
Abstract
Purpose
To assess the accuracy and reliability of comprehensive chromosome screening by next-generation sequencing (NGS) of human trophectoderm (TE) biopsy specimens.
Methods
The reliability and accuracy of diagnoses made by preimplantation genetic testing for aneuploidy (PGT-A) from TE biopsy were tested. Repeat biopsies of TE and inner cell mass (ICM) samples were obtained from thawed blastocysts previously tested by NGS. To test for the reliability of the NGS assay, biopsy samples were compared with the original PGT-A results. Prior NGS testing classified the TE samples as euploid, aneuploid, or aneuploid-mosaic. The resulting re-biopsied samples underwent SurePlex whole genome amplification followed by NGS via the MiSeq platform, with copy number value (CNV) determined using BlueFuse Multi Software. The primary outcome measure was reliability, defined as concordance between initial TE result and the repeat biopsies. Accuracy was determined by concordance between the TE and ICM samples, and compared between three chromosome types (disomic, aneuploid, and mosaic).
Results
Re-biopsies were performed on 32 embryos with prior PGT-A showing euploidy (10 embryos), aneuploidy of one or two chromosomes (4 embryos), or aneuploid-mosaic with one aneuploid chromosome and one mosaic chromosome (18 embryos). One hundred twenty-nine biopsy samples completed NGS (90 TE and 39 ICM biopsies) and 105 biopsy results were included in the analysis. TE biopsies provide a highly accurate test of the future fetus, with the ICM disomic concordance rate of 97.6%. Clinical concordance rates indicate that TE biopsies provide a reliable test when the result is euploid (99.5%) or aneuploid (97.3%), but less reliable when the result is mosaic (35.2%).
Conclusion
TE biopsies predict euploidy or aneuploidy in the ICM with a high degree of accuracy. PGT-A with NGS of TE biopsies is shown to be highly reliable, with clinically relevant concordance rates for aneuploidy and euploidy over 95%. TE biopsies indicating mosaicism were less reliable (35.2%), presumably because mitotic non-disjunction events are not uniformly distributed throughout the blastocyst. However, classification of TE biopsy of PGT-A with NGS results as either aneuploid or euploid provides a highly reliable test.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Aneuploidy is remarkably common during preimplantation development in human embryos and represents the major cause of implantation failure and miscarriage [1]. Preimplantation genetic testing for aneuploidy (PGT-A) was developed to select against aneuploid preimplantation embryos and identify euploid embryos allowing for increased pregnancy rates per transfer [2]. Early approaches to PGT-A biopsied just one or two cells from cleavage-stage embryos and counted a limited number of chromosomes using fluorescence in situ hybridization (FISH) [3]. The use of trophectoderm (TE) biopsy at the blastocyst stage [3] to perform PGT relies upon the premise that biopsy at the blastocyst stage of development enables safe sampling of four to five cells, and next-generation sequencing (NGS) provides comprehensive chromosome screening (CCS) of all 24 chromosomes [4]. It also assumes that the chromosome complement of the TE, the future placenta, accurately reflects that of the inner cell mass (ICM), the future embryo proper. However, controversy exists on its ability to do such [5]. In recent years, TE biopsy using NGS for CCS has had an increase in the classification of embryos as mosaic [6], with unclear information as to the outcome of these embryos if transferred [7].
Mosaicism most commonly results from post-zygotic mitotic errors [8, 9]. NGS has demonstrated accuracy of diagnosing mosaicism [10], and, as a result, has become more sensitive in the de-selection of compromised embryos, thus improving implantation and pregnancy rates [11]. Recent studies have shown successful pregnancies and live births [12] with the transfer of low-level mosaicism (< 40%), albeit with higher miscarriage rates and lower implantation rates [13]. The existence of confined placental mosaicism (CPM) in some fetuses, coupled with the observation that in mice the TE is more tolerant of mosaicism than the ICM [14], suggests that TE biopsies may not consistently predict the status of the ICM. Moreover, this puts the reliability of diagnosing mosaicism via TE biopsy into question and makes it unclear if mosaic embryos should be categorized as non-transferable [15].
To evaluate the accuracy of PGT-A to diagnose the ploidy status of the ICM and to determine the reliability of PGT-A within TE biopsies, we thawed previously tested human embryos, dissociated them, and repeated PGT-A in the ICM and TE. The objective of this study is to assess the accuracy and reliability of PGT-A by comparing the results of the initial clinical biopsy with repeat biopsies of TE and ICM from the same embryos. The primary outcome was the concordance between the initial TE biopsies and subsequent repeat biopsies. The secondary outcome is to estimate the accuracy of the TE to predict the ICM. Our hypothesis is that repeat TE biopsies will demonstrate concordance for euploid (disomic), aneuploid, and mosaic chromosomes. Additionally, we hypothesize that PGT-A with NGS using TE biopsies accurately represents the ICM across varying types of embryos (euploid, aneuploid, and aneuploid-mosaic) as well, showing no statistical significance between concordance rates of ICM and TE re-biopsies. With this study, we hope to estimate not the possibility of inaccuracies but rather the quantitative incidence of these inaccuracies within our testing paradigm, as well as assess if PGT-A has the ability to accurately identify an embryo as suitable or not suitable for transfer.
Materials and methods
IRB approval (H6902) was obtained to accession embryos that had undergone PGT-A by NGS from February 2015 to January 2017. Blastocysts were produced following standard protocols for controlled ovarian stimulation, oocyte retrieval, fertilization, and embryo culture. Biopsies of four to five TE cells were performed on days 5, 6, or 7 in the IVF laboratory of a large academic fertility center. Results using PGT-A were reported as euploid, aneuploid (for one or two chromosomes), or aneuploid plus mosaic (one aneuploid chromosome and one mosaic chromosome). A reference laboratory per the institution’s standard clinical protocol performed whole genome amplification (WGA) using SurePlex (Illumina, San Diego), followed by VeriSeq DNA library prep (Illumina, San Diego) and NGS MiSeq sequencing to assess for chromosomal copy number. Following biopsy, blastocysts were vitrified with the intention to thaw any euploid embryos for transfer in a subsequent frozen embryo transfer cycle as indicated. Only embryos donated for research by consenting patients were used in this study. Some of the euploid blastocysts re-biopsied in this study had been tested by aCGH due to the low availability of euploid blastocyst tested using NGS.
Embryos were warmed individually via a standard protocol for vitrified embryos (Irvine Scientific Vitrification Thaw kit). Embryos were placed in Global Total Media with global protein supplement and incubated at 37.2 °C with 6.0% CO2 until appropriate blastocyst expansion was noted. Biopsies were performed only on expanded blastocysts, which allowed for visualization of distinct ICM and TE. Multiple biopsies from each blastocyst were taken using a Hamilton Thorne Zilos-tk Red-1 Laser with 400-μs laser pulse. ICM biopsies were isolated from TE biopsies using a previously published method [16]. In cases where inner cell mass samples could not be isolated, TE only samples were taken or inner cell mass with few TE cells was obtained and considered as ICM samples.
All re-biopsied samples were placed in 2.5 μL of PBS media in Eppendorf PCR tubes and stored at − 4 °C. The re-biopsied samples were subjected to the same PGT-A protocol previously employed by the reference laboratory; whole genome amplification using the SurePlex DNA Amplification system (Illumina, San Diego CA), followed by the VeriSeq DNA Library prep (Illumina, San Diego CA) and MiSeq (S/N MSQ-M00595) NGS sequencing, was performed. MiSeq NGS analysis was completed with a maximum of 24 samples per run. The whole genome amplification, VeriSeq library prep, and MiSeq sequencing steps were performed at an academic Genomics Core laboratory, distinct from the reference laboratory where the initial clinical biopsies were analyzed. The NGS analysis utilized the same analytical techniques, which had been applied to the initial clinical biopsies at the reference laboratory (except the two euploid samples, which had been analyzed using aCGH at the same reference laboratory). The authors who were not involved in the analysis of the initial biopsy result interpreted the NGS results of the re-biopsied specimens.
Results were interpreted using BlueFuse Multi Software (Illumina, San Diego) and determined by manual interpretation by the same investigator for all samples, then correlated to previous clinical NGS results performed by the reference laboratory. The primary outcomes of the study were concordance between the initial TE biopsy and repeat biopsies (as a measure of reliability), and concordance between the TE and ICM (a measure of accuracy of PGT-A). The diagnosis criterion used in identifying aneuploidy was defined by a specific copy number variation (CNV) of 80% or more (< 1.2 = monosomy and > 2.8 = trisomy). The diagnostic criterion used to categorize a chromosome as being mosaic was defined by specific CNV threshold (1.21–1.79 = mosaic monosomy, 2.21–2.79 = mosaic trisomy). Both diagnostic criteria are based on the most current clinical recommendations by the Preimplantation Genetic Diagnosis International Society [7].
Results showing chaotic profile or excessive overall noise (derivative-log-ratio (DLR)) 0.4 or greater were classified as un-interpretable, per recommendations by the Illumina VeriSeq PGS-MiSeq QC Assessment Guide [17]. MiSeq run quality metrics were evaluated for each run using the Sequence Analysis Viewer (Illumina, San Diego, CA) software. Statistical analysis was performed using chi-square, Poisson’s expectation, and linear regression. Re-biopsy results were determined to be concordant (the exact same result as the initial biopsy) or discordant (containing a previously disomic chromosome that shows monosomy, trisomy, or mosaicism, the previously diagnosed aneuploid chromosome is found to be complementary (monosomy instead of trisomy) or mosaic, or the mosaic chromosome is found to be fully aneuploid, or disomic). Mosaic results were determined as being high level (≥ 40%) or low level (< 40%) based on prior studies discussing the diagnosis thresholds and outcomes for embryos with varying degrees of mosaicism [13, 18]. The discordant results were then further categorized as to whether could be considered clinically relevant (concordant); for example, aneuploid discordant results that showed high-level mosaicism (≥ 40%) or the complementary aneuploidy were considered to be clinically concordant. The end goal being able to identify whether PGT-A using NGS of TE biopsy is able to reliably categorize an embryo as being transferable or non-transferable.
Results
Thirty-two blastocysts from 17 patients were accessioned for this study. Patient and cycle characteristics are summarized in Table 1.
The results from initial clinical biopsies indicated that 10 embryos were euploid (8 from blastocysts previously tested with NGS and 2 from blastocysts previously tested with aCGH). Four embryos were aneuploid for either one or two chromosomes, and 18 embryos were aneuploid-mosaic (aneuploid for one chromosome and mosaic for another). Each blastocyst was re-biopsied, yielding 129 samples comprising 90 TE (69.8%) and 39 ICM (30.2%) biopsies. For each re-biopsied specimen, whole genome amplification and NGS were performed over six MiSeq runs. NGS results for 24 re-biopsied specimens (19.4%) were not interpretable because of noise levels greater than 0.4 (chaotic). The 24 chaotic results consisted of 16 (66.7%) TE samples and 8 (33.3%) ICM samples. The un-interpretable results were biopsies from 16 embryos, all of which were aneuploid-mosaic (13) or aneuploid (3). These samples were not included in further analysis.
NGS results for 105 biopsy specimens were included in the analysis. The average total reads (928,413 ± 282,245), percent mapped reads (81.22% ± 1.22%), and filtered reads (536,363 ± 201,248) for these samples were within established recommendations by Munne et al. [19] and the Illumina VeriSeq PGS-MiSeq QC Assessment Guide [17].
Concordance per biopsy
Re-biopsied specimens were considered concordant when they had the exact same result as the initial biopsy (no additional chromosomes with any aneuploidy or mosaicism and the same directionality of aneuploidy or mosaicism of chromosomes diagnosed to not be disomic). In total, 40.0% of the re-biopsied specimens (42/105) were concordant for all chromosomes in the initial biopsy. Of these, the concordance for inner cell mass (ICM) samples was 31.4% (11/35) and 44.3% (31/70) for trophectoderm (TE) samples (P = 0.11). When segregated by embryo type, the euploid embryo samples had 82.9% (34/41) concordance, aneuploid embryo samples had 46.2% (6/13) concordance, and aneuploid plus mosaic embryo samples had 3.9% (2/51) concordance.
The three groups of embryos had significantly different biopsy concordances (P < 0.001). Further comparisons were done combining mosaic blastocysts with aneuploid-mosaic blastocysts due to the smaller number of re-biopsied specimens from blastocysts with initial biopsy results of aneuploidy without mosaicism. The concordances for ICM and TE were similar for re-biopsy of euploid blastocysts (ICM 72.70% (8/11) vs. TE 86.67% (26/30); P = 0.167) and for blastocyst with any aneuploidy (ICM 16.67% (4/24) vs TE 10% (4/40); P = 0.232). In the following sections, we will explore these different concordances/discordances as chromosomal concordances for both ICM and TE biopsies.
Re-biopsy of euploid embryos
Forty-one re-biopsied specimens were obtained from 10 euploid embryos, 33 samples from 8 blastocysts diagnosed previously by NGS and 8 samples from 2 blastocysts diagnosed previously by aCGH. Discordance was seen in at least 1 specimen in 37.5% (3/8) of NGS blastocysts and 100% (2/2) of aCGH euploid blastocysts.
In order to compare the incidence of concordance and discordance, we chose to examine the concordance for each chromosome analyzed in each biopsy specimen. We refer to the concordance for individual chromosomes as the chromosomal concordance. Of the 1886 euploid chromosomes expected from initial euploid results (disomic for each autosome plus two sex chromosomes), 99.5% (1876) were concordant with the original results and 0.54% (10) were discordant (Table 2). Of the 10 discordant results, 5 were whole chromosome mosaic discordances and 5 were mosaic partial aneuploidies (7 of which were low-level mosaic (< 40%)).
Concordance per chromosome for the aCGH euploid embryos was 98.6% (363/368 chromosomes), which was significantly different than the concordance for the 8 NGS euploid embryos at 99.7% (1513/1518) (Table 2).
Re-biopsy of aneuploid embryos
Thirteen re-biopsied specimens were obtained from 4 blastocysts for which the results of the initial, clinical biopsy indicated either one or two aneuploid chromosomes (no previously diagnosed mosaicism). Of the 4 embryos, 100% (4/4) had results of at least one re-biopsied specimen that were concordant with the results of the initial biopsy. Three (75%) of the aneuploid embryos had at least one re-biopsied specimen that was discordant. None of the discordant biopsies was euploid.
Of 552 chromosomes with disomic results in the aneuploid embryos, 521 (94.4%) were concordant and 31 (5.6%) were discordant in the re-biopsied specimens (Table 2). All 31 (5.6%) were detected as mosaic aneuploidies in the re-biopsied specimens.
There were 23 chromosomes with aneuploid results in the initial biopsy; 19 (82.6%) were found to be concordant in re-biopsied specimens (Table 3). Two (8.6%) re-biopsied specimens showed that the aneuploid chromosome was found to be disomic; however, several additional mosaic chromosomes were seen within both samples.
Concordance of aneuploid-mosaic embryos
Fifty-one re-biopsied specimens were obtained from 18 aneuploid-mosaic blastocysts, in which a single aneuploid chromosome plus a single mosaic chromosome was identified in the initial biopsy. The total disomic chromosomal concordance rate for the aneuploid-mosaic embryos was 95.5% (2052/2142), with 90.1% (109/121) of the discordances being mosaic chromosomes (Table 2).
Of the 18 embryos, 11.1% (2/18) had results with at least one re-biopsied specimen that was exactly concordant with the results of the initial biopsy. Each of these two embryos had one ICM re-biopsied sample showing the same result as the initial biopsy. All of the discordant biopsy results included either additional aneuploid or mosaic chromosomes or resulted in the mosaic chromosome as being aneuploid or disomic. None of the re-biopsied samples had results that indicated euploidy.
A total of 51 re-biopsies from 18 aneuploid-mosaic embryos were included in the analysis with a 95.7% (2052/2142) disomic concordance rate (Table 2). The aneuploid chromosome concordance was evaluated separately from mosaic chromosome concordance within these same aneuploid-mosaic embryos. For the aneuploid chromosome, 88.9% (16/18) of the embryos had at least one re-biopsied specimen with the same aneuploid chromosome and the remaining 11.1% (2/18) of the embryos had at least one re-biopsied specimen with the complementary aneuploidy for the same chromosome (e.g., monosomy in place of trisomy). Considering all 51 aneuploid-mosaic re-biopsied specimens, 70.6% (36/51) had results that were concordant for the aneuploid chromosome (Table 3) and 29.4% (15/51) were discordant.
The aneuploid-mosaic embryos consisted of both full and partial mosaic chromosomes. The majority, (14/18 (77.8%)) were full chromosome mosaic aneuploidies and 22.2% (4/18) were mosaic partial aneuploidies. We have considered these embryos separately.
The 14 blastocysts with full chromosome mosaic aneuploidy had a total of 39 re-biopsy results included in the analysis. Only 14.3% (4/14) of the blastocysts had at least one re-biopsied specimen that showed the same mosaic chromosome as being mosaic, which included a total of 15.3% (6/39) re-biopsied specimens concordant for the mosaic chromosome (Table 4).
The four blastocysts with a mosaic partial aneuploidy had a total of 12 re-biopsied specimens included in the analysis. All of the 12 re-biopsied specimens were discordant for the partial mosaic chromosomes (Table 4); however, one (8.3%) of the samples had a whole chromosome mosaicism seen for the same chromosome found to be partial chromosome mosaic in the initial biopsy. The remainder (11/12) showed the partial mosaic chromosome to be disomic in the re-biopsied specimens.
In total, there were 51 re-biopsied samples from embryos containing one mosaic chromosome. The overall mosaic concordance rate inclusive of both types of mosaic embryos was 11.8% (6/51). No difference was seen between concordance rates comparing the TE and ICM (P > 0.05) (Table 4).
Concordance from aneuploidy combined blastocysts (aneuploid and aneuploid-mosaic embryos together)
Sixty-four samples had aneuploid chromosomes diagnosed in the initial biopsy, with 96.9% (62/64) confirming that the same aneuploid chromosomes were not disomic in the repeat biopsy. True aneuploidy was seen in 74.2% (46/62) of biopsies, while the remaining 25.8% (16/62) showed high-level mosaicism (≥ 40%).
In total, there were 74 aneuploid chromosomes from the 64 aneuploid and aneuploid-mosaic re-biopsied samples, with an overall aneuploid chromosome concordance rate of 74.3% (55/74) (Table 3). Only 2 (10.5%) of the discordant aneuploid chromosomes were disomic in the re-biopsied samples, arising from TE samples from differing aneuploid-mosaic blastocyst. Both, however, had additional chromosomes that were aneuploid or mosaic.
The 24 ICM re-biopsied samples included 28 aneuploid chromosomes, which showed 23 (82.1%) to be concordant. The ICM discordances seen were all high-level mosaics (≥ 40%) for the same aneuploid chromosome. The TE and ICM showed no difference in aneuploid concordance when aneuploid and aneuploid-mosaic embryos were combined (P > 0.05).
Comparisons between embryo types
The chromosomal concordances were compared between all 3 chromosome types: disomic, aneuploid, and mosaic. The disomic concordance results were significantly different comparing the 3 groups (P < 0.001). Further comparison between aneuploid and aneuploid-mosaic blastocysts showed no difference in the disomic concordance rates (P = 0.15; Table 2). Therefore, the concordances for the aneuploid blastocysts and the aneuploid plus mosaic blastocysts were combined for comparison with the euploid blastocysts in many cases. The disomic chromosome concordance for euploid embryos was significantly greater than the combined aneuploid group (P < 0.001). The disomic chromosome concordance (94.4%) for the aneuploid combined group was compared with its aneuploid chromosome concordance rate (74.3%), which was significantly different (P < 0.001). The aneuploid-mosaic embryos had a disomic chromosome concordance of 95.7%, which was significantly greater than both mosaic concordance of 11.8% (P < 0.001) and aneuploid concordance of 70.6% (36/51) (P < 0.001).
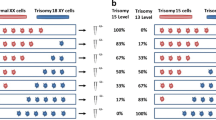
In order to assess the relationship between the disomic, aneuploid, and mosaic concordances to one another between the embryo types, a Poisson expectation calculation was performed. The number of discordant chromosomes per re-biopsy for euploid and the aneuploidy combined group was calculated. Using these values, the Poisson expectation was performed and indicated that the distribution of discordances for euploid embryos was consistent with the expectations for random, independent events (Fig. 1a). For the combined aneuploid embryo group, the number of discordant chromosomes showed a distribution of discordances inconsistent with the expectations for random, independent events (Fig. 1b), suggesting that in these embryos the discordances did not occur independently.

Poisson analysis of the number of disomy discordances per embryo. a The number of discordances per re-biopsied specimen was small (average = 0.244 per specimen). The number of biopsies with 0, 1, or > 1 discordances for disomic chromosomes was compared with Poisson expectations using the observed mean number of discordances. The observed distribution was not significantly different from the Poisson expectations (χ2 = 0.51; 1 degree of freedom; P > 0.05). b The number of discordances per re-biopsied specimens from blastocysts with initial results indicating aneuploidy or aneuploidy plus mosaicism was larger (average = 2.80 per specimen). The number of biopsies with 0, 1, 2, 3, and > 3 discordances was compared with Poisson expectations using the observed mean number of discordances. The observed distribution was significantly different than the expected distribution (χ2 = 7.93 with 3 degrees of freedom; P < 0.05)
Chromosomal concordance for the inner cell mass
Thirty-five ICM re-biopsied samples were included in the analysis with an overall disomic concordance rate of 97.6% (1481/1516) (Table 2). The 11 ICM re-biopsied samples from euploid embryos had a disomic concordance rate of 99.4% (503/506). The ICM biopsy results from aCGH showed 75% (1/4) biopsy concordance rate, while the NGS ICM biopsy concordance rate was 100% (7/7).
The 24 ICM re-biopsied samples from the aneuploid combined group had an aneuploid chromosomal concordance of 82.1% (23/28) (Table 3). One blastocyst was included in both the concordant and discordant groups because it had two biopsies of the ICM: one biopsy was concordant for the aneuploid chromosome, whereas the other biopsy had a mosaic result for the same aneuploid chromosome—neither showing the aneuploid chromosome to be disomic.
Only 13 of the 18 blastocysts with mosaic chromosomes had ICM samples, totaling 19 ICM re-biopsies included in the analysis. Only 4 (21.1%) were mosaic concordant, while 15 (78.9%) were discordant (Table 4). When disomic, aneuploid, and mosaic chromosomal concordances within the ICM samples were compared, significant differences were noted (χ2 = 295 P < 0.001), as well as between the aneuploid and mosaic concordances groups (χ2 = 14.9; P < 0.001).
Chromosomal concordance for the trophectoderm
The disomic concordance for TE re-biopsied specimens was 88.5% (23/26) in NGS euploid embryos and 75% (3/4) in aCGH euploid embryos. The TE disomic concordance rate was 98.9% (382/384) for aCGH embryos and 99.6% (1191/1196) for NGS embryos (P = 0.14).
There were 40 TE re-biopsied specimens from 21 of the 22 blastocysts with aneuploidy (aneuploid combined group). The disomic concordance rate of these TE samples was 96.9% (2968/3064) and the aneuploid chromosome concordance was 69.6% (32/46) (P < 0.001).
The aneuploid-mosaic embryos had 32 TE re-biopsied specimens (from 16/18 blastocysts) included in the analysis. Two (6.3%) showed mosaic chromosomal concordance, with the majority (93.8% (30/32)) not being mosaic concordant (Table 4).
Comparison of chromosomal concordances between ICM and TE
Disomic chromosome concordance was 97.6% for ICM re-biopsied samples compared with that of TE re-biopsied samples (96.9%) with no significant difference (P = 0.11). Aneuploid chromosome concordance in ICM re-biopsied samples was 82.1%, not different from TE re-biopsied sample concordance of 69.6% (P = 0.17). Mosaic chromosome concordance rates were low for both ICM (21.1%) and TE (6.3%) re-biopsied samples and with no difference between groups (P = 0.11).
A post hoc power analysis was conducted to assess if samples sizes were adequate to detect a 5% or greater difference in concordance between ICM and TE re-biopsied samples. The sample size of 4580 was used for disomic concordance of euploid embryos, with an alpha level of P < 0.05 which showed a power of 0.86 indicating an adequate sample size. The sample sizes of 74 (aneuploid concordance) and 51 (mosaic concordance) showed power of 0.064 and 0.056, respectively, indicating that these two groups were underpowered.
Clinically relevant concordance
In clinical practice, decisions about whether an embryo is considered transferable vs non-transferable are made based on PGT-A results of TE biopsies. The results of our re-biopsied specimens were analyzed in order to determine how often the results would have changed the clinical decision to transfer the embryo.
Transfers of embryos with higher level (≥ 40%) mosaic chromosomes behave closer to those of aneuploid embryos [13, 20] with lower implantation and ongoing pregnancy rates, favoring transfer of low-level mosaicism over those with higher level mosaicism [13]. For this reason, the aneuploid clinical concordance rate increases to 97.6% (72/74) when results with high-level mosaicism are included as concordant.
Clinical concordance for mosaic chromosomes is inclusive of a wider range of results. The underlying causes of mosaicism lead to malsegregation of chromosomes resulting in daughter cells with complementary aneuploidies. As a result, re-biopsy results showing the mosaic chromosome to be complementary mosaic or aneuploid are considered to be clinically concordant. The clinical concordance rate of mosaic chromosomes thereby increases to 35.3% (18/51).
The disomic concordance rate for euploid embryos was high (99.5%); 3/10 (30%) were partial high-level mosaic results, while 7/10 (70%) were low-level mosaics. Although high-level mosaics are likely to be considered comparable to aneuploid chromosomes, the implications of low-level mosaicism are unclear and thus, these results were not considered as concordant with disomy.
Significant differences were seen in clinical concordance rates between disomic, aneuploid, and mosaic chromosomes (χ2 = 87.4, P < 0.001), as well as between aneuploid and mosaic concordance (χ2 = 54.5, P < 0.001).
A summary of all biopsy results is included in Table 5.
Discussion
Recently, trophectoderm biopsy of the day-5 to 6 blastocyst-stage embryo has become the standard method of biopsy for PGT-A. Its reliability, accuracy, and the diagnosis of embryonic mosaicism, however, continue to make PGT-A a topic of great clinical interest, albeit a controversial one. The increased reporting of mosaic embryos with the use of NGS has many questions on the validity of the results as well as the safety when transferring these mosaic embryos. Several questions remain unanswered. What is the risk of mosaic fetuses or newborns following transfer of mosaic embryos and how well does NGS of TE biopsy represent the ICM and resulting embryo [21]? Our study demonstrated that NGS for comprehensive chromosome screening of TE biopsies provides an accurate and reliable representation of the ICM when detecting aneuploidy but not for mosaicism.
How reliable is a diagnosis of aneuploidy from PGT-A using TE biopsy with NGS?
Our data showed that PGT-A can reliably use TE biopsy to predict aneuploidy and euploidy, however not mosaicism. The positive predictive value (PPV) of PGT-A using NGS of detecting an aneuploid chromosome was shown to be 84.6% with a negative predictive value (NPV) of 99.0%. This suggests that a chromosome diagnosed as being aneuploid is likely to be aneuploid, and in the absence of aneuploidy, then with a high degree of certainty, it can be considered disomic. If we include the re-biopsied specimens with clinically relevant concordances (the aneuploid chromosome was found to be either complementary or mosaic), then the PPV of determining aneuploidy increases to 87.8% and the NPV to 99.9%.
How accurate is PGT-A using TE biopsy at determining the ploidy of the fetus? (How concordant are PGT-A results between ICM and TE?)
Our study finds that the TE biopsy is indeed remarkable in its ability to determine ploidy of the fetus. The inaccuracies as detected by chromosomal discordances of 2.4% in ICM samples are comparable (if not less than) with those of the aneuploid live births documented in prior studies [22]. There were 18 aneuploid and aneuploid-mosaic embryos containing at least one ICM re-biopsied specimen, all of which confirmed the aneuploid chromosome seen in the initial TE biopsy (inclusive of results showing the aneuploid chromosome as high-level mosaicism or complementary aneuploid). Low-level mosaicism was seen in aCGH ICM euploid samples, however none from ICM samples from NGS euploid embryos. Our study supports prior studies that demonstrate the NGS technology’s enhanced ability to pick up mosaicism [23] as seen by the greater percentage of aCGH euploid embryos showing mosaic results, thus validating the accuracy of euploidy in the TE biopsy using NGS as the testing modality.
Albeit low, the concordance rates for the mosaic chromosome did not differ between biopsied ICM (21.1%) and TE (6.3%) (P = 0.07). These findings vary from those seen in mouse model studies [14], indicating that, in humans, there does not appear to be a preferential allocation of mosaicism within the TE as compared with the ICM at this early stage. However, the overall low mosaic concordance rate does not allow for clear conclusions to be made regarding the reliability and accuracy of diagnosing the true status of mosaicism within a fetus via TE biopsy.
Nevertheless, our study does show that PGT-A using NGS continues to be a reliable method in determining the euploidy or aneuploidy status of the ICM and resulting fetus. A diagnosis as determined by the TE is a reliable representation of the future live born baby and seems to be consistent with prior studies using other PGT modalities such as FISH and aCGH [16, 24].
How do we interpret a mosaic result from a PGT-A of TE biopsy with NGS?
As stated previously, the same degree of certainty is not achieved when considering the diagnosis of mosaicism using PGT-A. The PPV of using TE biopsy with NGS to diagnose mosaicism was remarkably lower at 37.5% with a NPV of 97.7%. Although PPV (64.3%) and NPV (98.3%) increased when the clinical concordance rate (35.3%) for mosaicism was used, the data corroborates the continued uncertainty of mosaicism as evident by prior studies reporting healthy live births from transfer of mosaic embryos [13]. We showed that a TE biopsy without a diagnosis of mosaicism or aneuploidy can reliably be called euploid, but the true status of an embryo diagnosed as mosaic is unknown. Recently, a study by Grati et al. stratified various mosaic embryos into different risk classifications in an attempt to provide some insight into which are more likely to be considered acceptable for transfer [18]. Monosomy mosaics were declared lower risk than trisomies; however (as in our study), the degree of mosaicism in the initial biopsy does not appear to offer any further insight into the prognosis of that embryo transfer. Intuitively, the greater degree of mosaicism seen in the TE biopsy should correlate with a greater percentage of aneuploid cells within the sample. In our study, many of the aneuploid embryos had re-biopsied specimens showing the aneuploid chromosome to not be completely aneuploid, but instead a high-level mosaic (≥ 40%) for that same chromosome. High-level mosaicism seems to be associated with lower implantation rates; however, no trend was noted when attempting to reproduce the mosaic findings in subsequent biopsies (R = 0.1044; R2 = 0.010; slope for linear regression, 0.2145, P > 0.05). Mosaic embryos with a lower percent mosaicism appear to have more favorable pregnancy outcomes [13], but our study does not corroborate this. Our data showed 64.7% of the mosaic results seen in the initial biopsy went undetected in the re-biopsied specimens (resulted as disomic), with no trend regarding the percent mosaicism found in the initial biopsy. The percent mosaicism may be more suggestive of when the mitotic malsegregations occurred during embryo development and less likely to determine the reliability of PGT-A to determine mosaicism in a blastocyst. Due to the small sample size and many of our mosaic embryos being low-level mosaic (< 40%), we may be limited in the conclusions that can be made in regard to the percent mosaicism of the embryo contributing to the reproducibility of finding mosaicism in subsequent biopsies.
If mosaicism is believed to occur through malsegregation of chromosomes during mitosis, the prevalence of mosaic aneuploidies throughout the blastocyst depends on the stage at which the mitotic malsegregation occurs in the embryo. Mitotic malsegregations occurring early in development will impact a larger portion of the cells in the blastocyst and those occurring later in development will impact a smaller portion of the cells in the blastocyst. Therefore, we expect that mosaicism detected in only a small portion of the biopsies or in a large portion of the biopsies could reveal when the mosaicism-inducing malsegregations occurred.
Alternatively, a non-biological cause of mosaic diagnosis could be secondary to greater fluctuations in the copy number for the various small chromosome sections, making the data interpretation variable. Biopsies with more stochastic fluctuations may be more prone to detection of discordant results and potentially lead to a higher incidence of mosaic results, possibly only due to inaccuracies in interpreting the results. Albeit a low occurrence of mosaic concordance was noted, the presence of any mosaic concordance confirms that the initial diagnosis of the mosaicism was not simply a spurious interpretation of noisy NGS data but rather a true case of a mix of aneuploid and euploid cells.
The overall disomic chromosomal discordance rate for all embryos in our study was found to be less than 5% (the majority of which were low-level mosaicism). This suggests that thresholds designed to detect mosaicism with a 95% confidence limit would routinely allow up to 5% of chromosomal concordances to be classified as type I errors (i.e., disomic chromosomes detected as discordances). It is unclear whether these mosaic discordances are truly detection of mosaic aneuploidy or are simply type I errors (disomic chromosomes erroneously identified as aneuploid or mosaic). This low discordance suggests that disomy accuracy is really much higher (99.7%) when low-level mosaics (< 40%) are considered concordant.
This continued lack of certainty when discussing mosaicism in TE biopsies warrants further studies such as Grati et al. [18] to further elucidate potential adverse outcomes from the transfer of mosaic embryos. The low reproducibility of the mosaic chromosomes merits careful consideration of the fate of these embryos prior to deeming them as unacceptable for transfer, with varying potential for healthy live births [12, 25].
Is there a difference in chromosomal concordance in euploid versus aneuploid blastocysts?
We chose to consider euploid concordance by assessing disomic chromosomal concordance among all embryo types and comparing them. This seemed the most appropriate given this is the only type of chromosomal concordance that can be compared between euploid and aneuploid embryos (since there are no aneuploid or mosaic chromosomes in euploid blastocysts to be discordant). Significant differences in the disomic chromosomal concordance in euploid blasts (99.5%) are seen compared with aneuploidy blastocysts (95.7%) (P < 0.001), illustrating the notion that when a TE biopsy indicates all chromosomes within an embryo are disomic (euploid), that blastocyst is significantly less likely to have misdiagnosed a mosaic or aneuploid chromosome as being disomic (false negative).
Among the 131 (2.9%) discordant disomic chromosomes, the majority (93.1%) resulted as mosaic (114 full chromosomes, 8 partial chromosomes) and thus could be considered to have weakly confirmed the initial result but with less absolute agreement (all but 22 were low-level mosaics (< 40%)). Considering the 9 discordances that were found to be aneuploid, plus the high-level mosaics (22), the overall clinically relevant chromosomal discordance rate is 0.7% (31/4580).
When discordances are categorized by embryo type, a difference in disomic chromosome discordance was seen (P < 0.001). Euploid blastocyst (both aCGH- and NGS-diagnosed) only had mosaic discordances, the majority (70%) were low-level (< 40%), and none showed aneuploidy. Embryos diagnosed as either aneuploid or aneuploid-mosaic showed higher rates of discordances in the repeat biopsies. The majority of these were mosaic and not true aneuploid as well. When the overall discordance rates of aneuploid and aneuploid-mosaic embryos were compared with one another, no difference was noted (P > 0.05). Among these embryos, the vast majority (92.6%) of discordances in re-biopsied specimens were mosaic, with only a small percentage (7.4%) showing aneuploid results.
Poisson expectations (Fig. 1) were calculated to determine if discordances arose independently (of each other). This test of independence indicated that the disomic discordances occurred independently for re-biopsy results from embryos previously diagnosed as being euploid (Fig. 1a). The re-biopsied specimens showed a greater number of discordances seen within blastocysts previously diagnosed as being aneuploid and aneuploid-mosaic. These discordances did not match the Poison expectations for independent discordances (Fig. 1b). Therefore, they were generated in a way that lacked independence. The observation that discordance occurred independently in euploid embryos and without independence in aneuploid or aneuploid-mosaic embryos indicates that the initial biopsy predicts the independence of results for re-biopsied specimens. Biological explanations may include the idea that aneuploid embryos have more errors due to a common mechanism involving malsegregation of chromosomes during meiosis or mitosis. For example, a euploid initial result predicts that the incidence of discordances will be low whereas an aneuploid result predicts that the incidence of discordances in re-biopsied specimens will be both greater in number and less independent. The lack of independence could be associated with the underlying cause of aneuploidy (malsegregation) being more likely in embryos for which malsegregation has already been identified. The lack of independence seen among discordances within aneuploid embryos indicates that using the incidence of an aneuploid chromosome in one blastocyst to predict the incidence of aneuploidy in all blastocysts [21] may violate the principals of independence necessary to make valid numerical predictions.
Limitations
The diagnosis of mosaicism in a TE biopsy continues to pose a clinical dilemma. Prior studies have shown that the reliability of a mosaic result varies in TE, ICM, or whole blastocyst analysis [26, 27]. Our study, similarly, is unable to demonstrate whether mosaicism seen in the TE biopsy using NGS is a reliable determinant of whether that embryo should be considered safe for transfer. Limitations within our study may have contributed to these findings.
One notable limitation is that the mosaicism evaluated in our study may not be universally applicable, since all the blastocysts with mosaic results in the initial biopsy also shared an aneuploid result. The incidence of disomic concordance was significantly less in blastocysts when the initial biopsy had an aneuploid result compared with blastocysts that had initial euploid results. It is quite possible that the incidence of mosaicism could differ significantly between blastocysts with versus without aneuploidy, thus making our data less clinically applicable. Given the inconclusiveness of the outcomes of embryos diagnosed as mosaic, no mosaic embryos without additional aneuploidy were available for this study.
The analysis was performed in an academic genomics lab that does not routinely perform NGS on clinical samples. As a result, lab technique involved in amplification or DNA library prep could have led to NGS results with greater fluctuations or noise level when interpreting the data. This may have led to greater number of new mosaic chromosomes identified in the repeat biopsy specimens, and made the identification of the previously diagnosed mosaic chromosome more difficult, thus leading to falsely lower rates of mosaic concordance and greater rate of disomic discordance.
Additionally, post hoc power analysis showed that the sample size included in our study for aneuploid and mosaic chromosomes was underpowered to determine a 5% difference between ICM and TE concordance, thus making conclusions about the accuracy of TE biopsy limited. The sample size needed for both groups requires a large number of chromosomes (and embryos) and may be prohibitive due to limited availability of embryos for use in research at some institutions.
Lastly, the lack of uniformity between the ICM and TE biopsies may have introduced some bias into the analysis. Not all embryos had both ICM and TE re-biopsied samples included in the analysis and, in some cases, more than one ICM specimen was available for analysis from the same embryo. Given that discordances between ICM specimens from within the same embryo only occurred once, this likely did not have a significant effect on the interpretation of the results.
Conclusions
The incidence of concordance between the results of the initial biopsy and subsequent re-biopsied specimens was 97.1% for disomic chromosomes, 74.3% for aneuploid chromosomes, and 11.8% for mosaic chromosomes. Discordance did not occur independently and was significantly less prevalent in blastocysts with initial biopsy results indicating euploidy. Concordance results were not significantly different when comparing trophectoderm re-biopsy with inner cell mass biopsy, indicative that the inner cell mass at this early stage is not particularly protected from aneuploidies or mosaicism. Discordances were most frequently mosaic aneuploidies and, as such, were seldom indicative of non-mosaic aneuploidy or disomy that was not detected in the initial biopsy. By considering certain high-level mosaic results as aneuploid concordant, and aneuploid results as mosaic concordant, the clinical concordances can then be considered as 99.5%, 97.3%, and 35.3% for disomic, aneuploid, and mosaic chromosomes, respectively. The utility of the initial trophectoderm biopsy to determine the suitability of embryos for transfer was clearly demonstrated for euploid and aneuploid embryos however continues to be questioned for embryos diagnosed as mosaic by NGS.
References
Hassold TaH P. To err (meiotically) is human: the genesis of human aneuploidy. Nat Rev Genet. 2001;2:280–91.
Munné S, Weier H, Grifo J, Cohen J. Chromosome mosaicism in human embryos. Biol Reprod. 1994;51(3):373–9.
Munne S, Lee A, Rosenwaks Z, Grifo J, Cohen J. Diagnosis of major chromosome aneuploidies in human preimplantation embryos. Hum Reprod (Oxford, England). 1993;8(12):2185–91.
Schoolcraft WB, Fragouli E, Stevens J, Munne S, Katz-Jaffe MG, Wells D. Clinical application of comprehensive chromosomal screening at the blastocyst stage. Fertil Steril. 2010;94(5):1700–6. https://doi.org/10.1016/j.fertnstert.2009.10.015.
Malvestiti F, Agrati C, Grimi B, Pompilii E, Izzi C, Martinoni L, et al. Interpreting mosaicism in chorionic villi: results of a monocentric series of 1001 mosaics in chorionic villi with follow-up amniocentesis. Prenat Diagn. 2015;35(11):1117–27. https://doi.org/10.1002/pd.4656.
Maxwell SMGJ. Should every embryo undergo preimplantation genetic testing for aneuploidy? A review of the modern approach to in vitro fertilization. Best Pract Res Clin Obstet Gynaecol. 2018;53(Nov):38–47.
Cram DS, Leigh D, Handyside A, Rechitsky L, Xu K, Harton G, et al. PGDIS Position Statement on the Transfer of Mosaic Embryos 2019. Reprod BioMed Online. 2019;39(Supplement 1):e1–4.
Sachdev NMMS, Besser AG, Grifo JA. Diagnosis and clinical management of embryonic mosaicism. Fertil Steril. 2017;107(1):6–11.
Mantikou E, Wong KM, Repping S, Mastenbroek S. Molecular origin of mitotic aneuploidies in preimplantation embryos. Biochim Biophys Acta. 2012;1822(12):1921–30. https://doi.org/10.1016/j.bbadis.2012.06.013.
Kung A, Munne S, Bankowski B, Coates A, Wells D. Validation of next-generation sequencing for comprehensive chromosome screening of embryos. Reprod BioMed Online. 2015;31(6):760–9. https://doi.org/10.1016/j.rbmo.2015.09.002.
Friedenthal JMS, Munné S, Kramer Y, McCulloh DH, McCaffrey C, Grifo JA. Next generation sequencing for preimplantation genetic screening improves pregnancy outcomes compared with array comparative genomic hybridization in single thawed euploid embryo transfer cycles. Fertil Steril. 2018;109(Apr):627–32.
Greco E, Minasi MG, Fiorentino F. Healthy babies after intrauterine transfer of mosaic aneuploid blastocysts. N Engl J Med. 2015;373(21):2089–90. https://doi.org/10.1056/NEJMc1500421.
Munne SBJ, Large M, Martinez-Ortiz PA, Nisson H, Liu E, Tarozzi N, et al. Detailed investigation into the cytogenetic constitution and pregnancy outcome of replacing mosaic blastocysts detected with the use of high-resolution next-generation sequencing. Fertil Steril. 2017;108(1):62–71.
Helen Bolton SJLG, Van der AA N, Kumar P, Theunis K, Gallardo EF, Voet T, et al. Mouse model of chromosome mosaicism reveals lineage-specific depletion of aneuploid cells and normal developmental potential. Nat Commun. 2016;7(7):1165.
Vera-Rodriguez M, Rubio C. Assessing the true incidence of mosaicism in preimplantation embryos. Fertil Steril. 2017;107(15):1107–12.
Capalbo A, Wright G, Elliott T, Ubaldi FM, Rienzi L, Nagy ZP. FISH reanalysis of inner cell mass and trophectoderm samples of previously array-CGH screened blastocysts shows high accuracy of diagnosis and no major diagnostic impact of mosaicism at the blastocyst stage. Hum Reprod (Oxford, England). 2013;28(8):2298–307. https://doi.org/10.1093/humrep/det245.
Illumina. Veriseq PGS-MiSeq QC Assessment Guide. 2014.
Grati FRGG, Branca L, Maggi F, Simoni G, Yaron Y. An evidence-based scoring system for prioritizing mosaic aneuploid embryos following preimplantation genetic screening. Reprod Biol Endocrinol. 2018;2018(36):442–9.
Munné SWD. Detection of mosaicism at blastocyst stage with the use of high-resolution next-generation sequencing. Fertil Steril. 2017;107(5):1085–91.
Munné SSF, Grifo J, Zhang J, Beltran MP, Fragouli E, Fiorentino F. Clinical outcomes after the transfer of blastocysts characterized as mosaic by high resolution next generation sequencing- further insights. Eur J Med Genet. 2020;63(2):103741.
Gleicher N, Metzger J, Croft G, Kushnir VA, Albertini DF, Barad DH. A single trophectoderm biopsy at blastocyst stage is mathematically unable to determine embryo ploidy accurately enough for clinical use. Reprod Biol Endocrinol. 2017;15(1):33. https://doi.org/10.1186/s12958-017-0251-8.
Scott RT, Ferry K, Su J, Tao X, Scott K, Treff NR. Comprehensive chromosome screening is highly predictive of the reproductive potential of human embryos: a prospective, blinded, nonselection study. Fertil Steril. 2012;97. https://doi.org/10.1016/j.fertnstert.2012.01.104.
Goodrich D, Tao X, Bohrer C, Lonczak A, Xing T, Zimmerman R, et al. A randomized and blinded comparison of qPCR and NGS-based detection of aneuploidy in a cell line mixture model of blastocyst biopsy mosaicism. J Assist Reprod Genet. 2016;33(11):1473–80. https://doi.org/10.1007/s10815-016-0784-3.
Huang J, Yan L, Lu S, Zhao N, Qiao J. Re-analysis of aneuploidy blastocysts with an inner cell mass and different regional trophectoderm cells. J Assist Reprod Genet. 2017;34(4):487–93. https://doi.org/10.1007/s10815-017-0875-9.
Victor ARTJ, Brake AJ, Lepkowsky LT, Murphy AE, Griffin DK, McCoy RC, et al. One hundred mosaic embryos transferred prospectively in a single clinic: exploring when and why they result in healthy pregnancies. Fertil Steril. 2019;2019(111):280–93.
Victor AR, Griffin DK, Brake AJ, Tyndall JC, Murphy AE, Lepkowsky LT, et al. Assessment of aneuploidy concordance between clinical trophectoderm biopsy and blastocyst. Hum Reprod. 2019;34(1):181–92.
Lawrenz B, El Khatib I, Liñán A, Bayram A, Arnanz A, Chopra R, et al. The clinicians’ dilemma with mosaicism—an insight from inner cell mass biopsies. Hum Reprod. 2019;34(6):998–1010.
Author information
Authors and Affiliations
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Sachdev, N.M., McCulloh, D.H., Kramer, Y. et al. The reproducibility of trophectoderm biopsies in euploid, aneuploid, and mosaic embryos using independently verified next-generation sequencing (NGS): a pilot study. J Assist Reprod Genet 37, 559–571 (2020). https://doi.org/10.1007/s10815-020-01720-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10815-020-01720-x