternal and Child Health Journal, 16, 1266–1275.
Bretherton, I., Ridgeway, D., & Cassidy, J. (1990). Assessing internal working models of the attachment relationship: An attachment story completion task for 3-year-olds. In M. Greenberg, D. Cicchetti, & E. M. Cummings (Eds.), Attachment in the pre-school years (pp. 273–308). Chicago: University of Chicago Press.
Bronfenbrenner, U. (1977). Toward an experimental ecology of human development. American Psychologist, 32(7), 513–531.
Bronfenbrenner, U. (1994). Ecological models of human development. In International Encyclopedia of Education, vol. 3 (2nd ed.) (pp. 1643–1647). Oxford: Elsevier Sciences, Ltd.
Campbell, F. A., Helms, R., Sparling, J. J., & Ramey, C. T. (1998). Early-childhood programs and success in school: The Abecedarian study. In W. S. Barnett & S. S. Boocock (Eds.), Early care and education for children in poverty: Promises, programs, and long-term results. SUNY series, youth social services, schooling, and public policy/SUNY series, early childhood education: Inquiries and insights (pp. 145–166). Albany, NY: State University of New York Press.
Campbell, S. B., Shaw, D. S., & Gilliom, M. (2000). Early externalizing behavior problems: Toddlers and preschoolers at risk for later maladjustment. Development and Psychopathology, 12, 467–488.
Card, N. A., Stucky, B. D., Sawalani, G. M., & Little, T. D. (2008). Direct and indirect aggression during childhood and adolescence: A meta-analytic review of gender differences, intercorrelations, and relations to maltreatment. Child Development, 79, 1129–1185.
Cassidy, J. (1988). Child-mother attachment and the self in six-year-olds. Child Development, 59, 121–134.
Cauce, A. M., Reid, M., Landesman, S., & Gonzalez, N. (1990). Social support in young children: Measurement, structure, and behavioral impact. In B. R. Sarason, I. G. Sarason, & G. R. Pierce (Eds.), Social support: An interactional view (pp. 64–94). New York: John Wiley and Sons.
Cicchetti, D., & Lynch, M. (1995). Failures in the expectable environment and their impact on individual development: The case of child maltreatment. In D. Cicchetti & D. J. Cohen (Eds.), Developmental psychopathology vol. 2: Risk, disorder, and adaptation (pp. 32–71). NY: John Wiley and Sons.
Cicchetti, D., Toth, S. L., & Maughan, A. (2000). An ecological transactional model of child maltreatment. In A. J. Sameroff, M. Lewis, & S. M. Miller (Eds.), Handbook of developmental psychopathology (2nd ed., pp. 689–722). New York: Kluwer Academic/Plenum Publishers.
Crozier, J. C., & Barth, R. P. (2005). Cognitive and academic functioning in maltreated children. Children and Schools, 27, 197–206.
Daignault, I. V., & Hebert, M. (2009). Profiles of school adaptation: Social, behavioral, and academic functioning in sexually abused girls. Child Abuse and Neglect, 33, 102–115.
Deater-Deckard, K., Dodge, K. A., Bates, J. E., & Pettit, G. S. (1998). Multiple risk factors in the development of externalizing behavior problems: Group and individual differences. Development and Psychopathology, 10, 469–493.
Derogatis, L. R. (1993). BSI brief symptom inventory. Minneapolis, MN: National Computer Systems Inc.
Dodge, K. A., Pettit, G. S., & Bates, J. E. (1997). How the experience of early physical abuse leads children to become chronically aggressive. In D. Cicchetti & S. L. Toth (Eds.), Developmental perspectives on trauma: Theory, research, and intervention. Rochester symposium on developmental psychology (Vol. 8, pp. 263–288). Rochester, NY: University of Rochester Press.
Dodge, K. A., Coie, J. D., & Lynam, D. (2006). Aggression and antisocial behavior in youth. In N. Eisenberg, W. Damon, & R. M. Lerner (Eds.), Handbook of child psychology: Vol. 3, social, emotional, and personality development (6th ed., pp. 719–788). Hoboken, NJ: John Wiley and Sons, Inc.
Egeland, B. R., Carlson, E., & Sroufe, L. A. (1993). Resilience as process. Development and Psychopathology, 5, 517–528.
Egeland, B., Yates, T., Appleyard, K., & van Dulmen, M. (2002). The long-term consequences of maltreatment in the early years: A developmental pathway model to antisocial behavior. Children’s Services: Social Policy, Research, and Practice, 5, 249–260.
English, D. J., Upadhyaya, M. P., Litrownik, A. J., Marshall, J. M., Runyan, D. K., Graham, J. C., et al. (2005). Maltreatment’s wake: The relationship of maltreatment dimensions to child outcomes. Child Abuse and Neglect, 29, 597–619.
Feldman, R., Masalha, S., & Derdikman-Eiron, R. (2010). Conflict resolution in the parent-child, marital, and peer contexts and children’s aggression in the peer group: A process-oriented cultural perspective. Developmental Psychology, 46, 310–325.
Fluke, J. D., Yuan, Y.-Y. T., Hedderson, J., & Curtis, P. A. (2003). Disproportionate representation of race and ethnicity in child maltreatment: Investigation and victimization. Children and Youth Services Review, 25, 359–373.
Furstenberg, F. F., Jr, Cook, T., Eccles, J., Elder, G. H., & Sameroff, A. J. (1999). Urban families and adolescent success. Chicago: University of Chicago Press.
Ge, X., Best, K. M., Conger, R. D., & Simons, R. L. (1996). Parenting behaviors and the occurrence and co-occurrence of adolescent depressive symptoms and conduct problems. Developmental Psychology, 32, 717–731.
Gioia, G. A., Isquith, P. K., Guy, S. C., & Kenworthy, L. (2000). Behavior rating inventory of executive functioning, manual. Odessa, FL: Psychological Assessment Resources.
Goodman, R. (1995). The relationship between normal variation in IQ and common childhood psychopathology: A clinical study. European Child and Adolescent Psychiatry, 4, 187–196.
Goodman, S. H., & Gotlib, I. H. (Eds.). (2002). Children of depressed parents: Mechanisms of risk and implications for treatment. Washington, DC: American Psychological Association.
Graham, J. W. (2009). Missing data analysis: Making it work in the real world. Annual Review of Psychology, 60(6), 1–28.
Graham, J. W., Olchowski, A. E., & Gilreath, T. D. (2007). How many imputations are really needed? Some practical clarifications of multiple imputation theory. Prevention Science, 8, 206–213.
Harter, S., & Pike, R. (1984). The pictorial scale of perceived competence and social acceptance for young children. Child Development, 55, 1969–1982.
Haskett, M. E., Allaire, J. C., Kreig, S., & Hart, K. C. (2008). Protective and vulnerability factors for physically abused children: Effects of ethnicity and parenting context. Child Abuse and Neglect, 32, 567–576.
Haskett, M. E., Neupert, S. D., & Okado, Y. (2014). Factors associated with 3-year stability and change in parenting behavior of abusive parents. Journal of Child and Family Studies, 23(2), 263–274.
Herrenkohl, R., & Herrenkohl, T. (2009). Assessing a child’s experience of multiple maltreatment types: Some unfinished business. Journal of Family Violence, 24, 485–496.
Hoe, M., & Brekke, J. S. (2008). Cross-ethnic measurement invariance of the brief symptom inventory for individuals with severe and persistent mental illness. Social Work Research, 32, 71–78.
Jaffee, S. R., & Maikovich-Fong, A. K. (2011). Effects of chronic maltreatment and maltreatment timing on children’s behavior and cognitive abilities. Journal of Child Psychology and Psychiatry, 52, 184–194.
Kaufman, A. S., & Kaufman, N. L. (1990). Kaufman brief intelligence test manual. USA: American Guidance Service Inc.
Kelly, D., Faust, J., Runyon, M. K., & Kenny, M. C. (2002). Behavior problems in sexually abused children of depressed and non-depressed mothers. Journal of Family Violence, 17, 107–116.
Klimes-Dougan, B., & Kistner, J. (1990). Physically abused children’s responses to peers’ distress. Developmental Psychology, 26, 599–602.
Kolko, D. J. (1996). Individual cognitive-behavioral treatment and family therapy for physically abused children and their offending parents: A comparison of clinical outcomes. Child Maltreatment, 1, 322–342.
Lansford, J. E., Dodge, K. A., Pettit, G. S., Bates, J. E., Crozier, J., & Kaplow, J. (2002). A 12-year prospective study of the long-term effects of early child physical maltreatment on psychological, behavioral, and academic problems in adolescence. Archives of Pediatrics and Adolescent Medicine, 156, 824–830.
Little, R. J. A. (1988). A test of missing completely at random for multivariate data with missing values. Journal of the American Statistical Association, 83, 1198–1202.
Love, J. M., Chazan-Cohen, R., Raikes, H., & Brooks-Gunn, J. (Eds.). (2013). What makes a difference: Early Head Start evaluation findings in a developmental context. Monographs of the Society for Research in Child Development, Serial 306 (Vol. 78). Boston, MA: Wiley.
Manly, J. T., Kim, J. E., Rogosch, F. A., & Cicchetti, D. (2001). Dimensions of child maltreatment and children’s adjustment: Contributions of developmental timing and subtype. Development and Psychopathology, 13, 759–782.
Mantzicopoulos, P., French, B. F., & Maller, S. J. (2004). Factor structure of the pictorial scale of perceived competence and social acceptance with two pre-elementary samples. Child Development, 75, 1214–1228.
Maughan, A., & Cicchetti, D. (2002). Impact of child maltreatment and interadult violence on children’s emotion regulation abilities and socioemotional adjustment. Child Development, 73, 1525–1542.
McDonald, R., Jouriles, E. N., Tart, C. D., & Minze, L. C. (2009). Children’s adjustment problems in families characterized by men’s severe violence toward women: Does other family violence matter? Child Abuse and Neglect, 33, 94–101.
Murray, J., & Farrington, D. P. (2012). Risk factors for conduct disorder and delinquency: Key findings from longitudinal studies. The Canadian Journal of Psychiatry, 55, 633–642.
Nix, R. L., Pinderhughes, E. E., Dodge, K. A., Bates, J. E., Pettit, G. S., & McFayden-Ketchum, S. A. (1993). The relations between mothers’ hostile attribution tendencies and children’s externalizing behavior problems: The mediating role of mothers’ harsh discipline practices. Child Development, 70, 896–909.
Paley, B., Cox, M. J., & Kanoy, K. W. (2000). The young family interaction coding system. In P. K. Kerig & K. M. Lindahl (Eds.), Family observation coding systems: Resources for systematic research (pp. 273–288). Mahwah, NJ: Erlbaum.
Pears, K. C., Kim, H. K., & Fisher, P. A. (2008). Psychosocial and cognitive functioning of children with specific profiles of maltreatment. Child Abuse and Neglect, 32, 958–971.
Perez, C. M., & Widom, C. S. (1994). Childhood victimization and long-term intellectual and academic outcomes. Child Abuse and Neglect, 18, 617–633.
Raffaelli, M., Crockett, L. J., & Shen, Y.-L. (2005). Developmental stability and change in self-regulation from childhood to adolescence. The Journal of Genetic Psychology, 166, 54–75.
Robinson, J., Mantz-Simmons, L., Macfie, J., & The MacArthur Narrative Working Group. (1992). The narrative coding manual. Unpublished manuscript.
Rohner, R. P., & Britner, P. A. (2002). Worldwide mental health correlates of parental acceptance-rejection: Review of cross-cultural and intracultural evidence. Cross-Cultural Research, 36, 16–47.
Sameroff, A. J. (2000). Dialectical processes in developmental psychopathology. In A. Sameroff, M. Lewis, & S. Miller (Eds.), Handbook of developmental psychopathology (2nd ed., pp. 23–40). New York: Kluwer Academic/Plenum Publishers.
Sameroff, A. J., & Chandler, M. J. (1975). Reproductive risk and the continuum of caretaking casualty. In F. D. Horowitz, M. Hetherington, S. Scarr-Salapatek, & G. Sigel (Eds.), Review of child development research (Vol. 4, pp. 187–244). Chicago: University of Chicago Press.
SAS Institute, Inc. (2002–2004). SAS 9.1.3 Help and Documentation. Cary, NC: SAS Institute Inc.
Schafer, J. L. (1997). Analysis of incomplete multivariate data. Boca Raton, FL: Chapman Hall/CRC.
Sessa, F. M., Avenevoli, S., Steinberg, L., & Morris, A. S. (2001). Correspondence among informants on parenting: Preschool children, mothers, and observers. Journal of Family Psychology, 15, 53–68.
Shipman, K. L., Schneider, R., Fitzgerald, M. M., Sims, C., Swisher, L., & Edwards, A. (2007). Maternal emotion socialization in maltreating and non-maltreating families: Implications for children’s emotion regulation. Social Development, 16, 268–285.
Sroufe, L. A., & Rutter, M. (1984). The domain of developmental psychopathology. Child Development, 55, 17–29.
Staudt, M. M. (2001). Psychopathology, peer relations, and school functioning of maltreated children: A literature review. Children and Schools, 23, 85–101.
Toth, S. L., Cicchetti, D., Macfie, J., Rogosch, F. A., & Maughan, A. (2000). Narrative representations of moral-affiliative and conflictual themes and behavioral problems in maltreated preschoolers. Journal of Clinical Child Psychology, 29, 307–318.
US Department of Health and Human Services, Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau. (2012). Child Maltreatment 2011. http://www.acf.hhs.gov/programs/cb/stats_research/index.htm#can.
Vandenberg, B., & Marsh, U. (2009). Aggression in youths: Child abuse, gender, and SES. North American Journal of Psychology, 11, 437–442.
Veltman, M. W. M., & Browne, K. D. (2001). Three decades of child maltreatment research: Implications for the school years. Trauma, Violence, and Abuse, 2, 215–239.
Vidair, H. B., Reyes, J. A., Shen, S., Parrilla-Escobar, M. A., Heleniak, C. M., Hollin, I. L., et al. (2011). Screening parents during child evaluations: Exploring parent and child psychopathology in the same clinic. Journal of the American Academy of Child and Adolescent Psychiatry, 50, 441–445.
Vondra, J. I., Barnett, D., & Cicchetti, D. (1990). Self-concept, motivation, and competence among preschoolers from maltreating and comparison families. Child Abuse and Neglect, 14, 525–540.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Carmody, K.A., Haskett, M.E., Loehman, J. et al. Physically Abused Children’s Adjustment at the Transition to School: Child, Parent, and Family Factors. J Child Fam Stud 24, 957–969 (2015). https://doi.org/10.1007/s10826-014-9906-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-014-9906-7