
Abstract
We explored the association between maternal panic-like and depression symptoms with the offspring’s separation-related interpretive bias in a community sample. Separation anxiety has been found to be a precursor of panic disorders; therefore we focused on children and adolescents’ (aged 7–14 years) interpretive bias tapping into separation concerns using a story-based task. We collected self-reports and maternal reports of the levels of separation anxiety in the offspring. To assess maternal panic-like symptoms, we measured interoceptive and agoraphobic fears; as they have been found to increase the likelihood of experiencing panic disorders. The results showed that elevated levels of maternal interoceptive fears and agoraphobia co-occurring with depression were associated with an interpretive bias that related to separation anxiety concerns in children and adolescents. Offspring whose mothers experienced elevated panic-like symptoms together with depression did not show an interpretive bias linked to generalized anxiety concerns, suggesting the bias is content specific. The clinical significance of these findings stems from giving insight as to what extent separation interpretive biases would be influenced by maternal mental health variables, as these biases could constitute a vulnerability factor for later psychopathology. Further research is merited to address the findings with a longitudinal approach.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Separation Anxiety Disorder (SAD) is characterised as an intense fear of separation from the caretaking figure (American Psychiatric Association 2000). It is associated with significant distress (Jurbergs and Ledley 2005), school refusal and the disruption of educational attainment (Ehrenreich et al. 2008). SAD occurs in around four percent of young children (Dick-Niederhauser and Silverman 2006) and it is the most common anxiety diagnosis in those aged below 12 years of age (Cartwright-Hatton et al. 2006). Studies have found that childhood SAD is an antecedent to anxiety disorders later in life and it has strong links with the development of panic disorder (PD) and depression in young adults (Hirshfeld-Becker et al. 2008). Recent research indicates that interoceptive fears (fears of automatic bodily sensations) are related to SAD (Santucci et al. 2009) and can play a role in the development of PD (Acheson et al. 2007). Agoraphobia (a fear of being in situations from which escape might be difficult, as defined by the American Psychiatric Association 2000) has also been associated with SAD and PD (Biederman et al. 2004). Interoceptive and agoraphobic fears have been identified as distinct dimensions that are moderately correlated (Brown et al. 2005).
Theoretical frameworks (Dadds and Roth 2001) and empirical research (Elgar et al. 2004) highlight that parental psychopathology increases the likelihood of the offspring experiencing a mental health problem. With respect to SAD, parental PD and major depression both individually or co-occurring have been associated with higher rates of SAD in the offspring (Biederman et al. 2001, 2006; Unnewehr et al. 1998). Similarly, in a non-referred sample, SAD in childhood was associated with elevated symptoms of PD and/or Agoraphobia in the parents (Biederman et al. 2004).
Researchers have used cognitive frameworks to understand links between the presence of mental health problems in parents and anxiety in their children (Creswell et al. 2010; Hadwin et al. 2006) where this research is consistent with models of adult and childhood anxiety, which show that cognitive biases may constitute a vulnerability factor for anxiety disorders (reviews by Bar-Haim et al. 2007; Muris and Field 2008). Cognitive models of PD propose that interpretive biases can be a core disturbance in the disorder (Clark 1986; Teachman et al. 2007). In addition, studies that have considered associations between cognitive biases and separation anxiety have found that threat-related attentional biases in children with separation anxiety resemble those observed in adults (In-Albon et al. 2010; Perez-Olivas et al. 2008; Stirling et al. 2006). Children with SAD (compared with non-referred children) have also been found to rate ambiguous separation pictures as unpleasant and arousing (In-Albon et al. 2009). Further evidence suggests that interpretive biases in SAD are content specific; they focus on stories and events that link to separation concerns (Bögels et al. 2003; In-Albon et al. 2008). However, future research on the specificity of cognitive biases in childhood anxiety is urgently needed (Bögels et al. 2003; Schniering and Rapee 1997).
Empirical work has explored links between parental PD and cognitive biases in the offspring (Schneider et al. 2002). Here, children aged 8–15 years were asked to interpret three types of ambiguous scenarios, related to panic (body sensations such as heart pounding, dizziness), animal phobia (i.e. a spider) and colds (i.e. head pain and feeling bad). The authors found that children of parents experiencing PD (compared to children whose parents had animal phobia and healthy controls) showed greater interpretation bias towards panic-relevant stimuli after viewing a video of a woman with a panic disorder describing a severe panic attack.
In this paper we extend this research and utilise a developmental framework to consider the specificity of cognitive biases in typically developing children with elevated separation anxiety symptoms and their relationship to parental psychopathology. The main focus of interest was to understand links between parental panic-like symptoms (specifically interoceptive and agoraphobic fears) on their own or co-occurring with depression and children’s interpretive biases for separation-related events. The importance of our study stems from identifying a link between parental mental health and interpretive biases that relate to separation anxiety. Because separation anxiety precedes PD (Biederman et al. 2006) a separation-related interpretive bias may be more evident in childhood, compared with a panic-related interpretive bias. We focused on maternal and not paternal mental health and hypothesised that elevated maternal panic-like symptoms individually or co-occurring with depression would be significantly linked to an interpretive bias that relates to separation anxiety concerns in offspring. This bias could be predictive of elevated symptoms of separation anxiety in the child. Because interpretive biases may be content specific we did not expect that maternal panic-like symptoms on their own or together with depression would be significantly associated with generalized anxiety concerns in the offspring. The link between parental PD and SAD in the offspring has been extensively investigated therefore we did not further explore this issue.
Method
Participants
One hundred and thirty-three mothers, recruited through several sources (e.g., schools, church groups), expressed an interest in the study. To screen for offspring at risk for separation anxiety, they completed maternal mental health measures. Mothers were screened to provide cases for two 2 × 2 analyses. For the first analysis we wanted to look at typical or elevated levels of depression and typical or elevated levels of agoraphobia. For the second analysis we wanted to look at typical or elevated levels of depression and typical or elevated levels of interoceptive symptoms. Twenty-four of the offspring were selected as having mothers whose depression scores were 13 or above on the Beck’s depression Inventory (BDI-II; Beck et al. 1996); this cut-off point has been found adequate to discriminate between individuals with elevated or typical symptoms of depression in a community sample (Lasa et al. 2000). In addition, approximately half of the offspring selected (N = 27) had mothers whose levels of interoceptive symptoms were above the typical range (≥9.6) and more than half of the offspring selected (N = 36) had mothers whose levels of agoraphobia were above the typical range (≥12.8). These cut-off points of 9.6 and 12.8 were chosen as defining symptoms of interoceptive and agoraphobic fears based on previous research (Rapee et al. 1994) (Table 1).
The final sample consisted of 60 non-referred children and their mothers. The age range of the children was 7–14 years (mean age: 10.75 years; SD = 26.31 months; 29 males and 31 females). We could obtain the levels of family income for 40 cases. There were no significant differences in family income for offspring whose mothers had elevated symptoms of depression compared to those whose mothers did not. In addition no significant differences in family income were observed for offspring whose mothers had elevated symptoms of interoceptive fear or agoraphobia compared to those whose mothers did not.
All procedures were approved by the School of Psychology Ethics Committee at the University of Southampton, UK.
Maternal Measures
The Albany Panic and Phobia Questionnaire (APPQ) (Rapee et al. 1994) was used to assess maternal levels of panic-like symptoms. It is a 27-item self-report questionnaire that measures agoraphobia and social phobia, as well as fears of automatic bodily sensations (Brown et al. 2005). Hence, it consists of an agoraphobia subscale, a social phobia subscale and an interoceptive subscale. For the purposes of this study we employed the interoceptive and agoraphobia subscales. An analysis of the APPQ has provided evidence of the sound psychometric properties of these subscales (Brown et al. 2005). Each of the three subscales show adequate test–retest reliability and good to excellent internal consistency (α coefficients ranging from .87–.90).
We used the revised Beck’s Depression Inventory (BDI-II) (Beck et al. 1996) to measure general levels of depression in the mothers. The BDI-II has been identified as an appropriate instrument for screening depressive disorders in the general population, using a cut-off point of 13 to indicate elevated symptoms of depression (Lasa et al. 2000).
Child Measures
Interpretation Task
For the “Story task interpretation paradigm” we developed stories based on those used in previous research to assess interpretive biases in children (Muris et al. 2000a, b; Bögels and Zigterman 2000). We configured 8 story scenarios with black and white electronic pictures using a Superlab 6 programming environment. Below each drawing there were 2–3 sentences describing the situation. To explore cognitive specificity, five scenarios tapped into separation anxiety concerns and the other three into generalized anxiety concerns. For each story children were asked to choose one of three possible interpretations (threat-related, neutral, and positive). The characters in each scenario did not have any emotional expression as the faces in the pictures were left blank. We assessed to what extent the eight stories presented to the children were tapping into separation anxiety or generalized anxiety concerns with Cohen’s Kappa inter-rater agreement. We found a satisfactory agreement between two independent raters (K = .75). Whether the three different options in each story were tapping into a positive, threat-related or neutral appraisal was also examined with Cohen’s Kappa. This time Cohen’s Kappa was 1.0 indicating total inter-rater agreement.
Anxiety Measurements
The Revised Child Anxiety and Depression Scale (RCADS)—Child and Parent Versions (Chorpita et al. 2000) were used to measure symptoms of anxiety in offspring. The RCADS is a 47 item self-report measure that assesses symptoms of DSM IV-defined anxiety disorders and depression. The scales of the RCADS have adequate internal consistency and test–retest stability and the whole instrument has proven validity (Costa and Weems 2005; Chorpita et al. 2000). The present study employed the separation anxiety disorder scale and the generalized anxiety scale. In the parent version of the RCADS the wording in every item is changed from “I” to “My Child”. The normative data for the RCADS is based on a large sample of children aged 8–13 years. The mean for the separation anxiety scale is M = 3.49 (SD = 2.96) and the mean for the generalized anxiety scale is M = 7.19 (SD = 3.47) (Chorpita et al. 2000).
Procedure
We obtained informed consent to participate in the study from both mothers and offspring. We sent a questionnaire pack including the BDI-II, APPQ, RCADS-P and a FREE POST envelope to the mothers’ home. We conducted a 30 min child assessment individually and in a quiet environment. Children sat approximately 60 cm away from the computer screen to carry out the story task. Before the task, we told the children that they were going to see some pictures on the screen describing a story with a main character and that they had to decide what the main character was thinking. We presented the children with three possible options to choose from and we instructed them to press number 1, 2 or 3 on the computer keyboard depending on the option chosen. The order of presentation of the options was counterbalanced. In addition half of the children were shown the stories depicting separation anxiety concerns first and the other half was shown the stories depicting generalized anxiety concerns first. Within each story type, stories were randomly presented. We always administered the RCADS after the completion of the story task and debriefed mothers and offspring at the end of the study.
Results
Children’s Characteristics
We did not find significant differences in gender or age for offspring whose mother had typical levels of depression, interoceptive fears or agoraphobia compared to offspring whose mother had elevated symptoms. Based on the normative data of the RCADS the mean levels of self-report (M = 4.91, SD = 4.00) or maternal-report (M = 4.48, SD = 3.25) separation anxiety fell slightly above the normative range. The mean levels of self-report (M = 5.70, SD = 2.98) or maternal-report (M = 5.58, SD = 3.29) generalized anxiety fell below the normative range. With a paired sample t-test we did not find significant differences in the levels of separation or generalized anxiety as reported by the child or the mother. We found that maternal and child report of separation anxiety were significantly moderately correlated (r = .31, p < 0.05) whereas maternal and child report of generalized anxiety were not significantly correlated. The correlation between chronological age in the offspring and the levels of maternal-report separation anxiety was found to be approaching significance (r = −.24, p = 0.06) and indicated that reported symptoms of separation anxiety decreased with age. We did not find a significant correlation between the levels of self-report separation anxiety and chronological age or between the levels of self-report or maternal-report generalized anxiety and chronological age. Finally there were no significant differences in the mean separation or generalized anxiety levels by gender.
Mothers’ Characteristics
We found an association between elevated versus typical interoceptive symptoms group and elevated versus typical agoraphobia symptoms group (χ² = 4.05, df = 2, p < 0.05); but the size of the association was small φ = 0.26., which indicates a small overlap between the interoceptive and agoraphobia symptoms groups. Mothers with elevated interoceptive symptoms had elevated symptoms of depression, above the cut-off point of 13 (M = 14.88, SD = 10.66). Mothers with typical levels of interoceptive symptoms had typical levels of depression, below the cut-off of 13 (M = 10.12, SD = 9.58). In addition mothers with elevated symptoms of agoraphobia had elevated symptoms of depression (M = 13.22, SD = 10.08), whereas mothers with typical symptoms of agoraphobia had typical levels of depression (M = 10.83, SD = 9.94).
The Interpretation Task
We conducted a frequency count for each of the positive, neutral and threat-related interpretation options. For stories depicting separation anxiety concerns, the average number of positive interpretations was 2.10 (SD = 1.07), the average number of neutral interpretations was 1.55 (SD = 1) and the average number of threat-related interpretations was 1.33 (SD = 0.97). In addition the number of positive interpretations was negatively correlated with the number of threat-related interpretations (ρ = −0.52, p < 0.01). The number of positive, threat-related or neutral interpretations for stories depicting separation concerns was not significantly correlated with the number of positive, threat-related or neutral interpretations for stories depicting generalized anxiety concerns. This finding gives some evidence of the discriminant validity of the story task.
To explore interpretive biases, we computed an interpretive bias index score for separation and generalized stories as a sum across the 5 and 3 stories, respectively. When children chose a threat-related option a score of −1 was assigned, when they chose a neutral option a score of 0 was assigned and when they chose a positive option a score of +1 was assigned; a negative score indicated interpretive bias towards threat. In support of the discriminant validity of the story task, the separation anxiety bias index and the generalized anxiety bias index were not significantly correlated (r = 0.10, p = 0.44). In a further analysis we found that chronological age and gender did not significantly correlate with the interpretive bias index for separation or generalized stories in the offspring.
Maternal Mental Health and Offspring Interpretive Bias for Separation Stories
We conducted two 2 × 2 analyses of variance. Interoceptive and agoraphobic fears were treated as distinct constructs (Brown et al. 2005). The first analysis included the 36 cases with elevated levels of agoraphobia and the 24 with typical levels, along with the 24 cases with elevated levels of depression and the 36 cases with typical levels. In the second analysis we used the 27 cases with elevated levels of interoceptive symptoms and the 33 cases with typical levels. The same number of cases for mothers experiencing typical versus elevated levels of depression as in the first analysis were included.
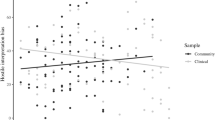
In the first 2 × 2 analysis of variance we found no significant main effects for the levels of depression (F (1,56) = 0.19, p = 0.65) or agoraphobia (F (1,56) = 0.75, p = 0.38) on the interpretation bias index for separation stories. However a significant interaction effect was found between the levels of depression and agoraphobia in the mother and the interpretive bias index F (1, 56) = 5.88, p < 0.05, ω2 = 0.07; see Fig. 1.

The interaction between maternal depressive and agoraphobic symptoms and the child’s separation interpretive bias
With a series of t-tests we further explored the interaction effect. The interpretive bias index was similar and did not significantly differ in offspring whose mothers had typical levels of depression (M = −0.60, SE = 0.45) or elevated levels of depression (M = 0.33, SE = 0.58) when the levels of agoraphobia in the mothers were typical. But an interpretive bias towards threat, as indicated by the negative sign was significantly evident in offspring whose mothers had elevated levels of depression (M = −0.40, SE = 0.45) as opposed to offspring whose mothers had typical levels of depression (M = 0.95, SE = 0.38), when the levels of agoraphobia in the mother were elevated (t (43) = 2.30, p < 0.05).
In the second 2 × 2 analysis of variance we found a significant interaction effect between the levels of depression and interoceptive fears in the mother on the separation interpretive bias index in the offspring (F(1, 56) = 4.35, p < 0.05, ω2 = 0.05). No significant main effects were observed for the levels of depression (F(1,56) = 0.67, p = 0.41) or interoceptive fears (F(1,56) = 0.69, p = 0.40) on the interpretation bias index (Fig. 2).

The interaction between maternal depressive and interoceptive symptoms and the child’s separation interpretive bias
We explore this interaction effect with a series of t-tests. An interpretive bias did not significantly differ in offspring whose mothers had typical levels of depression (M = 0.08, SE = 0.37) or elevated levels of depression (M = 0.70, SE = 0.56) when the levels of interoceptive symptoms in the mother were typical. However an interpretive bias towards threat, as indicated by the negative sign significantly emerged in offspring whose mothers had elevated levels of depression (M = −0.71, SE = 0.47) as opposed to offspring whose mothers had typical levels of depression (M = 0.69, SE = 0.49) when their mothers had elevated levels of interoceptive symptoms (t (25) = 2.10, p < 0.05).
Did Interpretive Biases for Stories Depicting Separation Concerns Predict Symptoms of Separation Anxiety?
We conducted two linear regression analyses with separation interpretive bias index as the predictor and maternal or child reports of separation anxiety in the offspring as the predicted variables. We found no significant associations even when controlling for chronological age.
Exploring the Specificity of the Interpretive Bias
To explore specificity of the effects of maternal depression and panic -like symptoms on children’s interpretive bias we conducted a 2 × 2 analysis of variance with the generalized anxiety bias index as the dependent variable. The analysis showed no significant main or interaction effects of the levels of depression, or agoraphobia on the generalized bias index. An additional two-way ANOVA showed no significant main or interaction effects for the levels of depression, or interoceptive fears on this generalized interpretive bias index. In addition with two linear regression analyses we found that the generalized interpretive bias index did not predict maternal or child reports of generalized anxiety.
Discussion
In the current study, we found that offspring whose mothers exhibited elevated symptoms of depression and agoraphobia showed a threat-related interpretive bias when presented with stories tapping into separation anxiety concerns. A similar result was found for offspring whose mothers exhibited elevated symptoms of depression and interoceptive fears. This pattern of findings was not found for interpretive biases towards threat in stories depicting generalized anxiety concerns; indicating some degree of content specificity in interpretive biases in this sample. This result is consistent with research that favours the inclusion of content specific to the individuals’ concerns when exploring interpretive biases (Bögels et al. 2003; In-Albon et al. 2008).
The association that we found between maternal panic-like symptoms co-occurring with depression and a separation-related interpretive bias in the child extends previous research which has found links between parental PD and interpretation biases in children. For example, Schneider and colleagues (2002) found that children of panic disordered parents showed a panic-like interpretive style after watching a video of a woman diagnosed with panic disorder describing a panic attack.
In addition, our data is indicative of an association between maternal panic-like symptoms co-occurring with depression and a separation-related interpretive bias in the child. This finding is consistent with researchers who have argued that SAD is not exclusively linked to panic anxiety (Lipsitz et al. 1994) as it may also be linked to other psychopathologies like depression.
Interestingly, we did not find that a threat-related interpretive bias significantly predicted elevated symptoms of anxiety in the child. This result is consistent with some previous research by In-Albon et al. (2009) here children with separation anxiety did not interpret pictures related to separation anxiety concerns in a more negative way than non-referred children. Our own result does merit further investigation; it raises the possibility that cognitive biases constitute a vulnerability factor to anxiety disorders (Bar-Haim et al. 2007; Muris and Field 2008) that can occur in the absence of anxiety symptoms. Longitudinal studies assessing the relationship between cognitive biases related to separation anxiety and anxiety symptoms at different points across development would shed some light on these findings. It would also be of interest to explore the link between these cognitive biases and the emergence of anxiety symptoms with a non-referred sample with moderate to borderline scores in anxiety.
Based on a developmental approach the current study took age into consideration when exploring the associations between maternal mental health with interpretive biases and elevated symptoms of anxiety in offspring. We found that age did not moderate these associations. One reason for not finding this moderating effect could be the restricted age range of our sample (7–14 years). Indeed a previous study found that age made a unique and significant contribution to the interpretation of physical symptoms related to anxiety with a sample of children aged 4–13, a wide age range (Muris et al. 2008). Our previous work (Perez-Olivas et al. 2008) showed that age was moderating associations between attentional biases to angry faces and the offspring’s levels of separation anxiety with a narrower age range than in Muris’s et al. (2008) study. Thus, it is possible that the emergence of attentional and interpretive biases follow different developmental patterns.
The present study extends previous research to highlight that interpretive biases specifically related to separation anxiety can be observed in offspring whose mothers show panic-like and depressive symptoms; however there are some limitations to the findings. The story task was developed based on previous work on interpretive biases (e.g. Muris et al. 2000a) but we did not collect children’s and adolescents’ views onto what extent they perceived the themes represented in the story scenarios as relevant to their own separation concerns. Further research would benefit from developing content-specific story tasks with proven psychometric properties adequate for children in different age groups. In line with this argument, recent research has developed a paradigm for assessing anxiety-disorder-specific interpretation biases with picture stimuli (In Albon et al. 2008).
Another limitation of our study is that it is cross-sectional in nature. Longitudinal research is important to further our understanding of trajectories of SAD and the influence of maternal mental health on content-specific interpretive biases. In addition, we used questionnaires, not observational measures and it could be argued that younger children may have differed in their report of anxiety, as they can have more difficulties in recalling symptoms (Biederman et al. 2007). Future studies would benefit from including multiple informants when aiming to understand the relationship between parental psychopathology and their children (De Los Reyes and Kazdin 2005; Kagan et al. 2002). The inclusion of paternal reports would also be of interest (Bögels and Brechman-Toussaint 2006).
Our sample consisted of high-risk children whose mothers had not been diagnosed with a mental health issue and future studies should investigate whether our findings would be replicated in a family with a history of psychopathology. Our study provides preliminary evidence for the role that maternal psychopathology can have on interpretive biases tapping into separation anxiety concerns. Literature suggests that separation anxiety may reflect an underlying anxiety diathesis that would increase risk for a range of adult anxiety disorders (Biederman et al. 2007). Hence, the clinical implications of further examining parental psychopathology and its links with separation-related interpretive biases is clear if we consider that cognitive biases can constitute a vulnerability factor for anxiety (Bar-Haim et al. 2007; Muris and Field 2008). The scope of this paper was not to explore mechanisms via which maternal psychopathology would influence separation-related interpretive biases in the offspring; but future research should address this issue. Creswell and colleagues have proposed various pathways informative for future research, which explain how parents could contribute to the emergence of cognitive processing biases in offspring. Some of the pathways the authors propose are parental cognition (for example the child and the parent would share a bias that favours threat) parental behaviour (modelling of anxious behaviours) or expectations (e.g. parental perceptions of offspring’s coping) (Creswell et al. 2010).
References
Acheson, D. T., Forsyth, J. P., Prenoveau, J. M., & Bouton, M. E. (2007). Interoceptive fear conditioning as a learning model of panic disorder: An experimental evaluation using 20% CO2-enriched air in a non-clinical sample. Behaviour Research and Therapy, 45, 2280–2294.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (DSM-IV-TR) (4th ed.). Washington DC: American Psychiatric Association.
Bar-Haim, Y., Lamy, D., Pergamin, L., Bakermans-Kranenburg, M. J., & van IJzendoorn, M. H. (2007). Threat-related attentional bias in anxious and nonanxious individuals: A meta-analytic study. Psychological Bulletin, 133, 1–24.
Beck, A. T., Steer, R. A., & Brown, G. K. (1996). The Beck depression inventory manual. San Antonio: The Psychological Corporation.
Biederman, J., Faraone, S. V., Hirshfeld-Becker, D. R., Friedman, D., Robin, J. A., & Rosenbaum, J. F. (2001). Patterns of psychopathology and dysfunction in high-risk children of parents with panic disorder and major depression. American Journal of Psychiatry, 158, 49–57.
Biederman, J., Monuteaux, M. C., Faraone, S. V., Hirshfeld-Becker, D. R., Henin, A., Gilbert, J., et al. (2004). Does referral bias impact findings in high-risk offspring for anxiety disorders? A controlled study of high-risk children of non-referred parents with panic disorder/agoraphobia and major depression. Journal of Affective Disorders, 82, 209–216.
Biederman, J., Petty, C., Faraone, S. V., Henin, A., Hirshfeld-Becker, D., Pollak, M. H., et al. (2006). Effects of parental anxiety disorders in children at high risk for panic disorder: A controlled study. Journal of Affective Disorders, 94, 191–197.
Biederman, J., Petty, C. R., Hirshfeld-Becker, D. R., Henin, A., Faraone, S. V., Fraire, M., et al. (2007). Developmental trajectories of anxiety disorders in offspring at high risk for panic disorder and major depression. Psychiatry Research, 153, 245–252.
Bögels, S. M., & Brechman-Toussaint, M. L. (2006). Family issues in child anxiety: Attachment, family functioning, parental rearing and beliefs. Clinical Psychology Review, 26, 834–856.
Bögels, S. M., Snieder, N., & Kindt, M. (2003). Specificity of dysfunctional thinking in children with social anxiety, separation anxiety and generalized anxiety. Behavior Change, 20, 160–169.
Bögels, S. M., & Zigterman, D. (2000). Dysfunctional cognitions in children with social phobia, separation anxiety disorder, and generalized anxiety disorder. Journal of Abnormal Child Psychology, 28, 205–211.
Brown, T. A., White, K. S., & Barlow, D. H. (2005). A psychometric reanalysis of the Albany panic and phobia questionnaire. Behavior Therapy, 43, 337–355.
Cartwright-Hatton, S., McNicol, K., & Doubleday, E. (2006). Anxiety in a neglected population: Prevalence of anxiety disorders in pre-adolescent children. Clinical Psychology Review, 26, 817–833.
Chorpita, B. F., Yim, L., Moffitt, C., Umemoto, L. A., & Francis, S. E. (2000). Assessment of symptoms of DSM IV anxiety and depression in children: A revised child anxiety and depression scale. Behaviour Research and Therapy, 38, 835–855.
Clark, D. M. (1986). A cognitive approach to panic. Behaviour Research and Therapy, 24, 461–470.
Costa, N. M., & Weems, C. F. (2005). Maternal and child anxiety: do attachment beliefs or children’s perceptions of maternal control mediate their association? Social Development, 14, 574–590.
Creswell, C., Cooper, P., & Murray, L. (2010). In J. A. Hadwin & A. P. Field (Eds.), Information processing biases and anxiety: A developmental perspective (pp. 279–296). Chichester: John Wiley & Sons, Ltd.
Dadds, M. R., & Roth, J. H. (2001). Family processes in the development of anxiety disorders. In M. Vasey & M. R. Dadds (Eds.), The developmental psychopathology of anxiety (pp. 278–303). Oxford: Oxford University Press.
De Los Reyes, A., & Kazdin, A. E. (2005). Informant discrepancies in the assessment of childhood psychopathology: A critical review, theoretical framework, and recommendations for further study. Psychological Bulletin, 131, 483–509.
Dick-Niederhauser, A., & Silverman, W. K. (2006). Separation anxiety disorder. In J. E. Fisher & W. T. O’ Donohue (Eds.), Practitioner’s guide to evidence based-psychotherapy (pp. 627–633). New York: Springer Science and Business Media.
Ehrenreich, J. T., Santucci, L. C., & Weiner, C. (2008). Separation anxiety disorder in youth: Phenomenology, assessment and treatment. Psicología Conductual, 16, 389–412.
Elgar, F. J., McGrath, P. J., Waschbusch, D. A., Stewart, S. H., & Curtis, L. J. (2004). Mutual influences on maternal depression and child adjustment problems. Clinical Psychology Review, 24, 441–459.
Hadwin, J. A., Garner, M., & Perez-Olivas, G. (2006). The development of information processing biases in childhood anxiety: A review and exploration of its origins in parenting. Clinical Psychology Review, 26, 876–894.
Hirshfeld-Becker, D. R., Micco, J. A., Simoes, N. A., & Henin, A. (2008). High risk studies and developmental antecedents of anxiety disorders. American Journal of Medical Genetics Part C: Seminars in Medical Genetics, 148, 99–117.
In-Albon, T., Dubi, K., Rapee, R. M., & Schneider, S. (2009). Forced choice reaction time paradigm in children with separation anxiety disorder, social phobia and nonanxious controls. Behaviour Research and Therapy, 47, 1058–1065.
In-Albon, T., Klein, A., Rinck, M., Becker, E., & Schneider, S. (2008). Development and evaluation of a new paradigm for the assessment of anxiety disorder-specific interpretation bias using picture stimuli. Cognition and Emotion, 22, 422–436.
In-Albon, T., Kossowsky, J., & Schneider, S. (2010). Vigilance and avoidance of threat in the eye movements of children with separation anxiety disorder. Journal of Abnormal Child Psychology, 38, 225–235.
Jurbergs, N., & Ledley, D. R. (2005). Separation anxiety disorder. Pediatric Annals, 34, 108–115.
Kagan, J., Snidman, N., McManis, M., Woodward, S., & Hardway, C. (2002). One measure, one meaning: Multiple measures, clearer meaning. Development and Psychopathology, 14, 463–475.
Lasa, L., Ayuso-Mateos, J. L., Vazquez-Barquero, J. L., Diez-Manrique, F. J., & Dowrick, C. F. (2000). The use of the Beck depression inventory to screen for depression in the general population: A preliminary analysis. Journal of Affective Disorders, 57, 261–265.
Lipsitz, J. D., Martin, L. Y., Mannuzza, S., Chapman, T. F., Liebowitz, M. R., Klein, D. F., et al. (1994). Childhood separation anxiety disorder in patients with adult anxiety disorders. American Journal of Psychiatry, 151, 927–929.
Muris, P., & Field, A. P. (2008). Distorted cognition and pathological anxiety in children and adolescents. Cognition and Emotion, 22, 395–421.
Muris, P., Luermans, J., Merckelbach, H., & Mayer, B. (2000a). “Danger is lurking everywhere”. The relation between anxiety and threat perception abnormalities in normal children. Journal of Behaviour Therapy and Experimental Psychiatry, 31, 123–136.
Muris, P., Merckelbach, H., & Damsma, E. (2000b). Threat perception bias in nonreferred, socially anxious children. Journal of Clinical Child Psychology, 29, 348–359.
Muris, P., Vermeer, E., & Horselenberg, R. (2008). Cognitive development and the interpretation of anxiety-related physical symptoms in 4–13 year old non-clinical children. Journal of Behavior Therapy and Experimental Psychiatry, 39, 73–86.
Perez-Olivas, G., Stevenson, J., & Hadwin, J. A. (2008). Do anxiety-related attentional biases mediate the link between maternal over involvement and separation anxiety in children? Cognition and Emotion, 22, 509–521.
Rapee, R. M., Craske, M. G., & Barlow, D. H. (1994). Assessment instrument for panic disorder that includes fear of sensation-producing activities: The Albany panic and phobia questionnaire. Anxiety, 1, 114–122.
Santucci, L. C., Ehrenreich, J. T., Trosper, S., Bennett, S. M., & Pincus, D. B. (2009). Development and preliminary evaluation of a one-week summer treatment program for separation anxiety disorder. Cognitive & Behavioral Practice, 16, 317–331.
Schneider, S., Unnewehr, S., Florin, I., & Margraf, J. (2002). Priming panic interpretations in children of patients with panic disorder. Journal of Anxiety Disorders, 16, 605–624.
Schniering, C. A., & Rapee, R. M. (1997). A test of the cognitive model of panic: Primed lexical decision in panic disorder. Journal of Anxiety Disorders, 11, 557–571.
Stirling, L., Eley, T. C., & Clark, D. M. (2006). Avoidance of negative faces and social anxiety in children. Journal of Clinical Child & Adolescent Psychology, 35, 440–445.
Teachman, B. A., Smith-Janik, S. B., & Saporito, J. (2007). Information processing biases and panic disorder: Relationships among cognitive and symptom measures. Behaviour Research and Therapy, 45, 1791–1811.
Unnewehr, S., Schneider, S., Florin, I., & Margraf, J. (1998). Psychopathology in children of patients with panic disorder or animal phobia. Psychopathology, 31, 69–84.
Acknowledgments
We would like to thank all the families and children that took part in the study. We would also like to thank the Economic Social and Research Council (E.S.R.C) for funding the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Perez-Olivas, G., Stevenson, J. & Hadwin, J.A. The Association Between Elevated Maternal Panic-Like and Depression Symptoms and Separation-Related Interpretive Biases in Offspring. J Child Fam Stud 20, 232–239 (2011). https://doi.org/10.1007/s10826-010-9408-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-010-9408-1